Abstract
According to Italian Essential Levels of Assistance (ELA), a colonoscopy is strongly recommended after a positive fecal occult blood test (FOBT) due to its effectiveness in early colorectal cancer detection. Despite the evidence, the Palermo province population (Italy), after a positive FOBT, have a lower colonoscopy adherence compared to Italian standards. This cross-sectional study analyzed patients’ perceptions of colonoscopy procedures to understand the reasons for non-adherence. Patients with a positive FOBT who did not undergo a colonoscopy within the national organized screening program were administered a telephone interview based on the Health Belief Model (HBM) questionnaire. The number of non-compliant patients with a colonoscopy after a positive FOBT were 182, of which 45 (25.7%) patients had undergone a colonoscopy in another healthcare setting. Among the HBM items, in a multivariate analysis only perceived benefits were significantly associated with colonoscopy adherence (aOR = 6.7, p = 0.03). Health promotion interventions should focus on the importance of the benefits of colorectal screening adherence to prevent colorectal cancer, implementing health communication by healthcare workers that have closer contacts with people, as general practitioners.
1. Introduction
Colorectal cancer (CRC) still has a considerable impact on population health and patient survival. In Italy, CRC affected at least 49,000 patients in 2019, whose male/female ratio was 1:2 [1]. In Sicily, one of the largest Italian administrative regions, there were estimated to be 3950 new cases of CRC during 2019, with a male/female ratio of 1:1 [1]. Even though the trend of new cases seemed to decline in the last few years, CRC has been estimated to cause about 11–12% of all oncological diseases in 2020 [2]. According to the most recent evaluations, 7.8–14.0/100,000 Italians died due to colorectal cancer during 2021, a lower proportion compared to that of 2015, which was 13.2–13.6% [3]. These data could suggest that colorectal cancer screening is the most efficacious preventive strategy, which is strongly recommended for people aged 50–69 years old [4,5].
According to Italian law [6], the essential levels of assistance (ELA) has included costless organized CRC screening for the target population aged 50–69 years old since 2006, with two steps: the first is the fecal occult blood test (FOBT); colonoscopy is the second-level examination, which is required if the previous test is positive [5].
In Italy, adherence to CRC screening was almost 45% from 2011 to 2019 [7]. CRC screening in Sicily has been made available in all the administrative regional areas since 2012, following the national oncological screenings guidelines [8]. Although fully available, CRC adherence in Sicily was lower than the national figure, with a coverage of 28% from 2012 to 2019 [7]. In detail, CRC screening adherence in those living in the Palermo area, the most populated province of Sicily, was 13.5% in 2018 [9], which increased to 22% in 2019 [10].
According to Doubeni et al., lethal outcomes due to CRC could be reduced by 67% in patients undergoing a colonoscopy exam [11]. The same observation was found in Italy, where colonoscopy adherence reduced both new cases and deaths by 1.3 and 2.4 times, respectively [2]. Despite its effectiveness in the early diagnosis of CRC [4,12], low adherence to colonoscopy among positive FOBT patients is still a challenge for public health in many countries [13]. Worldwide, a significant percentage of patients—between 10% and 45%—with a positive FOBT avoided a colonoscopy for several reasons, such as misinformation by healthcare workers [13]. In Europe, full adherence to colonoscopy after a positive FOBT has still not been achieved [14]. Although the European standard for adherence to secondary colonoscopy is 85–90%, this value has not been reached due to 8–27% non-compliance among patients [14]. In Italy, the recommended level of adherence to colonoscopy as second-level screening is 90%, but the updated adherence is nearly 80% [11]. The colonoscopy non-compliance trend in the years 2017–2019 progressively decreased among the targeted Italian population for CRC screening: 23.5% patients were non-adherent in 2017–2018 and 21.5% were non-adherent in 2019 [15]. To investigate perceptions about colonoscopy within the context of the national organized CRC screening program among non-compliant subjects with a positive FOBT, it was necessary to select a theoretical model to explore individuals’ reasons for avoiding such a preventive procedure. The Health Belief Model (HBM) was originated to interpret population behavior in relation to screening and it is useful when considering behaviors rarely performed, such as a colonoscopy as the second level of organized CRC screening [16].
