Abstract
This study examined older adults’ subjective wellbeing and related factors in the coastal area of Soma City nine and a half years after the Great East Japan Earthquake (GEJE). Data were collected from 65- to 84-year-old residents and 1297 participants via a questionnaire from October to November 2020. The participants were divided into two groups: housing complexes and non-housing complexes. The dependent variable was subjective wellbeing assessed via Lawton’s Philadelphia Geriatric Center Morale Scale (PGCMS). Using multivariate regression analysis, the factors most strongly related to a low PGCMS score for both groups were poor health conditions, difficulties resting while asleep, poor financial wellbeing, inability to chew certain foods, and fear of solitary death. The GEJE experience was further distinguished in the housing complex group by the loss of an important non-family individual; for the other group, important factors were female gender, junior high school education level or lower, limited social networks, and deterioration of a family member’s health. Older adults’ subjective wellbeing in Soma City was low after nine and a half years following the GEJE. For disaster victims and their families in both groups, it is crucial to implement measures such as long-term, continuous physical and mental health support.
1. Introduction
Older adults are more prone to mental health issues such as post-traumatic stress disorder (PTSD) due to natural disasters [1,2,3,4,5], which diminishes their quality of life (QOL) [6,7,8]. The Great East Japan Earthquake (GEJE) struck in March 2011, causing an immense earthquake and tsunami that killed 19,729 people and forced more than 470,000 to evacuate [9]. Furthermore, the Tokyo Electric Power Company’s Fukushima Daiichi Nuclear Power Plant (F1NPP) accident displaced 165,000 residents, 36,000 of whom are still unable to return home (as of March 2021) [9]. Of the total casualties, 66.1% were individuals aged 60 years or above, while 88.6% of disaster-related deaths were those aged 66 years or above [10]. Therefore, countries must plan and implement measures before, during, and after such disasters to reduce their repercussions for older adults [11,12].
Following the complex disaster (GEJE and F1NPP), the Fukushima prefectural government conducted the Fukushima Health Management Survey [13]. According to studies based on survey data, residents of evacuation areas experienced a deterioration in mental health [14], sleep dissatisfaction and excessive drinking [15], and an increase in lifestyle disease risks [16,17]. A different study by Moriyama et al. reported a decline in the social capital of older adults who moved from evacuation areas [18]. Furthermore, Tsubokura reported an increased diabetes risk since 2013 in coastal areas other than evacuation areas, suggesting that the disaster has had secondary effects on residents’ health [19]. Therefore, this study focused on the conditions of older adults in Soma City, which suffered from severe tsunami damage despite not being designated as an evacuation area.
In Soma City, 457 of 458 victims were killed by the tsunami, 5584 houses were damaged, and areas with many casualties were designated as “disaster risk areas” [20]. Based on surveys of disaster victims’ attitudes toward rebuilding their lives and discussions with city residents, Soma City constructed 410 dwellings in nine “public disaster housing complexes” (hereinafter referred to as “housing complexes”) [21,22]. The city undertook this project between 2013 and 2015, earlier than other municipalities, with the intent of sustainably revitalizing the local community and enabling residents to preserve their pre-disaster village communities as well as possible. Priority was given to people who lost their property due to tsunami damage and required government support to rebuild their lives, particularly older adult households. Community connections were fostered among residents, and regular check-ins were also conducted for older adults living alone [21,22]. Although people who did not relocate to the housing complexes also suffered from disaster damage, many remained in the same locations as before and rebuilt their lives on their own. Nine and a half years after the GEJE and 5 years after completing all housing complexes, it became possible to evaluate the QOL of older adults living both inside and outside the housing complexes. Such an evaluation is vital for measuring the effects of reconstruction measures and considering future measures.
The WHO [23] defines QOL as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and concerning their goals, expectations, standards and concerns”. There are several proposed QOL frameworks for older adults. For example, Lawton [24] suggests that four components constitute a good life for older adults: behavioral competence, objective environment, psychological wellbeing, and perceived QOL. Perceived QOL is expressed by the degree of satisfaction in various areas measured by subjective wellbeing scales [25], among which Neugarten et al.’s life satisfaction index A (LSIA) [26] and Lawton’s Philadelphia Geriatric Center Morale Scale (PGCMS) [27,28] are widely used.
This study employed the PGCMS to measure the QOL of older adults. The scale defines morale as a multidimensional concept while calculating it as a one-dimensional score, and has an appropriate length that does not tire the respondent [29]. A high score is considered to indicate “a basic sense of satisfaction for oneself”, “a sense of belonging to one’s environment”, and “an acceptance of unchangeable realities” [30]. Therefore, it was determined to be an effective measure to grasp the situation of disaster victims nine and a half years after the GEJE. Subjective wellbeing is the concept of the superordinate objective variable in this study, which is expressed as “morale” and is based on the PGCMS scores. This is the first study to use the PGCMS to measure the QOL of older adult survivors of disasters including the GEJE.
Based on findings from his 30-year study, Larson [25] reported that physical health, followed by functional state, economic factors, social interactions, marital status, and lifestyle status, were most strongly associated with subjective wellbeing, while abnormal emergencies were associated with a reduction in wellbeing. Additionally, previous studies on morale reported the following factors related to morale: gender [31,32]; age [33,34]; educational attainment [35]; housing [36]; living with another person or not [35]; higher-level competence, including instrumental activities of daily living [31,34]; health conditions [32,34,35]; sleep conditions [32,33,37]; financial wellbeing [32]; diet variety [37]; chewing ability [36,38]; satisfaction with dietary habits [37]; frequency of communal dining [39,40]; social networks [31,32,34]; perceived loneliness [33,36]; and accumulation of negative life events [40].
This study aimed to fulfill two objectives. The first was to compare the subjective wellbeing of older adults living inside and outside housing complexes. Although the GEJE and F1NPP accident most likely reduced the subjective wellbeing of older adults, there were no data on the participants’ PGCMS scores before the GEJE to use for comparison. Therefore, this study compared residents that were collectively relocated to housing complexes with those who rebuilt their lives outside the housing complexes. As Soma City has endeavored to restore and preserve communities in the housing complexes, it was expected that the subjective wellbeing of housing complex residents was close to that of non-housing complex residents.
The second purpose was to consider factors related to subjective wellbeing and compare them between the two groups. Due to differences in the severity of disaster damage experienced, living environment, and other background elements, the factors related to subjective wellbeing were predicted to differ between the groups. There were no studies that measure subjective wellbeing with PGCMS in post-disaster areas.
