
Lived Experience of Dementia in the New Zealand Indian Community: A Qualitative Study with Family Care Givers and People Living with Dementia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Settings
2.2. Semi-Structured Interviews
2.3. Data Analysis
2.4. Ethics
3. Results
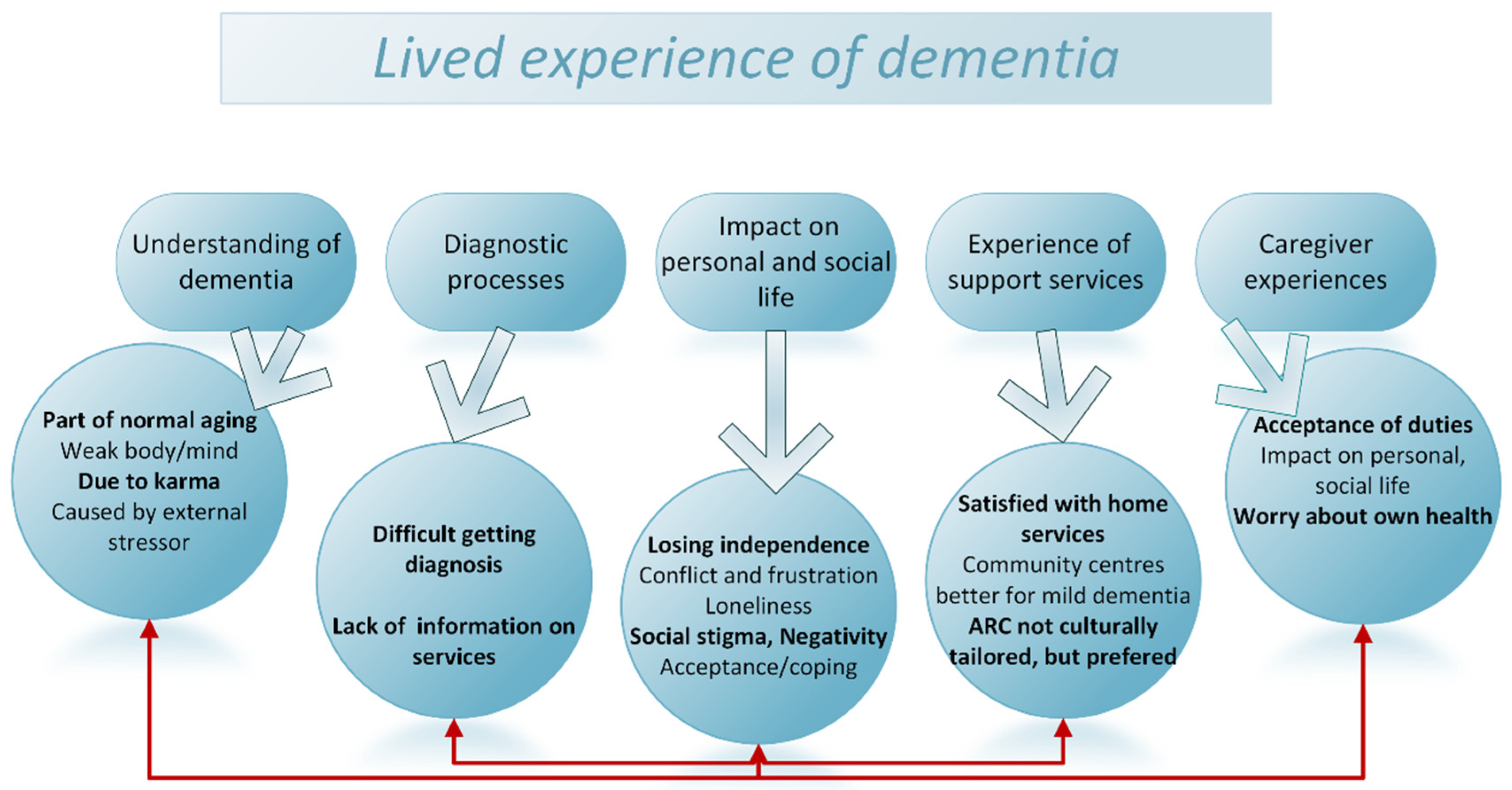
3.1. Thematic Analyses
3.1.1. Theme 1: Understanding of Dementia
- Subtheme 1.1: Dementia is a normal part of ageing
…this is normal…because he is getting older, he forgets. (C)
- Subtheme 1.2. Dementia may be caused by external stressors or ‘karma’
I see one person…he lost his job, he got dementia. (C)
There is loneliness here, without our own people. (C)
You are (un)lucky to get Alzheimer or unlucky to get dementia (laughs) (hmm hmm). That’s your, know your karma, it a rekha aur hmm depending in the lifestyle also you get dementia or not get dementia you know. (C)
3.1.2. Theme 2: Diagnostic Process
- Subtheme 2.1: Difficulty in getting a dementia diagnosis
She was very aggressive and… so I took her to the GP and then the GP said ummm… “she’s fine and old age, nothing to…” you know that, but I told to GP “no she’s definitely got some kind of an issue because you know, uhh, cos I know, my mum”. (C)
I had my scan in India, that’s what the doctors here used to diagnose me…doctor said its good you got the scan done. (P)
- Subtheme 2.2: Lack of information on services
GP referred to someone else, a girl came from Middlemore about 5–6 months before and asked about memory loss problem…like you people are asking about…and did not contact again…. (P)
3.1.3. Theme 3: Impact on Personal and Social Life (of Person Living with Dementia)
- Subtheme 3.1: Losing independence
Cooking… has got stopped altogether for her. We used to prepare meals together earlier. She used to cook alone but children stopped it. Doctor also advised not to go near stove. (C)
She prepared dinner today. She manages if I am at home…had to remind her every time to have dinner. (C)
Like I use to do a job…so this is my car (pointing out to his car)…I use to drive this…yes…so I use to go and take interviews from people…hmmm…on health issues…hmm…so I use to like that so much that I didn’t want to sit, …yes…when I got stroke, my driving also stopped. (P)
- Subtheme 3.2: Conflict and frustration between the person with dementia and caregiver
Like the routine house chores, she feels that she does that…hmm…but body…her body doesn’t allow it…hmm… She is not able to walk but from inside she thinks that she prepare meal, do the chores. (C)
Not stable, it is increasing. Because, earlier he use to help in house a lot, like putting bins outside and getting it in…he takes lots of time in wearing shoes, will wear it wrong. When we ask him to get shoes off… means he is getting too slow, thinks about it. This is why we don’t allow him to put bins now in a fear that he will fall. (C)
- Subtheme 3.3: Feelings of loneliness
If she learn how to drive a car then it will get difficult for me…I will be alone…how will I spend my time? (P)
- Subtheme 3.4: Social stigma and negativity