The main aim of this study is the assessment of second-level colonoscopy adherence among FOBT-positive non-compliant patients aged 50–69 years old of both sexes within the national organized CRC screening program, using a questionnaire based on the HBM. The secondary objective is to explore the factors associated with colonoscopy adherence as the second-level alternative setting.
2. Materials and Methods
2.1. Study Design
This cross-sectional study involved residents in Palermo area aged 50–69 years. It was conducted after a period of one year from CRC screening invitation (from July to August 2020). A telephone interview about colonoscopy adherence was administered to the target population, after a positive FOBT result. The management of the health data required collaboration between the Public Health Department at the University of Palermo, Italy and the Local Health Unit of Palermo (LHU). The local ethic committee (Palermo 1) approved the study on 24 June 2020.
2.2. Study Population
The administrative area of Palermo is the biggest in Sicily, covering 5009.28 km2 and containing 82 municipalities [17]. According to data from the National Statistics Institute, on 1 January 2019 the Palermo area had 1,231,602 inhabitants, of which 344,138 (27.9%) were 50–69-year-old residents [18]. The population density of the whole Palermo area was 248.3 inhabitants per km2 until 9 October 2011, which is 16 times lower than Palermo city (4094.60 inhabitants per km2) [17].
Since the colorectal screening services started in 2012 [8], each Sicilian resident of the study area aged 50–69 years receives an invitation letter from the LHU of Palermo [19,20] which contains all the necessary information about the performance of a FOBT [20]. If the patient does not adhere to the FOBT screening campaign after six months, the LHU of Palermo recalls non-compliant patients to invite them to the colorectal cancer screening [20]. Any resident patient with a positive FOBT can access a hospital located in the Palermo area to undergo the second level of colorectal screening [9,10]. All patients who did not undergo the second level of screening (colonoscopy) after a positive result for the first level of screening (FOBT) were eligible for the study.
2.3. Telephone Interview
All eligible patients received a phone call and a questionnaire was administered about colonoscopy perceptions. The questionnaire included a total of 20 questions which were divided into three sections: the first section solicited socio-demographic information, such as sex, age, educational level, and occupation; the second focused on colonoscopy adherence in a private context, sources of information about CRC prevention, the organization of other healthcare services (for those compliant with colonoscopy), such as attendance times for undergoing colonoscopies in other settings after a positive FOBT result and the issuing of a colonoscopy report, along with the reasons for not undergoing a colonoscopy; the third section was a revised HBM questionnaire using a five-point Likert scale. The range of agreement was from a minimum value of 1 (“I strongly disagree”) to a maximum of 5 (“I strongly agree”). HBM scores considered four key elements: perceived susceptibility to colorectal cancer due to increasing age; perceived severity of colorectal cancer disability and mortality; perceived barriers to accessing colonoscopy services; the perceived benefit of the effectiveness and perceptions of the safety of colonoscopy [21,22]. Each item consisted of two questions, as shown in Table 1.

Table 1.
HBM questionnaire with four domains (susceptibility, severity, barriers, and benefits) to detect the reasons for colonoscopy refusal.
2.4. Inclusion and Exclusion Criteria
Patients were included in the study if they met the following inclusion criteria: residence in the Palermo area, age between 50 and 70 years, positive result for FOBT performed between 1 January 2018 and 30 June 2019, and non-compliance with colonoscopy recall within the organized colorectal cancer screening program. Patients who were unreachable by phone after several attempts at calling or who were not fully respondent to the HBM section of the questionnaire were excluded.
2.5. Statistical Analysis
Absolute and relative frequencies were calculated for both qualitative and quantitative variables. Pearson’s chi-squares test was performed for all the factors affecting colonoscopy compliance, comparing non-compliant patients with compliant patients with other-setting colonoscopy. The Skewness and Kurtosis test examined the normal distribution of quantitative variables, from which the choice of the mean or median and related measures of dispersion, such as standard deviation (SD) or interquartile range (IQR), were derived.
The HBM total score was the sum of all the HBM question scores on the Likert scale, using the median as a cut-off (median = 27). The minimum and maximum obtainable score was 8 and 40, respectively. The HBM domain score was then re-categorized according to the following values: 0 = 1 (“I strongly disagree”) and/or 2 (“I disagree”) or 1 = 3 (“I neither agree nor disagree”), 4 (“I agree”), and/or 5 (“I strongly agree”). The re-categorized sum of the scores for each domain of the HBM could have a maximum level of 2 and the re-categorized score was included in the Pearson’s chi-squared test, as well as a bivariate and multivariate analysis.
