
Developing a Short Assessment of Environmental Health Literacy (SA-EHL)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Scale Development, Item Generation
2.2. Expert Review and Inclusion of Validation Items
2.3. Data Collection and Validation
2.4. Measures
2.4.1. Socio-Demographics
2.4.2. Short Assessment of Health Literacy (SAHL)
2.4.3. Short Assessment of Environmental Health Literacy (SA-EHL)
2.4.4. Statistical Analysis
2.4.5. Human Subjects’ Protection
3. Results
3.1. Univariate and Scale Diagnosis
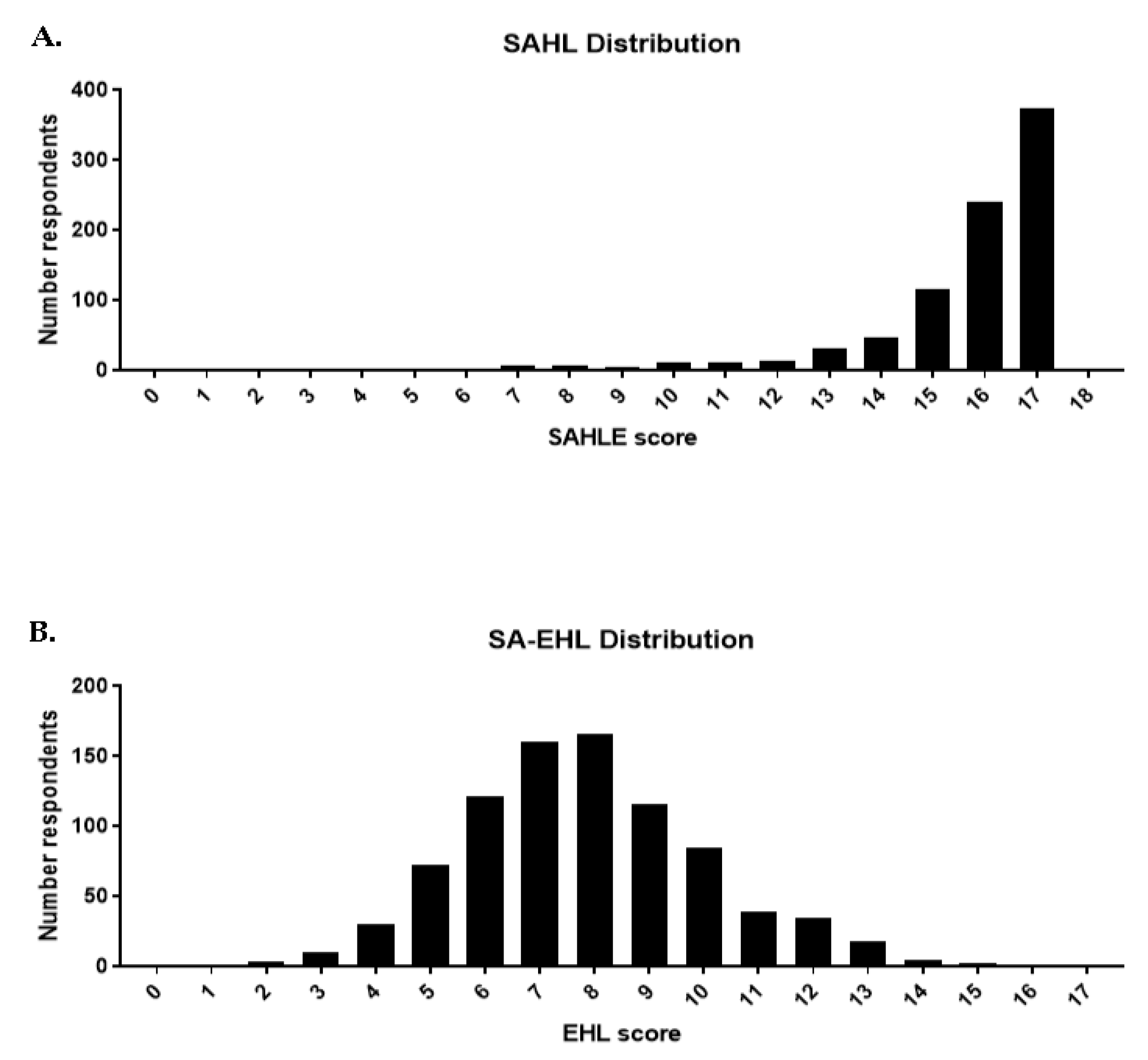
3.1.1. SAHL Univariate and Scale Diagnosis
3.1.2. SA-EHL Univariate and Scale Diagnosis
3.2. Criterion-Related Validity
3.3. Construct Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Finn, S.; O’Fallon, L. The emergence of environmental health literacy—From its roots to its future potential. Environ. Health Perspect. 2017, 125, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Hoover, A.G. Defining environmental health literacy. In Environmental Health Literacy; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–18. [Google Scholar]
- Gray, K.M.; Lindsey, M. Measuring environmental health literacy. In Environmental Health Literacy; Springer: Berlin/Heidelberg, Germany, 2019; pp. 19–43. [Google Scholar]
- Gray, K.M. From content knowledge to community change: A review of representations of environmental health literacy. Int. J. Environ. Res. Public Health 2018, 15, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, J.K.; Hendrickson, K.C.; Ercolano, E.; Quackenbush, R.; Dixon, J.P. The environmental health engagement profile: What people think and do about environmental health. Public Health Nurs. 2009, 26, 460–473. [Google Scholar] [CrossRef]