She has a little negativity…hmm…she thinks like the other person is thinking bad about her…hmm…it’s her thinking, and feeling…hmm. So she don’t like that kind… of people there. (C)
- Subtheme 3.5: Acceptance and coping strategies
I have memory problems…just sometimes I forget…a date, where I put something, that’s all, nothing major. (P)
I noticed…like…recently I…we read Ramayan*…read Hindi God books…hmm…yes…so it happens sometimes that I have read till here, and why have I started reading that again? …so I do not take stress of this. (P)
3.1.4. Theme 4: Experience of Support Services
- Subtheme 4.1: Satisfaction with home support services
First we take the service for 4 days, she goes to <support service> on Friday, hmm… but then she don’t want to go, hmm… then we introduced for fifth day then Saturday and Sunday. So now seven days coming. She got a fall in bathroom, hmmm…it’s pretty hard… so that’s why we put seven days for the shower as well. (C)
Yes they come at home sometime to give showers…we have asked for three times only. (C)
It’s enough. We are getting more than enough …okay…because we are getting help from <support service>…they give help for her. (C)
There comes three or four things, like you need physio help…need prescription since I am diabetic…so I need nurse…hmm… so they are always ready. Then they have references…like they referred me for my problem…of this…brain. (P)
He needs proper support every time people come over here they listen to us but no support … so many times he had a fall so many times we have had the same issue. …we seriously need some support I have someone who comes at the house and does cleaning and everything…. (C)
- Subtheme 4.2: Community centres more suited for people with mild dementia
Like today I went, there was a man aged 94 came…at <support service>…hmm… yes…so we feel very happy. Hmmm…he came on wheel chair…so we feel very happy, that this man also wants to live…yes…alright…someone who is 20 years older than me. (P)
People were cooperative, but as things are changing now, people are getting cut-off. (C)
- Subtheme 4.3: Aged Residential Care (ARC) does not meet cultural needs and expectations; culturally tailored ARC would make them feel at home
Yes, the main problem is that if you are from Fiji then you need someone who speaks Fiji Hindi…Language is the main problem and communication. If you find anyone speaks in your language…so, this is my feeling. (C)
Two things are important. Food is important (yes) umm…my mother also and we also in fact everybody…whosoever goes there takes food with them or make food for them…umm and then …umm… talking is important. (C)
Besides I am thinking that there should be a community here where there should be activities like playing carrom (popular board game in India). He would get better in this way, he would talk or play or look around, there was nothing like this what I would wish to. Not like, you go there and sit, then someone would feed you on time, just keep watching tv. You can watch that while staying at home. (C)
3.1.5. Theme 5: Caregiver Experiences