The bivariate analysis evaluated each independent variable linked to second-level colonoscopy compliance. Only the factors with p < 0.80 in the bivariate analysis were included in the multivariate backward regression model. Crude and adjusted odds ratios (cOR and aOR, respectively) with related p-values were reported. All the results were statistically significant, with the p-value set as ≤0.05. According to Taş et al., the assessment of HBM consistency (total and for each item) was tested by Cronbach’s alpha, with a value above 0.60 assumed to indicate fulfilment [23]. Statistical analyses were performed by Stata/SE 14.2 (Copyright 1985–2015, StataCorp LLC, College Station, TX, USA. Revision 29 January 2018).
3. Results
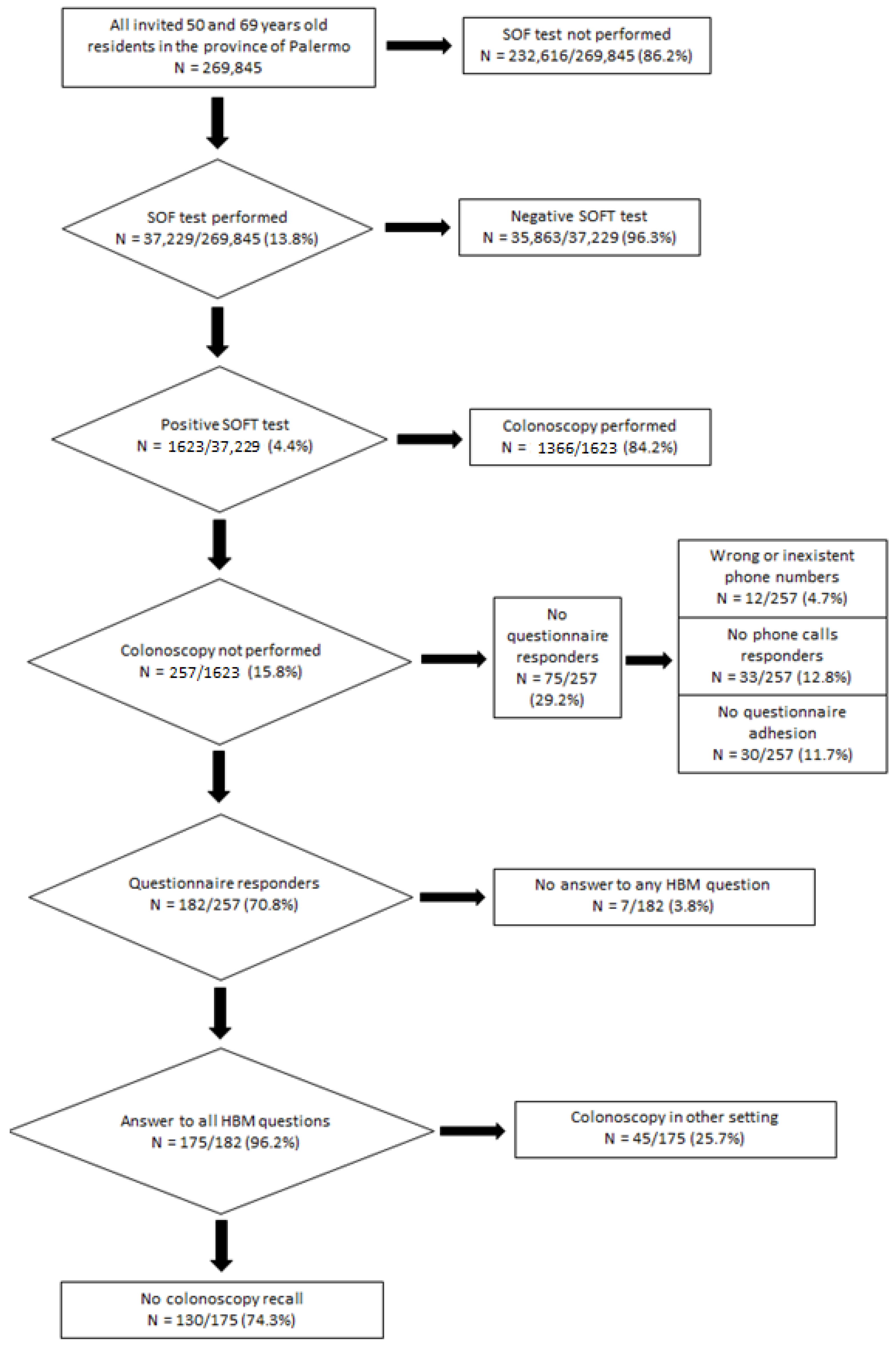
Overall, 269,845 residents in the province of Palermo received an invitation letter to undergo a FOBT between 1 January 2018 and 30 June 2019. Of these, only 37,229 (13.8%) had underwent a FOBT. The number of patients with a positive FOBT result was 1623 (4.4%). Of these, 1366 (84.2%) underwent the second level of organized colorectal screening, while 257 (15.8%) were non-compliant with colonoscopy within six months of a positive FOBT. Among this group, 75 (29.2%) were excluded from the study for the following reasons: 12 (16.0%) had wrong or non-existent phone numbers; 33 (44.0%) failed to respond after several attempts; 30 (40.0%) refused to answer the questionnaire.
A total of 182 people were eligible for the telephone interview; 175 of them (96.2%) answered all the questions and were included in the study, whereas 7 (3.8%) patients did not answer the HBM questions. A total of 45 (25.7%) interviewed patients had a colonoscopy performed in another healthcare setting. On the other hand, 130 (74.3%) patients were non-compliant with colonoscopy (Figure 1).
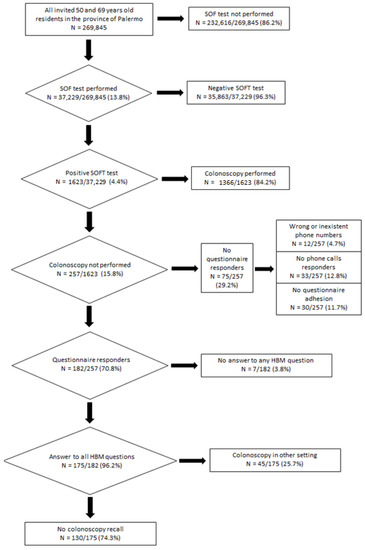
Figure 1.
Flowchart of patients involved in the study.
The sociodemographic characteristics of those who were non-compliant with secondary CRC screening are shown in Table 2. Most of them were female (52.7%, n = 92), residents in Palermo city (51.4%, n = 90), and aged under 64 years (57.1%, n = 100). The prevalent education level was middle school (42.3%, n = 74) and they were more frequently married (80.0%, n = 140).
