
Impact of Socioeconomic Environment on Home Social Care Service Demand and Dependent Users


Abstract
:1. Introduction
1.1. Problem Context and Description
- Assistance: personal care and hygiene (partial or total), food (cooking and organization), movement within the home, medication control, communication activities, and accompaniment outside the home;
- Educational and social: social care for underage and elderly users or users with other recognized dependencies, follow-up for adequate nutrition, and support and motivation in learning processes to reduce the impact of dependencies on the users’ basic needs;
- Prevention and detection: These tasks are complementary to the others and are especially important in complex services.
2. Materials and Methods
2.1. Datasets
2.2. Descriptive Analytics
3. Results
3.1. Preliminary Study
3.2. Population—SADEP Analysis
3.3. SADEP—SAD Analysis
4. Discussion
4.1. Population—SADEP Analysis
4.2. SADEP—SAD Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Additional Figures
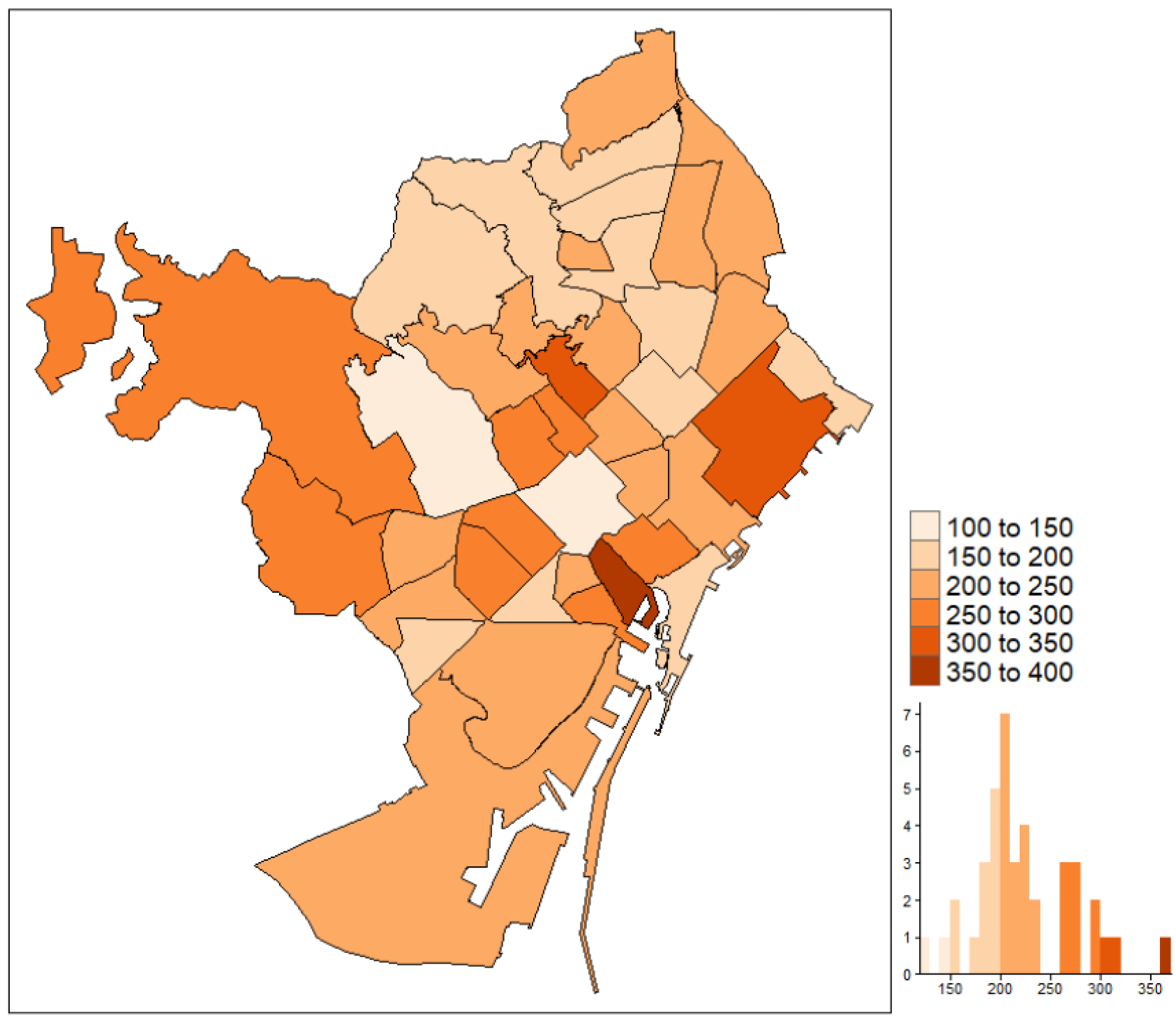
Appendix A.1. Barcelona Maps



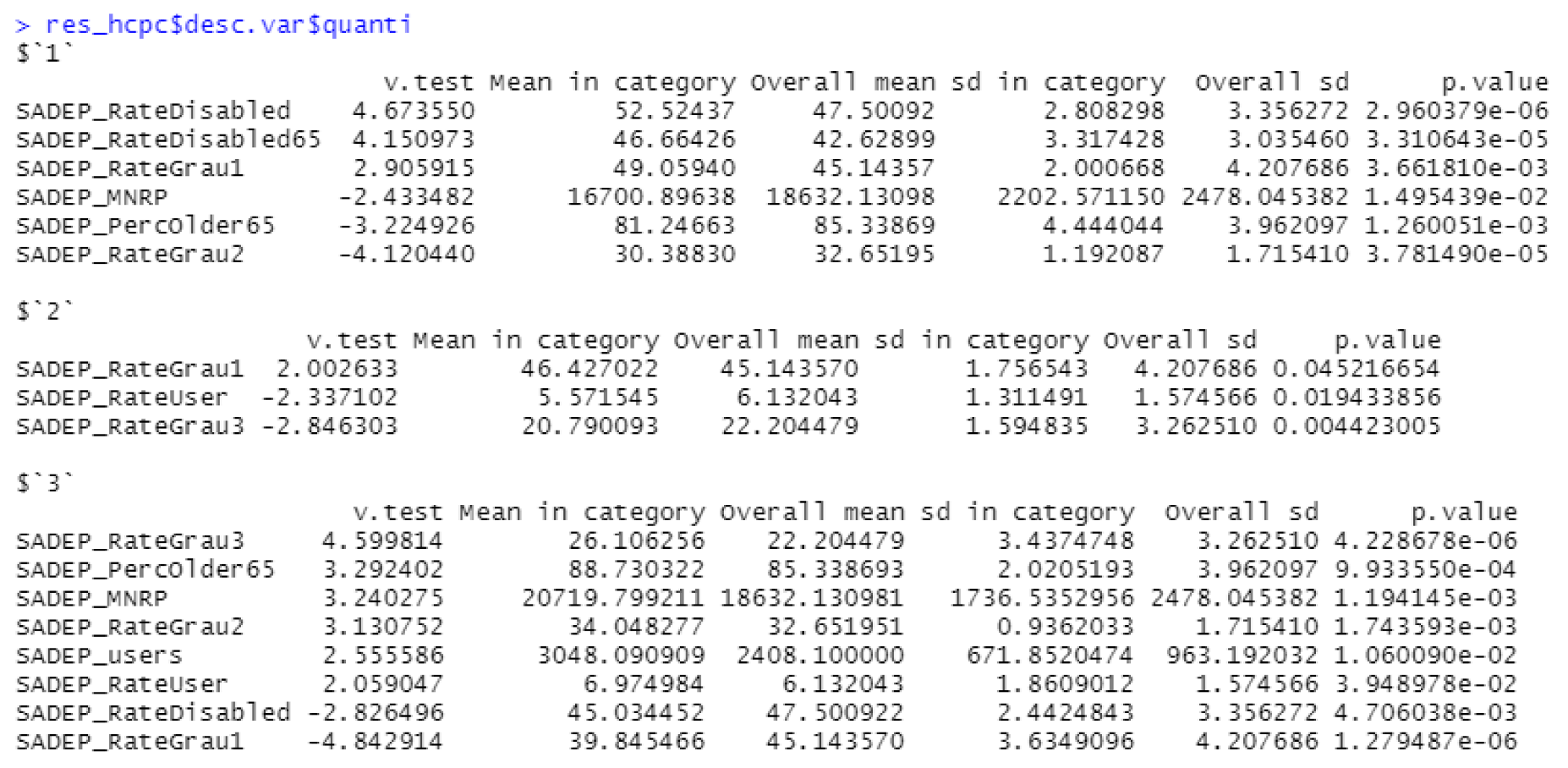
Appendix A.2. Hierarchical Clustering






Appendix A.3. Variables Description Table

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Data | Definition |
|---|---|---|
| Population | INE | Number of people |
| DensityResSurface | ODB | Number of people per residential surface in hectares |
| PercFemale | INE | Percentage of females over the population |
| PercOlder65 | INE | Percentage of people older than 65 over the population |
