
Reducing the Physical Burden of Older Persons’ Household Caregivers: The Effect of Household Handrail Provision



Abstract
:1. Introduction
2. Materials and Methods
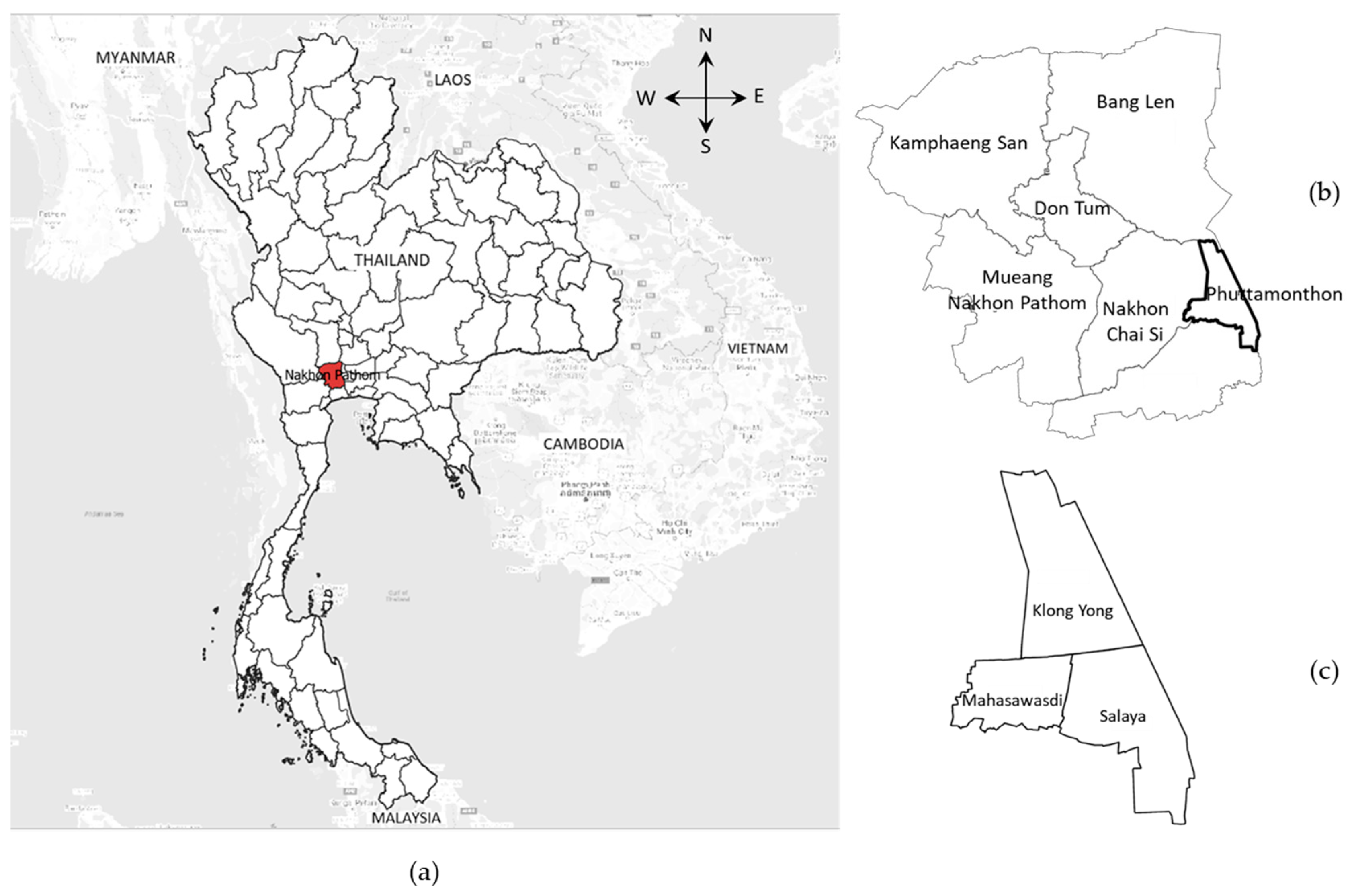
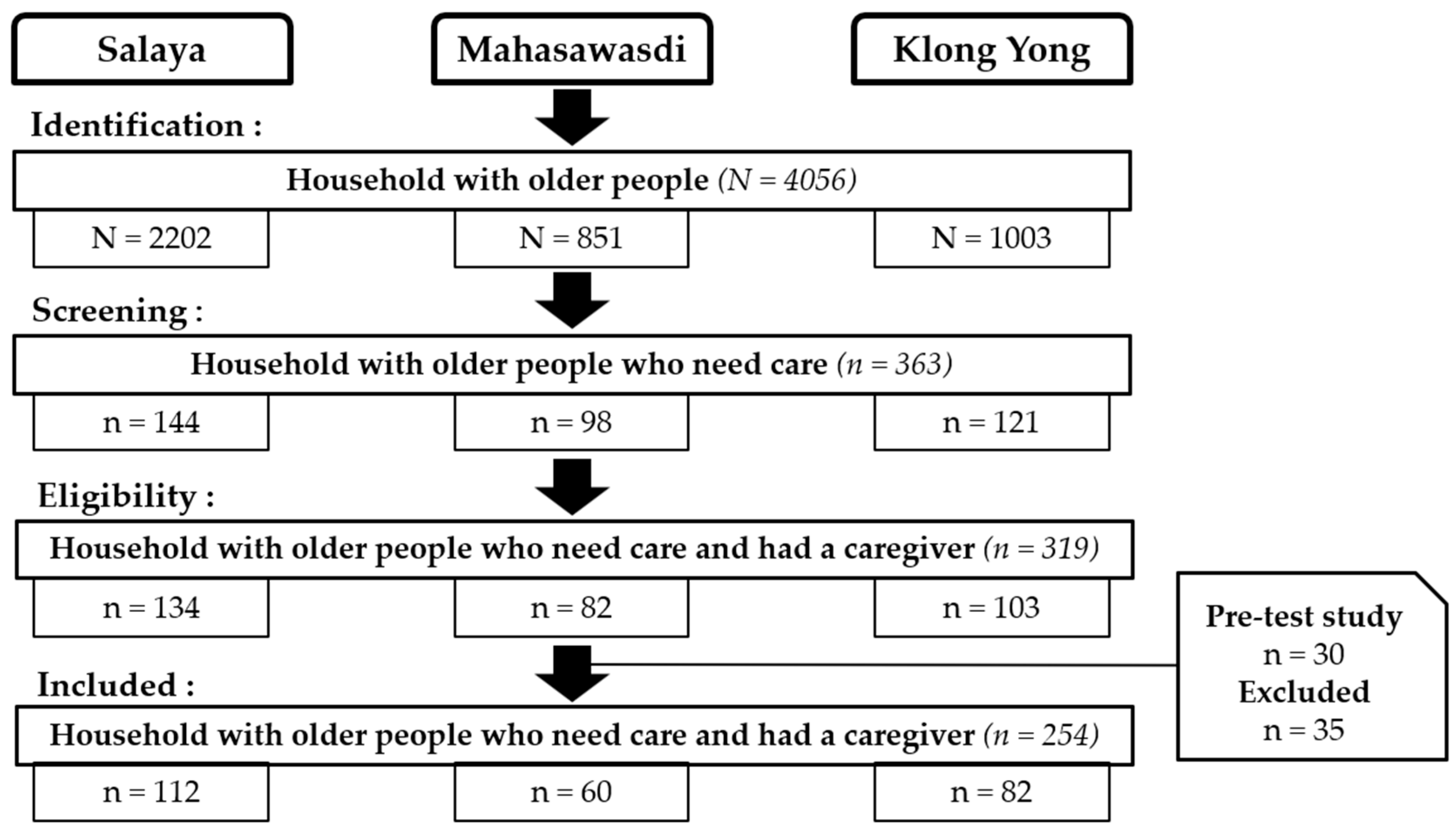
2.1. Study Design, Population, and Data Collection
2.2. Physical Caregiver Burden
2.3. Household Handrail Provision
2.4. Covariates
2.5. Statistical Methods
3. Results
3.1. Levels of Physical Caregiver Burden
3.2. Effects of Household Handrail Provision on Physical Caregiver Burden
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: The challenges ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Gitlin, L.N.; Winter, L.; Dennis, M.P. Assistive devices caregivers use and find helpful to manage problem behaviors of dementia. Gerontechnology 2010, 9, 408–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamford, G. Cohousing for older people: Housing innovation in the Netherlands and Denmark. Australas. J. Ageing 2005, 24, 44–46. [Google Scholar] [CrossRef] [Green Version]
- WikstrÃķm, B.-M. Congregate Housing for Old People: The Importance of the Physical Environment. Aust. J. Prim. Health 2007, 13, 85–90. [Google Scholar] [CrossRef]
- George, L.K.; Gwyther, L.P. Caregiver well-being: A multidimensional examination of family caregivers of demented adults. Gerontologist 1986, 26, 253–259. [Google Scholar] [CrossRef]
- Schölzel-Dorenbos, C.J.; Draskovic, I.; Vernooij-Dassen, M.J.; Rikkert, M.G.O. Quality of life and burden of spouses of Alzheimer disease patients. Alzheimer Dis. Assoc. Disord. 2009, 23, 171–177. [Google Scholar] [CrossRef]
- Schulz, R.; Sherwood, P.R. Physical and mental health effects of family caregiving. J. Soc. Work Educ. 2008, 44, 105–113. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Kasper, J.D.; Steinbach, U.; Andrews, J. Caregiver role appraisal and caregiver tasks as factors in ending caregiving. J. Aging Health 1994, 6, 397–414. [Google Scholar] [CrossRef]