Table 2.
Characteristics of patients with a positive FOBT who did not undergo the second-level examination as part of the organized colorectal screening colonoscopy program.
The main information source for CRC screening was a general practitioner (85.7%, n = 150). Healthcare professionals’ ability to provide clear information about CRC screening services were considered satisfactory enough for most of the patients (79.4%, n = 139). On the other hand, the main reason for non-colonoscopy compliance in the organized service was misinformation about colonoscopy after a positive FOBT (70.0%, n = 91), followed by undefined personal reasons (23.1%, n = 30). Most residents compliant with colonoscopy in other settings reported having undergone the second-level screening after a positive FOBT (88.9%, n = 40), but the colonoscopy report could be ascertained for only a few of them (24.4%, n = 11).
The HBM questionnaire detected perceptions about colonoscopy in patients with a positive FOBT result. The Cronbach’s alpha for all HBM questions was 0.78, but this value changed according to the considered item (susceptibility: 0.66; severity: 0.94; barriers: 0.56; benefits: 0.69). The median of the HBM score was 27 (IQR = 24–31). The highest scores for patients concerned perceived benefits and perceived severity (both 81.7%, n = 143), followed by perceived susceptibility (74.9%, n = 131) and perceived barriers (59.4%, n = 104). Although patients who adhered to colonoscopy in another setting had a higher total HBM score than non-compliant patients (66.7% vs. 57.7%), this result was not statistically significant (p = 0.29). On the other hand, perceived benefits of colonoscopy were significantly greater among patients undergoing colonoscopy in another setting compared to patients who did not undergo the procedure (93.3% vs. 77.7%, p = 0.02), whereas perceived severity was only marginally significant (91.1% vs. 78.5%, p = 0.06).