| PercOlder80 | INE | Percentage of people older than 80 over the population |
| PercOlder65Alone | ODB | Percentage of people older than 65 and living alone |
| PercDisabled | ODB | Percentage of people with a recognized disability |
| PercOlder65Disabled | ODB | Percentage of people older than 65 and some disability |
| PercDisabledDg1 | ODB | Percentage of people with disability lower than 33% |
| PercDisabledDg2 | ODB | Percentage of people with disability between 33% and 65% |
| PercDisabledDg3 | ODB | Percentage of people with disability greater than 65% |
| MNRP | INE | Mean net rate per person. |
| SADEPRateUser | BCN | Percentage of SADEP users over the population |
| SADEP_MNRP | BCN | MNRP computed from the latest updated rent |
| SADEP_PercOlder65 | BCN | Percentage of SADEP users older than 65 |
| SADEP_RateGrau1 | BCN | Percentage of SADEP users with 1st dependency degree |
| SADEP_RateGrau2 | BCN | Percentage of SADEP users with 2nd dependency degree |
| SADEP_RateGrau3 | BCN | Percentage of SADEP users with 3rd dependency degree |
| SADEP_RateDisabled | BCN | Percentage of SADEP users with recognized disabilities |
| SADEP_RateDisabled65 | BCN | Percentage of SADEP users with recognized disabilities and older than 65 |
| SAD_RateUser | BCN | Percentage of SAD users over the population |
| SAD_RateUserSADEP | BCN | Percentage of SAD users over SADEP users |
| UserTF_2019 | BCN | Number of SAD users counted in 2019 |
| UserNET_2019 | BCN | Number of users of home care cleaning services |
| TFPerUser_2019 | BCN | Number of caregivers per user |
| NETPerUser_2019 | BCN | Number of home cleaners per user |
