
Perceived Partner’s Self-Control and Social Support Effects on Relationship Satisfaction in Couples Experiencing Infertility or Miscarriage: Dyadic Analyses


Abstract
:1. Introduction
1.1. Infertility and Its Importance for the Functioning of a Couple and the Quality of Their Relationship
1.2. Experiencing a Miscarriage and Its Consequences for the Functioning of the Couple
1.3. Self-Control and Relationship Satisfaction
2. The Purpose of the Study
3. Materials and Methods
3.1. Participants
3.2. Procedures
3.3. Measures
4. Analysis Strategies
5. Results
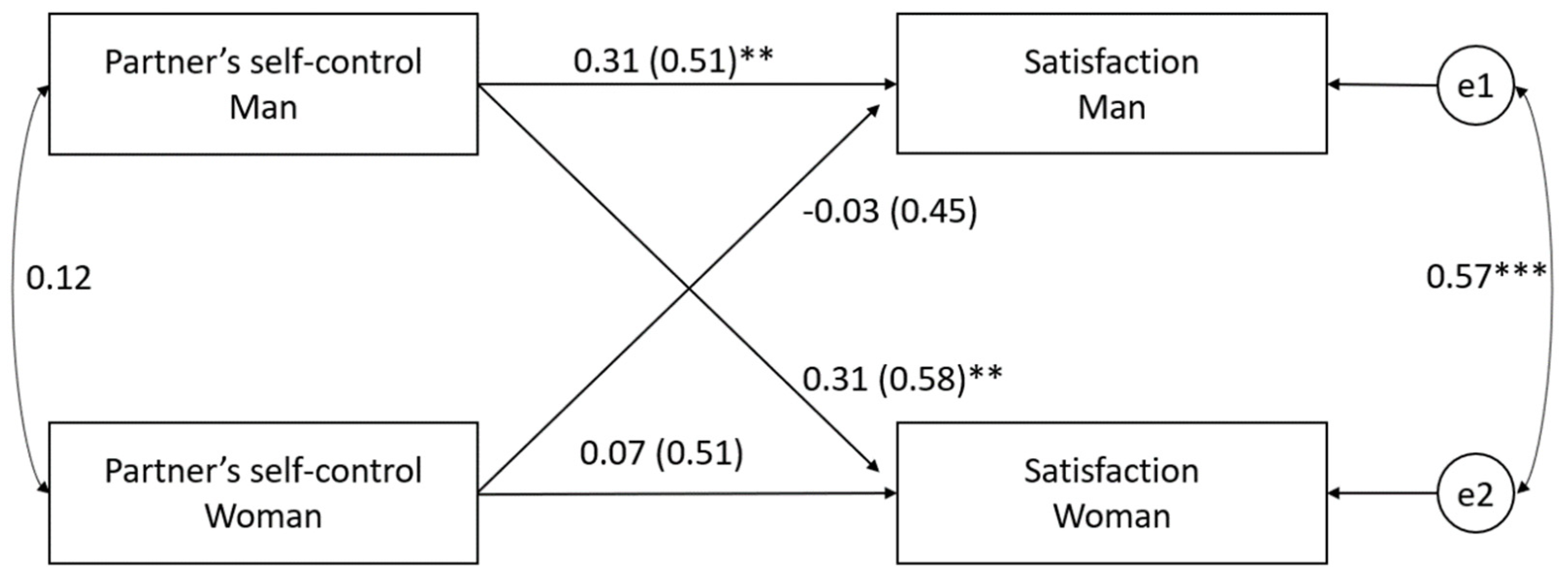
5.1. The Spouses’ Perception of Their Partner’s Self-Control as a Predictor of Marital Satisfaction
5.2. Moderating Effect of Acquiring Social Support on the Relationship between Partner’s Perceived Self-Control and Relationship Satisfaction
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greil, A.L.; McQuillan, J.; Johnson, K.; Slauson-Blevins, K.; Shreffler, K.M. The Hidden Infertile: Infertile Women without Pregnancy Intent in the United States. Fertil. Steril. 2010, 93, 2080–2083. [Google Scholar] [CrossRef] [Green Version]
- Zurlo, M.C.; Cattaneo Della Volta, M.F.; Vallone, F. Predictors of Quality of Life and Psychological Health in Infertile Couples: The Moderating Role of Duration of Infertility. Qual. Life Res. 2018, 27, 945–954. [Google Scholar] [CrossRef]
- Galhardo, A.; Cunha, M.; Pinto-Gouveia, J.; Matos, M. The Mediator Role of Emotion Regulation Processes on Infertility-Related Stress. J. Clin. Psychol. Med. Settings 2013, 20, 497–507. [Google Scholar] [CrossRef] [Green Version]
- Gourounti, K.; Anagnostopoulos, F.; Vaslamatzis, G. Psychosocial Predictors of Infertility Related Stress: A Review. CWHR 2010, 6, 318–331. [Google Scholar] [CrossRef]
- Amini, L.; Ghorbani, B.; Afshar, B. The Comparison of Infertility Stress and Perceived Social Support in Infertile Women and Spouses of Infertile Men. IJN 2020, 32, 80–90. [Google Scholar] [CrossRef]
- Galhardo, A.; Alves, J.; Moura-Ramos, M.; Cunha, M. Infertility-Related Stress and Depressive Symptoms—The Role of Experiential Avoidance: A Cross-Sectional Study. J. Reprod. Infant Psychol. 2020, 38, 139–150. [Google Scholar] [CrossRef]
- Rooney, K.L.; Domar, A.D. The Relationship between Stress and Infertility. Transl. Res. 2018, 20, 7. [Google Scholar]
- Ockhuijsen, H.D.L.; van den Hoogen, A.; Boivin, J.; Macklon, N.S.; de Boer, F. Pregnancy After Miscarriage: Balancing Between Loss of Control and Searching for Control: PREGNANCY AFTER MISCARRIAGE. Res. Nurs. Health 2014, 37, 267–275. [Google Scholar] [CrossRef]
- Thiemann, K.L.; Thiemann, J.M. A Tale of Unseen Suffering: Experience of Recurrent Miscarriage Through Duoethnography. Qual. Inq. 2020, 26, 678–686. [Google Scholar] [CrossRef]
- Robinson, J. Provision of Information and Support to Women Who Have Suffered an Early Miscarriage. Br. J. Midwifery 2014, 22, 175–180. [Google Scholar] [CrossRef]
- DiPietro, J.A.; Novak, M.F.S.X.; Costigan, K.A.; Atella, L.D.; Reusing, S.P. Maternal Psychological Distress During Pregnancy in Relation to Child Development at Age Two. Child Dev. 2006, 77, 573–587. [Google Scholar] [CrossRef]
- Tavoli, Z.; Mohammadi, M.; Tavoli, A.; Moini, A.; Effatpanah, M.; Khedmat, L.; Montazeri, A. Quality of Life and Psychological Distress in Women with Recurrent Miscarriage: A Comparative Study. Health Qual. Life Outcomes 2018, 16, 150. [Google Scholar] [CrossRef] [Green Version]
- Qu, F.; Wu, Y.; Zhu, Y.-H.; Barry, J.; Ding, T.; Baio, G.; Muscat, R.; Todd, B.K.; Wang, F.-F.; Hardiman, P.J. The Association between Psychological Stress and Miscarriage: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 1731. [Google Scholar] [CrossRef] [PubMed]
- Terzioglu, F.; Turk, R.; Yucel, C.; Dilbaz, S.; Cinar, O.; Karahalil, B. The Effect of Anxiety and Depression Scores of Couples Who Underwent Assisted Reproductive Techniques on the Pregnancy Outcomes. Afr. Health Sci. 2016, 16, 441. [Google Scholar] [CrossRef] [Green Version]
- Hutti, M.H. Parents’ Perceptions of the Miscarriage Experience. Death Stud. 1992, 16, 401–415. [Google Scholar] [CrossRef]
- Tunaley, J.R.; Slade, P.; Duncan, S.B. Cognitive Processes in Psychological Adaptation to Miscarriage: A Preliminary Report. Psychol. Health 1993, 8, 369–381. [Google Scholar] [CrossRef]
- Folkman, S. The Oxford Handbook of Stress, Health, and Coping; Oxford University Press: Oxford, UK, 2011; ISBN 0-19-537534-3. [Google Scholar]
- Chen, X.; Liu, Y.; Cheung, W.C.; Zhao, Y.; Huang, J.; Chung, J.P.W.; Wang, C.C.; Li, T.C. Increased Expression of Angiogenic Cytokines in CD56+ Uterine Natural Killer Cells from Women with Recurrent Miscarriage. Cytokine 2018, 110, 272–276. [Google Scholar] [CrossRef]
- Januszewski, A. Test Giessen [Giessen Test]; Katolicki Uniwersytet Lubelski Katedra Psychologii Ogólnej: Lublin, Poland, 1992. [Google Scholar]
- Duckworth, A.L. The Significance of Self-Control. Proc. Natl. Acad. Sci. USA 2011, 108, 2639–2640. [Google Scholar] [CrossRef] [Green Version]
- Rachlin, H. The Science of Self-Control; Harvard University Press: Cambridge, MA, USA, 2000; ISBN 978-0-674-00093-3. [Google Scholar]
