
Patient Navigation—Who Needs What? Awareness of Patient Navigators and Ranking of Their Tasks in the General Population in Germany

 , , and
, , and
Abstract
:1. Introduction
Aim of the Study
2. Materials and Methods
2.1. Study Design
2.2. Assessment of PN Awareness and Importance of Navigator Tasks
‘In healthcare, there is a service provided by PNs who support and advise patients over a longer period of time after an acute illness/event such as stroke, or a longer-lasting disease such as cancer, e.g., in filling out applications. Have you heard of PNs?’
- assistance with administrative matters, e.g., applications for rehabilitation care,
- provision of healthcare information,
- counseling and support for emotional problems resulting from the disease’.
2.3. Sociodemographic Characteristics and Health Status
2.4. Statistical Analysis
3. Results
3.1. The Most Important Tasks of PNs
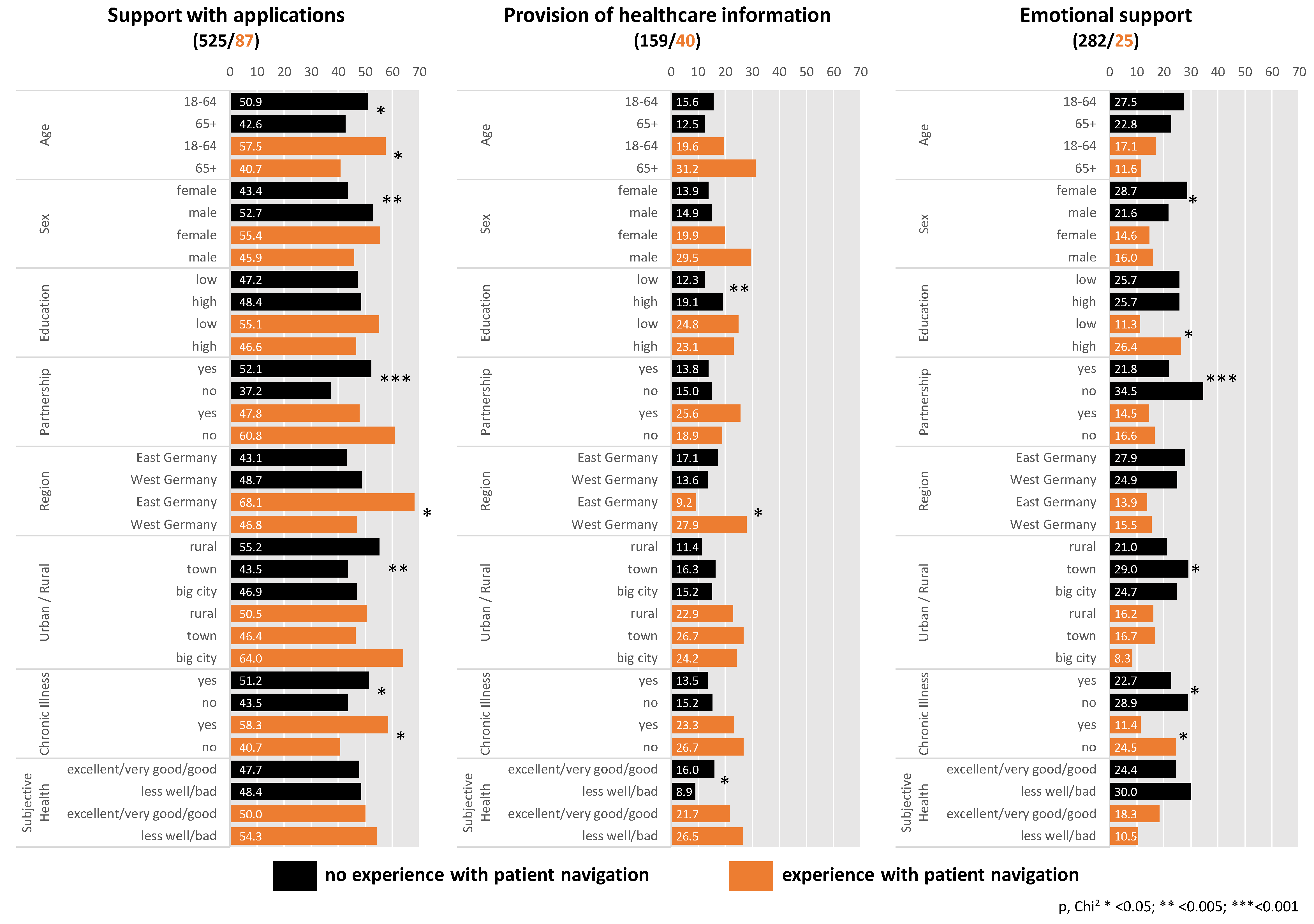
3.2. Support with Applications
3.3. Provision of Healthcare Information
3.4. Emotional Support
4. Discussion
4.1. Comparison between Persons with and without Experience of PNs
4.2. Support with Applications
4.3. Provision of Health Information
4.4. Emotional Support
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fügemann, H.; Goerling, U.; Gödde, K.; Desch, A.K.; Müller-Nordhorn, J.; Mauckisch, V.; Siegerink, B.; Rieckmann, N.; Holmberg, C. What do people with lung cancer and stroke expect from patient navigation? A qualitative study in Germany. BMJ Open 2021, 11, e050601. [Google Scholar] [CrossRef] [PubMed]
- Glaeske, G.; Hoffmann, F. Der Wettbewerb der Leitlinien bei älteren Menschen–Multimorbidität und Polypharmazie als Problem. Neuro Geriatr. 2009, 6, 115–119. [Google Scholar]
- Ludt, S.; Heiss, F.; Glassen, K.; Noest, S.; Klingenberg, A.; Ose, D.; Szecsenyi, J. Patients’ perspectives beyond sectoral borders between inpatient and outpatient care-patients’ experiences and preferences along cross-sectoral episodes of care. Gesundh. (Bundesverb. Arzte Offentlichen Gesundh. (Ger.)) 2013, 76, 359–365. [Google Scholar]
- Nolte, E.; Knai, C.; Hofmarcher, M.; Conklin, A.; Erler, A.; Elissen, A.; Flamm, M.; Fullerton, B.; Sönnichsen, A.; Vrijhoef, H.J. Overcoming fragmentation in health care: Chronic care in Austria, Germany and The Netherlands. Health Econ. Policy Law 2012, 7, 125–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaeffer, D.; Berens, E.M.; Vogt, D. Health Literacy in the German Population. Dtsch. Arztebl. Int. 2017, 114, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Tille, F.; Weishaar, H.; Gibis, B.; Schnitzer, S. Patients’ understanding of health information in Germany. Patient Prefer. Adher. 2019, 13, 805–817. [Google Scholar] [CrossRef] [Green Version]
