
Dental Implants in People with Osteogenesis Imperfecta: A Systematic Review

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Selection Process and Data Extraction
- Patient characteristics:
- ○
- Age of patient;
- ○
- Sex of patient;
- ○
- Subtype of OI;
- ○
- If the patient was taking bisphosphonates;
- ○
- If the patient was smoking.
- Surgical procedures:
- ○
- If bone augmentation was performed (ridge augmentation or sinus floor elevation);
- ○
- If antibiotics were administered during surgery;
- ○
- One- or two-phase surgical procedure.
- Implant characteristics:
- ○
- Number of implants;
- ○
- Implant position;
- ○
- Type of implant;
- ○
- Bone- or tissue-level implant;
- ○
- Months between placement and loading of implants;
- ○
- Type of suprastructure on abutment.
- Outcome and follow-up
- ○
- Time of follow-up;
- ○
- Probing depth;
- ○
- Radiological bone loss (intraoral single-tooth radiograph or panoramic radiography);
- ○
- If the implant was lost (with reason of failure);
- ○
- Time between surgery and failure.
2.5. Quality Assessment
3. Results
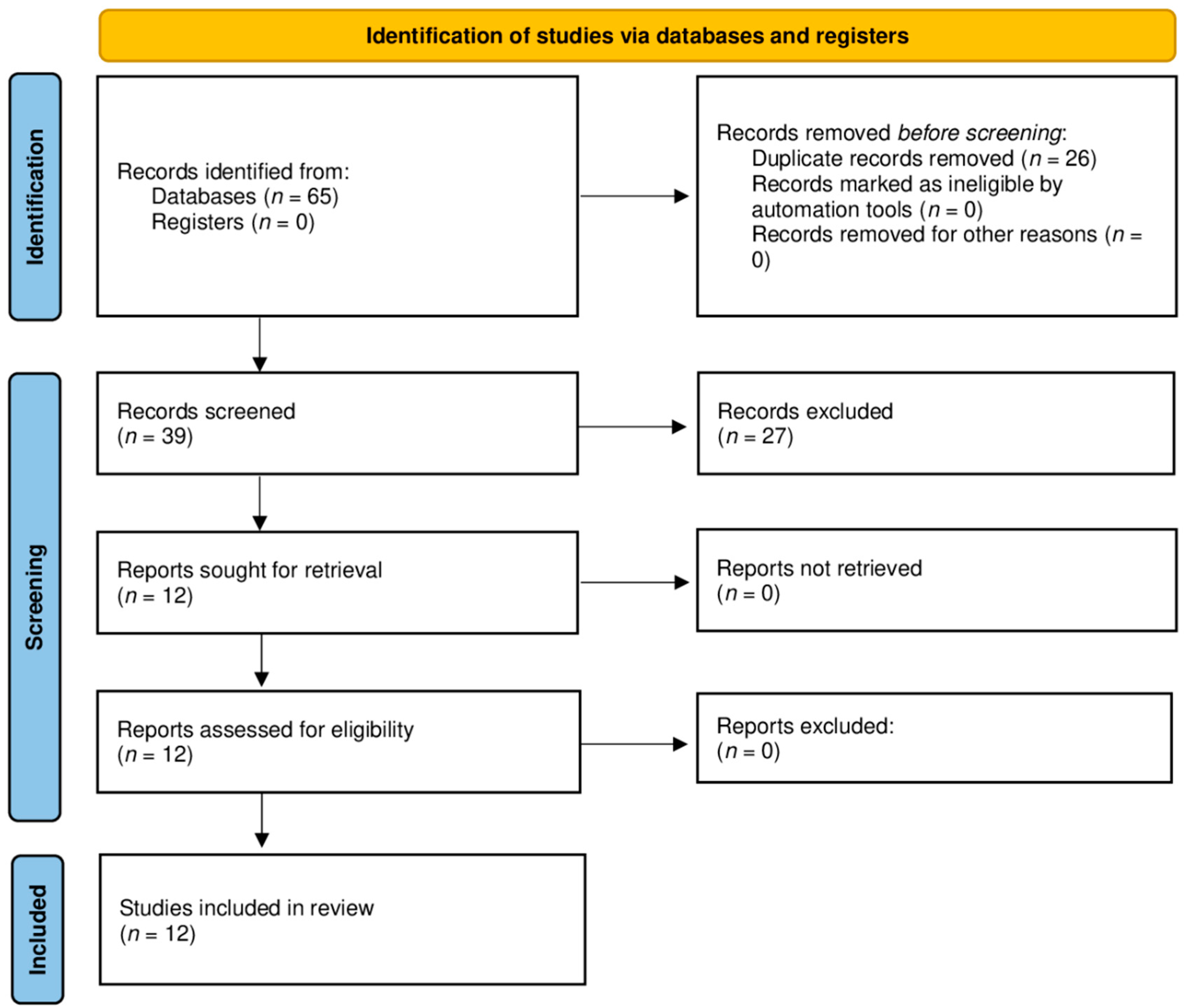
3.1. Literature Search
3.2. Study Characteristics
3.3. Quality Assessment
3.4. Description of the Included Studies and Patients
3.5. Bisphosphonates
3.6. Bone Augmentation
3.6.1. Ridge Augmentation
3.6.2. Sinus Floor Elevation
3.7. Antibiotics
3.8. Implant Characteristics
3.9. Implant Placement and Prosthodontic Rehabilitation
3.10. Outcome and Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herdea, A.; Ulici, A.; Qirjako, D.; Toma, A.; Derihaci, R.P.; Lungu, C.N.; Charkaoui, A. Evaluating the Functional Outcomes and the Quality of Life for Pediatric Patients with Osteogenesis Imperfecta after Fracture Treatment with Intramedullary Rodding. Children 2021, 8, 1066. [Google Scholar] [CrossRef] [PubMed]
- Forlino, A.; Marini, J.C. Osteogenesis Imperfecta. Lancet Lond. Engl. 2016, 387, 1657–1671. [Google Scholar] [CrossRef]
- Sillence, D.O.; Senn, A.; Danks, D.M. Genetic Heterogeneity in Osteogenesis Imperfecta. J. Med. Genet. 1979, 16, 101–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marom, R.; Rabenhorst, B.M.; Morello, R. Osteogenesis Imperfecta: An Update on Clinical Features and Therapies. Eur. J. Endocrinol. 2020, 183, R95–R106. [Google Scholar] [CrossRef]
- Weaver, J.S.; Revels, J.W.; Elifritz, J.M.; Whitlow, B.; Retrouvey, M.; Wang, S.S. Clinical Manifestations and Medical Imaging of Osteogenesis Imperfecta: Fetal Through Adulthood. Acta Med. Acad. 2021, 50, 277–291. [Google Scholar] [CrossRef]
- Dwan, K.; Phillipi, C.A.; Steiner, R.D.; Basel, D. Bisphosphonate Therapy for Osteogenesis Imperfecta. Cochrane Database Syst. Rev. 2016, 10, CD005088. [Google Scholar] [CrossRef]