- Duckworth, A.L.; Taxer, J.L.; Eskreis-Winkler, L.; Galla, B.M.; Gross, J.J. Self-Control and Academic Achievement. Annu. Rev. Psychol. 2019, 70, 373–399. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual Differences in Two Emotion Regulation Processes: Implications for Affect, Relationships, and Well-Being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Eisenberg, N.; Duckworth, A.L.; Spinrad, T.L.; Valiente, C. Conscientiousness: Origins in Childhood? Dev. Psychol. 2014, 50, 1331–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.; Tsukayama, E.; Goodwin, G.P.; Patrick, S.; Duckworth, A.L. A Tripartite Taxonomy of Character: Evidence for Intrapersonal, Interpersonal, and Intellectual Competencies in Children. Contemp. Educ. Psychol. 2017, 48, 16–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Infertility: A Tabulation of Available Data on Prevalence of Primary and Secondary Infertility; World Health Organization: Geneva, Switzerland, 1991. [Google Scholar]
- Cwikel, J.; Gidron, Y.; Sheiner, E. Psychological Interactions with Infertility among Women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 117, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Domar, A.D. Impact of Psychological Factors on Dropout Rates in Insured Infertility Patients. Fertil. Steril. 2004, 81, 271–273. [Google Scholar] [CrossRef]
- Martins, M.V.; Peterson, B.D.; Almeida, V.; Mesquita-Guimaraes, J.; Costa, M.E. Dyadic Dynamics of Perceived Social Support in Couples Facing Infertility. Hum. Reprod. 2014, 29, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaffe, J. Reproductive Trauma: Psychotherapy for Pregnancy Loss and Infertility Clients from a Reproductive Story Perspective. Psychotherapy 2017, 54, 380–385. [Google Scholar] [CrossRef]
- Panagopoulou, E.; Montgomery, A.; Tarlatzis, B. Experimental Emotional Disclosure in Women Undergoing Infertility Treatment: Are Drop Outs Better Off? Soc. Sci. Med. 2009, 69, 678–681. [Google Scholar] [CrossRef]
- Stanton, A.L.; Lobel, M.; Sears, S.; DeLuca, R.S. Psychosocial Aspects of Selected Issues in Women’s Reproductive Health: Current Status and Future Directions. J. Consult. Clin. Psychol. 2002, 70, 751–770. [Google Scholar] [CrossRef]
- Peterson, B.D.; Gold, L.; Feingold, T. The Experience and Influence of Infertility: Considerations for Couple Counselors. Fam. J. 2007, 15, 251–257. [Google Scholar] [CrossRef]
- Kroemeke, A.; Kubicka, E. Positive and Negative Adjustment in Couples Undergoing Infertility Treatment: The Impact of Support Exchange. PLoS ONE 2018, 13, e0200124. [Google Scholar] [CrossRef] [Green Version]
- Maroufizadeh, S.; Hosseini, M.; Rahimi Foroushani, A.; Omani-Samani, R.; Amini, P. The Relationship between Perceived Stress and Marital Satisfaction in Couples with Infertility: Actor-Partner Interdependence Model. Int. J. Fertil. Steril. 2019, 13, 66–71. [Google Scholar] [CrossRef]
- Kapısız, S.; Akgül Gök, F.; Yılmaz, N.; Özcan, S.; Duyan, V. İnfertil Çiftlerde Evlilik Doyumu ve Evlilik Doyumunu Etkileyen Faktörler [Marital Satisfaction and Influencing Factors in Infertile Couples]. Cukurova Med. J. 2019, 44, 1074–1084. [Google Scholar] [CrossRef] [Green Version]
- Warawan, L.; Wycisk, J. Satysfakcja Małżeńska u Kobiet Niepłodnych z Uwzględnieniem Stylu Radzenia Sobie Ze Stresem [The Marital Satisfaction of Infertility Women, Taking into Consideration a Coping Style]. Psychol. Jakości Życia 2013, 12, 75–89. [Google Scholar]
- Monga, M.; Alexandrescu, B.; Katz, S.E.; Stein, M.; Ganiats, T. Impact of Infertility on Quality of Life, Marital Adjustment, and Sexual Function. Urology 2004, 63, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Tao, P.; Coates, R.; Zhao, Y.; Maycock, B. The Effects of Translating the Multidimensional Sexuality Questionnaire from English to Mandarin: A Test of Reliability and Validity. Sex. Health 2012, 9, 304. [Google Scholar] [CrossRef] [PubMed]
- Onat, G.; Beji, N.K. Marital Relationship and Quality of Life Among Couples with Infertility. Sex. Disabil. 2012, 30, 39–52. [Google Scholar] [CrossRef]
- Nakić Radoš, S.; Soljačić Vraneš, H.; Tomić, J.; Kuna, K. Infertility-Related Stress and Sexual Satisfaction: A Dyadic Approach. J. Psychosom. Obstet. Gynecol. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Newson, L.; Postmes, T.; Lea, S.E.G.; Webley, P.; Richerson, P.J.; Mcelreath, R. Influences on Communication about Reproduction: The Cultural Evolution of Low Fertility☆. Evol. Hum. Behav. 2007, 28, 199–210. [Google Scholar] [CrossRef]
- El Kissi, Y.; Romdhane, A.B.; Hidar, S.; Bannour, S.; Ayoubi Idrissi, K.; Khairi, H.; Ben Hadj Ali, B. General Psychopathology, Anxiety, Depression and Self-Esteem in Couples Undergoing Infertility Treatment: A Comparative Study between Men and Women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 167, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Péloquin, K.; Brassard, A.; Arpin, V.; Sabourin, S.; Wright, J. Whose Fault Is It? Blame Predicting Psychological Adjustment and Couple Satisfaction in Couples Seeking Fertility Treatment. J. Psychosom. Obstet. Gynecol. 2018, 39, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Maroufizadeh, S.; Ghaheri, A.; Almasi-Hashiani, A.; Mohammadi, M.; Navid, B.; Ezabadi, Z.; Omani Samani, R. The Prevalence of Anxiety and Depression among People with Infertility Referring to Royan Institute in Tehran, Iran: A Cross-Sectional Questionnaire Study. Middle East Fertil. Soc. J. 2018, 23, 103–106. [Google Scholar] [CrossRef]