This study addressed the dearth of long-term research on the wellbeing of older adults who live in the complex disaster-stricken areas in Fukushima. Most of the literature in this field to date has been related to general populations that were evacuated from disaster-stricken areas [18,41], while little work has been focused on the older populations that stayed in their hometowns after tsunami damage [42]. This study will contribute to policy, research, and practice regarding public health in disaster-stricken areas. It highlights the benefits of early group relocation [43], serves as a guide to future research on the long-term effects of disasters, and validates the care provided by public health professionals.
Subsequently, this study sought to measure the subjective wellbeing of older adult survivors who collectively relocated to housing complexes, compared to those who did not, and examine the related factors.
2. Materials and Methods
2.1. Setting
The study site was Soma City, located in the northeastern part of Fukushima Prefecture, approximately 45 km from the Fukushima Daiichi Nuclear Power Plant. The city has a population of 34,631, of which 30.9% were aged 65 years and over as of 29 February 2020 [44]. A tsunami with a height of over 9 m struck the city’s coastal area during the GEJE, flooding 29 km2 of land (14.6% of the city’s total area) [45].
The survey was conducted in seven town municipalities designated as “land restructuring areas” in the coastal areas (Haragama, Obama, Isobe, Kabaniwa, Niinuma, Hodota, and Babano). There were 114 villages and approximately 8000 residents in the seven towns; however, some areas that were heavily damaged by the tsunami became “disaster risk areas” (off-limit zones), and a total of 410 public disaster housing units and condominiums were constructed in nine new public disaster housing complexes (housing complexes) [21] (Figure 1).
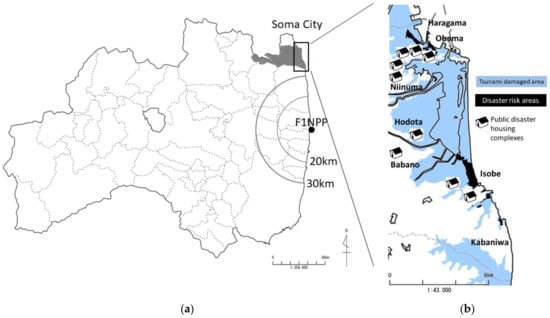
Figure 1.
(a)The geographical location of Soma City in Fukushima Prefecture, (b) illustration of its coastal area (areas that suffered tsunami damage, disaster risk areas, and public housing complexes).
This study employed a cross-sectional design. The survey was conducted between 15 October to 30 November 2020 and took the form of an anonymous, self-administered questionnaire. With the cooperation of the administrative ward mayor (chairperson of the neighborhood association), investigators familiar with the local community visited the residents’ homes, distributed the questionnaire, and collected them 1 to 2 weeks later according to the drop-off and pick-up method.
2.2. Participants
The survey targeted individuals aged 65 to 84, and it was estimated that 2503 residents from the seven towns would be potential respondents. The nine villages with housing complexes, which primarily sheltered residents who lost their property due to tsunami damage and required government support to rebuild their lives, were surveyed. Other villages without housing complexes, in which residents generally remained in the same locations as before the GEJE and rebuilt their lives on their own, were randomly selected through cluster sampling; with an effect size of 0.10 [46], a significance level of 0.05, the statistical power of 0.8, and 12 input items, the sample size needed to be at least 184 respondents from both groups to conduct a multivariate regression analysis [47]. Assuming a valid response rate of 60%, the necessary number of participants was estimated to be 309 for the housing complex group (expected collection of 185) and 548 for the non-housing complex group (expected collection of 329). Although the population ratio of housing complex residents to non-housing complex residents was estimated to be 1:7, the survey extracted participants at a ratio of 1:4 to better reflect the population and enable a stratified analysis. For the non-housing complex group, 105 towns without housing complexes were randomly selected through cluster sampling (selection probability of 0.25) until 22 towns with 560 participants were extracted as the survey sample.
Based on the Basic Resident Register (as of 1 September 2020), a list of survey participants from 31 villages was created. A total of 737 residents from the nine villages with housing complexes, including housing complex residents and general housing residents who lived around the area and 560 residents from the 22 villages without housing complexes, were extracted, amounting to a total of 1297 participants.
Excluding the 39 participants who were identified as uninvestigable through the administrative ward mayor (eight deceased, 24 who moved or were non-residents, seven in facilities or hospitalized), the questionnaire was distributed to 1258 residents. There were 1133 respondents in total (for a response rate of 87.4%), and after removing 55 incomplete answers, the final number of participants for analysis was 1078 (for a valid response rate of 83.1%). The participants were divided into the “housing complex group” and “non-housing complex group” based on their housing types, not based on their villages. As the disaster experiences of the two groups and their living environments as participants in reconstruction measures were significantly different, they were analyzed separately (Figure 2).
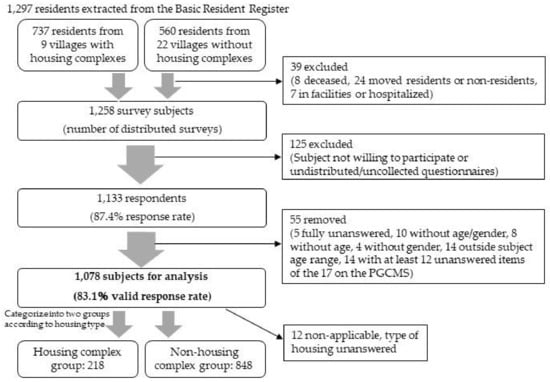
Figure 2.
A flow chart illustrating the survey procedure.
2.3. Dependent Variable
The dependent variable was subjective wellbeing, which was measured using the PGCMS total score. The Japanese translated version [48] of Lawton’s revised Philadelphia Geriatric Center Morale Scale [27,28,49] was used for measurement. The scale consists of 17 questions, such as “are you satisfied with your current life?”, to which the respondent answers by selecting either “yes” or “no”. An answer indicating high morale is counted as one point, whereas an answer indicating low morale, or a blank answer, is counted as zero points. The subscales consist of “I: psychological agitation (0–6 points)”, “II: attitude towards aging (0–5 points)”, and “III: loneliness and dissatisfaction (0–6 points)”, with higher points suggesting a higher level of subjective wellbeing. It is generally understood that 13–17 points, 10–12 points, and 0–9 points on the scale signify high, moderate, and low morale, respectively [48].
Based on previous studies, only responses with 12 or more of the 17 questions completed were considered valid [40,48,50,51]. Of the total of 1078 participants for analysis, 957 (88.8%) answered all 17 questions.
