
Polish Nurses’ Knowledge of Heart Failure Self-Management Principles

Abstract
:1. Background
2. Methods
2.1. Study Design and Sample
2.2. Instrument
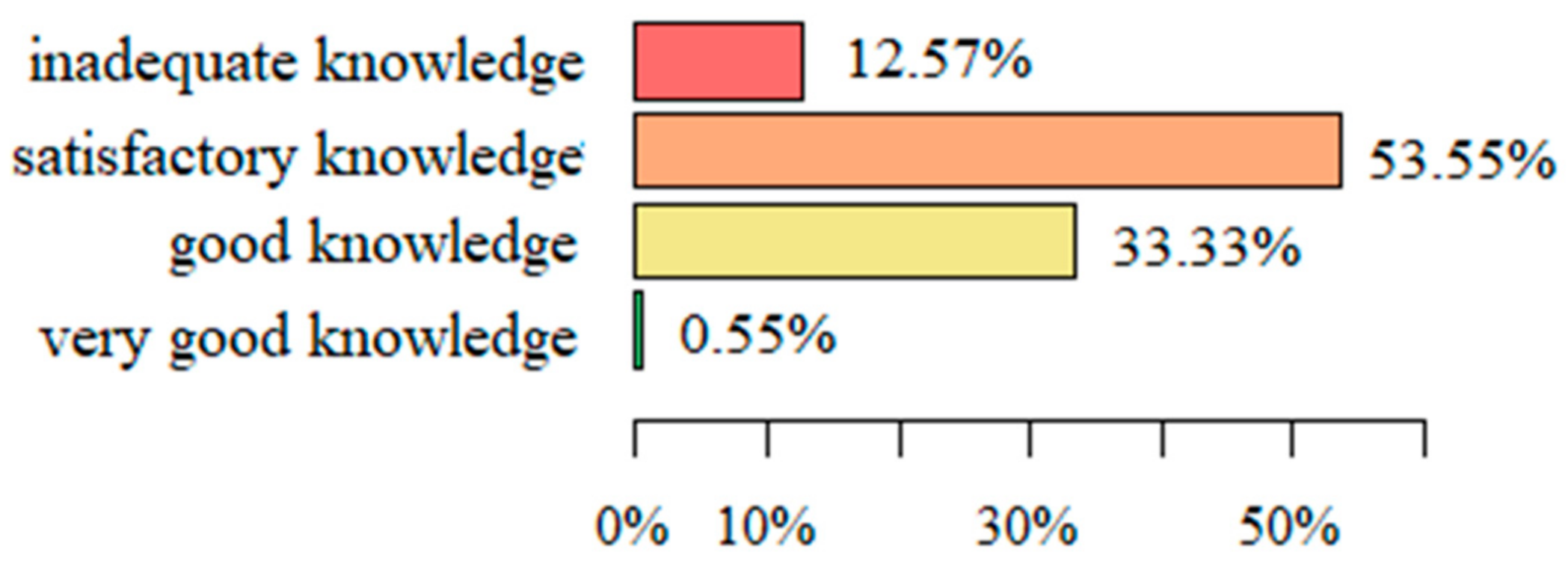
- 0–10 of correct answers (0–50% questions): inadequate knowledge;
- 11–15 of correct answers (50–75% questions): satisfactory knowledge;
- 16–18 of correct answers (75–90% questions): good knowledge; and
- 19–20 of correct answers (90–100% questions): very good knowledge.