- Hirsch, A.M.; Hirsch, S.M. The Effect of Infertility on Marriage and Self-concept. J. Obstet. Gynecol. Neonatal Nurs. 1989, 18, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Arnn Phipps, S.A. A Phenomenological Study of Couples’ Infertility: Gender Influence. Holist. Nurs. Pract. 1993, 7, 44–56. [Google Scholar] [CrossRef]
- Kornas-Biela, D. Wokół Początku Życia Ludzkiego [About the Beginning of Human Life]; Instytut Wydawniczy PAX: Warszawa, Poland, 2004. [Google Scholar]
- Kornas-Biela, D. Zdobywane Macierzyństwo: Doświadczenia Matek Związane Ze Wspomaganą Prokreacją [Acquired Motherhood: Mothers’ Experiences of Assisted Procreation]. In Oblicza Macierzyństwa; Red. Wydawnictw Katolickiego Uniwersytetu Lubelsliego: Lublin, Poland, 1999. [Google Scholar]
- Barton-Smoczyńska, I. O Dziecku, Które Odwróciło Się Na Pięcie [About a Child Who Turned on It’s Heel]; NAF: Łomianki, Poland, 2006. [Google Scholar]
- Kendall-Tackett, K.A. Treating the Lifetime Health Effects of Childhood Victimization; Civic Research Institute, Inc.: Kingston, NJ, USA, 2003. [Google Scholar]
- Bellhouse, C.; Temple-Smith, M.; Watson, S.; Bilardi, J. “The Loss Was Traumatic… Some Healthcare Providers Added to That”: Women’s Experiences of Miscarriage. Women Birth 2019, 32, 137–146. [Google Scholar] [CrossRef]
- Collins, C.; Riggs, D.W.; Due, C. The Impact of Pregnancy Loss on Women’s Adult Relationships. Grief Matters 2014, 7, 44–50. [Google Scholar]
- Evans, L.; Lloyd, D.; Considine, R.; Hancock, L. Contrasting Views of Staff and Patients Regarding Psychosocial Care for Australian Women Who Miscarry: A Hospital Based Study. Aust. N. Z. J. Obstet. Gynaecol. 2002, 42, 155–160. [Google Scholar] [CrossRef]
- Adolfsson, A. Meta-Analysis to Obtain a Scale of Psychological Reaction after Perinatal Loss: Focus on Miscarriage. PRBM 2011, 4, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Hamama-Raz, Y.; Hemmendinger, S.; Buchbinder, E. The Unifying Difference: Dyadic Coping With Spontaneous Abortion Among Religious Jewish Couples. Qual. Health Res. 2010, 20, 251–261. [Google Scholar] [CrossRef]
- Rinehart, M.S.; Kiselica, M.S. Helping Men with the Trauma of Miscarriage. Psychother. Theory Res. Pract. Train. 2010, 47, 288–295. [Google Scholar] [CrossRef]
- Bubiak, A.; Bartnicki, J.; Knihinicka-Mercik, Z. Psychologiczne aspekty utraty dziecka w okresie prenatalnym. Piel. Zdr. Publ. 2014, 4, 69–78. [Google Scholar]
- Bielan, Z.; Machaj, A.; Stankowska, I. Psychoseksualne konsekwencje straty dziecka w okresie ciąży i porodu. Seksuologia Pol. 2010, 8, 41–46. [Google Scholar]
- Swanson, K.M.; Karmali, Z.A.; Powell, S.H.; Pulvermakher, F. Miscarriage Effects on Couples’ Interpersonal and Sexual Relationships During the First Year After Loss: Women’s Perceptions. Psychosom. Med. 2003, 65, 902–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFrain, J.; Millspaugh, E.; Xie, X. The Psychosocial Effects of Miscarriage: Implications for Health Professionals. Fam. Syst. Health 1996, 14, 331–347. [Google Scholar] [CrossRef]
- Gold, K.J.; Sen, A.; Hayward, R.A. Marriage and Cohabitation Outcomes After Pregnancy Loss. Pediatrics 2010, 125, e1202–e1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shreffler, K.M.; Hill, P.W.; Cacciatore, J. Exploring the Increased Odds of Divorce Following Miscarriage or Stillbirth. J. Divorce Remarriage 2012, 53, 91–107. [Google Scholar] [CrossRef]
- Darnell, W.H.; Buckley, A.N.; Scott, A.M. “It’s Not Something You Expect a 15-Year-Old to Be Sad about”: Sources of Uncertainty and Strategies of Uncertainty Management among Adolescent Women Who Have Experienced Miscarriage. Health Commun. 2019, 34, 1795–1805. [Google Scholar] [CrossRef] [PubMed]
- Callister, L.C. Perinatal Loss: A Family Perspective. J. Perinat. Neonatal Nurs. 2006, 20, 227–234. [Google Scholar] [CrossRef]
- Hutti, M.H.; Armstrong, D.S.; Myers, J.A.; Hall, L.A. Grief Intensity, Psychological Well-Being, and the Intimate Partner Relationship in the Subsequent Pregnancy after a Perinatal Loss. J. Obstet. Gynecol. Neonatal Nurs. 2015, 44, 42–50. [Google Scholar] [CrossRef]
- Hiefner, A.R. Dyadic Coping and Couple Resilience After Miscarriage. Fam. Relat. 2021, 70, 59–76. [Google Scholar] [CrossRef]
- Lang, A.; Fleiszer, A.R.; Duhamel, F.; Sword, W.; Gilbert, K.R.; Corsini-Munt, S. Perinatal Loss and Parental Grief: The Challenge of Ambiguity and Disenfranchised Grief. Omega 2011, 63, 183–196. [Google Scholar] [CrossRef]
- Boyce, P.M.; Condon, J.T.; Ellwood, D.A. Pregnancy Loss: A Major Life Event Affecting Emotional Health and Well-being. Med. J. Aust. 2002, 176, 250–251. [Google Scholar] [CrossRef] [PubMed]