- Hanisch, M.; Maus, M.; Kleinheinz, J. Implant-Prosthetic Restoration of a Patient with Osteogenesis Imperfecta: A Case Report. Int. J. Environ. Res. Public Health 2021, 18, 4169. [Google Scholar] [CrossRef]
- Caicedo-Rubio, M.; Ferrés-Amat, E.; Ferrés-Padró, E. Implant-Supported Fixed Prostheses in a Patient with Osteogenesis Imperfecta: A 4-Year Follow-Up. J. Clin. Exp. Dent. 2017, 9, e1482–e1486. [Google Scholar] [CrossRef]
- Myint, M.; Støvne, S.A.; Sæves, R.; Bjørnland, T.; Jensen, J.L. Dental Implants in Individuals with Osteogenesis Imperfecta: A 6-Year Follow-up Study. Oral Surg. 2019, 12, 272–277. [Google Scholar] [CrossRef]
- Nguyen, H.T.T.; Vu, D.C.; Nguyen, D.M.; Dang, Q.D.; Tran, V.K.; Le, H.; Tong, S.M. Dentinogenesis Imperfecta and Caries in Osteogenesis Imperfecta among Vietnamese Children. Dent. J. 2021, 9, 49. [Google Scholar] [CrossRef]
- Saeves, R.; Wekre, L.L.; Ambjørnsen, E.; Axelsson, S.; Nordgarden, H.; Storhaug, K. Oral Findings in Adults with Osteogenesis Imperfecta. Spec. Care Dentist. 2009, 29, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Malmgren, B.; Norgren, S. Dental Aberrations in Children and Adolescents with Osteogenesis Imperfecta. Acta Odontol. Scand. 2002, 60, 65–71. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, A.C.; Marini, J.C. Evaluation of Oral Problems in an Osteogenesis Imperfecta Population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1999, 87, 189–196. [Google Scholar] [CrossRef]
- Hartsfield, J.K.; Hohlt, W.F.; Roberts, W.E. Orthodontic Treatment and Orthognathic Surgery for Patients with Osteogenesis Imperfecta. Semin. Orthod. 2006, 12, 254–271. [Google Scholar] [CrossRef]
- Morton, D.; Gallucci, G.; Lin, W.-S.; Pjetursson, B.; Polido, W.; Roehling, S.; Sailer, I.; Aghaloo, T.; Albera, H.; Bohner, L.; et al. Group 2 ITI Consensus Report: Prosthodontics and Implant Dentistry. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 215–223. [Google Scholar] [CrossRef] [PubMed]
- Wannfors, K.; Johansson, C.; Donath, K. Augmentation of the Mandible via a “Tent-Pole” Procedure and Implant Treatment in a Patient with Type III Osteogenesis Imperfecta: Clinical and Histologic Considerations. Int. J. Oral Maxillofac. Implant. 2009, 24, 1144–1148. [Google Scholar]
- Lee, C.Y.; Ertel, S.K. Bone Graft Augmentation and Dental Implant Treatment in a Patient with Osteogenesis Imperfecta: Review of the Literature with a Case Report. Implant Dent. 2003, 12, 291–295. [Google Scholar] [CrossRef]
- Friberg, B. Brånemark System Implants and Rare Disorders: A Report of Six Cases. Int. J. Periodontics Restor. Dent. 2013, 33, 139–148. [Google Scholar] [CrossRef]
- Jensen, J.L.; Brox, H.T.; Storhaug, K.; Ambjørnsen, E.; Støvne, S.A.; Bjørnland, T. Dental Implants in Patients with Osteogenesis Imperfecta: A Retrospective and Prospective Study with Review of the Literature. Oral Surg. 2011, 4, 105–114. [Google Scholar] [CrossRef]