- Jitapunkul, S.; Wivatvanit, S. National policies and programs for the aging population in Thailand. Ageing Int. 2008, 33, 62–74. [Google Scholar] [CrossRef]
- Kwon, S. Future of long-term care financing for the elderly in Korea. J. Aging Soc. Policy 2008, 20, 119–136. [Google Scholar] [CrossRef] [PubMed]
- Menon, J.; Melendez, A.C. Ageing in Asia: Trends, impacts and responses. ASEAN Econ. Bull. 2009, 26, 293–305. [Google Scholar] [CrossRef]
- Rozario, P.A.; Rosetti, A.L. “Many Helping Hands”: A review and analysis of long-term care policies, programs, and practices in Singapore. J. Gerontol. Soc. Work 2012, 55, 641–658. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Prospects 2019. Online Edition. Available online: https://population.un.org/wpp/Download/Standard/Population/ (accessed on 16 August 2020).
- Adams, T.; Bridge, C.; Carnemolla, P.; McNamara, N.; Quinn, J. Consumer Factsheet: Arranging Home Modifications; Consumer Factsheet Series; Home Modification Information Clearinghouse: Sydney, Australia, 2014. [Google Scholar]
- Carnemolla, P.; Bridge, C. A scoping review of home modification interventions—Mapping the evidence base. Indoor Built Environ. 2020, 29, 299–310. [Google Scholar] [CrossRef]
- Carnemolla, P.; Bridge, C. Housing design and community care: How home modifications reduce care needs of older people and people with disability. Int. J. Environ. Res. Public Health 2019, 16, 1951. [Google Scholar] [CrossRef] [Green Version]
- Carter, S.E.; Campbell, E.M.; Sanson-Fisher, R.W.; Gillespie, W.J. Accidents in older people living at home: A community-based study assessing prevalence, type, location and injuries. Aust. N. Z. J. Public Health 2000, 24, 633–636. [Google Scholar] [CrossRef]
- Ishihara, K.; Nagamachi, M.; Komatsu, K.; Ishihara, S.; Ichitsubo, M.; Mikami, F.; Osuga, Y.; Imamura, K.; Osaki, H. Handrails for the elderly: A survey of the need for handrails and experiments to determine the optimal size of staircase handrails. Gerontechnology 2002, 1, 175–189. [Google Scholar] [CrossRef]