- Guzewicz, M.; Steuden, S.; Szymona-Pałkowska, K. Original Article Changes in the Perception of Self-Image and the Sense of Purpose and Meaning in Life, among Women Who Lost Their Child before Birth. Health Psychol. Rep. 2014, 3, 162–175. [Google Scholar] [CrossRef]
- Conway, K.; Russell, G. Couples’ Grief and Experience of Support in the Aftermath of Miscarriage. Br. J. Med. Psychol. 2000, 73, 531–545. [Google Scholar] [CrossRef] [PubMed]
- McCreight, B.S. A Grief Ignored: Narratives of Pregnancy Loss from a Male Perspective. Sociol Health Illn. 2004, 26, 326–350. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.P.; Puddifoot, J.E. The Grief Response in the Partners of Women Who Miscarry. Br. J. Med. Psychol. 1996, 69, 313–327. [Google Scholar] [CrossRef]
- Due, C.; Chiarolli, S.; Riggs, D.W. The Impact of Pregnancy Loss on Men’s Health and Wellbeing: A Systematic Review. BMC Pregnancy Childbirth 2017, 17, 380. [Google Scholar] [CrossRef] [Green Version]
- Finkel, E.J.; Campbell, W.K. Self-Control and Accommodation in Close Relationships: An Interdependence Analysis. J. Personal. Soc. Psychol. 2001, 81, 263–277. [Google Scholar] [CrossRef]
- Karremans, J.C.; Pronk, T.M.; van der Wal, R.C. Executive Control and Relationship Maintenance Processes: An Empirical Overview and Theoretical Integration: Executive Control and Relationship Maintenance. Soc. Personal. Psychol. Compass 2015, 9, 333–347. [Google Scholar] [CrossRef]
- Vohs, K.D.; Finkenauer, C.; Baumeister, R.F. The Sum of Friends’ and Lovers’ Self-Control Scores Predicts Relationship Quality. Soc. Psychol. Personal. Sci. 2011, 2, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Gomillion, S.; Lamarche, V.M.; Murray, S.L.; Harris, B. Protected By Your Self-Control: The Influence of Partners’ Self-Control on Actors’ Responses to Interpersonal Risk. Soc. Psychol. Personal. Sci. 2014, 5, 873–882. [Google Scholar] [CrossRef]
- Righetti, F.; Finkenauer, C. If You Are Able to Control Yourself, I Will Trust You: The Role of Perceived Self-Control in Interpersonal Trust. J. Personal. Soc. Psychol. 2011, 100, 874–886. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, J.X.; van Dellen, M.R.; Shaffer, A. Examining Trait Self-Control and Communication Patterns in Romantic Couples Using the Actor-Partner Interaction Model. Personal. Individ. Differ. 2017, 106, 222–225. [Google Scholar] [CrossRef]
- Pronk, T.M.; Karremans, J.C. Does Executive Control Relate to Sacrificial Behavior during Conflicts of Interests?: Executive Control and Sacrificial Behavior. Pers. Relatsh. 2014, 21, 168–175. [Google Scholar] [CrossRef]
- Burnette, J.L.; Davisson, E.K.; Finkel, E.J.; Van Tongeren, D.R.; Hui, C.M.; Hoyle, R.H. Self-Control and Forgiveness: A Meta-Analytic Review. Soc. Psychol. Personal. Sci. 2014, 5, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Zuo, P.-Y.; Karremans, J.C.; Scheres, A.; Kluwer, E.S.; Burk, W.J.; Kappen, G.; Ter Kuile, H. A Dyadic Test of the Association Between Trait Self-Control and Romantic Relationship Satisfaction. Front. Psychol. 2020, 11, 594476. [Google Scholar] [CrossRef]
- Pronk, T.M.; Righetti, F. How Executive Control Promotes Happy Relationships and a Well-Balanced Life. Curr. Opin. Psychol. 2015, 1, 14–17. [Google Scholar] [CrossRef]
- Pronk, T.M.; Karremans, J.C.; Overbeek, G.; Vermulst, A.A.; Wigboldus, D.H.J. What It Takes to Forgive: When and Why Executive Functioning Facilitates Forgiveness. J. Personal. Soc. Psychol. 2010, 98, 119–131. [Google Scholar] [CrossRef]
- Findley, M.B.; Carvallo, M.; Bartak, C.P. The Effect of Self-Control on Willingness to Sacrifice in Close Relationships. Self Identity 2014, 13, 334–344. [Google Scholar] [CrossRef]
- Righetti, F.; Finkenauer, C.; Finkel, E.J. Low Self-Control Promotes the Willingness to Sacrifice in Close Relationships. Psychol. Sci. 2013, 24, 1533–1540. [Google Scholar] [CrossRef]
- Visserman, M.L.; Righetti, F.; Kumashiro, M.; Van Lange, P.A.M. Me or Us? Self-Control Promotes a Healthy Balance Between Personal and Relationship Concerns. Soc. Psychol. Personal. Sci. 2017, 8, 55–65. [Google Scholar] [CrossRef]
- Peterson, B.D.; Newton, C.R.; Rosen, K.H.; Schulman, R.S. Coping Processes of Couples Experiencing Infertility. Fam. Relat. 2006, 55, 227–239. [Google Scholar] [CrossRef]
- Bolvin, J.; Lancastle, D. Medical Waiting Periods: Imminence, Emotions and Coping. Womens Health 2010, 6, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Diamond, R. Couple Therapy for Infertility; The Guilford family therapy series; Guilford Press: New York, NY, USA, 1999; ISBN 978-1-57230-511-3. [Google Scholar]
- Huić, A.; Krznarić, T.; Kamenov, Ž. Time Perspective, Perceived Stress, Self-Control and Relationship Satisfaction in Heterosexual Dating Relationships of Emerging Adults. PSICOLOGIA 2018, 32, 63–78. [Google Scholar] [CrossRef]