- Subtheme 5.1: Acceptance of duties and responsibilities
He has collected so many things on its own. Hmm…So, I do not touch these…I will pick them; he will collect again. (C)
There are expectations and responsibility at the children’s end, that’s why she is at home. (C)
- Subtheme 5.2: Impact on caregiver’s personal and social life
So we used to be party people but we slowly slowly restrict our social circle. (C)
I get bored staying at home…going for a walk around, come back having a look around of the playground. (C)
- Subtheme 5.3: Worries about own health
Now that I have aged, I said I cannot work too much now. (C)
I also get tired beta (*child), I am 77, will be 78 in December. So, it’s not all possible for me doing as well. I have got severe arthritis. (C)
Have to remind again…that she is human as well, look at her…she is sick as well…hmm… I am also doing (work). (C)
4. Discussion
4.1. Understanding of Dementia
4.2. Experience of the Diagnostic Process
4.3. Experience of Post-Diagnostic Support Services
4.4. Impact on Personal and Social Life of the Person Living with Dementia
4.5. Caregiver Experiences
4.6. Strengths
4.7. Limitations
4.8. Implications for Future Research and Service Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| What do we mean by dementia? | Getting the diagnosis Could you tell us how it has been for you? |
| “Different communities have different understandings of dementia, some see dementia as a disease, others see it as a natural part of normal ageing” | What did you first notice? Could you describe the changes What was your explanation |
| Tell me what you know about dementia and memory changes as people get older? | Who diagnosed you? (GP/hospital doc/other?) |
| What are the Indian terms use to talk about dementia? What is your understanding of dementia? What do those words mean? Why do you think older people get dementia? How are dementia and normal ageing related? What are the signs that someone has dementia? What do you think causes dementia? | Can you remember what happened Did they tell you the results of your blood tests/memory tests/scan? How did you feel when they told you the diagnosis? How were the staff towards you (sympathetic? value your opinion? respectful?) What kind of information did they offer on what to do next (or about services)? What were the most significant moments in the process (what do you remember most clearly)? |
| “Could you tell me more about that?” | “Could you tell me more about that?” |
| After the diagnosis. How are things now? What changes have you made to cope? What help do you need? How do your family/community help you? Has it changed your role in the family/community? What are the positive things that have happened? How do other people outside the family act towards you? Do you tell other people about the diagnosis? (if not, why not?) “Could you tell me more about that?” think about risks eg cooking, driving, being home alone; but also positive changes eg) more family time, increased understanding of their experience, less arguments