- Gödde, K.; Fügemann, H.; Müller-Nordhorn, J.; Grimberg, M.; Goerling, U.; Siegerink, B.; Rieckmann, N.; Holmberg, C. Structured Collection of Data on Support Offers for Lung Cancer and Stroke Patients in Berlin. Gesundh. (Bundesverb. Arzte Offentlichen Gesundh. (Ger.)) 2020, 84, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Stumm, J.; Peter, L.; Sonntag, U.; Kümpel, L.; Heintze, C.; Döpfmer, S. Non-medical aspects in the care for multimorbid patients in general practice. What kind of support and cooperation is desired? Focus groups with general practitioners in Berlin. Z. Evidenz Fortbild. Qual. Gesundh. 2020, 158, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Stickel, A.; Gröpper, S.; Pallauf, A.; Goerling, U. Patients’ knowledge and attitudes towards Cancer peer support programs. Oncology 2015, 89, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.K.; Humiston, S.G.; Meldrum, S.C.; Salamone, C.M.; Jean-Pierre, P.; Epstein, R.M.; Fiscella, K. Patients’ experiences with navigation for cancer care. Patient Educ. Couns. 2010, 80, 241–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, H.P. The origin, evolution, and principles of patient navigation. Cancer Epidemiol. Prev. Biomark. 2012, 21, 1614–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBrien, K.A.; Ivers, N.; Barnieh, L.; Bailey, J.J.; Lorenzetti, D.L.; Nicholas, D.; Tonelli, M.; Hemmelgarn, B.; Lewanczuk, R.; Edwards, A.; et al. Patient navigators for people with chronic disease: A systematic review. PLoS ONE 2018, 13, e0191980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peart, A.; Lewis, V.; Brown, T.; Russell, G. Patient navigators facilitating access to primary care: A scoping review. BMJ Open 2018, 8, e019252. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.H.; Wilson, S.; McConigley, R. Experiences of cancer patients in a patient navigation program: A qualitative systematic review. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 136–168. [Google Scholar] [CrossRef]
- van Ee, I.B.; Hagedoorn, M.; Slaets, J.P.; Smits, C.H. Patient navigation and activation interventions for elderly patients with cancer: A systematic review. Eur. J. Cancer Care (Engl.) 2017, 26, e12621. [Google Scholar] [CrossRef] [PubMed]
- Freund, K.M.; Battaglia, T.A.; Calhoun, E.; Dudley, D.J.; Fiscella, K.; Paskett, E.; Raich, P.C.; Roetzheim, R.G.; Patient Navigation Research Program Group. National Cancer Institute Patient Navigation Research Program: Methods, protocol, and measures. Cancer 2008, 113, 3391–3399. [Google Scholar] [CrossRef] [PubMed]
- Porzig, R.; Neugebauer, S.; Heckmann, T.; Adolf, D.; Kaskel, P.; Froster, U.G. Evaluation of a cancer patient navigation program (“Onkolotse”) in terms of hospitalization rates, resource use and healthcare costs: Rationale and design of a randomized, controlled study. BMC Health Serv. Res. 2018, 18, 413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillion, L.; Cook, S.; Veillette, A.M.; Aubin, M.; de Serres, M.; Rainville, F.; Fitch, M.; Doll, R. Professional navigation framework: Elaboration and validation in a Canadian context. Oncol. Nurs. Forum. 