Bivariate and multivariate logistic regression analysis examined all factors associated with a secondary colonoscopy performed in another setting (Table 3). Although communication about CRC screening effectiveness from healthcare workers (aOR = 4.5, p = 0.29), Internet sources (aOR = 2.44, p = 0.54), and general practitioners (aOR = 1.65, p = 0.66) seemed to increase colonoscopy compliance, these results were not statistically significant. The only factor significantly associated with the performance of a colonoscopy in another healthcare setting was the perceived benefits score <2 vs. ≥2 (aOR = 6.7, p = 0.03).
Table 3.
Bivariate and multivariate logistic regression analysis of all the factors associated with colonoscopy acceptance as the second-level screening.
4. Discussion
Using the HBM model, this study analyzed perceptions of colonoscopy as the second level of screening among Palermo province residents with a positive FOBT result who did not undergo a colonoscopy in accordance with CRC screening guidelines [5].
Considering both colonoscopy within the context of the national organized screening program (84.2%) and in another healthcare setting (2.8%), the total percentage of compliant patients (86.9%) in the province of Palermo was lower than national standards (90%) [7,16]. On the other hand, colonoscopy adherence in the province of Palermo was higher than the national mean in the years 2017–2018 (76.5%) and 2019 (78.5%) [15]. These data underline the need to monitor colonoscopy adherence in contexts other than those of the national-level program in order to achieve an overall estimate of colonoscopy adherence.
The main factor influencing adherence to colonoscopy in other settings was the perception of benefits, which seems to determine a near seven-fold increase in the odds of accepting a colonoscopy. These results were similar to another study conducted among Afro-American people in the USA, where it was shown that colonoscopy adherence improved among patients with greater perceptions of benefits [24]. Another study conducted in France among siblings showed that a familial medical history for CRC increased perceptions of benefit and adherence to colonoscopy (aOR = 3.9, p = 0.0037) [25]. On the other hand, in a study conducted within the context of national organized screening in Southern Korea, both severity (OR = 0.39, 95% CI 0.25–0.61) and barrier (OR = 2.15, 95% CI 1.23–3.78) perception influenced colonoscopy adherence given a positive FOBT [21]. Overall, perceptions about CRC and the reason for adherence to colonoscopy might change from country to country, depending on several demographic and socio-cultural factors [21,25]. Furthermore, healthy people have poorer risk perception for being affected by cancer [26]. In this context, several cultural points of view or a lack of information about the effectiveness of oncological prevention strategies might determine an underestimation of the worsening prognosis of an asymptomatic cancer or early signals of CRC, such as bleeding [14,27]. This information needs to be underlined by healthcare workers concerned with health promotion in relation to long-lasting diseases, such as cancer, in order to improve CRC screening adherence [14,23]. Consequently, an analysis of factors that affect CRC screening adherence, according to a behavioral model, should be performed before planning interventions aiming to increase second-level screening adherence.
According to the HBM construction [26], benefit perception is influenced by the nuisance and efficacy of CRC screening. The annoyance due to colonoscopy procedures could be another reason for avoiding colonoscopy [5,14,27]. In detail, some personal reasons, such as the fear of pain during the procedure (aOR = 0.3, p = 0.009) and discomfort (aOR = 0.3, p = 0.016), negatively affected colonoscopy adherence [5]. Fifty-nine percent of European patients compliant with colonoscopy declared that better information and communication could help patients to control the fear of pain [28]. Furthermore, colonoscopy centers in Italy provided general anesthesia for more anxious patients [29]. According to a survey, barely half of Italian patients were sedated before undergoing colonoscopy [28].