- Lichtveld, M.Y.; Covert, H.H.; Sherman, M.; Shankar, A.; Wickliffe, J.K.; Alcala, C.S. Advancing environmental health literacy: Validated scales of general environmental health and environmental media-specific knowledge, attitudes and behaviors. Int. J. Environ. Res. Public Health 2019, 16, 4157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratnapradipa, D.; Middleton, W.K.; Wodika, A.B.; Brown, S.L.; Preihs, K. What does the public know about environmental health? A qualitative approach to refining an environmental health awareness instrument. J. Environ. Health 2015, 77, 22–29. [Google Scholar] [PubMed]
- Irvin, V.L.; Rohlman, D.; Vaughan, A.; Amantia, R.; Berlin, C.; Kile, M.L. Development and validation of an environmental health literacy assessment screening tool for domestic well owners: The water environmental literacy level scale (WELLS). Int. J. Environ. Res. Public Health 2019, 16, 881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, K.M.; Triana, V.; Lindsey, M.; Richmond, B.; Hoover, A.G.; Wiesen, C. Knowledge and Beliefs Associated with Environmental Health Literacy: A Case Study Focused on Toxic Metals Contamination of Well Water. Int. J. Environ. Res. Public Health 2021, 18, 9298. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. Health Literacy Measurement Tools (Revised). Available online: https://www.ahrq.gov/health-literacy/research/tools/index.html (accessed on 5 December 2021).