- Binger, T.; Rücker, M.; Spitzer, W.J. Dentofacial Rehabilitation by Osteodistraction, Augmentation and Implantation despite Osteogenesis Imperfecta. Int. J. Oral Maxillofac. Surg. 2006, 35, 559–562. [Google Scholar] [CrossRef]
- Prabhu, S.; Fortier, K.; May, M.; Reebye, U. Implant Therapy for a Patient with Osteogenesis Imperfecta Type I: Review of Literature with a Case Report. Int. J. Implant Dent. 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Payne, M.A.; Postlethwaite, K.R.; Smith, D.G.; Nohl, F.S. Implant-Supported Rehabilitation of an Edentate Patient with Osteogenesis Imperfecta: A Case Report. Int. J. Oral Maxillofac. Implant. 2008, 23, 947–952. [Google Scholar]
- Zola, M.B. Staged Sinus Augmentation and Implant Placement in a Patient with Osteogenesis Imperfecta. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2000, 58, 443–447. [Google Scholar] [CrossRef]
- Prabhu, N.; Duckmanton, N.; Stevenson, A.R.; Cameron, A. The Placement of Osseointegrated Dental Implants in a Patient with Type IV B Osteogenesis Imperfecta: A 9-Year Follow-Up. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 349–354. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; The PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological Quality and Synthesis of Case Series and Case Reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Najirad, M.; Madathil, S.A.; Rauch, F.; Sutton, V.R.; Lee, B.; Retrouvey, J.-M.; Members of the Brittle Bone Diseases Consortium; Esfandiari, S. Malocclusion Traits and Oral Health-Related Quality of Life in Children with Osteogenesis Imperfecta: A Cross-Sectional Study. J. Am. Dent. Assoc. 2020, 151, 480–490.e2. [Google Scholar] [CrossRef]
- Stenvik, A.; Larheim, T.A.; Storhaug, K. Incisor and Jaw Relationship in 27 Persons with Osteogenesis Imperfecta. Eur. J. Oral Sci. 1985, 93, 56–60. [Google Scholar] [CrossRef]
- Lund, A.M.; Jensen, B.L.; Nielsen, L.A.; Skovby, F. Dental Manifestations of Osteogenesis Imperfecta and Abnormalities of Collagen I Metabolism. J. Craniofac. Genet. Dev. Biol. 1998, 18, 30–37. [Google Scholar] [PubMed]
- Cachia Mintoff, J.M.; Riddington, M.; Parekh, S. Oral Health-Related Quality of Life in Children with Osteogenesis Imperfecta. Eur. Arch. Paediatr. Dent. 2021. [Google Scholar] [CrossRef] [PubMed]
- Members of the BBD; Najirad, M.; Ma, M.S.; Rauch, F.; Sutton, V.R.; Lee, B.; Retrouvey, J.-M.; Esfandiari, S. Oral Health-Related Quality of Life in Children and Adolescents with Osteogenesis Imperfecta: Cross-Sectional Study. Orphanet J. Rare Dis. 2018, 13, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjørup, H.; Beck-Nielsen, S.S.; Hald, J.D.; Haubek, D. Oral Health-related Quality of Life in X-linked Hypophosphataemia and Osteogenesis Imperfecta. J. Oral Rehabil. 2021, 48, 160–168. [Google Scholar] [CrossRef]