- Farren, J.; Jalmbrant, M.; Falconieri, N.; Mitchell-Jones, N.; Bobdiwala, S.; Al-Memar, M.; Tapp, S.; Van Calster, B.; Wynants, L.; Timmerman, D.; et al. Differences in Post-traumatic Stress, Anxiety and Depression Following Miscarriage or Ectopic Pregnancy between Women and Their Partners: Multicenter Prospective Cohort Study. Ultrasound Obs. Gynecol. 2021, 57, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Basanta, S.; Coronado, C.; Movilla-Fernández, M. Multicultural Coping Experiences of Parents Following Perinatal Loss: A Meta-ethnographic Synthesis. J. Adv. Nurs. 2020, 76, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Kiełek-Rataj, E.; Wendołowska, A.; Kalus, A.; Czyżowska, D. Openness and Communication Effects on Relationship Satisfaction in Women Experiencing Infertility or Miscarriage: A Dyadic Approach. Int. J. Environ. Res. Public Health 2020, 17, 5721. [Google Scholar] [CrossRef]
- Horstman, H.K.; Holman, A. Communicated Sense-Making After Miscarriage: A Dyadic Analysis of Spousal Communicated Perspective-Taking, Well-Being, and Parenting Role Salience. Health Commun. 2018, 33, 1317–1326. [Google Scholar] [CrossRef]
- McCormick, T.M. Out of Control: One Aspect of Infertility. JOGN J. Obstet. Gynecol. Neonatal. Nurs. 1980, 9, 205–206. [Google Scholar] [CrossRef]
- Donnellan, M.B.; Conger, R.D.; Burzette, R.G. Personality Development From Late Adolescence to Young Adulthood: Differential Stability, Normative Maturity, and Evidence for the Maturity-Stability Hypothesis. J. Personal. 2007, 75, 237–264. [Google Scholar] [CrossRef]
- Lavner, J.A.; Clark, M.A. Workload and Marital Satisfaction over Time: Testing Lagged Spillover and Crossover Effects during the Newlywed Years. J. Vocat. Behav. 2017, 101, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.; Jarnecke, A.M.; South, S.C. Impulsivity, Communication, and Marital Satisfaction in Newlywed Couples: Impulsivity and Marital Relationships. Pers. Relatsh. 2017, 24, 423–439. [Google Scholar] [CrossRef]
- Stroud, C.B.; Durbin, C.E.; Saigal, S.D.; Knobloch-Fedders, L.M. Normal and Abnormal Personality Traits Are Associated with Marital Satisfaction for Both Men and Women: An Actor-Partner Interdependence Model Analysis. J. Res. Personal. 2010, 44, 466–477. [Google Scholar] [CrossRef] [Green Version]
- Mead, N.L. Personality Predictors of Relationship Satisfaction among Engaged and Married Couples: An Analysis of Actor and Partner Effects; Brigham Young University: Provo, UT, USA, 2005. [Google Scholar]
- Patrick, S.; Sells, J.N.; Giordano, F.G.; Tollerud, T.R. Intimacy, Differentiation, and Personality Variables as Predictors of Marital Satisfaction. Fam. J. 2007, 15, 359–367. [Google Scholar] [CrossRef]
- Kenny, D.A. Models of Non-Independence in Dyadic Research. J. Soc. Pers. Relatsh. 1996, 13, 279–294. [Google Scholar] [CrossRef]
- Campbell, L.; Stanton, S.C.E. Actor-Partner Interdependence Model. In The Encyclopedia of Clinical Psychology; Cautin, R.L., Lilienfeld, S.O., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; pp. 1–7. ISBN 978-1-118-62539-2. [Google Scholar]
- Kenny, D.A.; Kashy, D.A.; Cook, W.L. Dyadic Data Analysis; Methodology in the social sciences; Guilford Press: New York, NY, USA, 2006; ISBN 978-1-57230-986-9. [Google Scholar]
- Cook, W.L.; Kenny, D.A. The Actor-Partner Interdependence Model: A Model of Bidirectional Effects in Developmental Studies. Int. J. Behav. Dev. 2005, 29, 101–109. [Google Scholar] [CrossRef]
- Braun-Gałkowska, M. Psychologiczna Analiza Systemów Rodzinnych Osób Zadowolonych i Niezadowolonych z Małżeństwa [Psychological Analysis of the Family Systems of Satisfied and Dissatisfied People from Marriage]; Towarzystwo Naukowe Katolickiego Uniwersytetu Lubelskiego: Lublin, Poland, 1992. [Google Scholar]
- Beckmann, D.; Brähler, E.; Richter, H.-E. Der Giessen-Test (GT); Huber: Bern, Switzerland, 1991. [Google Scholar]
- McCubbin, H.I.; Olson, D.H.; Larsen, A. Family Crisis-Oriented Personal Evaluation Scales (F-COPES) 1981. In Handbook of Measurements for Marriage and Family Therapy; Brunner Mazel Publ: New York, NY, USA, 1987. [Google Scholar]
- Radochoński, M. Choroba a Rodzina. Adaptacja Systemu Rodzinnego Do Sytuacji Stresowej Wywołanej Choroba Somatyczna [Illness and the Family. Adaptation of the Family System to the Induced Stress Situation Somatic Disease]; WSP: Rzeszów, Poland, 1987. [Google Scholar]
- Cohen, S.; Schulz, M.S.; Weiss, E.; Waldinger, R.J. Eye of the Beholder: The Individual and Dyadic Contributions of Empathic Accuracy and Perceived Empathic Effort to Relationship Satisfaction. J. Fam. Psychol. 2012, 26, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Mueller, O.; Hancock, G.R. Structural Equation Modeling. In The Reviewer’s Guide to Quantitative Methods in the Social Sciences, Hancock, G.R., Stapleton, L.M., Mueller, R.O., Eds.; 2nd ed.; Routledge, Taylor & Francis Group: New York, NY, USA, 2019; ISBN 978-1-138-80012-0. [Google Scholar]
- Kenny, D.A.; Ledermann, T. Detecting, Measuring, and Testing Dyadic Patterns in the Actor-Partner Interdependence Model. J. Fam. Psychol. 2010, 24, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Ackerman, R.A.; Ledermann, T.; Kenny, D.A. APIMPower: An Interactive Tool for Actor-Partner Interdependence Model Power Analysis. Available online: https://robert-a-ackerman.shinyapps.io/apimpower/ (accessed on 4 May 2021).