2.4. Independent Variables
The survey asked questions about 24 variables in six categories related to subjective wellbeing. The demographic variables of gender [31,32], age [33,34], and educational attainment [35] were used as moderator variables (Supplementary Materials).
2.4.1. Living Environment
The questions asked about the housing type (housing complex or non-housing complex, homeownership) and whether the participants lived with another person.
2.4.2. Physical Conditions
The degree of independence of higher-level competence was measured using the TMIG Index of Competence [52]. The total score was 13 points, with higher values indicating a greater level of independence. Based on previous studies, the respondents’ results were divided into two groups—0–10 points and 11–13 points [53]. To describe the participants’ basic attributes, the survey also asked about their height and weight (BMI) and whether they had visited a hospital.
2.4.3. Living Conditions
For health conditions, the survey asked respondents, “how is your current health condition?” They answered using a five-item scale (“very good”, “good”, “normal”, “bad”, and “very bad”) in which the final two options indicated “poor health conditions” For sleep conditions, the survey asked, “over the past month, did you get enough rest while sleeping?” and provided a four-item scale (“sufficient”, “moderate”, “inadequate”, and “none”) in which the final two indicated “difficulties resting while asleep”. For financial wellbeing, the survey asked, “how do you feel about your current financial lifestyle?” The participants responded on a five-item scale (“struggling”, “somewhat struggling”, “normal”, “somewhat comfortable”, and “comfortable”), in which the first two indicate “poor financial wellbeing”.
2.4.4. Dietary Habits
The Dietary Variety Score (DVS) [54] measured food intake diversity. Information was collected about the respondents’ weekly intake of ten food groups. The score ranged from 0 to 10 points, with higher values indicating a larger variety of food intake. Based on previous studies, the respondents’ results were divided into two groups: 0–2 points and 3–10 points [55]. For chewing ability, the survey asked about “situations when respondents chew food” and provided a four-item scale (“can chew any foods”, “cannot chew some foods”, “cannot chew many foods”, and “cannot chew any foods”), in which the final three indicated that the respondent “cannot chew certain foods”. For frequency of communal dining, the survey asked, “how often do you eat with friends, family, relatives, or other individuals?” The participants responded on a six-item scale (“almost every day”, “four-five days per week”, “two-three days per week”, “once per week”, “once or twice per month”, and “rarely”), in which the final option indicated “limited opportunities for communal dining”. For satisfaction with dietary habits, the survey asked, “are you satisfied with your dietary habits (everyday meals)?” The participants responded on a four-item scale (“very satisfied”, “somewhat satisfied”, “not very satisfied”, and “not satisfied”), in which the final two indicated “a lack of satisfaction with dietary habits”.
2.4.5. Community Connections
The degree of social isolation was measured using the Japanese translated version [56] of the simplified Lubben Social Network Scale (LSNS-6) [57,58]. The score results ranged from 0 to 30 points, with higher values indicating a greater social network and any values under 12 indicating social isolation. For fear of solitary death, the survey replicated the Annual Report on the Aging Society [10], asking, “do you consider solitary death (passing away without anyone’s care and being discovered afterward) to be a personally relevant issue?” The participants responded on a five-item scale (“very much”, “somewhat”, “somewhat not”, “not at all”, and “unsure”) in which the first two answers indicated “imminent fear of solitary death”.
2.4.6. Experiences from the GEJE
Regarding the Fukushima Health Management Survey [13], the survey asked respondents to select events they experienced due to the GEJE. The full 12-item list of options was as follows: displacement, living separately from family, living together with family, personal health deterioration, deterioration of a family member’s health, caregiving for a family member, divorce/separation/loss of spouse/partner, loss of a family member other than spouse/partner, loss of an important non-family individual, unemployment, financial hardships, and difficulties in interpersonal relations.
2.5. Data Analysis
First, the participants’ characteristics and the distribution of each variable were identified. Next, a univariate analysis was conducted to examine the relationship between the dependent variable, subjective wellbeing (indicated by the PGCMS scores), and all other variables. Continuous variables were analyzed using the t-test, and categorical variables were analyzed using Pearson’s chi-squared test.
Of the variables significantly related to subjective wellbeing in these tests, 13 were selected based on Spearman’s rank correlation coefficient between each variable and insight from previous studies. Among the factors that had a high significance in univariate analysis, “deterioration in personal health (GEJE experience)” was similar in content to “poor health condition” (correlation coefficient of ρ = 0.256 for housing complex group, ρ = 0.351 for the non-housing complex group, both p < 0.001); therefore, “poor health condition” was selected. “Caregiving for a family member (GEJE experience)” was also similar in content to “deterioration of a family member’s health condition” and was selected. “Caregiving for a family member (GEJE experience)” was also similar in content to “deterioration of a family member’s health (GEJE experience)” (correlation coefficient of ρ = 0.468 for housing complex group, ρ = 0.358 for the non-housing complex group, both p < 0.001); thus, “deterioration of a family member’s health” was selected. Furthermore, “Unemployment (GEJE experience)” was similar in content to “financial hardships (GEJE experience)”, which was also similar to “poor financial wellbeing” (housing complex group ρ = 0.491, non-housing complex group ρ = 0.430, both p < 0.001); thus, “poor financial wellbeing” was selected. As “a lack of satisfaction with dietary habits” was based on the respondent’s subjective judgment of satisfaction and could be seen as an outcome variable that relates to the same factors as subjective wellbeing, it was not included in the analysis.
A multivariate regression analysis was then conducted, with the independent variables being the binarized data of “no homeownership”, “lack of higher-level competence”, “poor health condition”, “difficulties resting while asleep”, “poor financial wellbeing”, “low DVS”, “cannot chew certain foods”, “limited opportunities for communal dining”, “limited social networks”, “fear of imminent solitary death”, and “experiences from the GEJE (deterioration of a family member’s health, loss of an important non-family individual, difficulties in interpersonal relations)”. The covariate variables were “female”, age (continuous data), and “educational attainment up to junior high school”.
The housing complex and non-housing complex groups were analyzed separately to compare the results. The significance level was set at 0.05. All statistical analyses were conducted using the software IBM SPSS Statistics 27 (IMB Corp., Armonk, NY, USA).
2.6. Ethical Considerations
The respondents were informed beforehand of the study purpose and methods, that participation was voluntary, and that the results were entirely anonymous. After a respondent filled out the questionnaire, it was enclosed and sealed in a collection envelope. Questionnaire submission was considered to signal the respondent’s consent to participate. The study was conducted with the approval of the ethics committee of Fukushima Medical University (25 May 2020, approval number: 2020-037).