| ServTime_2019 | BCN | Amount of time employed in SAD services |
| SAD_RateUser65SADEP | BCN | Percentage of SAD users older than 65 over SADEP users |
| SAD_RateDisabled | BCN | Percentage of SAD users that have a disability |
| SAD_RateDisabled65 | BCN | Percentage of SAD users that have a disability and are older than 65 |
References
- World Population Ageing 2020, United Nations, Department of Economic and Social Affairs. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2020/Nov/undesa_pd-2020_world_population_ageing_highlights.pdf (accessed on 17 December 2021).
- World Social Report 2020, United Nations, Department of Economic and Social Affairs. Available online: https://www.un.org/development/desa/dspd/wp-content/uploads/sites/22/2020/02/World-Social-Report2020-FullReport.pdf (accessed on 17 December 2021).
- Available online: https://www.statista.com/statistics/271056/age-distribution-in-spain/ (accessed on 31 January 2022).
- European Comission. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Ageing_Europe_-_statistics_on_population_developments (accessed on 17 December 2021).
- Wittenberg, R.; Hu, B. Projections of Demand for and Costs of Social Care for Older People and Younger Adults in England. PSSRU 2015. Available online: http://eprints.lse.ac.uk/id/eprint/40720 (accessed on 19 December 2020).
- OpenDataBCN, Barcelona Council. Available online: https://opendata-ajuntament.barcelona.cat (accessed on 17 December 2021).
- Instituto Nacional de Estadística. Available online: https://www.ine.es (accessed on 17 December 2021).