2.3. Statistical Analysis
3. Results
3.1. Evaluation of Preparing for Education and Knowledge Regarding Issues of HF Patients and Their Preparation for Self-Care (The Nurses’ Knowledge of Heart Failure Education Principles Questionnaire)
3.2. Characteristics of Answers Regarding the Specific Subject Areas
3.3. Knowledge Regarding Individual Questions in the Nurses’ Knowledge of Heart Failure Education Principles Questionnaire
3.4. Analysis of Correlations between the Selected Sociodemographic Variables and the Level of Knowledge Related to the Score in The Nurses’ Knowledge of Heart Failure Education Principles Questionnaire
4. Discussion
5. Conclusions
5.1. Study Implications
5.2. Summary
5.3. Study Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nessler, J.; Kozierkiewicz, A.; Gackowski, A.; Ponikowski, P.; Hryniewiecki, T.; Gruchała, M.; Gąsior, M.; Grodzicki, T.; Kaźmierczak, J.; Legutko, J.; et al. Heart failure treatment in Poland in 2010–2017. Kardiol. Polska 2019, 77, 994–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Ziaeian, B.; Fonarow, B.Z.G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inamdar, A.A.; Inamdar, A.C. Heart Failure: Diagnosis, Management and Utilization. J. Clin. Med. 2016, 5, 62. [Google Scholar] [CrossRef]
- Nessler, J.; Zalewski, J.; Kozierkiewicz, A. Project of comprehensive care program for patients with heart failure. Kardiol. Inwazyjna 2018, 13, 10–17. [Google Scholar]
- Jankowska-Polańska, B.; Brzykowska, M.; Uchmanowicz, I.; Lisiak, M.; Rosinczuk, J. Polish Nurses’ Knowledge of Heart Failure Self-Care Education Principles. Clin. Nurse Spec. 2017, 31, E7–E13. [Google Scholar] [CrossRef]
- Nessler, J.; Kozierkiewicz, A.; Gackowski, A.; Ponikowski, P.; Straburzynska-Migaj, E.; Uchmanowicz, I.; Hoffman, P.; Chlebus, K.; Gielerak, G.; Gąsior, M.; et al. Coordinated heart failure care in Poland: Towards optimal organisation of the health care system. Kardiol. Polska 2018, 76, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Jankowska-Polańska, B.; Świątoniowska-Lonc, N.; Sławuta, A.; Krówczyńska, D.; Dudek, K.; Mazur, G. Patient-Reported Compliance in older age patients with chronic heart failure. PLoS ONE 2020, 15, e0231076. [Google Scholar] [CrossRef] [Green Version]
- Riegel, B.; Westland, H.; Iovino, P.; Barelds, I.; Slot, J.B.; Stawnychy, M.A.; Osokpo, O.; Tarbi, E.; Trappenburg, J.C.; Vellone, E.; et al. Characteristics of self-care interventions for patients with a chronic condition: A scoping review. Int. J. Nurs. Stud. 2020, 116, 103713. [Google Scholar] [CrossRef]
- Albert, N.M.; Collier, S.; Sumodi, V.; Wilkinson, S.; Hammel, J.P.; Vopat, L.; Willis, C.; Bittel, B. Nurses’s knowledge of heart failure education principles. Heart Lung 2002, 31, 102–112. [Google Scholar] [CrossRef]
- Krówczyńska, D.; Jankowska-Polańska, B. Nurses as educators in the comprehensive heart failure care programme—Are we ready for it? Nurs. Open 2020, 7, 1–13. [Google Scholar] [CrossRef]
- Riegel, B.; Jaarsma, T.; Lee, C.S.; Strömberg, A. Integrating Symptoms into the Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2019, 42, 206–215. [Google Scholar] [CrossRef]
- Ross, A.; Yang, L.; Wehrlen, L.; Perez, A.; Farmer, N.; Bevans, M. Nurses and health-promoting self-care: Do we practice what we preach? J. Nurs. Manag. 2018, 27, 599–608. [Google Scholar] [CrossRef]
- Center For Disease Control: Chronic Disease Program. Chronic Disease Overview. Available online: http://www.cdc.gov/print.do?url=http://www.cdc.gov/nccdphp/overview.htm (accessed on 26 November 2021).
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Koelling, T.M.; Johnson, M.L.; Cody, R.J.; Aaronson, K.D. Discharge Education Improves Clinical Outcomes in Patients with Chronic Heart Failure. Circulation 2005, 111, 179–185. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Amatruda, J.; Smith, G.; A Mattera, J.; A Roumanis, S.; Radford, M.J.; Crombie, P.; Vaccarino, V. Randomized trial of an education and support intervention to preventreadmission of patients with heart failure. J. Am. Coll. Cardiol. 2002, 39, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Stewart, S.; Horowitz, J. Home-based intervention in congestive heart failure: Long-term implications on readmission and survival. ACC Curr. J. Rev. 2002, 11, 55–56. [Google Scholar] [CrossRef]
- De Loor, S. Nurse-managed heart failure programmes in the Netherlands. Eur. J. Cardiovasc. Nurs. 2002, 1, 123–129. [Google Scholar] [CrossRef]
- Hart, P.L.; Spiva, L.; Kimble, L.P. Nurses’ knowledge of heart failure education principles survey: A psychometric study. J. Clin. Nurs. 2011, 20, 3020–3028. [Google Scholar] [CrossRef]
- Krum, H.; Forbes, A.; Yallop, J.; Driscoll, A.; Croucher, J.; Chan, B.; A Clark, R.; Davidson, P.; Huynh, L.; Kasper, E.K.; et al. Telephone Support to Rural and Remote Patients with Heart Failure: The Chronic Heart Failure Assessment by Telephone (CHAT) study. Cardiovasc. Ther. 2013, 31, 230–237. [Google Scholar] [CrossRef]
- Clark, A.M.; Thompson, D.R. What heart failure programme works best? Wrong question, wrong assumptions. Eur. J. Heart Fail. 2010, 12, 1271–1273. [Google Scholar] [CrossRef]
- WHO Guidelines on Translation. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 26 November 2021).