- Benyamini, Y.; Gozlan, M.; Kokia, E. Women’s and Men’s Perceptions of Infertility and Their Associations with Psychological Adjustment: A Dyadic Approach. Br. J. Health Psychol. 2009, 14, 1–16. [Google Scholar] [CrossRef]
- Mohammadi, M.; Samani, R.O.; Navid, B.; Maroufizadeh, S.; Sabeti, S. Coping Strategy in Infertile Couples Undergoing Assisted Reproduction Treatment. Middle East Fertil. Soc. J. 2018, 23, 482–485. [Google Scholar] [CrossRef]
- Farren, J.; Jalmbrant, M.; Falconieri, N.; Mitchell-Jones, N.; Bobdiwala, S.; Al-Memar, M.; Tapp, S.; Van Calster, B.; Wynants, L.; Timmerman, D.; et al. Posttraumatic Stress, Anxiety and Depression Following Miscarriage and Ectopic Pregnancy: A Multicenter, Prospective, Cohort Study. Am. J. Obstet. Gynecol. 2020, 222, 367.e1–367.e22. [Google Scholar] [CrossRef] [PubMed]
- Oti-Boadi, M.; Oppong Asante, K. Psychological Health and Religious Coping of Ghanaian Women with Infertility. BioPsychoSoc. Med. 2017, 11, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojedokun, I.M. Influence of Family and Spiritual Supports on Coping with Infertility among Couples in Ibadan Oyo State Nigeria. Afr. J. Psychol. Study Soc. Issues 2019, 22, 205–216. [Google Scholar]
- Kalu, F. Women’s Experiences of Utilizing Religious and Spiritual Beliefs as Coping Resources After Miscarriage. Religions 2019, 10, 185. [Google Scholar] [CrossRef] [Green Version]
- Iwanowicz-Palus, G.; Mróz, M.M.; Bień, A. Social Support and Subjective Assessment of Psychophysical Condition, Health, and Satisfaction with Quality of Life among Women after Pregnancy Loss; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Cannon, M.D. The Power and Challenge of Facilitating Reframing: Applications in Teaching Negotiation. Manag. Teach. Rev. 2017, 2, 179–192. [Google Scholar] [CrossRef]
- Nagórska, M.; Obrzut, B.; Ulman, D.; Darmochwał-Kolarz, D. The Need of Personalized Medicine in Coping with Stress during Infertility Treatment. J. Pers. Med. 2021, 11, 56. [Google Scholar] [CrossRef]
- Swanson, K.M.; Connor, S.; Jolley, S.N.; Pettinato, M.; Wang, T.-J. Contexts and Evolution of Women’s Responses to Miscarriage during the First Year after Loss. Res. Nurs. Health 2007, 30, 2–16. [Google Scholar] [CrossRef]
- Berghuis, J.P.; Stanton, A.L. Adjustment to a Dyadic Stressor: A Longitudinal Study of Coping and Depressive Symptoms in Infertile Couples over an Insemination Attempt. J. Consult. Clin. Psychol. 2002, 70, 433–438. [Google Scholar] [CrossRef]
- Husaini, B.A.; Newbrough, J.R.; Neff, J.A.; Moore, M.C. The Stress-Buffering Role of Social Support and Personal Competence among the Rural Married. J. Communrry Psychol. 1982, 10, 409–426. [Google Scholar] [CrossRef]
- Ryan, M.A. Faith and Infertility. In On Moral Medicine: Theological Perspectives on Medical Ethics; Lysaugh, M.T., Kotva, J., Lammer, S.E., Verhey, A., Eds.; WB Eerdmans: Cambridge, MA, USA, 2012; pp. 865–869. [Google Scholar]
- Zandi, M.; Mohammadi, E.; Vanaki, Z.; Shiva, M.; Bagheri Lankarani, N.; Zarei, F. Confronting Infertility in Iranian Clients: A Grounded Theory. Human Fertil. 2017, 20, 236–247. [Google Scholar] [CrossRef]
- Fatehizadeh, M.S.; Badiee, D. The Relationship of Spirituality Experience with Coping Strategies with Stress Among Students of Razi University. Islamic Perspect. Educ. Sci. 2016, 4, 139–156. [Google Scholar] [CrossRef]
- Agustus, P.; Munivenkatappa, M.; Prasad, P. Sexual Functioning, Beliefs about Sexual Functioning and Quality of Life of Women with Infertility Problems. J. Hum. Reprod. Sci. 2017, 10, 213. [Google Scholar] [CrossRef]
- Fassino, S.; Piero, A.; Boggio, S.; Piccioni, V.; Garzaro, L. Anxiety, Depression and Anger Suppression in Infertile Couples: A Controlled Study. Hum. Reprod. 2002, 17, 2986–2994. [Google Scholar] [CrossRef] [PubMed]
- Woollett, A. Childlessness: Strategies for Coping with Infertility. Int. J. Behav. Dev. 1985, 8, 473–482. [Google Scholar] [CrossRef]
- Kamal, E.; Abd El-Ghany, N.; Abdulla, S.; Badran, A. Impact of Male Infertility on Men’s Self-Esteem. Hum. Androl. 2019, 9, 40–47. [Google Scholar] [CrossRef]
- Hjelmstedt, A.; Andersson, L.; Skoog-SVANBERG, A.; Bergh, T.; Boivin, J.; Collins, A. Gender Differences in Psychological Reactions to Infertility among Couples Seeking IVF- and ICSI-Treatment. Acta Obstet. Gynecol. Scand. 1999, 78, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.M. Integrating Family Resilience and Family Stress Theory. J. Marriage Fam. 2002, 64, 349–360. [Google Scholar] [CrossRef]