- Lin, D.; Borjan, M.; Seanell, D.; Kelly, C. The role of PT, OT, and other therapies in palliative care for seriously ill patients. In Oxford Textbook of Palliative Nursing, 5th ed.; Ferrell, B.R., Coyle, N., Paice, J., Eds.; Oxford University Press: Oxford, UK, 2019; pp. 154–196. [Google Scholar]
- Agree, E.M.; Freedman, V.A.; Cornman, J.C.; Wolf, D.A.; Marcotte, J.E. Reconsidering substitution in long-term care: When does assistive technology take the place of personal care? J. Gerontol. B Psychol. Sci. Soc. Sci. 2005, 60, S272–S280. [Google Scholar] [CrossRef] [Green Version]
- Powell, J.; Mackintosh, S.; Bird, E.; Ige, J.; Garrett, H.; Roys, M. The Role of Home Adaptations in Improving Later Life; Centre for Ageing Better: London, UK, 2017. [Google Scholar]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef]
- Yates, M.E.; Tennstedt, S.; Chang, B.-H. Contributors to and mediators of psychological well-being for informal caregivers. J. Gerontol. B Psychol. Sci. Soc. Sci. 1999, 54, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Schulz, R.; O’Brien, A.T.; Bookwala, J.; Fleissner, K. Psychiatric and physical morbidity effects of dementia caregiving: Prevalence, correlates, and causes. Gerontologist 1995, 35, 771–791. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Corcoran, M.A. OTR/L managing dementia at home. Top. Geriatr. Rehabil. 1996, 12, 28–39. [Google Scholar] [CrossRef]
- Nakhon Pathom Provincial Hall. Available online: http://www.nakhonpathom.go.th/files/com_news_describe/2017–11_d47c24414a18dec.pdf (accessed on 17 December 2020).
- Department of Provincial Administration, Ministry of Interior. Available online: http://service.nso.go.th/nso/web/statseries/statseries01.html (accessed on 8 June 2020).
- Mariyasoosai, R.; Chompikul, J.; Keiwkarnka, B.; Wongsawass, S. Hypertension preventive behavior among pre-hypertensive adults in Phutthamonthon district, Nakhon Pathom province, Thailand. J. Public Health Dev. 2015, 13, 51–65. [Google Scholar]