- Otero, A.; Garcia de Yebenes, M.J.; Rodríguez-Laso, A.; Zunzunegui, M.V. Unmet home care needs among community-dwelling elderly people in Spain. Aging Clin. Exp. Res. 2003, 15, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Angus, J.; Kontos, P.; Dyck, I.; Mckeever, P.; Poland, B. The personal significance of home: Habitus and the experience of receiving long-term home care. Sociol. Health Illness 2005, 27, 161–187. [Google Scholar] [CrossRef] [PubMed]
- Chappell, N.; Havens, B.; Hollander, M.J.; Miller, J.A.; McWilliam, C. Comparative Costs of Home Care and Residential Care. Gerontologist 2004, 44, 389–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Wang, J.D. The Determinants of Telehealth Provision: Empirical Evidence from OECD Countries. Int. J. Environ. Res. Public Health 2021, 18, 8288. [Google Scholar] [CrossRef] [PubMed]
- D’herde, J.; Gruijthuijsen, W.; Vanneste, D.; Draulans, V.; Heynen, H. ’I Could Not Manage This Long-Term, Absolutely Not.’ Aging in Place, Informal Care, COVID-19, and the Neighborhood in Flanders (Belgium). Int. J. Environ. Res. Public Health 2021, 18, 6482. [Google Scholar] [CrossRef]
- Fajardo-Bullón, F.; Pérez-Mayo, J.; Esnaola, I. The Association of Interpersonal Relationships and Social Services with the Self-Rated Health of Spanish Homelessness. Int. J. Environ. Res. Public Health 2021, 18, 9392. [Google Scholar] [CrossRef]
- Higi, A.H.; Debelew, G.T.; Dadi, L.S. Perception and Experience of Health Extension Workers on Facilitators and Barriers to Maternal and Newborn Health Service Utilization in Ethiopia: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 10467. [Google Scholar] [CrossRef]
- Islam, M.; Hasan, M.; Wang, X.; Germack, H.; Noor-E-Alam, M. A Systematic Review on Healthcare Analytics: Application and Theoretical Perspective of Data Mining. Healthcare 2018, 6, 54. [Google Scholar] [CrossRef] [Green Version]
- Mollalo, A.; Tatar, M. Spatial Modeling of COVID-19 Vaccine Hesitancy in the United States. Int. J. Environ. Res. Public Health 2021, 18, 9488. [Google Scholar] [CrossRef]
- Stone, K.; McCusker, P.; Davidson, G.; Vicary, S. An Exploratory Survey of Mental Health Social Work in Europe. Int. J. Environ. Res. Public Health 2021, 18, 10462. [Google Scholar] [CrossRef]
- Rodriguez-Pereira, J.; de Armas, J.; Garbujo, L.; Ramalhinho, H. Descriptive analytics, Disabled population, Elder population, Health care services. Int. J. Environ. Res. Public Health 2020, 17, 8071. [Google Scholar] [CrossRef] [PubMed]
- Balan, S.; Otto, J. Big Data Analysis of Home Healthcare Services. Inf. Technol. Manag. Sci. 2017, 19, 53–56. [Google Scholar] [CrossRef]
- Genet, N.; Boerma, W.G.; Kringos, D.S.; Bouman, A.; Francke, A.L.; Fagerström, C.; Melchiorre, M.; Greco, C.; Devillé, W. Home care in Europe: A systematic literature review. BMC Health Serv. Res. 2011, 11, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, K.M.; Noel, S.E.; Lai, C.Q.; Christensen, J.J.; Ordovas, J.M.; Dawson-Hughes, B.; Tucker, K.L.; Parnell, L.D. Diet-derived fruit and vegetable metabolites show sex-specific inverse relationships to osteoporosis status. Bone 2021, 144, 115780. [Google Scholar] [CrossRef] [PubMed]
- Akjiratikarl, C.; Yenradee, P.; Drake, P.R. PSO-based algorithm for home care worker scheduling in the UK. Comput. Ind. Eng. 2007, 53, 559–583. [Google Scholar] [CrossRef]
- Rasmussen, M.S.; Justesen, T.; Dohn, A.; Larsen, J. The home care crew scheduling problem: Preference-based visit clustering and temporal dependencies. Eur. J. Oper. Res. 2012, 219, 598–610. [Google Scholar] [CrossRef] [Green Version]
- Euchi, J. Optimising the routing of home health caregivers: Can a hybrid ant colony metaheuristic provide a solution? Br. J. Healthc. Manag. 2020, 26, 192–196. [Google Scholar] [CrossRef]