2012, 39, E58–E69. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, B.; Bruce, S.D. Patient navigation: A “win-win” for all involved. Oncol. Nurs. Forum. 2010, 37, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Frick, J.; Schindel, D.; Gebert, P.; Grittner, U.; Schenk, L. Improving quality of life in cancer patients through higher participation and health literacy: Study protocol for evaluating the oncological social care project (OSCAR). BMC Health Serv. Res. 2019, 19, 754. [Google Scholar] [CrossRef] [PubMed]
- Bundesverband Managed Care: BMC Lotsenprojekte in Deutschland. Available online: https://www.bmcev.de/wp-content/uploads/BMC-Lotsenlandkarte.pdf (accessed on 28 February 2022).
- Kassenärztliche Bundesvereinigung. Versichertenbefragung der Kassenärztlichen Bundesvereinigung. 2019. Available online: https://www.kbv.de/media/sp/Berichtband_Ergebnisse_der_Versichertenbefragung_2019.pdf (accessed on 20 February 2022).
- IBM Corp. IBM SPSS Statistics for Windows. Version 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Mackey, L.M.; Doody, C.; Werner, E.L.; Fullen, B. Self-Management Skills in Chronic Disease Management: What Role Does Health Literacy Have? Med. Decis. Mak. 2016, 36, 741–759. [Google Scholar] [CrossRef] [PubMed]
- Nordanstig, A.; Asplund, K.; Norrving, B.; Wahlgren, N.; Wester, P.; Rosengren, L. Impact of the Swedish National Stroke Campaign on stroke awareness. Acta Neurol. Scand. 2017, 136, 345–351. [Google Scholar] [CrossRef]
- Reilly, K.H.; Neaigus, A.; Shepard, C.W.; Cutler, B.H.; Sweeney, M.M.; Rucinski, K.B.; Jenness, S.M.; Wendel, T.; Marshall, D.M.; Hagan, H. It’s Never Just HIV: Exposure to an HIV Prevention Media Campaign and Behavior Change among Men Who Have Sex with Men Participating in the National HIV Behavioral Surveillance System in New York City. LGBT Health 2016, 3, 314–318. [Google Scholar] [CrossRef]
- Schaeffer, D.; Klinger, J.; Berens, E.M.; Gille, S.; Griese, L.; Vogt, D.; Hurrelmann, K. Health Literacy in Germany before and during the COVID-19 Pandemic. Gesundheitswesen 2021, 83, 781–788. [Google Scholar] [PubMed]
- Luke, A.; Luck, K.E.; Doucet, S. Experiences of Caregivers as Clients of a Patient Navigation Program for Children and Youth with Complex Care Needs: A Qualitative Descriptive Study. Int. J. Integr. Care 2020, 20, 10. [Google Scholar] [CrossRef]
- Spencer, J.C.; Samuel, C.A.; Rosenstein, D.L.; Reeder-Hayes, K.E.; Manning, M.L.; Sellers, J.B.; Wheeler, S.B. Oncology navigators’ perceptions of cancer-related financial burden and financial assistance resources. Support. Care Cancer 2018, 26, 1315–1321. [Google Scholar] [CrossRef]
- Lang-Rollin, I.; Berberich, G. Psycho-oncology. Dialogues Clin. Neurosci. 2018, 20, 13–22. [Google Scholar] [PubMed]