- Andersson, I.-M.; Nilsson, S.; Adolfsson, A. How Women Who Have Experienced One or More Miscarriages Manage Their Feelings and Emotions When They Become Pregnant Again - a Qualitative Interview Study: Master Feelings during Pregnancy after Miscarriage. Scand. J. Caring Sci. 2012, 26, 262–270. [Google Scholar] [CrossRef]
- Martins, M.V.; Peterson, B.D.; Costa, P.; Costa, M.E.; Lund, R.; Schmidt, L. Interactive Effects of Social Support and Disclosure on Fertility-Related Stress. J. Soc. Pers. Relatsh. 2013, 30, 371–388. [Google Scholar] [CrossRef]
- Luk, B.H.-K.; Loke, A.Y. The Impact of Infertility on the Psychological Well-Being, Marital Relationships, Sexual Relationships, and Quality of Life of Couples: A Systematic Review. J. Sex Marital. Ther. 2015, 41, 610–625. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, M.K.; Stephenson, M.D. “Information-Rich” Reproductive Outcomes in Carriers of a Structural Chromosome Rearrangement Ascertained on the Basis of Recurrent Pregnancy Loss. Fertil. Steril. 2012, 97, 894–903. [Google Scholar] [CrossRef]
- Wang, S.-Y.; Chen, C.-H. The Association Between Prenatal Depression and Obstetric Outcome in Taiwan: A Prospective Study. J. Women’s Health 2010, 19, 2247–2251. [Google Scholar] [CrossRef]
- Tian, X.; Solomon, D.H. Grief and Post-Traumatic Growth Following Miscarriage: The Role of Meaning Reconstruction and Partner Supportive Communication. Death Stud. 2020, 44, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Wiweko, B.; Anggraheni, U.; Elvira, S.D.; Lubis, H.P. Distribution of Stress Level among Infertility Patients. Middle East Fertil. Soc. J. 2017, 22, 145–148. [Google Scholar] [CrossRef]
- Thorn, P.; Wischmann, T. German Guidelines for Psychosocial Counselling in the Area of Gamete Donation. Human Fertil. 2009, 12, 73–80. [Google Scholar] [CrossRef]
- Gergett, B.; Gillen, P. Pregnancy Loss: Perceptions of Healthcare Professionals Evidence Based Midwifery. Evid. Based Midwifery 2014, 12, 29–34. [Google Scholar]
- Bellhouse, C.; Temple-Smith, M.J.; Bilardi, J.E. “It’s Just One of Those Things People Don’t Seem to Talk about...” Women’s Experiences of Social Support Following Miscarriage: A Qualitative Study. BMC Women’s Health 2018, 18, 176. [Google Scholar] [CrossRef]
- Chen, Z.J.; Bechara, A.O.; Worthington, E.L.; Davis, E.B.; Csikszentmihalyi, M. Trauma and Well-Being in Colombian Disaster Contexts: Effects of Religious Coping, Forgivingness, and Hope. J. Posit. Psychol. 2021, 16, 82–93. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Infertility (n = 50) | Miscarriage (n = 40) | t-Test Men | t-Test Women | Men | Women | Sex Diff | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men M/SD | Women M/SD | Men M/SD | Women M/SD | M | SD | M | SD | ||||||||
| Satisfaction | 74.40 | 19.73 | 73.58 | 21.40 | 67.19 | 22.16 | 60.72 | 25.95 | 1.63 | 2.58 * | 71.20 | 21.32 | 67.86 | 24.26 | −1.57 |
| Self-contr_O | 27.18 | 3.76 | 28.24 | 3.85 | 27.33 | 3.72 | 24.43 | 4.25 | −0.18 | 1.19 | 27.24 | 3.72 | 27.74 | 4.45 | 0.82 |
| Self-contr_P | 29.86 | 3.76 | 27.94 | 5.06 | 27.20 | 4.29 | 26.45 | 4.23 | 3.13 ** | 1.49 | 28.68 | 4.74 | 27.28 | 4.19 | −2.24 * |
| Soc. support | 27.38 | 5.38 | 30.34 | 5.80 | 26.53 | 5.96 | 29.63 | 5.53 | 0.71 | 0.59 | 27 | 5.63 | 30.02 | 5.66 | 4.36 *** |
| Spir. support | 12.88 | 4.45 | 14.72 | 4 | 10.80 | 4.56 | 11.88 | 4.54 | 2.18 * | 3.16 ** | 11.96 | 4.59 | 13.46 | 4.46 | 4.42 *** |
| Help accept. | 15.16 | 3.29 | 16.84 | 3.20 | 15.43 | 2.48 | 16.02 | 3.83 | −0.42 | 1.10 | 15.28 | 2.94 | 16.48 | 3.50 | 2.84 ** |
| Pas. appraisal | 7.86 | 3.01 | 7.54 | 2.48 | 8.35 | 2.28 | 8.00 | 2.67 | −0.85 | −0.85 | 8.08 | 2.71 | 7.74 | 2.56 | −1.07 |
| Reframing | 26.90 | 4.16 | 27.12 | 5.24 | 26.38 | 3.51 | 24.43 | 4.25 | 0.64 | 2.63 * | 25.67 | 3.87 | 27.92 | 4.98 | −1.62 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Satisfaction_A | 1.00 | |||||||||||||||
| 2 | Social suport_A | 0.14 | 1.00 | ||||||||||||||
| 3 | Spiritual suport_A | 0.34 ** | 0.13 | 1.00 | |||||||||||||
| 4 | Help acceptance_A | 0.17 | 0.64 ** | 0.15 | 1.00 | ||||||||||||
| 5 | Passive appraisal_A | −0.01 | 0.17 | 0.17 | 0.16 | 1.00 | |||||||||||
| 6 | Reframing_A | 0.23 * | −0.02 | 0.36 ** | 0.00 | 0.28 ** | 1.00 | ||||||||||
| 7 | Self-control_O_A | −0.01 | −0.09 | 0.07 | −0.11 | −0.22 | 0.12 | 1.00 | |||||||||
| 8 | Self-control_P_A | 0.11 | 0.10 | 0.11 | 0.17 | −0.07 | −0.17 | −0.01 | 1.00 | ||||||||
| 9 | Satisfaction_P | 0.61 ** | 0.13 | 0.19 | 0.18 | −0.08 | 0.16 | −0.08 | 0.01 | 1.00 | |||||||
| 10 | Social suport_P | 0.11 | 0.32 ** | 0.15 | 0.19 | 0.21 | 0.31 ** | 0.03 | 0.00 | 0.19 | 1.00 | ||||||