- Nakamura, T.; Igarashi, H.; Ito, T.; Jensen, R.T. Important of Case-Reports/Series, in Rare Diseases: Using Neuroendocrine Tumors as an Example. World J. Clin. Cases 2014, 2, 608–613. [Google Scholar] [CrossRef]
- Whicher, D.; Philbin, S.; Aronson, N. An Overview of the Impact of Rare Disease Characteristics on Research Methodology. Orphanet J. Rare Dis. 2018, 13, 14. [Google Scholar] [CrossRef]
- Ruck, J.; Dahan-Oliel, N.; Montpetit, K.; Rauch, F.; Fassier, F. Fassier–Duval Femoral Rodding in Children with Osteogenesis Imperfecta Receiving Bisphosphonates: Functional Outcomes at One Year. J. Child. Orthop. 2011, 5, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Bishop, N.; Adami, S.; Ahmed, S.F.; Antón, J.; Arundel, P.; Burren, C.P.; Devogelaer, J.-P.; Hangartner, T.; Hosszú, E.; Lane, J.M.; et al. Risedronate in Children with Osteogenesis Imperfecta: A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2013, 382, 1424–1432. [Google Scholar] [CrossRef]
- Polymeri, A.A.; Kodovazenitis, G.J.; Polymeris, A.D.; Komboli, M. Bisphosphonates: Clinical Applications and Adverse Events in Dentistry. Oral Health Prev. Dent. 2015, 13, 289–299. [Google Scholar] [CrossRef]
- Lotwala, R.B.; Greenlee, G.M.; Ott, S.M.; Hall, S.H.; Huang, G.J. Bisphosphonates as a Risk Factor for Adverse Orthodontic Outcomes: A Retrospective Cohort Study. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 625–634.e3. [Google Scholar] [CrossRef]
- Tyrovola, J.B.; Spyropoulos, M.N. Effects of Drugs and Systemic Factors on Orthodontic Treatment. Quintessence Int. Berl. Ger. 1985 2001, 32, 365–371. [Google Scholar]
- Friedrich, R.E.; Scheuer, H.A.; Höltje, W. The Effect of Bisphosphonate Medication on Orthodontics and Orthognathic Surgery in Patients with Osteogenesis Imperfecta. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2019, 8, Doc06. [Google Scholar] [CrossRef] [PubMed]
- Mendes, V.; dos Santos, G.; Calasans-Maia, M.; Granjeiro, J.; Moraschini, V. Impact of Bisphosphonate Therapy on Dental Implant Outcomes: An Overview of Systematic Review Evidence. Int. J. Oral Maxillofac. Surg. 2019, 48, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; Luzzi, V.; Ierardo, G.; Raimondo, E.; Boccellino, M.; Ferati, K.; Bexheti-Ferati, A.; Inchingolo, F.; Di Domenico, M.; Serpico, R.; et al. Bisphosphonate-Related Osteonecrosis of the Jaws and Dental Surgery Procedures in Children and Young People with Osteogenesis Imperfecta: A Systematic Review. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 556–562. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, C.A.; Lemos, C.A.A.; Santiago-Júnior, J.F.; Faverani, L.P.; Pellizzer, E.P. Bone Augmentation Using Autogenous Bone versus Biomaterial in the Posterior Region of Atrophic Mandibles: A Systematic Review and Meta-Analysis. J. Dent. 2018, 76, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starch-Jensen, T.; Aludden, H.; Hallman, M.; Dahlin, C.; Christensen, A.-E.; Mordenfeld, A. A Systematic Review and Meta-Analysis of Long-Term Studies (Five or More Years) Assessing Maxillary Sinus Floor Augmentation. Int. J. Oral Maxillofac. Surg. 2018, 47, 103–116. [Google Scholar] [CrossRef]
- Raghoebar, G.M.; Onclin, P.; Boven, G.C.; Vissink, A.; Meijer, H.J.A. Long-Term Effectiveness of Maxillary Sinus Floor Augmentation: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 307–318. [Google Scholar] [CrossRef] [Green Version]
- Ye, M.; Liu, W.; Cheng, S.; Yan, L. Outcomes of Implants Placed after Osteotome Sinus Floor Elevation without Bone Grafts: A Systematic Review and Meta-Analysis of Single-Arm Studies. Int. J. Implant Dent. 2021, 7, 72. [Google Scholar] [CrossRef]
- Park, J.; Tennant, M.; Walsh, L.; Kruger, E. Is There a Consensus on Antibiotic Usage for Dental Implant Placement in Healthy Patients? Aust. Dent. J. 2018, 63, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.S.; Abdelhay, N.; Levin, L.; Walters, J.D.; Gibson, M.P. Antibiotic Prophylaxis for Implant Placement: A Systematic Review of Effects on Reduction of Implant Failure. Br. Dent. J. 2020, 228, 943–951. [Google Scholar] [CrossRef]
- Ireland, R.S.; Palmer, N.O.; Lindenmeyer, A.; Mills, N. An Investigation of Antibiotic Prophylaxis in Implant Practice in the UK. Br. Dent. J. 2012, 213, E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, A.B.; Larson, E.L. Antibiotic Prophylaxis and Postoperative Complications after Tooth Extraction and Implant Placement: A Review of the Literature. J. Dent. 2007, 35, 881–888. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, H.; Raes, S.; Ostman, P.-O.; Cosyn, J. Immediate Loading in Partially and Completely Edentulous Jaws: A Review of the Literature with Clinical Guidelines. Periodontol. 2000 2014, 66, 153–187. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.O.; Hamilton, A.; Zhou, W.; Buser, D.; Chen, S. Implant Placement and Loading Protocols in Partially Edentulous Patients: A Systematic Review. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 106–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Zhou, W.; Wu, Y.; Wang, F. Clinical Outcomes of Immediate Implant Loading with Fixed Prostheses in Edentulous Maxillae: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2021, 36, 503–519. [Google Scholar] [CrossRef]
