
Behavioral Assessment and Treatment via Telehealth for Children with Autism: From Local to Global Clinical Applications

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Settings and Materials
2.2.1. Participants
2.2.2. Therapists
2.2.3. Interpreters
2.3. General Study Procedures
2.3.1. Telehealth Visits
2.3.2. Functional Analysis
2.3.3. Functional Communication Training
2.4. Dependent Variables and Interobserver Agreement
2.4.1. Challenging Behavior and Independent Communication
2.4.2. Interobserver Agreement
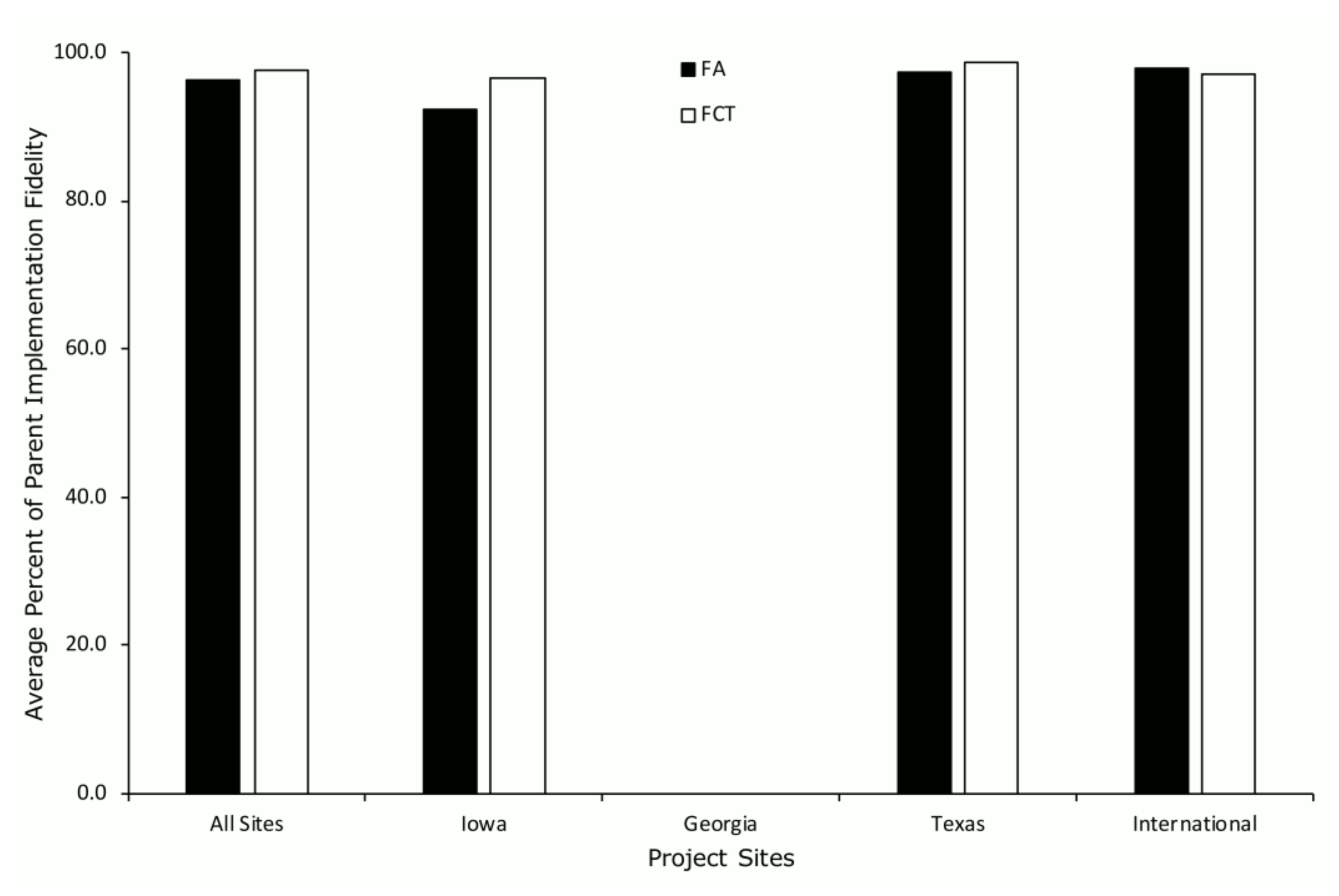
2.5. Procedural Fidelity and Interobserver Agreement
2.6. Data Analysis
2.6.1. Project Status Outcomes
2.6.2. Outcomes for Completers
2.6.3. Outcomes for Non-Completers
2.6.4. Outcomes for Completers and Non-Completers
3. Results
3.1. Participants
3.1.1. Child Participants
3.1.2. Behavior Therapists
3.1.3. Interpreters
3.2. Outcomes
3.2.1. Outcomes for Completers
3.2.2. Outcomes for Non-Completers
3.2.3. Outcomes for Completers and Non-Completers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, J.O.; Heron, T.E.; Heward, W.L. Applied Behavior Analysis, 3rd ed.; Pearson Education: Hoboken, NJ, USA, 2020. [Google Scholar]
- Steinbrenner, J.R.; Hume, K.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, Ş.; Savage, M.N. Evidence-Based Practices for Children, Youth, and Young Adults with Autism; The University of North Carolina at Chapel Hill, Frank Porter Graham Child Development Institute, National Clearinghouse on Autism Evidence and Practice Review Team: Chapel Hill, NC, USA, 2020. [Google Scholar]
- Beavers, G.A.; Iwata, B.A.; Lerman, D.C. Thirty years of research on the functional analysis of problem behavior. J. Appl. Behav. Anal. 2013, 46, 1–21. [Google Scholar] [CrossRef]
- Iwata, B.A.; Dorsey, M.F.; Slifer, K.J.; Bauman, K.E.; Richman, G.S. Toward a functional analysis of self-injury. J. Appl. Behav. Anal. 1994, 27, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Carr, E.G.; Durand, V.M. Reducing behavior problems through functional communication training. J. Appl. Behav. Anal. 1985, 18, 111–126. [Google Scholar] [CrossRef] [Green Version]