3. Results
3.1. Survey Participants’ Characteristics
Table 1 illustrates the survey results for the variables related to the participants’ basic characteristics (Table 1). The total sample was 54.7% women and had a mean age of 73.0 ± 5.4 years old, with no significant difference between the housing complex and non-housing complex groups. The characteristics unique to the housing complex group included a greater proportion of people with an educational attainment of up to junior high school, who lived alone, and who had no homeownership, a low degree of higher-level competence, high BMI, and limited social networks for men. The housing complex group’s mean score was significantly lower (p < 0.001), while women’s scores were significantly lower when comparing results between genders (p = 0.006, not listed in the table).

Table 1.
Participant characteristics.
3.2. Univariate Analysis of PGC Morale
The survey responses for each independent variable were divided according to the two groups, and a Student’s t-test was performed on the PGCMS scores (Table 2).
Table 2.
Results of univariate analysis of independent variables and subjective wellbeing (PGCMS scores).
Of the 24 variables, those significantly related to the housing complex group were “higher-level competence”, “health condition”, “sleep conditions”, “financial wellbeing”, “DVS”, “chewing ability”, “satisfaction with dietary habits”, “social networks”, and “fear of solitary death;” from the GEJE experiences, “personal health deterioration”, “deterioration of a family member’s health”, “unemployment”, “financial hardships”, and “difficulties in interpersonal relations”, in addition to the moderator variable “educational attainment”.
The variables significantly related (p < 0.05) to the non-housing complex group were “type of housing (homeownership)”, “higher-level competence”, “health condition”, “sleep conditions”, “financial wellbeing”, “DVS”, “chewing ability”, “frequency of communal dining”, “satisfaction with eating habits”, “social networks”, and “fear of solitary death”; from the GEJE experiences, “deterioration of personal health”, “deterioration of a family member’s health”, “caregiving for a family member”, “loss of an important non-family individual”, “unemployment”, “financial hardships”, and “difficulties in interpersonal relations”, in addition to the moderator variables “gender”, “age”, and “educational attainment”.
The variables that had no significant difference between the housing complex and non-housing complex groups were “living alone or with another person”; from the GEJE experiences, “displacement”, “living separately from family”, “living together with family”, “divorce/separation/loss of spouse/partner”, and “loss of a family member other than spouse/partner”.
3.3. Multivariate Regression Analysis of PGC Morale
Furthermore, a multivariate regression analysis was conducted on 13 independent variables to examine their relationships with the PGCMS scores (Table 3).
Table 3.
Factors related to Subjective wellbeing.
The factors significantly related with the PGCMS scores for both groups were “poor health condition” (housing complex group β = −0.222, non-housing complex group β = −0.263), “difficulties resting while asleep” (housing complex group β = −0.185, non-housing complex group β = −0.229), “poor financial wellbeing” (housing complex group β = −0.341, non-housing complex group β = −0.207), “cannot chew certain foods” (housing complex group β = −0.117, non-housing complex group β = −0.112), and “fear of solitary death”. The related factor was “loss of an important non-family individual (GEJE experience)” (β = −0.125) only for the housing complex group. However, the related factors were “women” (β = −0.099), “educational attainment up to junior high school” (β = −0.062), “limited social networks” (β = −0.113), and “deterioration of a family member’s health (GEJE experience)” (β = −0.076) only for the non-housing complex group.
The variance inflation factor (VIF) for the housing complex and non-housing complex groups was 1.062–1.061 and 1.043–1.343, respectively. Both values were sufficiently low, and no multicollinearity was observed. The coefficient of determination (R2) was 0.391 for both housing complex and non-housing complex groups.
4. Discussion
This study examined the subjective wellbeing of older adults in the coastal area of Soma City nine and a half years after the GEJE, in addition to its related factors. Older adults’ subjective wellbeing in Soma City was observed to be at relatively low levels. There were commonalities and differences in the factors related to subjective wellbeing between older adults in the housing complex group and those in the non-housing com-plex group. Both groups had significant levels of satisfaction if the following five needs were addressed: health, sleep, finance, ability to chew, and perceptions of solitary death. Their levels of wellbeing differed depending on individual attributes and relationships with others. These included the loss of friends and acquaintances due to the GEJE for the housing complex group, and gender, educational attainment, social networks, and health of family members for the non-housing complex group.
The mean subjective wellbeing of the survey participants was 9.1 ± 4.4 overall, 8.0 ± 4.6 for the housing complex group, and 9.4 ± 4.3 for the non-housing complex group. Before the GEJE, Nagata et al. [31], who studied Japanese older adults aged 75 years and above, reported morale to be 13.1 ± 2.7 and 12.4 ± 3.0 for men and women, respectively, while Demura et al. [32], who focused on people aged 60 years and above, reported 11.6 ± 3.78 and 11.2 ± 4.02 for men and women, respectively. Lawton explains that scores ranging between 17 to 13, 12 to 10, and 9 to 0 indicate high, medium, and low morale, respectively; therefore, one can infer that the subjective wellbeing of the housing complex group was at relatively low levels [49]. One plausible reason for this decline was the participants’ experiences from the GEJE nine and a half years earlier. In particular, the housing complex group recorded significantly lower subjective wellbeing scores than the non-housing complex group, most likely because they lost their houses and land property to the tsunami. The survey results demonstrate that a greater proportion of the housing complex group experienced “displacement” (housing complex group 67.4%, non-housing complex group 18.2%), “financial hardships” (housing complex group 37.2%, non-housing complex group 24.6%), and “loss of a family member other than spouse/partner” (housing complex group, 21.1%; non-housing complex group, 14.9%) due to the GEJE. Furthermore, Rehdanz et al. [59] reported that the residents who experienced a fall in subjective wellbeing 1 year after the GEJE were those living near tsunami-stricken areas and the F1NPP. This suggests that the experiences of tsunami damage have particularly affected the subjective wellbeing of the housing complex group.
Factors significantly related to subjective wellbeing for both groups were “poor health conditions”, “difficulties resting while asleep”, “poor financial wellbeing”, “cannot chew certain foods”, and “imminent fear of solitary death”. As previous studies have reported similar findings regarding health conditions [32,34,35], sleep conditions [32,33,37], financial wellbeing [2], and chewing ability [37,38], they can be considered as issues shared among older adults in general.