The most frequent reason reported by patients for not undergoing secondary colonoscopy is misinformation about colonoscopy after a positive FOBT result. Similar data were observed in Europe, where 55% of patients reported misinformation about the usefulness of this medical procedure as their reason for non-compliance with colonoscopy [28]. A strategy to counteract misinformation could be to underline the disability due to CRC: affected patients have a lower quality of life due to negative consequences of surgical and medical treatments, such as painful experiences, the onset of low anterior resection syndrome, and colostomy-related discomfort. For these reasons, healthcare professionals, especially general practitioners, should highlight colonoscopy safety (5.4–17.5/10,000 perforations and severe bleedings) and its effectiveness in decreasing deaths due to CRC [12,30].
Low accessibility to screening centers can be another relevant aspect of reduced adherence [31]. In Palermo province, there was only one healthcare facility performing colonoscopy as the second step of CRC screening [9]. This can increase the attendance time required to perform the procedure after patients were informed of a positive first-level screening test [31]. Furthermore, Italian guidelines recommend performing the second level of screening within 30 days after the positive FOBT result [15]. Consequently, well informed patients might choose to undergo a colonoscopy in another setting to have the test performed earlier [31].
The HBM is an individual-level model of behavioral change useful when people should perform a non-habitual preventive action [26,32]. This model allows understanding of the underlying belief that militates against performing a preventive action. However, the results can differ among several screening practices, such as cervical cancer and CRC screening, performed by individuals living in the same area. For example, another study conducted among Sicilian women exploring HBM factors associated with cervical screening adherence showed a major role of susceptibility perception [33]. The different roles of beliefs in different screening programs can be related to perceptions of how invasive a test is. Indeed, colonoscopy might be perceived to be more painful than a Pap test or a HPV DNA test. Consequently, healthcare workers who want to plan a health promotion intervention should focus on a particular insight regarding preventive strategies and what a local population believes.
Some limitations of this study should be considered. Recall and missing bias might have influenced the results of this study. A few eligible patients were unreachable and their medical information was not collectable otherwise. No medical examination could verify the answers of telephone questionnaires, introducing either recall and desirability bias, and colonoscopy reports in other settings were undetectable for most of the participants, as were colonoscopy contraindications. Nevertheless, this study showed that perceptions of benefit by patients with a positive FOBT should be the set of beliefs to improve in order to reach sustainable adherence to the second level of screening in Sicily. This should be considered a health system priority, especially considering that subjects who were non-compliant with colonoscopy may need very demanding healthcare services in the next few years.
5. Conclusions
Among Palermo area residents, benefit perception is the main factor associated with higher adherence to secondary colonoscopy to prevent CRC.
Health promotion interventions should focus on the importance of CRC screening adherence to prevent CRC and the implementation of effective health communication by those healthcare workers who have closer contacts with people, as general practitioners. More extensive studies should investigate colonoscopy perceptions within the national organized screening program to improve healthcare services performance.
Author Contributions
Conceptualization, V.R., M.V., P.I. and A.C.; methodology, V.R. and A.D.; software, V.R.; validation, A.D., V.R. and G.M.; formal analysis, V.R. and G.M.; investigation, A.D.; resources, M.V., A.C., E.A. and W.M.; data curation, A.D. and G.M.; writing—original draft preparation, V.R.; writing—review and editing, G.M., P.I., E.A., W.M. and V.R.; visualization, P.I.; supervision, V.R.; project administration, V.R.; funding acquisition, M.V., A.C., E.A., W.M. and V.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Palermo 1 (24 June 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be made available upon reasonable request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- AIOM, AIRTUM. I Numeri Del Cancro in Italia 2019. Available online: https://www.aiom.it/wp-content/uploads/2019/09/2019_Numeri_Cancro-operatori-web.pdf (accessed on 8 June 2020).
- AIOM. I Numeri Del Cancro in Italia 2020. Available online: https://www.aiom.it/wp-content/uploads/2020/10/2020_Numeri_Cancro-operatori_web.pdf (accessed on 2 December 2021).
- AIOM. Registri Tumori Italiani–Gruppo di Lavoro Numeri del Cancro 2021, SIAPEC-IAP; Fondazione AIOM.; ONS.; PASSI e PASSI d’argento. I Numeri Del Cancro in Italia 2021. Available online: https://www.aiom.it/wp-content/uploads/2021/10/2021_NumeriCancro_web.pdf (accessed on 23 February 2022).