- Tiger, J.H.; Hanley, G.P.; Bruzek, J. Functional communication training: A review and practical guide. Behav. Anal. Pract. 2008, 1, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Cooper, L.J.; Wacker, D.P.; Sasso, G.M.; Reimers, T.M.; Donn, L.K. Using parents as therapists to evaluate appropriate behavior of their children: Applicatiton to a tertiary diagnostic clinic. J. Appl. Behav. Anal. 1990, 23, 285–296. [Google Scholar] [CrossRef] [Green Version]
- Kurtz, P.F.; Chin, M.D.; Huete, J.M.; Tarbox, R.S.F.; O’Connor, J.T.; Paclawskyj, T.R.; Rush, K.S. Functional analysis and treatment of self-injurious behavior in young children: A summary of 30 cases. J. Appl. Behav. Anal. 2003, 36, 205–219. [Google Scholar] [CrossRef] [Green Version]
- Northup, J.; Wacker, D.P.; Berg, W.K.; Kelly, L.; Sasso, G.; DeRaad, A. The treatment of severe behavior problems in school settings using a technical assistance model. J. Appl. Behav. Anal. 1994, 27, 33–47. [Google Scholar] [CrossRef] [Green Version]
- Rooker, G.W.; Jessel, J.; Kurtz, P.F.; Hagopian, L.P. Functional communication training with and without alternative reinforcement and punishment: An analysis of 58 applications. J. Appl. Behav. Anal. 2013, 46, 708–722. [Google Scholar] [CrossRef] [PubMed]
- Wacker, D.P.; Berg, W.K.; Harding, J.W.; Derby, K.M.; Asmus, J.M.; Healy, A. Evaluation and long-term treatment of aberrant behavior displayed by young children with disabilities. J. Dev. Behav. Pediatrics 1998, 19, 260–266. [Google Scholar] [CrossRef]
- Wacker, D.P.; Schieltz, K.M.; Berg, W.K.; Harding, J.W.; Padilla Dalmau, Y.C.; Lee, J.F. The long-term effects of functional communication training conducted in young children’s home settings. Educ. Treat. Child. 2017, 40, 43–56. [Google Scholar] [CrossRef] [PubMed]
- American Telemedicine Association Telehealth: Defining 21st Century Care. Available online: https://www.americantelemed.org/resource/why-telemedicine/ (accessed on 12 December 2021).