- Frifita, S.; Masmoudi, M.; Euchi, J. General variable neighborhood search for home healthcare routing and scheduling problem with time windows and synchronized visits. Electron. Notes Discret. Math. 2017, 58, 63–70. [Google Scholar] [CrossRef]
- Decerle, J.; Grunder, O.; El Hassani, A.H.; Barakat, O. A memetic algorithm for a home health care routing and scheduling problem. Oper. Res. Health Care 2018, 16, 59–71. [Google Scholar] [CrossRef]
- Guericke, D.; Suhl, L. The home health care problem with working regulations. OR Spectrum Heidelberg 2017, 39, 977–1010. [Google Scholar] [CrossRef]
- Statistical Yearbook of the City of Barcelona 2021, Barcelona City Council. Available online: https://ajuntament.barcelona.cat/estadistica/angles/Anuaris/Anuari/index.htm (accessed on 31 January 2022).
- Quintana, D.; Cervantes, A.; Saez, Y.; Isasi, P. Clustering technique for large-scale home care crew scheduling problems. Appl. Intell. 2017, 47, 443–455. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, Y.; Jin, X.; Wang, Z.; Wu, Y. Zhao, D.; Chen, G.; Li, D.; Wang, X. Cao, H.; et al. A circulating miRNA signature as a diagnostic biomarker for non-invasive early detection of breast cancer. Breast Cancer Res. Treat. 2015, 154, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Gao, Y.; Chen, Z.; Zhao, G.; Liu, J.; Wang, X.; Gao, S.; Zhang, D.; Jia, L. Metabolomics analysis of the soapberry (Sapindus mukorossi Gaertn.) pericarp during fruit development and ripening based on UHPLC-HRMS. Sci. Rep. 2021, 11, 11657. [Google Scholar] [CrossRef] [PubMed]
- Julià, A.; Rojas, A. La diversitat de la cura de les persones grans en situació de dependència funcional a Barcelona. Barc. Soc. 2020, 25, 42–57. [Google Scholar]
- Kim, J.; Kim, J.; Han, A. Leisure Time Physical Activity Mediates the Relationship Between Neighborhood Social Cohesion and Mental Health Among Older Adults. J. Appl. Gerontol. 2020, 39, 292–300. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D.; Ahrentzen, S.; Feng, H. Exploring the inner relationship among neighborhood environmental factors affecting quality of life of older adults based on SLR–ISM method. J. Hous. Built Environ. 2020, 35, 215–242. [Google Scholar] [CrossRef]
- Julià, A.; Escapa, S.; Gallo, P. Influence of socio-economic profile of neighbourhoods on the selection of home care strategies for older dependants. Ageing Soc. 2021, 1–19. [Google Scholar] [CrossRef]
- Safian, N.; Shah, S.A.; Mansor, J.; Mohammad, Z.; Nurumal, S.R.; Ibadullah, W.A.H.W.; Ahmad, S.; Shobugawa, Y. Factors Associated with the Need for Assistance among the Elderly in Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 730. [Google Scholar] [CrossRef]
- Pardo-Garcia, I.; Amo-Saus, E.; Moya-Martinez, P. Socioeconomic and Lifestyle Factors Related to Cost and Frequency of Hospitalization in European Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 2833. [Google Scholar] [CrossRef]
- Rodríguez-Sánchez, B.; Pascual Sáez, M.; Cantarero-Prieto, D. Dependent, Poorer, and More Care-Demanding? An Analysis of the Relationship between Being Dependent, Household Income, and Formal and Informal Care Use in Spain. Int. J. Environ. Res. Public Health 2021, 18, 4339. [Google Scholar] [CrossRef]
- Aung, T.N.N.; Aung, M.N.; Moolphate, S.; Koyanagi, Y.; Ichikawa, M.; Supakankunti, S.; Yuasa, M. Estimating Service Demand for Intermediary Care at a Community Integrated Intermediary Care Center among Family Caregivers of Older Adults Residing in Chiang Mai, Northern Thailand. Int. J. Environ. Res. Public Health 2021, 18, 6087. [Google Scholar] [CrossRef] [PubMed]
- Sarasa, S.; Porcel, S.; Navarro-Varas, L. L’impacte social de la crisi a l’Àrea Metropolitana de Barcelona i a Catalunya. Pap. Regió Metrop. Barcelona Territ. EstratèGies, Planejament 2013, 10–87. Available online: https://raco.cat/index.php/PapersIERMB/article/view/265059 (accessed on 3 February 2022).