- Lee, S.Y.D.; Stucky, B.D.; Lee, J.Y.; Rozier, R.G.; Bender, D.E. Short assessment of health literacy—Spanish and English: A comparable test of health literacy for Spanish and English speakers. Health Serv. Res. 2010, 45, 1105–1120. [Google Scholar] [CrossRef] [PubMed]
- Castro-Sánchez, E.; Vila-Candel, R.; Soriano-Vidal, F.J.; Navarro-Illana, E.; Díez-Domingo, J. Influence of health literacy on acceptance of influenza and pertussis vaccinations: A cross-sectional study among Spanish pregnant women. BMJ Open 2018, 8, e022132. [Google Scholar] [CrossRef] [Green Version]
- Stonbraker, S.; Smaldone, A.; Luft, H.; Cushman, L.F.; Lerebours Nadal, L.; Halpern, M.; Larson, E. Associations between health literacy, HIV-related knowledge, and information behavior among persons living with HIV in the Dominican Republic. Public Health Nurs. 2018, 35, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Fong, H.-f.; Rothman, E.F.; Garner, A.; Ghazarian, S.R.; Morley, D.S.; Singerman, A.; Bair-Merritt, M.H. Association Between Health Literacy and Parental Self-Efficacy among Parents of Newborn Children. J. Pediatrics 2018, 202, 265–271.e263. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Codina, O.; Juvinyà-Canal, D.; Amil-Bujan, P.; Bertran-Noguer, C.; González-Mestre, M.A.; Masachs-Fatjo, E.; Santaeugènia, S.J.; Magrinyà-Rull, P.; Saltó-Cerezuela, E. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health 2019, 19, 1122. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development: Theory and applications; Sage Publications: Thousand Oaks, CA, USA, 2016; Volume 26. [Google Scholar]
- Hauser, D.J.; Schwarz, N. Attentive Turkers: MTurk participants perform better on online attention checks than do subject pool participants. Behav. Res. Methods 2016, 48, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Difallah, D.; Filatova, E.; Ipeirotis, P. Demographics and dynamics of mechanical turk workers. In Proceedings of the Eleventh ACM International Conference on Web Search and Data Mining, Marina Del Ray, CA, USA, 5–9, February, 2018; pp. 135–143. [Google Scholar]
- Huff, C.; Tingley, D. “Who are these people?” Evaluating the demographic characteristics and political preferences of MTurk survey respondents. Res. Politics 2015, 2, 2053168015604648. [Google Scholar] [CrossRef]
- Ipeirotis, P.G. Analyzing the amazon mechanical turk marketplace. XRDS Crossroads ACM Mag. Stud. 2010, 17, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Behaviorial Risk Factor Surveillance System-BRFSS Questionnaires. Available online: https://www.cdc.gov/brfss/questionnaires/index.htm (accessed on 9 February 2022).
- Ramirez-Andreotta, M. Engaging with Ethnically Diverse Community Groups. In Environmental Health Literacy; Finn, S., O’Fallon, L.R., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 67–96. [Google Scholar] [CrossRef]
- Somerville, R.C. Communicating the science of climate change. Phys. Today 2012. Available online: https://climatecommunication.org/wp-content/uploads/2011/10/Somerville-Hassol-Physics-Today-2011.pdf (accessed on 9 February 2022.). [CrossRef] [Green Version]