- Hurst, E.J. Evolutions in telemedicine: From smoke signals to mobile health solutions. J. Hosp. Librariansh. 2016, 16, 174–185. [Google Scholar] [CrossRef]
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, S.; Wacker, D.; Suess, A.; Schieltz, K.; Pelzel, K.; Kopelman, T.; Lee, J.; Romani, P.; Waldron, D. Telehealth and autism: Treating challenging behavior at lower cost. Pediatrics 2016, 137, S167–S175. [Google Scholar] [CrossRef] [Green Version]
- Schieltz, K.M.; Wacker, D.P. Functional assessment and function-based treatment delivered via telehealth: A brief summary. J. Appl. Behav. Anal. 2020, 53, 1242–1258. [Google Scholar] [CrossRef]
- Tsami, L.; Lerman, D.; Toper-Korkmaz, O. Effectiveness and acceptability of parent training via telehealth among families around the world. J. Appl. Behav. Anal. 2019, 52, 1113–1129. [Google Scholar] [CrossRef]
- Wacker, D.P.; Lee, J.F.; Padilla Dalmau, Y.C.; Kopelman, T.G.; Lindgren, S.D.; Kuhle, J.; Pelzel, K.E.; Waldron, D.B. Conducting functional analyses of problem behavior via telehealth. J. Appl. Behav. Anal. 2013, 46, 31–46. [Google Scholar] [CrossRef] [Green Version]
- Wacker, D.P.; Lee, J.F.; Padilla Dalmau, Y.C.; Kopelman, T.G.; Lindgren, S.D.; Kuhle, J.; Pelzel, K.E.; Dyson, S.; Schieltz, K.M.; Waldron, D.B. Conducting Functional Communication Training via Telehealth to Reduce the Problem Behavior of Young Children with Autism. J. Dev. Phys. Disabil. 2013, 25, 35–48. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, S.; Wacker, D. Comparing Behavioral Assessments Using Telehealth for Children with Autism; US Department of Health and Human Services, National Institutes of Health, National Institute of Mental Health: Washington, DC, USA, 2015. [Google Scholar]
- Bullock, C.E.; Fisher, W.W.; Hagopian, L.P. Description and validation of a computerized behavioral data program: “BDataPro”. Behav. Anal. 2017, 40, 275–285. [Google Scholar] [CrossRef]
- Suess, A.N.; Romani, P.W.; Wacker, D.P.; Dyson, S.M.; Kuhle, J.L.; Lee, J.F.; Lindgren, S.D.; Kopelman, T.G.; Pelzel, K.E.; Waldron, D.B. Evaluating the Treatment Fidelity of Parents Who Conduct In-Home Functional Communication Training with Coaching via Telehealth. J. Behav. Educ. 2014, 23, 34–59. [Google Scholar] [CrossRef]
- Roane, H.S.; Fisher, W.W.; Kelley, M.E.; Mevers, J.L.; Bouxsein, K.J. Using modified visual-inspection criteria to interpret functional analysis outcomes. J. Appl. Behav. Anal. 2013, 46, 130–146. [Google Scholar] [CrossRef]
- Reimers, T.M.; Wacker, D.P.; Cooper, L.J. Evaluation of the acceptability of treatments for children’s behavioral difficulties. Child Fam. Behav. Ther. 1991, 13, 53–71. [Google Scholar] [CrossRef]
- O’Brien, M.J.; Schieltz, K.M.; Berg, W.K.; McComas, J.J.; Wacker, D.P. Delivering Interventions Via Telehealth: Functional Communication Training with a Child with Autism as a Case Example. Res. Pract. Pers. Sev. Disabil. 2021, 46, 53–60. [Google Scholar] [CrossRef]
- O’Brien, M.J.; Pelzel, K.E.; Hendrix, N.M.; Schieltz, K.M.; Miller, K.; Call, N.A.; Tsami, L.; Lerman, D.C.; Berg, W.K.; Kopelman, T.G.; et al. Parent Ratings of Generalized and Indirect Effects of Functional Communication Training for Children with Autism Spectrum Disorder. Behav. Modif. 2021. [Google Scholar] [CrossRef]
- Behavior Analyst Certificatioono Board BACB Certificant Registry. Available online: https://www.bacb.com/services/o.php?page=101135 (accessed on 12 December 2021).