However, the “fear of imminent solitary death” factor should be interpreted with caution due to a lack of previous studies that report its correlation with subjective wellbeing. The term “solitary death” (kodoku-shi in Japanese) first became known when it occurred widely during the 1995 Great Hanshin earthquake [60]. Since then, it has increasingly become a matter of public concern, primarily because of the mass media; however, the term still lacks a solid definition [61]. This study defines it as “passing away without anyone’s care and being discovered afterward” based on the Cabinet Office’s Annual Report on the Aging Society [10]. The government has been implementing measures to ensure that older adults living alone can enjoy life in their community without fearing solitary death. In the 10 years following the GEJE, Fukushima prefecture reported 155 solitary deaths [62], one of which was found in Soma City in 2015 [63]. Despite the local government in Soma City conducting check-in visits for disaster victims, a man in his 50s passed away in temporary housing and was discovered about a week later. The city has since endeavored to prevent similar deaths, particularly in housing complexes, by ensuring that the chairpersons of each administrative ward visit residents about once every 2 days [21]. In the case of the survey participants, although solitary death did not frequently occur in their city, 63.7% of the housing complex group and 52.6% of the non-housing complex group subjectively felt that solitary death was an issue of personal relevance. The survey results also indicated that fear of solitary death was associated with lower levels of subjective wellbeing. Future prevention measures should focus on supporting men and residents living alone, who are most prone to solitary death. Implementing better methods to monitor people’s health, such as a robust family doctor system and the active use of caregivers, will also be necessary [64].
Older adults are prone to conditions such as tooth loss, tooth decay, periodontal disease, and xerostomia, resulting in reduced chewing ability [65]. Chewing ability is closely related to older adults’ QOL [38]. Ohara reported the effectiveness of educational programs such as oral hygiene instruction, facial and tongue muscle exercises, and salivary gland massage for xerostomia [66]. Katagiri reported the efficacy of mastication training using ice chips [67]. Therefore, guidance by dentists and dental hygienists is important [65]. In addition, since elderly people with oral function problems tend to have low multiple nutrient intake [68], nutritional guidance by registered dietitians, including assessments of dietary status and suggestions on how to eat, is also considered necessary.
The factor “loss of an important non-family individual (GEJE experience)” only had a strong correlation with subjective wellbeing for the housing complex group. This may be because many housing complex residents, who had lived in coastal settlements in which neighbors closely supported each other, lost valuable people and community connections due to the tsunami. Kun et al. [4] reported that people in areas with greater earthquake damage were at a higher risk of post-traumatic stress disorder (PTSD). Additionally, Jia et al. [5] reported that risk factors for PTSD symptoms in earthquake survivors include older age, loss of family members, a sense of guilt over someone’s death or injury, and lack of mental health support. Thus, it is crucial that residents who experienced the GEJE, many of whom live in housing complexes, receive continuous professional mental health support.
On the contrary, the factors “female”, “educational attainment up to junior high school”, “limited social networks”, and “deterioration of a family member’s health (GEJE experience)” only had a strong correlation with subjective wellbeing for the non-housing complex group. Nagata et al. [31] and Demura et al. [32] both indicate that the female gender is related to low levels of morale; however, Hamashima [69] suggests that gender differences are not evident for older age groups. The “female” in the non-housing complex group may have low levels of subjective wellbeing because the residents live in conditions similar to those of the average Japanese resident. The low morale level associated with educational attainment was previously shown by Hamashima [69] and Iwasa et al. [35]. Regarding social networks, low subjective wellbeing was associated with social isolation due to fewer opportunities to interact with family members, relatives, and friends. Nagata et al. [31], Okamoto [34], and Demura et al. [32] concur, reporting “frequency of socializing opportunities”, “family conversations”, and “number of close friends” as factors related to subjective wellbeing. Although there was no observable relationship between social networks and subjective wellbeing for the housing complex group, the quantity and quality of social networks of older adults are greatly significant [33]. Subjective wellbeing can be improved by building various social connections with people, including friends and family members [70], which suggests that community development must be supported in non-housing complex areas as well. As the GEJE experience factor “deterioration of a family member’s health” had no relation with the factors “divorce/separation/loss of spouse/partner” and “loss of a family member other than spouse/partner”, the struggles of caring for unwell family members may affect the subjective wellbeing of older adult GEJE survivors, separate from the direct grief of losing a family member. Therefore, it is vital to provide long-term, continuous physical and mental health support to disaster victims and their families.
The results of this study suggest that health conditions, sleep conditions, financial wellbeing, chewing ability, and fear of solitary death may be related to older adults’ subjective wellbeing in disaster-stricken areas. Additionally, the loss of an important non-family individual may be related to subjective wellbeing for housing complex residents (consisting mostly of individuals who experienced severe tsunami damage), while gender, educational attainment, social networks, and the deterioration of a family member’s health may relate to subjective wellbeing for residents outside housing complexes. The difference in related factors between the housing complex and non-housing complex groups indicates that Soma City’s housing complexes have helped maintain social networks by revitalizing community connections. In future instances of group relocation in disaster-stricken areas, housing complexes should be developed to preserve pre-existing village communities as much as possible.
This study had several limitations. First, it followed a cross-sectional design and thus did not illustrate any causal relationships. Second, as the study did not measure PGCMS scores before the GEJE, it cannot be denied that participants’ subjective wellbeing levels may have been low before the GEJE. In the future, surveys of PGCMS scores in other disaster-stricken areas should be conducted. Despite the above limitations, the study used data that had a high response rate (87.4%) and were representative of the region. For the first time, nine and a half years after the GEJE, the study successfully revealed the subjective wellbeing of older adults affected by the earthquake, tsunami, and F1NPP accident in Soma City.
Finally, there may be limitations to the generalizability of this study’s findings, because it was conducted in a single region in Japan. However, the high response rate suggests that the findings reflected the reality in that region. Similar disasters will likely occur in other parts of the world in the future (e.g., tsunamis, complex disasters, etc.), and the findings may be generalizable to regions with similar geographic conditions and social backgrounds. The findings, therefore, may help those areas develop supportive measures.
5. Conclusions
The subjective wellbeing of older adults in Soma City was observed to be at relatively low levels nine and a half years after the community suffered severe damage from the earthquake, tsunami, and F1NPP accident in March 2011.There were similarities and differences in the related factors for the housing complex and non-housing complex groups. These results indicate that, for both groups, it is crucial to implement measures such as long-term, continuous physical and mental health support for disaster victims and their families; better welfare support and family doctor systems, as well as encouragements to use caregivers actively; communication within local communities; and oral health guidance and nutrition support. The results also suggest that continuous professional support for mental health and greater community development are vital for the housing complex and non-housing complex groups, respectively.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph19052639/s1, “Questionnaire Survey on Living Conditions and Wellbeing in Soma City following the Great East Japan Earthquake”.