- Mahramus, T.L.; Penoyer, D.A.; Sole, M.L.; Wilson, D.; Chamberlain, L.; Warrington, W. Clinical Nurse Specialist Assessment of Nurses’ Knowledge of Heart Failure. Clin. Nurse Spec. 2013, 27, 198–204. [Google Scholar] [CrossRef]
- Willette, E.W.; Surrells, D.; Davis, L.L.; Bush, C.T. Nurses’ knowledge of heart failure self-management. Prog. Cardiovasc. Nurs. 2007, 22, 190–195. [Google Scholar] [CrossRef]
- Kalogirou, F.; Lambrinou, E.; Middleton, N.; Sourtzi, P. Cypriot nurses’ knowledge of heart failure self-management principles. Eur. J. Cardiovasc. Nurs. 2012, 12, 159–166. [Google Scholar] [CrossRef]
- Fowler, S. Improving Community Health Nurses’ Knowledge of Heart Failure Education Principles. Home Healthc. Nurse 2012, 30, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Washburn, S.C.; Hornberger, C.A.; Klutman, A.; Skinner, L. Nurses’ Knowledge of Heart Failure Education Topics as Reported in a Small Midwestern Community Hospital. J. Cardiovasc. Nurs. 2005, 20, 215–220. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Values | |
|---|---|---|
| Age | Mean (SD) | 42.55 (10.03) |
| Me | 45 | |
| Years of experience | Mean (SD) | 19.41 (11.34) |
| Me | 21 | |
| Site | City hospital | 36 (11.84%) |
| Regional hospital in small towns | 19 (6.25%) | |
| Provincial specialist hospital | 87 (28.62%) | |
| University hospital | 161 (52.96%) | |
| Private sector | 1 (0.33%) | |
| Gender | Female | 276 (90.79%) |
| Male | 28 (9.21%) | |
| Place of work | Non-invasive treatment ward/Intensive care unit | 45 (14.80%) |
| Emergency care ward/Short-term care | 36 (11.84%) | |
| Telemetric monitoring cardiology ward | 89 (29.28%) | |
| Intensive cardiology care ward | 77 (25.33%) | |
| Cardiosurgery ward | 21 (6.91%) | |
| Cardiology rehabilitation ward | 17 (5.59%) | |
| Outpatient care | 19 (6.26%) | |
| Work schedule | Usually a day shift, on weekdays | 88 (28.95%) |
| Usually other than a day shift, on weekdays | 27 (8.88%) | |
| Usually weekend shifts | 1 (0.33%) | |
| Balance of day and other shifts | 180 (59.21%) | |
| Temporary/irregular work | 8 (2.63%) | |
| Level of education | Secondary | 88 (28.95%) |
| University | 216 (71.05%) | |
| Specializations | Yes | 77 (25.33%) |
| No | 227 (74.67%) | |
| Question | % of Correct Answers |
|---|---|
| 13. Lean delicate meat can be a part of the diet of patients with heart failure | 96.72 |
| 20. New onset or worsening of leg weakness, or lower ability to do exercises | 93.99 |
| 6. Abdominal swelling may suggest that excessive fluid is retained due to worsening heart failure | 91.26 |
| 19. New onset or worsening of fatigue | 89.62 |
| 1. Patients with heart failure should drink a lot of fluids every day | 86.89 |
| 14. Once patients’ heart failure symptoms are gone, there is no need for them to obtain daily weights | 83.06 |
| 17. A 2 kg weight gain in 5 days without symptoms | 82.51 |
| 7. If patients take drugs and modify their lifestyle as recommended, their heart failure will not recur | 78.14 |
| 16. BP of 80/56 without any heart failure symptoms | 77.05 |
| 2. As long as food is not salted, there are no dietary restrictions for patients with heart failure | 71.58 |
| 5. If patients put on weight more than 2 kg in 48 h without other heart failure | 69.95 |