- Machalicek, W.; O’Reilly, M.; Chan, J.M.; Lang, R.; Rispoli, M.; Davis, T.; Shogren, K.; Sigafoos, J.; Lancioni, G.; Antonucci, M.; et al. Using Videoconferencing to Conduct Functional Analysis of Challenging Behavior and Develop Classroom Behavioral Support Plans for Students with Autism. Educ. Train. Dev. Disabil. 2009, 44, 207–217. [Google Scholar]
- Pollard, J.S.; Karimi, K.A.; Ficcaglia, M.B. Ethical considerations in the design and implementation of a telehealth service delivery model. Behav. Anal. Res. Pract. 2017, 17, 298–311. [Google Scholar] [CrossRef]
- Barretto, A.; Wacker, D.P.; Harding, J.; Lee, J.; Berg, W.K. Using telemedicine to conduct behavioral assessments. J. Appl. Behav. Anal. 2006, 39, 333–340. [Google Scholar] [CrossRef]
- Gerow, S.; Radhakrishnan, S.; Akers, J.S.; McGinnis, K.; Swensson, R. Telehealth parent coaching to improve daily living skills for children with ASD. J. Appl. Behav. Anal. 2021, 54, 566–581. [Google Scholar] [CrossRef]
- Schlichenmeyer, K.J.; Roscoe, E.M.; Rooker, G.W.; Wheeler, E.E.; Dube, W.V. Idiosyncratic Variables That Affect Functional Analysis Outcomes: A Review (2001–2010). J. Appl. Behav. Anal. 2013, 46, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Schieltz, K.M.; Romani, P.W.; Wacker, D.P.; Suess, A.N.; Huang, P.; Berg, W.K.; Lindgren, S.D.; Kopelman, T.G. Single-Case Analysis to Determine Reasons for Failure of Behavioral Treatment via Telehealth. Remedial Spec. Educ. 2018, 39, 95–105. [Google Scholar] [CrossRef]
- Jones, S.H.; St. Peter, C.C.; Ruckle, M.M. Reporting of demographic variables in the Journal of Applied Behavior Analysis. J. Appl. Behav. Anal. 2020, 53, 1304–1315. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Sites | All US Sites | Iowa 1 | Georgia 2 | Texas 2 | International 3 |
|---|---|---|---|---|---|---|
| Participants Enrolled (n) | 199 | 152 | 59 | 37 | 56 | 47 |
| Age (in months) | ||||||
| Mean (SD) | 56.4 (20.6) | 51.8 (16.4) | 50.6 (15.1) | 56.4 (16.8) | 49.9 (17.2) | 71.5 (25.4) |
| Range | 20–156 | 20–97 | 20–78 | 22–83 | 20–97 | 24–156 |
| Sex (% male) | 79.9 | 80.9 | 81.4 | 75.7 | 83.9 | 76.6 |
| ASD Diagnosis (%) | 99.0 | 100.0 | 100.0 | 100.0 | 100.0 | 80.4 |
| Race 4 (%) | ||||||
| White | 72.4 | 83.1 | 59.5 | 69.6 | ||
| Black or African American | 13.8 | 5.1 | 32.4 | 10.7 | ||
| American Indian/Alaska Native | 0.7 | 1.7 | 0.0 | 0.0 | ||
| Asian | 7.9 | 3.4 | 2.7 | 16.1 | ||
| Native Hawaiian/Other Pacific Islander | 0.0 | 0.0 | 0.0 | 0.0 | ||
| Two or More Races | 4.6 | 6.8 | 2.7 | 3.6 | ||
| Not Reported | 0.7 | 0.0 | 2.7 | 0.0 | ||
| Country of Origin 5 (%) | ||||||
| Algeria | 2.1 | |||||
| Cameroon | 4.3 | |||||
| China | 2.1 | |||||
| Costa Rica | 2.1 | |||||
| Egypt | 2.1 | |||||
| Ghana | 2.1 | |||||
| Greece | 17.0 | |||||
| India | 4.3 | |||||
| Iran | 2.1 | |||||
| Mexico | 6.4 | |||||
| Morocco | 6.4 | |||||
| Nepal | 2.1 | |||||
| Nigeria | 4.3 | |||||
| Pakistan | 12.8 | |||||
| Russia | 2.1 | |||||
| Saudi Arabia | 6.4 | |||||
| Turkey | 6.4 | |||||
| Ukraine | 2.1 | |||||
| United Kingdom | 2.1 | |||||
| Venezuela | 4.3 | |||||
| Vietnam | 6.4 | |||||
| Ethnicity (%) | ||||||