- Novak, M.; Guest, C. Application of a multidimensional caregiver burden inventory. Gerontologist 1989, 29, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.-R.; Jiann-Chyun, L.; Chu, H. The reliability and validity of the Chinese version of the caregiver burden inventory. Nurs. Res. 2002, 51, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Marvardi, M.; Mattioli, P.; Spazzafumo, L.; Mastriforti, R.; Rinaldi, P.; Polidori, M.C.; Cherubini, A.; Quartesan, R.; Bartorelli, L.; Bonaiuto, S. The Caregiver Burden Inventory in evaluating the burden of caregivers of elderly demented patients: Results from a multicenter study. Aging. Clin. Exp. Res. 2005, 17, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Valer, D.B.; Aires, M.; Fengler, F.L.; Paskulin, L.M.G. Adaptation and validation of the Caregiver Burden Inventory for use with caregivers of elderly individuals1. Rev. Latino-Am. Enfermagem. 2015, 23, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Vázquez, F.L.; Otero, P.; Simón, M.A.; Bueno, A.M.; Blanco, V. Psychometric properties of the Spanish version of the caregiver burden inventory. Int. J. Environ. Res. Public Health 2019, 16, 217. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.; Sekiguchi, Y.; Honda, K.; Izumi, S.-I.; Kanetaka, H. Comparison of handrail reaction forces between two different handrails during sit-to-stand movement in the elderly. Clin. Biomech. 2020, 80, 105130. [Google Scholar] [CrossRef]
- Chacko, T.V.; Thangaraj, P.; Muhammad, G. How fall-safe is the housing for the elderly in rural areas? A cross sectional study using fall prevention screening checklist. J. Indian Acad. Geriatr. 2017, 13, 124–130. [Google Scholar]
- Chan, M.Y. Ageing-in-Place: Home Enhancement to Give Elderly a “Dream Home”. Asia Pacific Institute of Ageing Studies Newsletter. Available online: http://commons.ln.edu.hk/apiasnlj/vol6/iss1/15/ (accessed on 3 December 2021).