| 12. If patients wake up at night and have breathing problems, and if these problems abate when patients get out of bed and walk around, it does not mean that heart failure has worsened | 69.4 |
| 18. Dizziness when getting up which subsides within 10–15 min | 69.4 |
| 11. When patients use additional pillows at night to relieve short breath, it does not mean that heart failure has worsened | 64.48 |
| 4. Patients with heart failure should limit activity and avoid most forms of exercises | 61.2 |
| 8. When patients feel pain, aspirin and non-steroid anti-inflammatory drugs (such as ibuprofen) should be recommended | 59.56 |
| 10. If patients feel thirsty, they can be allowed to give up the fluid regimen and drink | 49.73 |
| 9. Potassium-based salt substitutes (ex. “no-salt” or “salt-sense”) can be used to season food | 41.53 |
| 3. Coughing and nausea/loss of appetite are common symptoms of advanced HF. | 37.16 |
| 15. When assessing weight results, patients’ weight on a given day should be compared to their weight on the previous day, and not their ideal or ‘dry’ weight | 20.77 |
| Parameter | Knowledge Level | p Value | |
|---|---|---|---|
| Type of hospital | City hospital | 12.83 ± 2.88 | <0.001 NP |
| Regional hospital in small town | 11.89 ± 3.46 | ||
| Provincial specialist hospital | 14.98 ± 1.94 | ||
| University hospital | 14.35 ± 2.85 | ||
| Ward | Non-invasive treatment ward/Intensive care unit | 13.54 ± 1.90 | 0.001 NP |
| Emergency care ward/Short-term care | 12.53 ± 2.78 | ||
| Telemetric monitoring cardiology | 13.69 ± 3.00 | ||
| Intensive cardiology care | 14.68 ± 2.10 | ||
| Cardiosurgery | 15.44 ± 1.80 | ||
| Cardiology rehabilitation | 15.00 ± 3.10 | ||
| Type of job | Usually dayshift, on weekdays | 13.33 ± 2.55 | 0.013 NP |
| Usually other shiftthan on weekdays | 13.72 ± 2.44 | ||
| Balance of dayand other shifts | 14.47 ± 2.79 | ||
| Level of education | Secondary | 13.3 ± 2.68 | 0.038 |
| Higher | 14.24 ± 2.78 | ||
| Postgraduate education | Specialty | 14.7 ± 2.36 | 0.004 |
| No specialty | 13.39 ± 2.94 | ||
| Type of specializationeducation | Cardiological specialty | 15.52 ± 1.65 | 0.002 |
| Specialtyother than cardiological | 13.71 ± 2.84 | ||
| Correlation with the level of knowledge | |||
| Parameter | Correlation rate | p value | |
| Age | −0.088 | p = 0.244 NP | |
| Professional experience | −0.062 | p = 0.401 NP | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krówczyńska, D.; Jankowska-Polańska, B. Polish Nurses’ Knowledge of Heart Failure Self-Management Principles. Int. J. Environ. Res. Public Health 2022, 19, 1327. https://doi.org/10.3390/ijerph19031327
Krówczyńska D, Jankowska-Polańska B. Polish Nurses’ Knowledge of Heart Failure Self-Management Principles. International Journal of Environmental Research and Public Health. 2022; 19(3):1327. https://doi.org/10.3390/ijerph19031327
Chicago/Turabian StyleKrówczyńska, Dorota, and Beata Jankowska-Polańska. 2022. "Polish Nurses’ Knowledge of Heart Failure Self-Management Principles" International Journal of Environmental Research and Public Health 19, no. 3: 1327. https://doi.org/10.3390/ijerph19031327
APA StyleKrówczyńska, D., & Jankowska-Polańska, B. (2022). Polish Nurses’ Knowledge of Heart Failure Self-Management Principles. International Journal of Environmental Research and Public Health, 19(3), 1327. https://doi.org/10.3390/ijerph19031327