with family as they understand the disorder | Services. What kind of help do you get?eg) GP, nurse, home/day care? What kind of things help/don’t help? What do you need but don’t get? Do you use “day centres”? (which one) How often do you go? What do you think about those services? What do you like/didn’t like? Is it specifically for people from …(country) How do you think things might change in the future? What do you think you might need in the future? “Could you tell me more about that?” If you weren’t living in New Zealand how do you think your life would be different? (if you were still living in …) |
| Questions for people with dementia | Questions for caregivers |
| Is there anything you want to add? What are your main concerns now? What is most difficult for you? What is most positive? In our culture we are often expected to look after our elders—how is that for youHave you planned for the future? “Could you tell me more about that?” | Is there anything you want to add? How many hours on average are you a care partner for [Name] at your home? Describe what caring you provide. How does your caring routine impact your daily life? Do you talk with others about your role as a care partner? How do you do this? Does anyone else provide care for [Name]? What is your reason for taking on the role of care partner? What are your main concerns around caring for your relative with dementia? What is most difficult for you? What is most positive? In our culture we are often expected to look after our elders—how is that for you Have you planned for the future? “Could you tell me more about that?” |
| Is there anything that we have missed? | Is there anything that we have missed? |
| “Could you tell me more about that?” | “Could you tell me more about that?” |
References
- Prince, M.J.; Anders, W.; Guerchet, M.M.; Ali, G.C.; Wu, Y.; Matthew, P. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Available online: http://www.alz.co.uk/research/world-report-2015 (accessed on 19 November 2021).
- Terum, T.M.; Andersen, J.R.; Rongve, A.; Aarsland, D.; Svendsboe, E.J.; Testad, I. The relationship of specific items on the Neuropsychiatric Inventory to caregiver burden in dementia: A systematic review. Int. J. Geriatr. Psychiatry 2017, 32, 703–717. [Google Scholar] [CrossRef] [PubMed]
- StatsNZ. 2018 Census Population and Dwelling Counts. Available online: https://www.stats.govt.nz/information-releases/2018-census-population-and-dwelling-counts (accessed on 19 November 2021).
- Auckland Council. Auckland’s Asian Population. Available online: https://www.aucklandcouncil.govt.nz/plans-projects-policies-reports-bylaws/our-plans-strategies/auckland-plan/about-the-auckland-plan/Pages/aucklands-asian-population.aspx (accessed on 19 November 2021).
- Ma’u, E.; Cullum, S.; Yates, S.; Te Ao, B.; Cheung, G.; Burholt, V.; Dudley, M.; Krishnamurthi, R.; Kerse, N. Dementia Economic Impact Report 2020. Available online: https://cdn.alzheimers.org.nz/wp-content/uploads/2021/09/Dementia-Economic-Impact-Report-2020.pdf (accessed on 19 November 2021).