- Homma, K.; Yamada, Y.; Matsumoto, O.; Ono, E.; Lee, S.; Horimoto, M.; Suzuki, T.; Kanehira, N.; Suzuki, T.; Shiozawa, S. A proposal of a method to reduce burden of excretion care using robot technology. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 621–625. [Google Scholar]
- Yu, Y.; Liu, Z.-W.; Li, T.-X.; Li, Y.-L.; Xiao, S.-Y.; Tebes, J.K. Test of the stress process model of family caregivers of people living with schizophrenia in China. Soc. Sci. Med. 2020, 259, 113113. [Google Scholar] [CrossRef] [PubMed]
- Yakubu, Y.A.; Schutte, D.W. Caregiver attributes and socio-demographic determinants of caregiving burden in selected low-income communities in cape town, South Africa. J. Compassionate Health Care 2018, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bastawrous, M. Caregiver burden—A critical discussion. Int. J. Nurs. Stud. 2013, 50, 431–441. [Google Scholar] [CrossRef]
- Casado, B.; Sacco, P. Correlates of caregiver burden among family caregivers of older Korean Americans. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 331–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raina, P.; O’Donnell, M.; Schwellnus, H.; Rosenbaum, P.; King, G.; Brehaut, J.; Russell, D.; Swinton, M.; King, S.; Wong, M. Caregiving process and caregiver burden: Conceptual models to guide research and practice. BMC Pediatr. 2004, 4, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- McKenzie, D.J. Measuring inequality with asset indicators. J. Popul. Econ. 2005, 18, 229–260. [Google Scholar] [CrossRef]
- Kim, H.; Chang, M.; Rose, K.; Kim, S. Predictors of caregiver burden in caregivers of individuals with dementia. J. Adv. Nurs. 2012, 68, 846–855. [Google Scholar] [CrossRef]
- Shiba, K.; Kondo, N.; Kondo, K. Informal and formal social support and caregiver burden: The AGES caregiver survey. J. Epidemiol. 2016, 26, 622–628. [Google Scholar] [CrossRef] [Green Version]
- StataCorp, L. StataCorp Stata Statistical Software: Release 14; StataCorp LP.: College Station, TX, USA, 2015. [Google Scholar]
- Lee, J. Cumulative logit modelling for ordinal response variables: Applications to biomedical research. Comput. Appl. Biosci. 1992, 8, 555–562. [Google Scholar] [CrossRef]
- McCullagh, P. Regression models for ordinal data. J. R. Stat. Soc. Ser. B Stat. Methodol. 1980, 42, 109–127. [Google Scholar] [CrossRef]
- Williams, R. Generalized ordered logit/partial proportional odds models for ordinal dependent variables. Stata J. 2006, 6, 58–82. [Google Scholar] [CrossRef] [Green Version]
- Mekawichai, P.; Saetang, S. Caregiver burden among Thai dementia patients’ caregivers. J. Psychiatr. Assoc. Thail. 2013, 58, 101–110. [Google Scholar]
- Muangpaisan, W.; Praditsuwan, R.; Assanasen, J.; Srinonprasert, V.; Assantachai, P.; Intalapaporn, S.; Pisansalakij, D. Caregiver burden and needs of dementia caregivers in Thailand: A cross-sectional study. J. Med. Assoc. Thai 2010, 93, 601–607. [Google Scholar] [PubMed]
- Griffiths, J.; Bunrayong, W. Problems and needs in helping older people with dementia with daily activities: Perspectives of Thai caregivers. Br. J. Occup. Ther. 2016, 79, 78–84. [Google Scholar] [CrossRef]