- Baccolini, V.; Rosso, A.; Di Paolo, C.; Isonne, C.; Salerno, C.; Migliara, G.; Prencipe, G.; Massimi, A.; Marzuillo, C.; De Vito, C. What is the Prevalence of Low Health Literacy in European Union Member States? A Systematic Review and Meta-analysis. J. Gen. Intern. Med. 2021, 36, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, M.; Chen, S.-R.; Ben, R.; Manoogian, M.; Spradlin, J. Defining Environmental Health Literacy. Int. J. Environ. Res. Public Health 2021, 18, 11626. [Google Scholar] [CrossRef]
- Brach, C.; Keller, D.; Hernandez, L.M.; Baur, C.; Parker, R.; Dreyer, B.; Schyve, P.; Lemerise, A.J.; Schillinger, D. Ten attributes of health literate health care organizations. NAM Perspect. 2012. Available online: https://nam.edu/wp-content/uploads/2015/06/BPH_Ten_HLit_Attributes.pdf (accessed on 9 February 2022). [CrossRef]
- Weiss, B.D. Assessing Patients’ Healthy Literacy Skills Not Necessary in Clinical Practice. Am. Fam. Physician 2018, 97, 768. [Google Scholar] [PubMed]
- Symanski, E.; Han, H.A.; Han, I.; McDaniel, M.; Whitworth, K.W.; McCurdy, S.; Perkison, W.B.; Rammah, A.; Lewis, P.G.T.; Delclos, G.L. Responding to natural and industrial disasters: Partnerships and lessons learned. Disaster Med. Public Health Prep. 2021, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Marfori, M.T.; Campbell, S.L.; Garvey, K.; McKeown, S.; Veitch, M.; Wheeler, A.J.; Borchers-Arriagada, N.; Johnston, F.H. Public Health Messaging During Extreme Smoke Events: Are We Hitting the Mark? Front. Public Health 2020, 8, 465. [Google Scholar] [CrossRef] [PubMed]
- Van Deventer, D.; Marecaux, J.; Doubleday, A.; Errett, N.; Isaksen, T.M.B. Wildfire smoke risk communication efficacy: A content analysis of Washington State’s 2018 statewide smoke event public health messaging. J. Public Health Manag. Pract. 2021, 27, 607–614. [Google Scholar] [CrossRef]
- Leroy, G.; Kauchak, D. The effect of word familiarity on actual and perceived text difficulty. J. Am. Med. Inform. Assoc. 2014, 21, e169–e172. [Google Scholar] [CrossRef] [Green Version]
- Ramirez-Andreotta, M.D.; Brody, J.G.; Lothrop, N.; Loh, M.; Beamer, P.I.; Brown, P. Improving Environmental Health Literacy and Justice through Environmental Exposure Results Communication. Int. J. Environ. Res. Public Health 2016, 13, 690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohlman, D.; Donatuto, J.; Heidt, M.; Barton, M.; Campbell, L.; Anderson, K.A.; Kile, M.L. A case study describing a community-engaged approach for evaluating polycyclic aromatic hydrocarbon exposure in a native American community. Int. J. Environ. Res. Public Health 2019, 16, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohlman, D.; Frey, G.; Kile, M.L.; Harper, B.; Harris, S.; Motorykin, O.; Simonich, S.L.M.; Harding, A.K. Communicating Results of a Dietary Exposure Study Following Consumption of Traditionally Smoked Salmon. Environ. Justice 2016, 9, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brody, J.G.; Brown, P.; Morello-Frosch, R.A. Returning chemical exposure results to individuals and communities. In Environmental Health Literacy; Springer: Berlin/Heidelberg, Germany, 2019; pp. 135–163. [Google Scholar] [CrossRef]