- Beschnidt, S.M.; Cacaci, C.; Dedeoglu, K.; Hildebrand, D.; Hulla, H.; Iglhaut, G.; Krennmair, G.; Schlee, M.; Sipos, P.; Stricker, A.; et al. Implant Success and Survival Rates in Daily Dental Practice: 5-Year Results of a Non-Interventional Study Using CAMLOG SCREW-LINE Implants with or without Platform-Switching Abutments. Int. J. Implant Dent. 2018, 4, 33. [Google Scholar] [CrossRef]


{kind=link}
| Focused Question | |
|---|---|
| PICO model | Can people with osteogenesis imperfecta (P) be successfully treated and prosthetically restored (O) with dental implants (I)? |
| Search query | #1 (osteogenesis imperfecta) OR (brittle bone disease) |
| #2 (dental implants) OR (guided tissue regeneration) OR (alveolar bone grafting) | |
| #1 AND #2 | |
| Study design | All clinical study designs |
| Authors (Year) | Type of Study 1 | No. of Subjects | No. of Implants |
|---|---|---|---|
| Binger et al. (2006) | CS | 1 | 5 |
| Caicedo-Rubio et al. (2017) | CS | 1 | 3 |
| Friberg et al. (2013) | CS | 1 | 6 |
| Hanisch et al. (2021) | CS | 1 | 2 |
| Jensen et al. (2011) (Myint et al. 2019) | R/P | 13 | 46 |
| Lee et al. (2003) | CS | 1 | 2 |
| Payne et al. (2008) | CS | 1 | 11 |
| Prabhu et al. (2007) | CS | 1 | 11 |
| Prabhu et al. (2018) | CS | 1 | 10 |
| Wannfors et al. (2009) | CS | 1 | 4 |
| Zola et al. (2000) | CS | 1 | 16 |
| Study | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 | Question 8 | Overall Judgement |
|---|---|---|---|---|---|---|---|
| Binger et al. (2006) | Yes | Yes | Yes | No | Yes | Yes | Good quality |
| Caicedo-Rubio et al. (2017) | Yes | Yes | Yes | Yes | Yes | Yes | Good quality |
| Friberg et al. (2013) | Yes | Partially | Partially | Yes | Partially | Partially | Medium quality |
| Hanisch et al. (2021) | Yes | Yes | Yes | Yes | Partially | Yes | Good quality |
| Jensen et al. (2011) | Yes | Yes | Yes | Partially | Yes | Yes | Good quality |
| Lee et al. (2003) | Yes | Yes | Partially | No | Partially | Yes | Medium quality |
| Myint et al. (2019) | Yes | Yes | Yes | Yes | Yes | Yes | Good quality |
| Payne et al. (2008) | Yes | Yes | Yes | No | Partially | Yes | Good quality |
| Prahbu et al. (2007) | Yes | Yes | Yes | No | Yes | Yes | Good quality |
| Prahbu et al. (2018) | Yes | Yes | Partially | No | Partially | Yes | Good quality |
| Wannfors et al. (2009) | Yes | Yes | Partially | No | Partially | Yes | Good quality |
| Zola et al. (2000) | Yes | Yes | No | No | Partially | Yes | Medium quality |
| ID 1 | Sex 2 | Age | Subtype of OI 3 | Smoker | Bisphosphonates 4 | Ridge Augmentation 4 | Antibiotics during Surgery 4 | Sinus Floor Elevation 4 | Number of Implants | Implant Characteristics | Two-Phase/One-Phase 5 | Abutment Type 6 | Follow-Up Time 7 | Implant Survival |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 [20] | F | 32 | NA | NA | NA | Yes | NA | Yes | 5 | Straumann standard implants | Tp | r+od | 48 | 5/5 |
| 2 [8] | M | 61 | IV | Yes | Yes | NA | Yes | No | 3 | MIS C1 3.75 × 10 /3.75 × 11.5 | Tp | c | 48 | 3/3 |