- Healy, M.A.; Thirumurthi, S.; You, Y.N. Screening High-Risk Populations for Colon and Rectal Cancers. J. Surg. Oncol. 2019, 120, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Bocci, G.; Troiano, G.; Messina, G.; Nante, N.; Civitelli, S. Factors That Could Influence Women’s Participation in Colorectal Cancer Screening: An Italian Study. Ann. Ig. Med. Prev. E Comunita 2017, 29, 151–160. [Google Scholar] [CrossRef]
- Italia Decreto Del Presidente Del Consiglio Dei Ministri 12 Gennaio 2017. Definizione e Aggiornamento Dei Livelli Essenziali Di Assistenza, Di Cui All’articolo 1, Comma 7, Del Decreto Legislativo 30 Dicembre 1992, n. 502. Gazzetta Uff. Della Repubblica Ital. Ser. Gen. Suppl Ordin. N 65 18-03-2017. Available online: https://www.gazzettaufficiale.it/eli/id/2017/03/18/17A02015/sg (accessed on 8 June 2020).
- Screening Colorettale Dati Sorveglianza Passi. Available online: https://www.epicentro.iss.it/passi/dati/ScreeningColorettale (accessed on 8 June 2020).
- Regione Siciliana. Assessorato della Salute Decreto 18 Settembre 2012. Direttive Regionali per l’esecuzione Degli Screening Oncologici in Sicilia. Available online: https://pti.regione.sicilia.it/portal/page/portal/PIR_PORTALE/PIR_LaStrutturaRegionale/PIR_AssessoratoSalute/PIR_AreeTematiche/PIR_Screeningoncologici/Decreto%20direttive%20screening%20oncologici.pdf (accessed on 8 June 2020).
- ASP 6 Palermo Relazione Sulla Performance 2018. Available online: http://www.asppalermo.org/Archivio/trasparenza/performance/2018%20Relazione%20sulla%20Performance%20-%20completa.pdf (accessed on 8 June 2020).
- ASP 6 Palermo Relazione Sulla Performance 2019. Available online: http://www.asppalermo.org/Archivio/trasparenza/performance/Relazione%20sulla%20performance%202019-completa.pdf (accessed on 8 June 2020).
- Doubeni, C.A.; Corley, D.A.; Quinn, V.P.; Jensen, C.D.; Zauber, A.G.; Goodman, M.; Johnson, J.R.; Mehta, S.J.; Becerra, T.A.; Zhao, W.K.; et al. Effectiveness of Screening Colonoscopy in Reducing the Risk of Death from Right and Left Colon Cancer: A Large Community-Based Study. Gut 2018, 67, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.A.; Kasi, P.M.; Wallace, M.B. Colorectal Cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef]
- Correia, A.; Rabeneck, L.; Baxter, N.N.; Paszat, L.F.; Sutradhar, R.; Yun, L.; Tinmouth, J. Lack of Follow-up Colonoscopy after Positive FOBT in an Organized Colorectal Cancer Screening Program Is Associated with Modifiable Health Care Practices. Prev. Med. 2015, 76, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Sali, L.; Grazzini, G.; Mascalchi, M. CT Colonography: Role in FOBT-Based Screening Programs for Colorectal Cancer. Clin. J. Gastroenterol. 2017, 10, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Osservatorio Nazionale Screening Lo Screening Colorettale. Dati Di Attività Dal 2013 al 2019. Available online: https://www.osservatorionazionalescreening.it/content/lo-screening-colorettale (accessed on 17 July 2021).
- Restivo, V.; Palmeri, S.; Bono, S.; Caracci, F.; Russo Fiorino, G.; Foresta, A.; Gaglio, V.; Graziano, G.; Marchese, V.; Maniglia, M.; et al. Knowledge and attitudes of parents after the implementation of mandatory vaccination in kindergartens of Palermo, Italy. Acta Biomed. 2020, 91 (Suppl. 3), 41–47. [Google Scholar] [CrossRef]
- Istituto Nazionale di Statistica-ISTAT Principali Statistiche Geografiche sui Comuni. Available online: https://www.istat.it/it/archivio/156224 (accessed on 21 April 2021).
- Istituto Nazionale di Statistica-ISTAT Popolazione Residente al 1° Gennaio 2019 per Età, Sesso e Stato Civile. Available online: http://demo.istat.it/popres/index.php?anno=2019&lingua=ita (accessed on 22 April 2021).