- Limpawattana, P.; Theeranut, A.; Chindaprasirt, J.; Sawanyawisuth, K.; Pimporm, J. Caregivers burden of older adults with chronic illnesses in the community: A cross-sectional study. J. Community Health 2013, 38, 40–45. [Google Scholar] [CrossRef]
- Ondee, P.; Panitrat, R.; Pongthavornkamol, K.; Senanarong, V.; Harvath, T.A.; Nittayasudhi, D. Factors predicting depression among caregivers of persons with dementia. Pac. Rim Int. J. Nurs. Res. 2013, 17, 167–180. [Google Scholar]
- Knodel, J.; Teerawichitchainan, B.P.; Prachuabmoh, V.; Pothisiri, W. The Situation of Thailand’s Older Population: An Update based on the 2014 Survey of Older Persons in Thailand; Research Collection School of Social Sciences, Paper 1948; HelpAge International: Chiang Mai, Thailand, 2015. [Google Scholar]
- Chang, B.-H.; Noonan, A.E.; Tennstedt, S.L. The role of religion/spirituality in coping with caregiving for disabled elders. Gerontologist 1998, 38, 463–470. [Google Scholar] [CrossRef]
- Subgranon, R.; Lund, D.A. Maintaining caregiving at home: A culturally sensitive grounded theory of providing care in Thailand. J. Transcult. Nurs. 2000, 11, 166–173. [Google Scholar] [CrossRef]
- Wiseso, W.; Fongkaew, W.; Pinyokham, N.; Spiers, J. Caring for terminally Ill persons with cancer: Experiences of Thai Buddhist family caregivers. Pac. Rim Int. J. Nurs. Res. 2017, 21, 317–330. [Google Scholar] [CrossRef]
- Gray, R.S.; Hahn, L.; Thapsuwan, S.; Thongcharoenchupong, N. Strength and stress: Positive and negative impacts on caregivers for older adults in Thailand. Australas. J. Ageing 2016, 35, 7–12. [Google Scholar] [CrossRef]
- Sethabouppha, H.; Kane, C. Caring for the seriously mentally ill in Thailand: Buddhist family caregiving. Arch. Psychiatr. Nurs. 2005, 19, 44–57. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Sancarlo, D.; Addante, F.; Ciccone, F.; Cascavilla, L.; Paris, F.; Picoco, M.; Nuzzaci, C.; Elia, A.C.; Greco, A. Caregiver burden characterization in patients with Alzheimer’s disease or vascular dementia. Int. J. Geriatr. Psychiatry 2015, 30, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Chappell, N.L.; Reid, R.C. Burden and well-being among caregivers: Examining the distinction. Gerontologist 2002, 42, 772–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marras, W.S.; Davis, K.G.; Kirking, B.C.; Bertsche, P.K. A comprehensive analysis of low-back disorder risk and spinal loading during the transferring and repositioning of patients using different techniques. Ergonomics 1999, 42, 904–926. [Google Scholar] [CrossRef]
- Wilson, K. Ergonomics and the bariatric patient. Bariatr. Surg. Patient Care 2006, 1, 173–178. [Google Scholar] [CrossRef]
- Marquardt, G.; Johnston, D.; Black, B.S.; Morrison, A.; Rosenblatt, A.; Lyketsos, C.G.; Samus, Q.M. A descriptive study of home modifications for people with dementia and barriers to implementation. J. Hous. Elder. 2011, 25, 258–273. [Google Scholar] [CrossRef] [Green Version]
- Hasselkus, B.R. Meaning in family caregiving: Perspectives on caregiver/professional relationships. Gerontologist 1988, 28, 686–691. [Google Scholar] [CrossRef]