- Brown, P.; Clark, S.; Zimmerman, E.; Valenti, M.; Miller, M.D. Health Professionals’ Environmental Health Literacy. In Environmental Health Literacy; Finn, S., O’Fallon, L.R., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 196–227. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Univariate Distribution | SAHL a | SA-EHL b |
|---|---|---|---|
| Total sample | n = 864 c | ||
| Mean (SD) | Correlation | Correlation | |
| Age * | 38 (11.6) | 0.16 (p < 0.01) | 0.03 (p = 0.35) |
| Percentage (n) | Mean (SD) | Mean (SD) | |
| Gender * | p < 0.01 | p = 0.9 | |
| Male | 41.3% (357) | 15.4 (2.1) | 7.9 (2.1) |
| Female | 57.9% (500) | 15.9 (1.7) | 7.8 (2.3) |
| Prefer not to answer | <1% (5) | 15.6 (1.7) | 7.4 (1.8) |
| Missing | <1% (2) | 15.5 (2.1) | 7.5 (0.7) |
| Ethnicity | |||
| Hispanic or Latino | 6.8% (59) | 15.3 (2.2) | 7.6 (2.3) |
| Not Hispanic or Latino | 93.1% (804) | 15.7 (1.9) | 7.9 (2.2) |
| Prefer not to answer | <1% (1) | 14 (0) | 7 (0) |
| Missing | 0% (0) | --- | |
| Education * | p ≤ 0.001 | p ≤ 0.001 | |
| College Graduate | 52% (449) | 15.7 (1.8) | 8.1 (2.3) |
| Some College | 34.5% (298) | 15.8 (1.8) | 7.7 (2.1) |
| High School Graduate | 12.4% (107) | 15.4 (2.2) | 7.3 (2.2) |
| Some High School | <1% (2) | 13.5 (4.9) | 6 (4.2) |
| Prefer not to answer | <1% (6) | 12 (3.5) | 7 (2.9) |
| Missing | <1% (2) | 15 (1.8) | 8.5 (1.3) |
| Income | p = 0.36 | p = 0.26 | |
| USD 0–35,999 | 35.2% (304) | 15.6 (2.1) | 7.4 (2.2) |
| USD 36,000–50,000 | 19.2% (166) | 15.5 (1.9) | 7.7 (2.4) |
| USD 51,000–75,999 | 19.4% (168) | 15.9 (1.6) | 7.8 (2.3) |
| USD 76,000 or higher | 24.0% (207) | 15.7 (1.7) | 8.1 (2.1) |
| Prefer not to answer | 2.2% (19) | 15.6 (2.4) | 7.4 (2.0) |
| Missing | 0% (0) | --- | --- |
| Rent/own | p = 0.7 | p = 0.6 | |
| Own | 49.2% (425) | 15.8 (1.8) | 7.9 (2.2) |
| Rent | 43.9% (379) | 15.6 (2.1) | 7.7 (2.3) |
| Other arrangement | 6.8% (59) | 15.8 (1.8) | 7.8 (2.0) |
| Missing | <1% (1) | 15 (0) | 9 (0) |
| Marital Status * | p ≤ 0.0001 | p = 0.72 | |
| Married | 44.5% (383) | 15.6 (2.0) | 7.8 (2.2) |
| Divorced | 8.6% (74) | 16.2 (1.1) | 7.9 (2.3) |
| Widowed | 1.4% (12) | 15.8 (2.1) | 7.8 (1.3) |
| Separated | 1.5% (13) | 16.7 (0.5) | 8.2 (2.0) |
| Never married | 28.6% (247) | 15.4 (2.1) | 7.9 (2.2) |
| Unmarried couple | 14.2% (123) | 16.1 (1.3) | 7.8 (2.4) |
| Prefer not to answer | 1.0% (9) | 13.2 (3.8) | 6.7 (2.5) |
| Missing | <1.0% (3) | --- | --- |
| SAHL-E | n | % | DIFF | |
|---|---|---|---|---|
| Dose | Amount | 843 | 97.6 | −3.28 |
| Sleep | 20 | 2.3 | ||
| Don’t know/skipped | 1 | <1.0 | ||
| Kidney | Urine | 797 | 92.3 | −3.10 |
| Fever | 24 | 2.8 | ||
| Don’t know/skipped | 43 | 5.0 | ||
| Medication | Treatment | 832 | 96.3 | −3.0 |
| Instrument | 29 | 3.4 | ||
| Don’t know/skipped | 3 | <1.0 | ||
| Miscarriage | Loss | 847 | 98.0 | −3.87 |
| Marriage | 9 | 1.0 | ||
| Don’t know/skipped | 8 | <1.0 | ||