- Regione Siciliana. Direttive per l’esecuzione Degli Screening Oncologici in Sicilia. 2012. Available online: https://pti.regione.sicilia.it/portal/page/portal/PIR_PORTALE/PIR_LaStrutturaRegionale/PIR_AssessoratoSalute/PIR_AreeTematiche/PIR_Screeningoncologici (accessed on 8 June 2020).
- Ministero della Salute Gli Screening Oncologici Vademecum. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_774_allegato.pdf (accessed on 8 June 2020).
- Choi, E.; Jeon, J.; Kim, J. Factors Influencing Colonoscopy Behaviour among Koreans with a Positive Faecal Occult Blood Tests. Eur. J. Cancer Care 2019, 28, e13008. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, E.E. Access to Health Care, Beliefs, and Behaviors about Colorectal Cancer Screening among Korean Americans. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 2021–2027. [Google Scholar] [CrossRef] [PubMed]
- Taş, F.; Kocaöz, S.; Çirpan, R. The Effect of Knowledge and Health Beliefs about Colorectal Cancer on Screening Behaviour. J. Clin. Nurs. 2019, 28, 4471–4477. [Google Scholar] [CrossRef] [PubMed]
- Kiviniemi, M.T.; Jandorf, L.; Erwin, D.O. Disgusted, Embarrassed, Annoyed: Affective Associations Relate to Uptake of Colonoscopy Screening. Ann. Behav. Med. Publ. Soc. Behav. Med. 2014, 48, 112–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taouqi, M.; Ingrand, I.; Beauchant, M.; Migeot, V.; Ingrand, P. Determinants of Participation in Colonoscopic Screening by Siblings of Colorectal Cancer Patients in France. BMC Cancer 2010, 10, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.-R.; Tauscher, J.; Cardel, M. Distrust in Health Care and Cultural Factors Are Associated with Uptake of Colorectal Cancer Screening in Hispanic and Asian Americans. Cancer 2018, 124, 335–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, D.; Serenity, M.; Conn, L.G.; Bravo, C.A.; McCurdy, B.R.; Dubé, C.; Baxter, N.N.; Paszat, L.; Rabeneck, L.; Peters, A.; et al. Reasons For Lack of Follow-up Colonoscopy among Persons with a Positive Fecal Occult Blood Test Result: A Qualitative Study. Am. J. Gastroenterol. 2018, 113, 1872–1880. [Google Scholar] [CrossRef] [PubMed]
- Amlani, B.; Radaelli, F.; Bhandari, P. A Survey on Colonoscopy Shows Poor Understanding of Its Protective Value and Widespread Misconceptions across Europe. PLoS ONE 2020, 15, e0233490. [Google Scholar] [CrossRef] [PubMed]
- Osservatorio Nazionale Screening; Gruppo Italiano Screening Colorettale (GISCoR) Le 100 Domande Sullo Screening Colorettale 2018. Available online: https://www.osservatorionazionalescreening.it/content/le-100-domande-sullo-screening-colorettale-e-sullo-screening-con-la-sigmoidoscopia (accessed on 8 June 2020).
- Lin, J.S.; Perdue, L.A.; Henrikson, N.B.; Bean, S.I.; Blasi, P.R. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2021, 325, 1978–1998. [Google Scholar] [CrossRef] [PubMed]
- Zappa, M. I Programmi Organizzati Di Screening Aiutano a Superare Le Disuguaglianze in Prevenzione? Available online: https://plotly.com/~sergio_cima/632/nord-centro-sud-isole-italia/ (accessed on 31 May 2020).
- Almadi, M.A.; Alghamdi, F. The Gap between Knowledge and Undergoing Colorectal Cancer Screening Using the Health Belief Model: A National Survey. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2019, 25, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Restivo, V.; Costantino, C.; Marras, A.; Napoli, G.; Scelfo, S.; Scuderi, T.; Casuccio, A.; Cernigliaro, A.; Giusti, A.; Spila Alegiani, S. Pap Testing in a High-Income Country with Suboptimal Compliance Levels: A Survey on Acceptance Factors among Sicilian Women. Int. J. Environ. Res. Public. Health 2018, 15, 1804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).