- Aldrich, J.H.; Nelson, F.D. Linear Probability, Logit, and Probit Models; Sage: London, UK, 1984. [Google Scholar]
- Long, J.S.; Long, J.S. Regression Models for Categorical and Limited Dependent Variables; Sage: Thousand Oaks, CA, USA, 1997; Volume 7. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Household Handrail Provision | ||||
|---|---|---|---|---|
| Characteristics | All | No Handrails (%) | Having a Handrail in One Place (%) | Having Handrails in More Than One Place (%) |
| n = 254 | 43.3 | 35.8 | 20.9 | |
| Households | ||||
| Living arrangement of older person | ||||
| lived alone/with another older person | 12 | 66.6 | 16.7 | 16.7 |
| lived with only their caregiver | 29 | 48.3 | 34.5 | 17.2 |
| lived with caregiver and others | 192 | 41.1 | 36.5 | 22.4 |
| lived with others but not a caregiver | 21 | 42.8 | 42.9 | 14.3 |
| Relative household wealth | ||||
| quintile 1, poorest | 51 | 62.8 | 33.3 | 3.9 |
| quintile 2, poor | 50 | 58.0 | 26.0 | 16.0 |
| quintile 3, medium | 51 | 54.9 | 33.3 | 11.8 |
| quintile 4, rich | 53 | 28.3 | 45.3 | 26.4 |
| quintile 5, richest | 49 | 12.3 | 40.8 | 46.9 |
| Caregivers | ||||
| Age mean (SD) (range: 21–90 years) | 54.6 (12.6) | 51.8 (13.3) | 57.6 (10.0) | 55.3 (14.1) |
| non-older | 170 | 47.7 | 32.9 | 19.4 |
| older | 84 | 34.5 | 41.7 | 23.8 |
| Sex | ||||
| male | 42 | 52.4 | 30.9 | 16.7 |
| female | 212 | 41.5 | 36.8 | 21.7 |
| Marital status | ||||
| married/cohabiting | 166 | 43.4 | 37.3 | 19.3 |
| single | 42 | 33.3 | 42.9 | 23.8 |
| widowed/divorced/separated | 46 | 52.2 | 23.9 | 23.9 |
| Educational level | ||||
| primary or less | 153 | 42.5 | 42.5 | 15.0 |
| secondary school | 67 | 50.8 | 17.9 | 31.3 |
| higher secondary | 34 | 32.3 | 41.2 | 26.5 |
| Working status | ||||
| working | 174 | 44.8 | 36.8 | 18.4 |
| not working | 80 | 40.0 | 33.8 | 26.2 |
| Relationship to older person | ||||
| kinship | 240 | 43.3 | 36.7 | 20.0 |
| non-kinship | 14 | 42.9 | 21.4 | 35.7 |
| Sandwich carer | ||||
| yes | 63 | 49.2 | 28.6 | 22.2 |
| no | 191 | 41.4 | 38.2 | 20.4 |
| Duration of care for older person (years) | ||||
| ≤2 | 69 | 39.1 | 52.2 | 8.7 |
| 3–4 | 37 | 35.1 | 35.2 | 29.7 |
| >4 | 148 | 47.3 | 28.4 | 24.3 |
| Health status of older persons | ||||
| Functional dependency | ||||
| all independent | 121 | 33.9 | 47.1 | 19.0 |
| ≥1 dependent | 133 | 51.9 | 25.6 | 22.5 |
| Cognitive impairment | ||||
| all absent | 128 | 37.5 | 42.2 | 20.3 |
| ≥ 1 present | 126 | 49.2 | 29.4 | 21.4 |
| Behavioral problem | ||||
| all absent | 155 | 45.8 | 34.2 | 20.0 |
| ≥1 present | 99 | 39.4 | 38.4 | 22.2 |
| Caregiving hours | ||||
| <1 | 78 | 38.4 | 43.6 | 18.0 |
| 1.1–3.0 | 97 | 49.5 | 28.9 | 21.6 |
| >3 | 79 | 40.5 | 36.7 | 22.8 |
| Social support of caregivers | ||||
| non-received | 37 | 35.2 | 40.5 | 24.3 |
| received | 217 | 44.7 | 35.0 | 20.3 |
| Household Handrail Provision | ||||
|---|---|---|---|---|
| Physical Caregiver Burden | All | No Handrails | Having a Handrail in One Place | Having Handrails in More Than One Place |
| n = 254 | n = 110 | n = 91 | n = 53 | |