| 3 [18] | F | 51 | NA | NA | NA | NA | Yes | Yes | 6 | Regular-platform TiUnite Brånemark System Implants | Tp | r+od | 48 | 6/6 |
| 4 [7] | F | 64 | I | NA | Yes | No | Yes | No | 2 | Straumann Standard Plus SLActive 3.3 mm × 10 mm | Tp | l+od | 12 | 2/2 |
| 5 [19] | F | 73 | I | No | NA | NA | NA | NA | 1 | Nobel | Na | b | >120 | 1/1 |
| 6 [19] | M | 52 | Ib | Yes | NA | NA | NA | NA | 5 | AstraTech Tioblast 3.5 × 15/3.5 × 17 | Tp | b | 135 | 5/5 |
| 7 [19] | M | 69 | I | Yes | NA | NA | NA | NA | 5 | AstraTech Tioblast 4.0 × 15/3.5 × 11 | Tp | b | 60 | 5/5 |
| 8 [19] | M | 49 | IV | No | NA | NA | NA | NA | 1 | AstraTech Tioblast 4.5 × 13 | Na | c | 79 | 1/1 |
| 9 [19] | F | 58 | IV | Yes | NA | NA | NA | NA | 6 | AstraTech Tioblast 3.5 × 13/4.0 × 13/3.5 × 15 | Tp | c+od | 83 | 6/6 |
| 10 [19] | F | 52 | III | Yes | NA | NA | NA | NA | 7 | AstraTech Osseospeed 3.5 × 9/3.5 × 11 NobelDirect 3.0 × 15/3.0 × 10 | Mixed | c+od | 29–57 | 5/7 |
| 11 [19] | M | 75 | I | No | NA | NA | NA | NA | 7 | Straumann 4.1 × 12 AstraTech Osseospeed 3.5 × 13 | Mixed | c+od | 11–22 | 7/7 |
| 12 [19] | F | 65 | Ib | No | NA | NA | NA | NA | 2 | AstraTech Osseospeed 3.5 × 13/4.0 × 13 | Tp | c | 23 | 2/2 |
| 13 [9,19] | M | 58 | Ib | Yes | NA | NA | NA | NA | 5 | AstraTech Osseospeed 4.0 × 13 | Tp | c | 103–109 | 5/5 |
| 14 [19] | M | 20 | III | No | NA | NA | NA | NA | 1 | Biomet 3i tapered 3.25 × 11 | Op | c | 22 | 1/1 |
| 15 [9,19] | M | 39 | Ib | No | NA | NA | NA | NA | 3 | AstraTech Osseospeed 3.5 × 13 Biomet 3i tapered 3.25 × 11 | Tp | c | 104–106 | 3/3 |
| 16 [9,19] | F | 48 | I | No | NA | NA | NA | NA | 2 | AstraTech Osseospeed 4.5 × 11/5.0 × 11 | Tp | c | 76–91 | 1/2 |
| 17 [9,19] | F | 56 | IV | Yes | Yes | NA | NA | NA | 1 | Straumann 4.1 × 8 | Tp | c | 94 | 1/1 |
| 18 [17] | F | 43 | III | NA | NA | Yes | NA | No | 2 | Paragon Screw-vent internal hexed implants | Tp | b | 24 | 2/2 |
| 19 [22] | F | 34 | IV | NA | NA | Some implants | Yes | Some implants | 11 | Brånemark System Mk III Ti-Unite implants 3.75 × 15/3.75 × 10/3.75 × 11.5/4 × 15 | Tp | r+od | 24 | 11/11 |
| 20 [24] | M | 34 | IVb | NA | NA | No | NA | No | 11 | Brånemark titanium bone-tapped implants 13/15 | Tp | r+od | 108 | 10/11 |
| 21 [21] | M | 53 | I | NA | No | Some implants | NA | NA | 10 | NobelActive Implant 3.5 × 13/3.5 × 10/4.3 × 10/4.3 × 11/4.3 × 13/5 × 10 | Op | b/c | 13–40 | 10/10 |
| 22 [16] | F | 30 | III | NA | Yes | Yes | NA | No | 4 | Astra Tech OsseoSpeed 3.5 × 11 | Tp | b | 36 | 4/4 |
| 23 [23] | M | 20 | NA | NA | NA | Some implants | Yes | Some implants | 16 | 3.5 × 10/3.5 × 13/4.0 × 10/4.0 × 13/4.0 × 15 | Tp | b | 65–86 | 13/16 |
| Implant Region | No. Implants (%) | Implant Survival (%) | Implant Failure (%) |