- Hillcoat-Nalletamby, S. ‘Pathways to choice’ of care setting. Ageing Soc. 2019, 39, 277–306. [Google Scholar] [CrossRef] [Green Version]
- Morilla-Luchena, A.; Muñoz-Moreno, R.; Chaves-Montero, A.; Vázquez-Aguado, O. Telework and Social Services in Spain during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 725. [Google Scholar] [CrossRef] [PubMed]
- Inzitari, M.; Risco, E.; Cesari, M. Nursing Homes and Long Term Care After COVID-19: A New ERA? J. Nutr. Health Aging 2020, 24, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Mosallanezhad, B.; Chouhan, V.K.; Paydar, M.M.; Hajiaghaei-Keshteli, M. Disaster relief supply chain design for personal protection equipment during the COVID-19 pandemic. Appl. Soft Comput. 2021, 112, 107809. [Google Scholar] [CrossRef]
- Kimes, P.K.; Liu, Y.; Hayes, D.N.; Marron, J.S. Statistical Significance for Hierarchical Clustering. Biometrics 2017, 73, 811–821. [Google Scholar] [CrossRef] [Green Version]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Fathollahi-Fard, A.; Govindan, K.; Hajiaghaei-Keshteli, M.; Ahmadi, A. A green home health care supply chain: New modified simulated annealing algorithms. J. Clean. Prod. 2019, 240, 118200. [Google Scholar] [CrossRef]
- Frifita, S.; Masmoudi, M. VNS methods for Home Care routing and scheduling problem with Temporal Dependencies, and Multiple Structures and Specialties. Int. Trans. Oper. Res. 2018, 27, 291–313. [Google Scholar] [CrossRef] [Green Version]
- Fathollahi-Fard, A.M.; Hajiaghaei-Keshteli, M.; Tavakkoli-Moghaddam, R.; Smith, N.R. Bi-level programming for home health care supply chain considering outsourcing. J. Ind. Inf. Integr. 2022, 25, 100246. [Google Scholar] [CrossRef]
- Chouhan, V.K.; Khan, S.H.; Hajiaghaei-Keshteli, M. Sustainable planning and decision-making model for sugarcane mills considering environmental issues. J. Environ. Manag. 2022, 303, 114252. [Google Scholar] [CrossRef] [PubMed]








| Data Source | Last Update | Features |
|---|---|---|
| INE (Public) | 2018–2020 | Population/age/gender/economic |
| OpenDataBCN (Public) | 2018–2020 | Live alone/disability |
| BCN Council (Private) | 2019–2020 | Volume and type of service/SADEP and SAD |
| Users/dependency/economic/disability |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badell, D.; de Armas, J.; Julià, A. Impact of Socioeconomic Environment on Home Social Care Service Demand and Dependent Users. Int. J. Environ. Res. Public Health 2022, 19, 2053. https://doi.org/10.3390/ijerph19042053
Badell D, de Armas J, Julià A. Impact of Socioeconomic Environment on Home Social Care Service Demand and Dependent Users. International Journal of Environmental Research and Public Health. 2022; 19(4):2053. https://doi.org/10.3390/ijerph19042053
Chicago/Turabian StyleBadell, Daniel, Jesica de Armas, and Albert Julià. 2022. "Impact of Socioeconomic Environment on Home Social Care Service Demand and Dependent Users" International Journal of Environmental Research and Public Health 19, no. 4: 2053. https://doi.org/10.3390/ijerph19042053