- Zamawe, F.C. The implication of using NVivo software in qualitative data analysis: Evidence-based reflections. Malawi Med. J. 2015, 27, 13–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terry, G.; Hayfield, N.; Clarke, V.; Braun, V. Thematic analysis. In The SAGE Handbook of Qualitative Research in Psychology; Willig, C., Stainton Rogers, W., Eds.; SAGE: London, UK, 2017; pp. 17–37. [Google Scholar]
- Hossain, M.; Crossland, J.; Stores, R.; Dewey, A.; Hakak, Y. Awareness and understanding of dementia in South Asians: A synthesis of qualitative evidence. Dementia 2020, 19, 1441–1473. [Google Scholar] [CrossRef]
- Mukadam, N.; Cooper, C.; Basit, B.; Livingston, G. Why do ethnic elders present later to UK dementia services? A qualitative study. Int. Psychogeriatr. 2011, 23, 1070–1077. [Google Scholar] [CrossRef]
- Giebel, C.M.; Worden, A.; Challis, D.; Jolley, D.; Bhui, K.S.; Lambat, A.; Kampanellou, E.; Purandare, N. Age, memory loss and perceptions of dementia in South Asian ethnic minorities. Aging Ment. Health 2019, 23, 173–182. [Google Scholar] [CrossRef]
- La Fontaine, J.; Ahuja, J.; Bradbury, N.M.; Phillips, S.; Oyebode, J.R. Understanding dementia amongst people in minority ethnic and cultural groups. J. Adv. Nurs. 2007, 60, 605–614. [Google Scholar] [CrossRef]
- Johnston, K.; Preston, R.; Strivens, E.; Qaloewai, S.; Larkins, S. Understandings of dementia in low and middle income countries and amongst indigenous peoples: A systematic review and qualitative meta-synthesis. Aging Ment. Health 2020, 24, 1183–1195. [Google Scholar] [CrossRef]
- Brijnath, B. Alzheimer’s and the Indian appetite. Med. Anthropol. 2011, 30, 610–628. [Google Scholar] [CrossRef]
- Patel, V.; Prince, M. Ageing and mental health in a developing country: Who cares? Qualitative studies from Goa, India. Psychol. Med. 2001, 31, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Cahill, S.; Pierce, M.; Werner, P.; Darley, A.; Bobersky, A. A systematic review of the public’s knowledge and understanding of Alzheimer’s disease and dementia. Alzheimer Dis. Assoc. Disord. 2015, 29, 255–275. [Google Scholar] [CrossRef]
- Tiwari, S.C.; Pandey, N.M. The Indian concepts of lifestyle and mental health in old age. Indian J. Psychiatry 2013, 55, S288–S292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, T.R.; Nielsen, D.S.; Waldemar, G. Barriers in access to dementia care in minority ethnic groups in Denmark: A qualitative study. Aging Ment. Health 2021, 25, 1424–1432. [Google Scholar] [CrossRef] [PubMed]
- Parveen, S.; Peltier, C.; Oyebode, J.R. Perceptions of dementia and use of services in minority ethnic communities: A scoping exercise. Health Soc. Care Community 2017, 25, 734–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunn, F.; Goodman, C.; Sworn, K.; Rait, G.; Brayne, C.; Robinson, L.; McNeilly, E.; Iliffe, S. Psychosocial factors that shape patient and carer experiences of dementia diagnosis and treatment: A systematic review of qualitative studies. PLoS Med. 2012, 9, e1001331. [Google Scholar] [CrossRef] [Green Version]
- Bowes, A.; Wilkinson, H. We didn’t know it would get that bad’: South Asian experiences of dementia and the service response. Health Soc. Care Community 2003, 11, 387–396. [Google Scholar] [CrossRef]
- Hossain, M.Z.; Khan, H.T.A. Dementia in the Bangladeshi diaspora in England: A qualitative study of the myths and stigmas about dementia. J. Eval. Clin. Pract. 2019, 25, 769–778. [Google Scholar] [CrossRef]
- Nguyen, T.; Li, X. Understanding public-stigma and self-stigma in the context of dementia: A systematic review of the global literature. Dementia 2020, 19, 148–181. [Google Scholar] [CrossRef]
- Herat-Gunaratne, R.; Cooper, C.; Mukadam, N.; Rapaport, P.; Leverton, M.; Higgs, P.; Samus, Q.; Burton, A. “In the Bengali vocabulary, there is no such word as care home”: Caring experiences of UK Bangladeshi and Indian family carers of people living with dementia at home. Gerontologist 2020, 60, 331–339. [Google Scholar] [CrossRef]
- Emmatty, L.M.; Bhatti, R.S.; Mukalel, M.T. The experience of burden in India. Dementia 2016, 5, 223–232. [Google Scholar] [CrossRef]
- Shaji, K.S.; Smitha, K.; Lal, K.P.; Prince, M.J. Caregivers of people with Alzheimer’s disease: A qualitative study from the Indian 10/66 Dementia Research Network. Int. J. Geriatr. Psychiatry 2003, 18, 1–6. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, E.; Lamb-Yorski, R.; Thompson, A.; Grootveld, C. This is Our Story: A Qualitative Research Report on Living with Dementia. Available online: https://cdn.alzheimers.org.nz/wp-content/uploads/2021/05/Report-This-is-our-story-1.pdf (accessed on 17 November 2021).