Author Contributions
Conceptualization, Y.K., C.N., N.I., N.M., H.I., and S.Y.; methods, Y.K., C.N., N.I., N.M., H.I., and S.Y.; investigation, Y.K., N.I., and S.Y.; resources, Y.K.; data curation, Y.K., C.N.; writing—original draft preparation, Y.K.; writing—review and editing, Y.K., C.N., N.I., N.M., H.I., and S.Y.; visualization, Y.K.; supervision, S.Y.; project administration, Y.K.; funding acquisition, Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
The first author was funded by the Kawamura Ikuei Scholarship from the Japan Dietetic Association and Kobe College Megumi Association.
Informed Consent Statement
Written informed consent was obtained from the participants to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
We sincerely thank the people of Soma City for their cooperation in conducting this study’s survey.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Parker, G.; Lie, D.; Siskind, D.J.; Martin-Khan, M.; Raphael, B.; Crompton, D.; Kisely, S. Mental health implications for older adults after natural disasters—A systematic review and meta-analysis. Int. Psychogeriatrics 2015, 28, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Ticehurst, S.; Webster, R.A.; Carr, V.J.; Lewin, T.J. The psychosocial impact of an earthquake on the elderly. Int. J. Geriatr. Psychiatry 1996, 11, 943–951. [Google Scholar] [CrossRef]
- Viswanath, B.; Maroky, A.S.; Math, S.B.; John, J.P.; Benegal, V.; Hamza, A.; Chaturvedi, S.K. Psychological Impact of the Tsunami on Elderly Survivors. Am. J. Geriatr. Psychiatry 2012, 20, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Kun, P.; Tong, X.; Liu, Y.; Pei, X.; Luo, H. What are the determinants of post-traumatic stress disorder: Age, gender, ethnicity or other? Evidence from 2008 Wenchuan earthquake. Public Health 2013, 127, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Tian, W.; Liu, W.; Cao, Y.; Yan, J.; Shun, Z. Are the elderly more vulnerable to psychological impact of natural disaster? A population-based survey of adult survivors of the 2008 Sichuan earthquake. BMC Public Health 2010, 10, 172. [Google Scholar] [CrossRef] [PubMed]
- Zaetta, C.; Santonastaso, P.; Favaro, A. Long-term physical and psychological effects of the Vajont disaster. Eur. J. Psychotraumatology 2011, 2, 8454. [Google Scholar] [CrossRef]
- Tsai, K.-Y.; Chou, P.; Chou, F.H.-C.; Su, T.T.-P.; Lin, S.-C.; Lu, M.-K.; Ou-Yang, W.-C.; Su, C.-Y.; Chao, S.-S.; Huang, M.-W. Three-year follow-up study of the relationship between posttraumatic stress symptoms and quality of life among earthquake survivors in Yu-Chi, Taiwan. J. Psychiatr. Res. 2007, 41, 90–96. [Google Scholar] [CrossRef]
- Zhao, C.; Wu, Z.; Xu, J. The association between post-traumatic stress disorder symptoms and the quality of life among Wenchuan earthquake survivors: The role of social support as a moderator. Qual. Life Res. 2012, 22, 733–743. [Google Scholar] [CrossRef]
- Agency, R. Great East Japan Earthquake; Reconstruction Agency: Tokyo, Japan, 2021; Available online: https://www.reconstruction.go.jp/english/topics/GEJE/index.html (accessed on 24 January 2022).
- Annual Report on the Ageing Society FY2018 Japanese; Cabinet Office: Tokyo, Japan, 2018; Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2018/html/zenbun/s1_2_4.html (accessed on 24 January 2022).
- Sendai Framework for Disaster Risk Reduction 2015–2030; Disaster Risk Reduction: Geneva, Switzerland, 2015.
- WHO. WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K. Study Protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef]
- Kunii, Y.; Suzuki, Y.; Shiga, T.; Yabe, H.; Yasumura, S.; Maeda, M.; Niwa, S.-I.; Otsuru, A.; Mashiko, H.; Fukushima Health Management Survey Group; et al. Severe Psychological Distress of Evacuees in Evacuation Zone Caused by the Fukushima Daiichi Nuclear Power Plant Accident: The Fukushima Health Management Survey. PLoS ONE 2016, 11, e0158821. [Google Scholar] [CrossRef]
- Orui, M.; Ueda, Y.; Suzuki, Y.; Maeda, M.; Ohira, T.; Yabe, H.; Yasumura, S. The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2017, 14, 1281. [Google Scholar] [CrossRef]
- Ohira, T.; Nakano, H.; Nagai, M.; Yumiya, Y.; Zhang, W.; Uemura, M.; Sakai, A.; Hashimoto, S.; for the Fukushima Health Management Survey Group. Changes in Cardiovascular Risk Factors After the Great East Japan Earthquake. Asia Pac. J. Public Health 2017, 29, 47S–55S. [Google Scholar] [CrossRef]
- Tsubokura, M.; Hara, K.; Matsumura, T.; Sugimoto, A.; Nomura, S.; Hinata, M.; Shibuya, K.; Kami, M. The immediate physical and mental health crisis in residents proximal to the evacuation zone after Japan’s nuclear disaster: An observational pilot study. Disaster Med. Public Health Prep 2014, 8, 30–36. [Google Scholar] [CrossRef]
- Moriyama, N.; Iwasa, H.; Tsubokura, M.; Kuroda, Y.; Yasumura, S. Living in the Restoration Public Housing after the Great East Japan Earthquake Correlates with Lower Subjective Well-Being of Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 2696. [Google Scholar] [CrossRef]
- Tsubokura, M. Secondary health issues associated with the Fukushima Daiichi nuclear accident, based on the experiences of Soma and Minamisoma Cities. J. Natl. Inst. Public Health 2018, 67, 71–83. [Google Scholar]
- Fukushimaken 2011 Tohokuchihou Taiheiyouoki Jishin niyoru Higai Joukyou Sokuhou (Dai 1780 hou); Flash report on damage caused by the 2011 off the Pacific coast of Tohoku Earthquake in Fukushima Prefecture (No.1780); Fukushima Prefecture: Fukushima, Japan, 2021. (In Japanese)
- Soma City Reconstruction Plan (ver.4.1). Soma. 2021. Available online: https://www.city.soma.fukushima.jp/shinososhiki/kikakuseisakuka/fukkou_jouhou/1710.html (accessed on 24 January 2022).