| 11 | Spiritual suport_P | 0.33 ** | −0.02 | 0.75 ** | −0.01 | 0.00 | 0.30 ** | 0.06 | 0.07 | 0.20 | 0.22 * | 1.00 | |||||
| 12 | Help acceptance_P | 0.03 | 0.10 | 0.03 | 0.23 * | −0.03 | 0.16 | 0.13 | −0.03 | 0.18 | 0.50 ** | 0.06 | 1.00 | ||||
| 13 | Passive appraisal_P | −0.03 | −0.02 | 0.16 | −0.02 | 0.37 ** | 0.24 * | −0.12 | −0.19 | −0.06 | 0.24 * | 0.00 | 0.00 | 1.00 | |||
| 14 | Reframing_P | 0.20 | −0.12 | 0.16 | 0.01 | 0.35 ** | 0.54 ** | 0.01 | −0.19 | 0.20 | 0.15 | 0.19 | −0.03 | 0.33 ** | 1.00 | ||
| 15 | Self-control_O_P | −0.11 | −0.01 | −0.08 | 0.03 | 0.02 | 0.02 | 0.02 | 0.40 ** | −0.13 | 0.10 | −0.10 | 0.11 | −0.24 * | −0.11 | 1.00 | |
| 16 | Self-control_P_P | 0.32 ** | 0.00 | 0.20 | 0.21 | −0.05 | 0.25 * | 0.30 ** | 0.12 | 0.30 ** | 0.14 | 0.18 | 0.20 | −0.25 * | 0.16 | 0.07 | 1.00 |
| Model | Effect | Estimate | 95% CI | p | Beta | r |
|---|---|---|---|---|---|---|
| Model 1 | Women | |||||
| Intercept | 66.84 | 61.10 to 71.67 | <0.001 | |||
| Actor | 0.35 | −0.66 to 1.35 | 0.501 | 0.07 | 0.07 | |
| Partner | 1.81 | 0.68 to 2.95 | 0.002 | 0.31 | 0.31 | |
| Men | ||||||
| Intercept | 70.23 | 65.79 to 74.25 | <0.001 | |||
| Actor | 1.54 | 0.55 to 2.54 | 0.002 | 0.31 | 0.31 | |
| Partner | −0.14 | −1.02 to 0.74 | 0.761 | −0.03 | −0.03 | |
| Model 2 | Women | |||||
| Self-control_P | ||||||
| Intercept | 66.77 | 62.05 to 71.50 | <0.001 | |||
| Actor | 0.70 | −0.36 to 1.78 | 0.196 | 0.14 | 0.07 | |
| Partner | 2.03 | 0.87 to 3.20 | <0.001 | 0.35 | 0.31 | |
| Self-control_O | ||||||
| Intercept | 66.77 | 62.05 to 71.50 | <0.001 | |||
| Actor | −0.59 | −1.68 to 0.51 | 0.292 | −0.11 | −0.004 | |
| Partner | −1.24 | −2.59 to 0.12 | 0.074 | −0.19 | −0.11 | |
| Men | ||||||
| Self-control_P | ||||||
| Intercept | 69.98 | 65.87 to 74.08 | <0.001 | |||
| Actor | 1.85 | 0.84 to 2.86 | <0.001 | 0.37 | 0.31 | |
| Partner | 1.19 | −0.81 to 1.05 | 0.804 | 0.03 | −0.03 | |
| Self-control_O | ||||||
| Intercept | 69.98 | 65.87 to 74.08 | <0.001 | |||
| Actor | −0.93 | −2.10 to 0.25 | 0.123 | −0.16 | −0.13 | |
| Partner | −0.88 | −1.82 to 0.07 | 0.070 | 0.08 | ||
| Model 3 | Women | |||||
| Self-control_P | ||||||
| Intercept | 65.20 | 13.30 to 117.11 | 0.014 | |||
| Actor | 0.51 | −0.52 to 1.55 | 0.332 | 0.1 | 0.07 | |
| Partner | 1.47 | 0.29 to 2.65 | 0.015 | 0.25 | 0.31 | |
| Self-control_O | ||||||
| Intercept | 65.20 | 13.30 to 117.11 | 0.014 | |||
| Actor | −0.45 | −1.50 to 0.60 | 0.398 | −0.08 | −0.004 | |
| Partner | −1.05 | −2.36 to 0.25 | 0.112 | −0.19 | −0.11 | |
| Men | ||||||
| Self-control_P | ||||||
| Intercept | 79.23 | 33.33 to 125.13 | <0.001 | |||
| Actor | −0.51 | 0.47 to 2.56 | 0.005 | 0.30 | 0.31 | |
| Partner | 0.02 | −0.90 to 0.93 | 0.974 | 0.003 | −0.03 | |
| Self-control_O | ||||||
| Intercept | 79.23 | 33.33 to 125.13 | <0.001 | |||
| Actor | −0.83 | −1.98 to 0.33 | 0.159 | −0.15 | −0.13 | |
| Partner | −0.76 | −1.69 to 0.17 | 0.108 | 0.08 |
| Variables | Effect Type | Estimate | p Value | 95% CI | Standardized |
|---|---|---|---|---|---|
| Self-control_P | Actor | 0.87 | 0.01 | 0.17 to 1.57 | 0.25 |
| Partner | 0.77 | 0.03 | −0.31 to 1.46 | 0.20 | |
| Social support | Actor | 0.39 | 0.15 | −0.14 to 0.91 | 0.08 |
| Partner | 0.21 | 0.43 | −0.31 to 0.74 | 0.04 | |
| Interaction | Actor-Actor | −0.02 | 0.74 | −0.13 to 0.09 | −0.02 |
| Actor-Partner | 0.13 | 0.03 | 0.25 to 0.15 | 0.15 | |
| Partner-Actor | 0.03 | 0.59 | 0.15 to 0.04 | 0.04 | |
| Partner-Partner | −0.12 | 0.04 | −0.01 to −0.14 | −0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wendołowska, A.; Kiełek-Rataj, E.; Kalus, A.; Czyżowska, D. Perceived Partner’s Self-Control and Social Support Effects on Relationship Satisfaction in Couples Experiencing Infertility or Miscarriage: Dyadic Analyses. Int. J. Environ. Res. Public Health 2022, 19, 1970. https://doi.org/10.3390/ijerph19041970
Wendołowska A, Kiełek-Rataj E, Kalus A, Czyżowska D. Perceived Partner’s Self-Control and Social Support Effects on Relationship Satisfaction in Couples Experiencing Infertility or Miscarriage: Dyadic Analyses. International Journal of Environmental Research and Public Health. 2022; 19(4):1970. https://doi.org/10.3390/ijerph19041970
Chicago/Turabian StyleWendołowska, Anna, Ewa Kiełek-Rataj, Alicja Kalus, and Dorota Czyżowska. 2022. "Perceived Partner’s Self-Control and Social Support Effects on Relationship Satisfaction in Couples Experiencing Infertility or Miscarriage: Dyadic Analyses" International Journal of Environmental Research and Public Health 19, no. 4: 1970. https://doi.org/10.3390/ijerph19041970