- Alzheimers NZ; NZ Dementia Cooperative; Dementia New Zealand. Improving Dementia Services in New Zealand—Dementia Action Plan 2020 to 2025. Available online: https://dementia.nz/wp-content/uploads/2020/06/New-Zealand-Dementia-Action-Plan.pdf (accessed on 19 November 2021).

| Parameters | Person Living with Dementia (n = 5) | Caregivers (n = 10) |
|---|---|---|
| Age, median (range) | 74 (65–77) | 61 (41–81) |
| Female, n (%) | 1 (20%) | 6 (60%) |
| Marital status, n (%) | ||
| Married | 4 (80%) | 9 (90%) |
| Widowed | 1 (20%) | - |
| Divorced | - | 1 (10%) |
| Birthplace, n (%) | ||
| India | 2 (40%) | 7 (70%) |
| Fiji | 3 (60%) | 3 (30%) |
| Number of years living in NZ, median (range) | 11 (10–25) | 15 (3–25) |
| Preferred language, n (%) | ||
| Hindi | 2 (40%) | 5 (50%) |
| Fiji Hindi | 3 (60%) | 3 (30%) |
| English | - | 2 (20%) |
| Caregivers (C) | Characteristics and Relationship to Caregiver |
|---|---|
| C1 | Indian, female, living with son’s family, husband had moderate dementia (P1) |
| C2 | Indian, male, living with his family, mother had severe dementia |
| C3 | Indian, female, living with her son’s family, husband had severe dementia |
| C4 | Indian, female, living with her family, mother had severe dementia |
| C5 | Indian, female, living with her son’s family, husband had mild dementia (P5) |
| C6 | Indian, female, living with daughter’s family, husband had severe dementia |
| C7 | Indian, male, living alone, mother had severe dementia |
| C8 | Fiji Indian, female, living with her family, husband had mild dementia (P8) |
| C9 | Fiji Indian, male, living with his family, father had mild dementia (P9) |
| C10 | Fiji Indian, male, living with his family, wife had mild dementia (P10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krishnamurthi, R.V.; Dahiya, E.S.; Bala, R.; Cheung, G.; Yates, S.; Cullum, S. Lived Experience of Dementia in the New Zealand Indian Community: A Qualitative Study with Family Care Givers and People Living with Dementia. Int. J. Environ. Res. Public Health 2022, 19, 1432. https://doi.org/10.3390/ijerph19031432
Krishnamurthi RV, Dahiya ES, Bala R, Cheung G, Yates S, Cullum S. Lived Experience of Dementia in the New Zealand Indian Community: A Qualitative Study with Family Care Givers and People Living with Dementia. International Journal of Environmental Research and Public Health. 2022; 19(3):1432. https://doi.org/10.3390/ijerph19031432
Chicago/Turabian StyleKrishnamurthi, Rita V., Ekta Singh Dahiya, Reshmi Bala, Gary Cheung, Susan Yates, and Sarah Cullum. 2022. "Lived Experience of Dementia in the New Zealand Indian Community: A Qualitative Study with Family Care Givers and People Living with Dementia" International Journal of Environmental Research and Public Health 19, no. 3: 1432. https://doi.org/10.3390/ijerph19031432
APA StyleKrishnamurthi, R. V., Dahiya, E. S., Bala, R., Cheung, G., Yates, S., & Cullum, S. (2022). Lived Experience of Dementia in the New Zealand Indian Community: A Qualitative Study with Family Care Givers and People Living with Dementia. International Journal of Environmental Research and Public Health, 19(3), 1432. https://doi.org/10.3390/ijerph19031432