| Alcoholism | Addiction | 814 | 94.2 | −2.60 |
| Recreation | 45 | 5.2 | ||
| Don’t know/skipped | 5 | <1.0 | ||
| Hormones | Growth | 792 | 91.7 | −2.65 |
| Harmony | 42 | 4.9 | ||
| Don’t know/skipped | 30 | 3.5 | ||
| Pregnancy | Birth | 823 | 95.3 | −2.95 |
| Childhood | 29 | 3.4 | ||
| Don’t know/skipped | 12 | 1.4 | ||
| Seizure | Dizzy | 781 | 90.4 | −3.14 |
| Calm | 23 | 2.7 | ||
| Don’t know/skipped | 60 | 6.9 | ||
| Abnormal | Different | 834 | 96.5 | −3.10 |
| Similar | 25 | 2.9 | ||
| Don’t know/skipped | 5 | <1.0 | ||
| Nerves | Anxiety | 838 | 97.0 | −3.24 |
| Bored | 21 | 2.4 | ||
| Don’t know/skipped | 5 | <1.0 | ||
| Constipation | Blocked | 814 | 94.2 | −2.64 |
| Loose | 43 | 5.0 | ||
| Don’t know/skipped | 7 | <1.0 | ||
| Hemorrhoid | Veins | 705 | 81.6 | −2.64 |
| Heart | 38 | 4.4 | ||
| Don’t know/skipped | 121 | 14 | ||
| Syphilis | Condom | 573 | 66.3 | −1.12 |
| Contraceptive | 173 | 20.0 | ||
| Don’t know/skipped | 118 | 13.7 | ||
| Directed | Instruction | 750 | 86.8 | −1.85 |
| Decision | 99 | 11.5 | ||
| Don’t know/skipped | 15 | 1.7 | ||
| Occupation | Work | 833 | 96.4 | −3.03 |
| Education | 27 | 3.1 | ||
| Don’t know/skipped | 4 | <1.0 | ||
| Nutrition | Healthy | 838 | 97.0 | −3.51 |
| Soda | 15 | 1.7 | ||
| Don’t know/skipped | 11 | 1.3 | ||
| Infection | Plant | 21 | 2.4 | 3.14 |
| Virus | 833 | 96.4 | ||
| Don’t know/skipped | 10 | 1.2 | ||
| Diagnosis | Evaluation | 818 | 94.7 | −2.70 |
| Recovery | 40 | 4.6 | ||
| Don’t know/skipped | 6 | <1.0 | ||
| SA-EHL | n | % | DIFF | |
| Response a | Endpoint | 36 | 4.2 | --- |
| Answer | 809 | 93.6 | ||
| Don’t know/skipped | 19 | 2.2 | ||
| Exposure a | Contact | 819 | 94.8 | --- |
| Consumed | 32 | 3.7 | ||
| Don’t know/skipped | 13 | 1.5 | ||
| Concentration | Amount | 651 | 75.4 | −2.69 |
| Strong | 206 | 23.8 | ||
| Don’t know/skipped | 7 | 0.8 | ||
| Chemical | Substance | 637 | 73.7 | −2.56 |
| Solution | 214 | 24.8 | ||
| Don’t know/skipped | 13 | 1.5 | ||
| Acute | Short | 251 | 29.1 | 2.00 |
| Sharp | 588 | 68.1 | ||
| Don’t know/skipped | 25 | 2.9 | ||
| Chronic | Long | 649 | 75.1 | −2.70 |
| Disease | 205 | 23.7 | ||
| Don’t know/skipped | 10 | 1.2 | ||
| Risk | Possibility | 192 | 22.2 | 2.92 |
| Hazard | 670 | 77.6 | ||
| Don’t know/skipped | 2 | 0.2 | ||
| Particulate a | Dust | 553 | 64.0 | --- |
| Sand | 211 | 24.4 | ||
| Don’t know/skipped | 100 | 11.6 | ||
| Aerosol | Particle | 131 | 15.2 | 3.96 |
| Spray | 717 | 83.0 | ||
| Don’t know/skipped | 16 | 1.9 | ||
| Background | Natural | 192 | 22.1 | 2.65 |
| Explanation | 589 | 68.2 | ||
| Don’t know/skipped | 84 | 9.7 | ||
| Fraction | Amount | 467 | 54.1 | −0.43 |
| Division | 389 | 45.0 | ||
| Don’t know/skipped | 8 | 0.9 | ||
| Media | Environment | 227 | 26.3 | 2.13 |
| Digital | 566 | 65.5 | ||
| Don’t know/skipped | 71 | 8.2 | ||
| Organic | Carbon | 302 | 35.0 | 1.33 |
| Vegetables | 533 | 61.7 | ||
| Don’t know/skipped | 29 | 3.4 | ||
| Remediate a | Clean | 214 | 24.8 | --- |
| Repair | 533 | 61.7 | ||
| Don’t know/skipped | 117 | 13.5 | ||
| Susceptibility | Risk | 190 | 22.0 | 2.94 |