- Hachiya, H. Personal Account of Mayors from Disaster-Struck Municipalities: Great East Japan Earthquake: Origin Time: 11 March 2011, 2:46 p.m; Kindaishobo: Tokyo, Japan, 2018; pp. 144–243. [Google Scholar]
- World Health Organization. Programme on Mental Health Featured Publication WHOQOL User Manual. In Abuse Division of Mental Health and Prevention of Substance Abuse; WHO: Geneva, Switzerland, 2012; Available online: https://www.who.int/tools/whoqol (accessed on 20 February 2022).
- Lawton, M.P. A multidimensional view of quality of life in frail elders. In The Concept and Measurement of Quality of Life in the Frail Elderly; Academic Press: Cambridge, MA, USA, 1991; pp. 3–27. [Google Scholar]
- Larson, R. Thirty Years of Research on the Subjective Well-being of Older Americans. J. Gerontol. 1978, 33, 109–125. [Google Scholar] [CrossRef]
- Neugarten, B.L.; Havighurst, R.J.; Tobin, S.S. The measurement of life satisfaction. J. Gerontol. 1961, 16, 134–143. [Google Scholar] [CrossRef]
- Lawton, M.P. The Philadelphia Geriatric Center Morale Scale: A Revision. J. Gerontol. 1975, 30, 85–89. [Google Scholar] [CrossRef]
- Liang, J.; Bollen, K.A. The Structure of the Philadelphia Geriatric Center Morale Scale: A Reinterpretation. J. Gerontol. 1983, 38, 181–189. [Google Scholar] [CrossRef]
- Koyano, W. QOL nado wo sokuteisurutameno sokudo (2). Measure for measuring QOL etc. Jpn. J. Geriatr. Psychiatry 1996, 7, 431–441. (In Japanese) [Google Scholar]
- Lawton, M.P. The dimension of morale. In Research Planning and Action for the Elderly: The Power and Potential of Social Science; Kent, D.P., Kastenbaum, R., Sherwood, S., Eds.; Behavioral Publications, Inc.: New York, NY, USA, 1972; pp. 144–165. [Google Scholar]
- Nagata, A.; Yamagata, Z.; Nakamura, K.; Miyamura, T.; Asaka, A. Sex differences in subjective wellbeing and related factors in elderly people in the community aged 75 and over. Nihon Ronen Igakkai Zasshi 1999, 36, 868–873. (In Japanese) [Google Scholar] [CrossRef] [PubMed][Green Version]
- Demura, S.; Noda, M.; Minami, M.; Ishikawa, Y.; Tada, N.; Matsuzawa, J. Examination of lifestyle factors related to morale in community dwelling elderly: Comparison in gender and age-stages. Jpn. J. Physiol. Anthropol. 2003, 8, 231–235. (In Japanese) [Google Scholar]
- Näsman, M.; Niklasson, J.; Saarela, J.; Nygård, M.; Olofsson, B.; Gustafson, Y.; Nyqvist, F. Morale in Old Age and Its Association with Sociodemographic, Social, and Health-Related Factors in Different Age Groups. J. Aging Res. 2020, 2020, 3939718. [Google Scholar] [CrossRef]
- Okamoto, K. Agreement between reports by the aged themselves and by their family members on physical and psychological status. Nihon Ronen Igakkai Zasshi 2000, 37, 371–376. (In Japanese) [Google Scholar] [CrossRef][Green Version]
- Iwasa, H.; Kawaai, C.; Gondo, Y.; Inagaki, H.; Suzuki, T. Subjective well-being as a predictor of all-cause mortality among middle-aged and elderly people living in an urban Japanese community: A seven-year prospective cohort study. Geriatr. Gerontol. Int. 2006, 6, 216–222. [Google Scholar] [CrossRef]
- Wågert, P.V.H.; Rönnmark, B.; Rosendahl, E.; Lundin-Olsson, L.; Gustavsson, J.M.C.; Nygren, B.; Lundman, B.; Norberg, A.; Gustafson, Y. Morale in the oldest old: The Umeå 85+ study. Age Ageing 2005, 34, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Iinuma, T.; Arai, Y.; Takayama, M.; Takayama, M.; Abe, Y.; Osawa, Y.; Fukumoto, M.; Fukui, Y.; Shioda, Y.; Hirose, N.; et al. Satisfaction with dietary life affects oral health-related quality of life and subjective well-being in very elderly people. J. Oral Sci. 2017, 59, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Miura, H.; Miura, K.; Mizugai, H.; Arai, Y.; Umenai, T.; Isogai, E. Chewing ability and quality of life among the elderly residing in a rural community in Japan. J. Oral Rehabilitat. 2000, 27, 731–734. [Google Scholar] [CrossRef]
- Nakamura, K.; Abe, Y.; Shibayama, T.; Hidaka, K. Required support. An examination of the subjective quality of life and related factors in elderly people with a high functional capacity who need mild care. Nihon Ronen Igakkai Zasshi 2018, 55, 276–283. (In Japanese) [Google Scholar] [CrossRef]
- Näsman, M.; Niklasson, J.; Saarela, J.; Nygård, M.; Olofsson, B.; Conradsson, M.; Lövheim, H.; Gustafson, Y.; Nyqvist, F. Five-year change in morale is associated with negative life events in very old age. Aging Ment. Health 2017, 23, 84–91. [Google Scholar] [CrossRef]
- Murakami, M.; Hirosaki, M.; Suzuki, Y.; Maeda, M.; Yabe, H.; Yasumura, S.; Ohira., T. Reduction of radiation-related anxiety promoted wellbeing after the 2011 disaster: Fukushima Health Management Survey. J. Radiol. Prot. 2018, 38, 1428–1440. [Google Scholar] [CrossRef]
- Murakami, M.; Takebayashi, Y.; Ono, K.; Tsubokura, M. Risk trade-off analysis of returning home and radiation exposure after a nuclear disaster using a happy life expectancy indicator. J. Radiat. Res. 2021, 62, i101–i106. [Google Scholar] [CrossRef]
- Murakami, A.; Sasaki, H.; Pascapurnama, D.; Egawa, S. Noncommunicable Diseases After the Great East Japan Earthquake: Systematic Review, 2011–2016. Disaster Med. Public Health Prep. 2018, 12, 396–407. [Google Scholar] [CrossRef]
- Planning Policy Division, Soma City, Population by Age and Gender According to the Basic Resident Register in Soma City. Juuminkihondaicho Niyoru Nenreibetsu Seibetsu Jinkou. (In Japanese). Available online: https://www.city.soma.fukushima.jp/shiseijoho/somanodata/tokeijoho/3215.html (accessed on 2 March 2020).