| Hispanic or Latino | 19.1 | 21.1 | 8.5 | 5.4 | 44.6 | 12.8 |
| One-Way Distance (in km) | ||||||
| Mean | 2484.0 | 134.5 | 220.2 | 114.7 | 57.5 | 10078.5 |
| Range | 4.8–13,928.9 | 4.8–1395.3 | 4.8–1395.3 | 9.7–1044.5 | 4.8–346.0 | 1210.2–13,928.9 |
| Caregiver as Therapist (%) | ||||||
| Father | 6.5 | 5.9 | 8.5 | 0.0 | 7.1 | 8.5 |
| Mother | 93.0 | 93.4 | 91.5 | 100.0 | 91.1 | 91.5 |
| Other | 0.5 | 0.7 | 0.0 | 0.0 | 1.8 | 0.0 |
| Interpreter Used (%) | 13.6 | 0.0 | 0.0 | 0.0 | 0.0 | 57.4 |
| Variables | All Sites | Iowa | Georgia | Texas | International |
|---|---|---|---|---|---|
| Behavior Therapists 1 (n) | 10 | 6 | 1 | 1 | 3 |
| Age (in years) | |||||
| Mean | 38.3 | 40.0 | 38.0 | 44.0 | 35.0 |
| Range | 24–53 | 28–53 | 24–44 | ||
| Sex (% male) | 20.0 | 33.3 | 0.0 | 0.0 | 0.0 |
| Race 2 (%) | |||||
| White | 60.0 | 83.3 | 100.0 | 0.0 | 0.0 |
| Asian | 10.0 | 16.7 | 0.0 | 0.0 | 0.0 |
| Country of Origin 3 (%) | |||||
| India | 10.0 | 0.0 | 0.0 | 0.0 | 33.3 |
| Greece | 10.0 | 0.0 | 0.0 | 100.0 | 33.3 |
| Turkey | 10.0 | 0.0 | 0.0 | 0.0 | 33.3 |
| Ethnicity (%) | |||||
| Hispanic or Latino | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Highest Education Level (%) | |||||
| Doctorate | 50.0 | 66.7 | 0.0 | 0.0 | 33.3 |
| Master’s | 30.0 | 16.7 | 100.0 | 100.0 | 33.3 |
| Bachelor’s | 20.0 | 16.7 | 0.0 | 0.0 | 33.3 |
| Licenses and Certifications 4 (%) | |||||
| BCBA-D | 20.0 | 33.3 | 0.0 | 0.0 | 0.0 |
| BCBA | 30.0 | 16.7 | 100.0 | 100.0 | 33.3 |
| Licensed Psychologist | 40.0 | 66.7 | 0.0 | 0.0 | 0.0 |
| Experience with ASD (in months) | |||||
| Mean | 114.0 | 124.0 | 228 | 12 | 56 |
| Range | 12–228 | 56–196 | 12–120 | ||
| Experience in Behavior Analysis (in months) | |||||
| Mean | 143.2 | 176.7 | 180 | 36 | 64 |
| Range | 24–408 | 24–408 | 36–120 | ||
| Experience with FA and FCT (in months) | |||||
| Mean | 126.1 | 169.7 | 180 | 24 | 21 |
| Range | 3–396 | 24–396 | 3–36 | ||
| Experience with Telehealth (in months) | |||||
| Mean | 20.0 | 30.8 | 0 | 0 | 5.0 |
| Range | 0–80 | 1–80 | 0–12 |
| Variables | International |
|---|---|
| Interpreters (n) | 11 |
| Age (in years) | |
| Mean (SD) | 31.6 (6.9) |
| Range | 24–42 |
| Sex (% male) | 9.0 |
| Country of Origin (%) | |
| Cameroon | 9.0 |
| China | 9.0 |
| Iran | 9.0 |
| Mexico | 9.0 |
| Nepal | 9.0 |
| Pakistan | 9.0 |
| Russia | 9.0 |
| Saudi Arabia | 9.0 |
| United States | 9.0 |
| Venezuela | 9.0 |
| Vietnam | 9.0 |
| Ethnicity (%) | |
| Hispanic or Latino | 18.2 |
| Occupation (%) | |
| Parent | 18.2 |
| Graduate Student | 63.6 |
| Practitioner | 18.2 |
| Experience in country where family is located (in years) | |
| Mean (SD) | 15.9 (10.0) |
| Range | 0–33 |
| Families Interpreted For (n) | |
| Mean (SD) | 2.4 (2.1) |
| Range | 1–8 |
| Families Served in Each Country (%) | |
| Algeria | 4.0 |
| Cameroon | 8.0 |
| China | 4.0 |
| Costa Rica | 4.0 |
| Egypt | 4.0 |
| Iran | 4.0 |
| Mexico | 12.0 |
| Morocco | 12.0 |
| Nepal | 4.0 |
| Pakistan | 4.0 |
| Russia | 4.0 |
| Saudi Arabia | 12.0 |
| Ukraine | 4.0 |
| Venezuela | 8.0 |
| Vietnam | 12.0 |
| Languages Interpreted for Families (%) | |
| Arabic | 32.0 |