|---|---|---|---|
| 17–14 | 18 (15.5) | 16 (88.9) | 2 (1.1) |
| 13–23 | 26 (22.4) | 26 (100) | 0 (0) |
| 24–28 | 22 (18.9) | 21 (95.5) | 1 (4.5) |
| 38–34 | 17 (14.7) | 15 (88.2) | 2 (11.8) |
| 33–43 | 19 (16.4) | 18 (94.7) | 1 (5.3) |
| 44–48 | 14 (12.1) | 13 (92.9) | 1 (7.1) |
| Total | 116 (100) | 109 (94.0) | 7 (6.0) |
| Mean | SD | Range | |
|---|---|---|---|
| Implants per patient | 5.0 | ±3.8 | 1–16 |
| Time between implantation and loading (months) | 8.9 | ±6.3 | 0–40 |
| Follow-up time | 59.1 | ±36.1 | 11–135 |
| Radiological bone loss (mm) | 0.8 | ±1.3 | 0–7 |
| Time between surgery and failure of implants (months) | 39.1 | ±29.4 | 3–78 |
| No. of Subjects | No. of Implants | No. of Failed Implants | Survival Rate | |
|---|---|---|---|---|
| Subtype | ||||
| I | 10 | 42 | 1 * | 97.% |
| III | 4 | 14 | 2 | 85.7% |
| IV | 6 | 33 | 1 | 97.0% |
| NA | 3 | 17 | 3 * | 88.9% |
| Bone Augmentation | ||||
| Ridge Augmentation | ||||
| Autogenous bone used | 5 | 22 | 1 | 95.5% |
| Allograft used | 1 | 8 | 0 | 100% |
| No augmentation | 2 | 26 | 2 | 92.3% |
| NA | 15 | 60 | 4 ** | 93.4% |
| Sinus Floor Elevation | ||||
| Sinus floor elevation performed | 4 | 19 | 1 | 94.7% |
| Not performed | 9 | 55 | 6 ** | 89.1% |
| NA (or information missing on some implants) | 10 | 42 | 0 | 100% |
| Surgical Procedure | ||||
| Immediately loaded | 4 | 14 | 0 | 100% |
| Two-stage procedure | 18 | 100 | 7 ** | 93.0% |
| NA | 2 | 2 | 0 | 100% |
| Abutment | ||||
| Crown | 10 | 24 | 1 * | 95.8% |
| Bridge | 7 | 31 | 2 * | 93.5% |
| Crown + Overdenture | 3 | 17 | 0 | 100% |
| Locator + Overdenture | 1 | 2 | 0 | 100% |
| Ridge + Overdenture | 4 | 32 | 0 | 100% |
| NA | 1 | 7 | 1 | 85.7% |
| Failed before loading | 2 | 3 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oelerich, O.; Kleinheinz, J.; Bohner, L.; Wiesmüller, V.; Hanisch, M. Dental Implants in People with Osteogenesis Imperfecta: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 1563. https://doi.org/10.3390/ijerph19031563
Oelerich O, Kleinheinz J, Bohner L, Wiesmüller V, Hanisch M. Dental Implants in People with Osteogenesis Imperfecta: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(3):1563. https://doi.org/10.3390/ijerph19031563
Chicago/Turabian StyleOelerich, Ole, Johannes Kleinheinz, Lauren Bohner, Vera Wiesmüller, and Marcel Hanisch. 2022. "Dental Implants in People with Osteogenesis Imperfecta: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 3: 1563. https://doi.org/10.3390/ijerph19031563
APA StyleOelerich, O., Kleinheinz, J., Bohner, L., Wiesmüller, V., & Hanisch, M. (2022). Dental Implants in People with Osteogenesis Imperfecta: A Systematic Review. International Journal of Environmental Research and Public Health, 19(3), 1563. https://doi.org/10.3390/ijerph19031563