| Vulnerable | 665 | 77.0 | ||
| Don’t know/skipped | 9 | 1.0 | ||
| Safe | Secure | 570 | 66.0 | −1.68 |
| Clean | 280 | 32.4 | ||
| Don’t know/skipped | 14 | 1.6 | ||
| Treatment b | Fix | 715 | 82.8 | −4.04 |
| Drug | 127 | 14.7 | ||
| Don’t know/skipped | 22 | 2.6 | ||
| Monitor b | Watch | 767 | 88.8 | −4.84 |
| Investigate | 96 | 11.1 | ||
| Don’t know/skipped | 1 | 0.1 | ||
| Contaminant b | Pollutant | 751 | 86.9 | −4.56 |
| Not belong | 106 | 12.3 | ||
| Don’t know/skipped | 7 | 0.8 | ||
| Level | Amount | 711 | 82.3 | −3.75 |
| Even | 143 | 16.6 | ||
| Don’t know/skipped | 10 | 1.2 | ||
| Test | Measure | 575 | 66.6 | −1.64 |
| Exam | 286 | 33.1 | ||
| Don’t know/skipped | 3 | 0.4 | ||
| Source | Origin | 718 | 83.1 | −3.82 |
| Reference | 140 | 16.2 | ||
| Don’t know/skipped | 6 | 0.7 | ||
| Uncertainty b | Range | 112 | 13.0 | 4.41 |
| Unsure | 743 | 86.0 | ||
| Don’t know/skipped | 9 | 1.0 | ||
| Artifact a | Effect | 170 | 19.7 | --- |
| Remainder | 565 | 65.4 | ||
| Don’t know/skipped | 129 | 14.9 | ||
| Manipulation | Process | 149 | 17.3 | 3.54 |
| Change | 682 | 78.9 | ||
| Don’t know/skipped | 33 | 3.8 | ||
| Error | Difference | 159 | 18.4 | 3.46 |
| Mistake | 698 | 80.8 | ||
| Don’t know/skipped | 7 | 0.8 | ||
| Threshold a | Concentration | 63 | 7.3 | --- |
| Limit | 783 | 90.6 | ||
| Don’t know/skipped | 18 | 2.1 | ||
| Variability a | Range | 795 | 92.0 | --- |
| Error | 64 | 7.4 | ||
| Don’t know/skipped | 5 | 0.6 | ||
| Effects b | Change | 759 | 87.9 | −6.00 |
| Move | 57 | 6.6 | ||
| Don’t know/skipped | 48 | 5.6 | ||
| Chance a | Accidental | 779 | 90.2 | --- |
| Probability | 82 | 9.5 | ||
| Don’t know/skipped | 3 | 0.4 |
| Variable | Health Literacy (SAHL) Title 3 | Environmental Health Literacy (SA-EHL) | ||
|---|---|---|---|---|
| Scale Range | % Respondents | Scale Range | % Respondents | |
| SAHL Criteria 1 | ||||
| Low | 0–13 | 10.1 | 0–13 | 99.2 |
| High | 14–18 | 89.9 | 14–17 | 0.8 |
| Tertile criteria 2 | ||||
| Low | 0–6 | 0.1 | 0–6 | 27.6 |
| Medium | 7–12 | 6.4 | 7–12 | 69.6 |
| High | 13–18 | 93.5 | 13–17 | 2.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rohlman, D.; Kile, M.L.; Irvin, V.L. Developing a Short Assessment of Environmental Health Literacy (SA-EHL). Int. J. Environ. Res. Public Health 2022, 19, 2062. https://doi.org/10.3390/ijerph19042062
Rohlman D, Kile ML, Irvin VL. Developing a Short Assessment of Environmental Health Literacy (SA-EHL). International Journal of Environmental Research and Public Health. 2022; 19(4):2062. https://doi.org/10.3390/ijerph19042062
Chicago/Turabian StyleRohlman, Diana, Molly L. Kile, and Veronica L. Irvin. 2022. "Developing a Short Assessment of Environmental Health Literacy (SA-EHL)" International Journal of Environmental Research and Public Health 19, no. 4: 2062. https://doi.org/10.3390/ijerph19042062
APA StyleRohlman, D., Kile, M. L., & Irvin, V. L. (2022). Developing a Short Assessment of Environmental Health Literacy (SA-EHL). International Journal of Environmental Research and Public Health, 19(4), 2062. https://doi.org/10.3390/ijerph19042062