- About the Area (Approximate Value) of the Flooded Area Due to the Tsunami (5th Report). Tsunami Niyoru Shinsuihani no Menseki (Gairyakuchi) ni Tsuite (Dai 5 Hou); Geospatial Information Authority of Japan: Tokyo, Japan, 2011. (In Japanese)
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Soper, D. A-Priori Sample Size Calculator for Multiple Regression. Available online: https://www.danielsoper.com/statcalc/calculator.aspx?id=1 (accessed on 24 January 2022).
- Koyano, W. PGC morale scale (Philadelphia Geriatric Center Morale Scale) no kozo—Saikin no Kaiteisagyo ga Mota-rashitamono. Structure of the PGC Philadelphia Geriatric Center Morale Scale-What the Recent Revisions Brought about. Soc. Gerontol. 1989, 29, 64–74. (In Japanese) [Google Scholar]
- Lawton, M.P. Lawton’s PGC Morale Scale; Polisher Research Institute Abramson Center for Jewish Life (formerly the Philadelphia Geriatric Center): North Wales, PA, USA, 2003. [Google Scholar]
- Niklasson, J.; Näsman, M.; Nyqvist, F.; Conradsson, M.; Olofsson, B.; Lövheim, H.; Gustafson, Y. Higher morale is associated with lower risk of depressive disorders five years later among very old people. Arch. Gerontol. Geriatr. 2017, 69, 61–68. [Google Scholar] [CrossRef]
- Näsman, M.; Niklasson, J.; Nygård, M.; Olofsson, B.; Lövheim, H.; Gustafson, Y.; Nyqvist, F. Risk factors for a decrease in high morale in very old people over a 5-year period: Data from two Nordic countries. Eur. J. Ageing 2019, 17, 31–41. [Google Scholar] [CrossRef]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG Index of Competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef]
- Kim, H.; Suzuki, T.; Yoshida, H.; Yoshida, Y.; Sugiura, M.; Iwasa, H.; Kwon, J.; Furuna, T. Characteristics of urban community-dwelling elderly women with multiple symptoms of the geriatric syndrome and related factors. Nihon Koshu Eisei Zasshi 2007, 54, 43–52. (In Japanese) [Google Scholar]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Ya-sumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a com-munity. Nihon Koshu Eisei Zasshi 2003, 50, 1117–1124. (In Japanese) [Google Scholar]
- Kwon, J.; Suzuki, T.; Kumagai, S.; Shinkai, S.; Yukawa, H. Risk factors for dietary variety decline among Japanese elderly in a rural community: A 8-year follow-up study from TMIG-LISA. Eur. J. Clin. Nutr. 2005, 60, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Kurimoto, A.; Awata, S.; Ohkubo, T.; Tsubota-Utsugi, M.; Asayama, K.; Takahashi, K.; Suenaga, K.; Satoh, H.; Imai, Y. Reliability and validity of the Japanese version of the abbreviated Lubben Social Network Scale. Nippon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2011, 48, 149–157. [Google Scholar] [CrossRef]
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Health 1988, 11, 42–52. [Google Scholar] [CrossRef]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an Abbreviated Version of the Lubben Social Network Scale Among Three European Community-Dwelling Older Adult Populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef]
- Rehdanz, K.; Welsch, H.; Narita, D.; Okubo, T. Well-being effects of a major natural disaster: The case of Fukushima. J. Econ. Behav. Organ. 2015, 116, 500–517. [Google Scholar] [CrossRef]
- Oh, D. Discourses about “Kodokushi” (Solitary Death) Phenomenon—Study Based on the Analysis of Articles from Asahi Newspaper. Waseda J. Soc. Sci. 2017, 29, 122–137. (In Japanese) [Google Scholar]
- Fukukawa, Y.; Kawaguchi, K. A nationwide survey of Japanese municipalities on solitary deaths and countermeasures. Nihon Koshu Eisei Zasshi Jpn. J. Pub. Health 2011, 58, 959–966. (In Japanese) [Google Scholar]
- Yoshida, S. Kasetsu Fukkou Jutaku deno “Kodokushi” 614 nin, 3 Ken no 10 nen. Solitary Deaths in Temporary and Reconstructed Housing, 614 People, 10 Years in 3 Prefectures; The Asahi Shinbun. 2020. Available online: https://www.asahi.com/articles/ASP3762H2P35UTIL0BR.html (accessed on 24 January 2022). (In Japanese).
- Tachiya, H. Kodoku-shi. Solitary Death. Available online: https://www.city.soma.fukushima.jp/shinososhiki/hishoka/shichoshitsu/mailmaga/back_number/2015/5087.html (accessed on 24 January 2022). (In Japanese).
- Morita, S.; Nishi, K.; Furukawa, T.; Hitosugi, M. Investigation of the condition and background of solitary death among the elderly. J. Jpn. Counc. Traffic Sci. 2016, 15, 38–43. (In Japanese) [Google Scholar]
- Petersen, P.E.; Yamamoto, T. Improving the oral health of older people: The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2005, 33, 81–92. [Google Scholar] [CrossRef]
- Ohara, Y.; Yoshida, N.; Kono, Y.; Hirano, H.; Yoshida, H.; Mataki, S.; Sugimoto, K. Effectiveness of an oral health educational program on community—Dwelling older people with xerostomia. Geriatr. Gerontol. Int. 2015, 15, 481–489. [Google Scholar] [CrossRef]
- Hiroyuki, K. Efficacy of Mastication Training Using Ice Chips. Jpn. J. Dysphagia Rehabil. 2020, 24, 153–161. (In Japanese) [Google Scholar]
- Kugimiya, Y.; Motokawa, K.; Yamamoto, K.; Hayakawa, M.; Mikami, Y.; Iwasaki, M.; Ohara, Y.; Shirobe, M.; Edahiro, A.; Watanabe, Y.; et al. Relationship between the rate of a decreased oral function and the nutrient intake in community—Dwelling older persons: An examination using oral function-related items in a questionnaire for latter-stage elderly people. Nihon Ronen Igakkai Zasshi 2021, 58, 91–100. (In Japanese) [Google Scholar] [CrossRef]
- Hamashima, C. The quality of life in aged people. Nihon Eiseigaku Zasshi 1994, 49, 533–542. (In Japanese) [Google Scholar] [CrossRef]
- Litwin, H. Social Network Type and Morale in Old Age. Gerontology 2001, 41, 516–524. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).