| Mean (SD) | 5.0 (3.85) | 5.3 (3.60) | 4.3 (3.90) | 5.7 (4.10) |
| Range | 0–16 | 0–13 | 0–16 | 0–16 |
| Level of the physical burden | ||||
| no | 16.9% | |||
| low | 37.0% | |||
| high | 46.1% | |||
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical Caregiver Burden | Unadjusted | Adjusted for Caregiver Background | Adjusted for Caregiver and Household Backgrounds | Adjusted for Caregiver and Household Backgrounds and Older Person’s Health Status | Adjusted for Caregiver and Household Backgrounds and Older Person’s Health Status and Caregiving Hours | Adjusted for Caregiver and Household Backgrounds and Older Person’s Health Status and Caregiving Hours and Social Support | ||||||
| Household Handrail Provision | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Panel 1 (1 vs. 2 and 3) (Ref: no handrail) | ||||||||||||
| having a handrail in one place | 0.56 * | (0.33, 0.94) | 0.58 | (0.32, 1.04) | 0.42 ** | (0.22, 0.80) | 0.36 ** | (0.17, 0.75) | 0.30 ** | (0.14, 0.66) | 0.30 ** | (0.14, 0.67) |
| having handrails in more than one place | 3.11 | (0.90, 10.82) | 3.21 | (0.88, 11.69) | 1.81 | (0.46, 7.13) | 2.51 | (0.57, 11.00) | 5.82 * | (1.05, 32.29) | 5.29 | (0.98, 28.63) |
| Panel 2 (1 and 2 vs. 3) (Ref: no handrail) | ||||||||||||
| having a handrail in one place | 0.56 * | (0.33, 0.94) | 0.58 | (0.32, 1.04) | 0.42 ** | (0.22, 0.80) | 0.36 ** | (0.17, 0.75) | 0.30 ** | (0.14, 0.66) | 0.30 ** | (0.14, 0.67) |
| having handrails in more than one place | 0.82 | (0.43, 1.57) | 0.72 | (0.35, 1.50) | 0.45 | (0.20, 1.01) | 0.47 | (0.19, 1.15) | 0.43 | (0.16, 1.15) | 0.45 | (0.17, 1.19) |
| Log-likelihood | −254.01083 | −225.27539 | −209.40633 | −187.1365 | −163.71701 | −162.48592 | ||||||
| Wald Chi2 | 12.99 | 70.46 | 102.2 | 146.74 | 193.58 | 196.04 | ||||||
| Prob> Chi2 | 0.0047 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | ||||||
| Pseudo R2 | 0.0249 | 0.1352 | 0.1962 | 0.2816 | 0.3715 | 0.3763 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phetsitong, R.; Vapattanawong, P. Reducing the Physical Burden of Older Persons’ Household Caregivers: The Effect of Household Handrail Provision. Int. J. Environ. Res. Public Health 2022, 19, 2272. https://doi.org/10.3390/ijerph19042272
Phetsitong R, Vapattanawong P. Reducing the Physical Burden of Older Persons’ Household Caregivers: The Effect of Household Handrail Provision. International Journal of Environmental Research and Public Health. 2022; 19(4):2272. https://doi.org/10.3390/ijerph19042272
Chicago/Turabian StylePhetsitong, Ruttana, and Patama Vapattanawong. 2022. "Reducing the Physical Burden of Older Persons’ Household Caregivers: The Effect of Household Handrail Provision" International Journal of Environmental Research and Public Health 19, no. 4: 2272. https://doi.org/10.3390/ijerph19042272
APA StylePhetsitong, R., & Vapattanawong, P. (2022). Reducing the Physical Burden of Older Persons’ Household Caregivers: The Effect of Household Handrail Provision. International Journal of Environmental Research and Public Health, 19(4), 2272. https://doi.org/10.3390/ijerph19042272