| Farsi | 4.0 |
| French | 8.0 |
| Mandarin | 4.0 |
| Nepalese | 4.0 |
| Russian | 8.0 |
| Spanish | 12.0 |
| Urdu | 4.0 |
| Vietnamese | 12.0 |
| Experience with FA and FCT (% yes) | 9.0 |
| Location of Interpreter (% participants) | |
| With Behavior Therapist | 28.0 |
| With Family | 12.0 |
| Other in US | 44.0 |
| Other in Family Country | 0.0 |
| Other Country | 20.0 |
| Study Phase | All Sites | Iowa | Georgia | Texas | International |
|---|---|---|---|---|---|
| Behavioral Function(s) Identified% (n) | |||||
| Escape | 56.5 (83) | 52.5 (21) | 48.1 (13) | 69.6 (32) | 50.0 (17) |
| Tangible | 66.7 (98) | 47.5 (19) | 77.8 (21) | 82.6 (38) | 58.8 (20) |
| Attention | 25.9 (38) | 15.0 (6) | 14.8 (4) | 50.0 (23) | 14.7 (5) |
| Automatic | 0.7 (1) | 0.0 (0) | 0.0 (0) | 2.2 (1) | 0.0 (0) |
| No Function Identified | 12.9 (19) | 25.0 (10) | 11.1 (3) | 6.5 (3) | 8.8 (3) |
| Behavioral Function(s) Targeted in FCT% (n) | |||||
| Escape | 51.2 (64) | 60.0 (18) | 33.3 (8) | 57.1 (24) | 48.3 (14) |
| Tangible | 60.8 (76) | 46.7 (14) | 70.8 (17) | 66.7 (28) | 58.6 (17) |
| Attention | 6.4 (8) | 10.0 (3) | 4.2 (1) | 7.1 (3) | 3.4 (1) |
| Study Phase | All Sites | Iowa | Georgia | Texas | International |
|---|---|---|---|---|---|
| Before FA | |||||
| % (n) | 28.4 (29) | 31.7 (13) | 20.0 (3) | 20.8 (5) | 36.4 (8) |
| Mean Weeks Enrolled | 10.2 | 19.0 | 0.0 | 3.0 | 4.1 |
| During FA | |||||
| % (n) | 22.5 (23) | 14.6 (6) | 46.7 (7) | 20.8 (5) | 22.7 (5) |
| Mean Weeks Enrolled | 21.9 | 62.7 | 7.9 | 6.6 | 7.8 |
| Before FCT | |||||
| % (n) | 21.6 (22) | 24.4 (10) | 20.0 (3) | 16.7 (4) | 22.7 (5) |
| Mean Weeks Enrolled | 18.3 | 28.3 | 13.7 | 7.5 | 9.8 |
| During FCT | |||||
| % (n) | 27.5 (28) | 29.3 (12) | 13.3 (2) | 41.7 (10) | 18.2 (4) |
| Mean Weeks Enrolled | 30.2 | 51.7 | 10.0 | 13.2 | 18.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schieltz, K.M.; O’Brien, M.J.; Tsami, L.; Call, N.A.; Lerman, D.C. Behavioral Assessment and Treatment via Telehealth for Children with Autism: From Local to Global Clinical Applications. Int. J. Environ. Res. Public Health 2022, 19, 2190. https://doi.org/10.3390/ijerph19042190
Schieltz KM, O’Brien MJ, Tsami L, Call NA, Lerman DC. Behavioral Assessment and Treatment via Telehealth for Children with Autism: From Local to Global Clinical Applications. International Journal of Environmental Research and Public Health. 2022; 19(4):2190. https://doi.org/10.3390/ijerph19042190
Chicago/Turabian StyleSchieltz, Kelly M., Matthew J. O’Brien, Loukia Tsami, Nathan A. Call, and Dorothea C. Lerman. 2022. "Behavioral Assessment and Treatment via Telehealth for Children with Autism: From Local to Global Clinical Applications" International Journal of Environmental Research and Public Health 19, no. 4: 2190. https://doi.org/10.3390/ijerph19042190
APA StyleSchieltz, K. M., O’Brien, M. J., Tsami, L., Call, N. A., & Lerman, D. C. (2022). Behavioral Assessment and Treatment via Telehealth for Children with Autism: From Local to Global Clinical Applications. International Journal of Environmental Research and Public Health, 19(4), 2190. https://doi.org/10.3390/ijerph19042190