- Schnitzer, S.; Kuhlmey, A.; Balke, K.; Litschel, A.; Walter, A.; Schenk, L. Kenntnisstand und Bewertung gesundheitspolitischer Reformen im Spiegel sozialer Determinanten. Gesundheitswesen 2011, 73, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Heijmans, M.; Waverijn, G.; Rademakers, J.; van der Vaart, R.; Rijken, M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ. Couns. 2015, 98, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Schnitzer, S.; Kuhlmey, A.; Engelmann, F.; Budnick, A. Informal caregivers and how primary care physicians can support them. Dtsch. Arztebl. Int. 2021, 118, 507–508. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, D.; Vogt, D.; Berens, E.-M.; Hurrelmann, K. Gesundheitskompetenz der Bevölkerung in Deutschland: Ergebnisbericht. Univ. Bielef. Fak. Für Gesundh. 2016, 28, 2021. Available online: https://pub.uni-bielefeld.de/download/2908111/2908198/Ergebnisbericht_HLS-GER.pdf (accessed on 20 February 2022).
- Dalgard, O.S.; Dowrick, C.; Lehtinen, V.; Vazquez-Barquero, J.L.; Casey, P.; Wilkinson, G.; Ayuso-Mateos, J.L.; Page, H.; Dunn, G.; Group, O. Negative life events, social support and gender difference in depression: A multinational community survey with data from the ODIN study. Soc. Psych. Psych. Epid. 2006, 41, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Addis, M.E.; Mahalik, J.R. Men, masculinity, and the contexts of help seeking. Am. Psychol. 2003, 58, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Mackenzie, C.S.; Gekoski, W.L.; Knox, V.J. Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging Ment. Health 2006, 10, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men’s help-seeking for depression: A systematic review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Given, B.A.; Given, C.W.; Kozachik, S. Family support in advanced cancer. CA Cancer J. Clin. 2001, 51, 213–231. [Google Scholar] [CrossRef] [PubMed]
- Schindel, D.; Schneider, A.; Grittner, U.; Jobges, M.; Schenk, L. Quality of life after stroke rehabilitation discharge: A 12-month longitudinal study. Disabil. Rehabil. 2021, 43, 2332–2341. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Blüher, S.; Grittner, U.; Anton, V.; Schaeffner, E.; Ebert, N.; Jakob, O.; Martus, P.; Kuhlmey, A.; Wenning, V.; et al. Is there an association between social determinants and care dependency risk? A multi-state model analysis of a longitudinal study. Res. Nurs. Health 2020, 43, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Sparla, A.; Flach-Vorgang, S.; Villalobos, M.; Krug, K.; Kamradt, M.; Coulibaly, K.; Szecsenyi, J.; Thomas, M.; Gusset-Bahrer, S.; Ose, D. Individual difficulties and resources—A qualitative analysis in patients with advanced lung cancer and their relatives. Patient Prefer. Adher. 2016, 10, 2021–2029. [Google Scholar] [CrossRef] [Green Version]
- Hajek, A.; König, H.-H. Longitudinal predictors of functional impairment in older adults in Europe–evidence from the survey of health, ageing and retirement in Europe. PLoS ONE 2016, 11, e0146967. [Google Scholar] [CrossRef]
- Oedekoven, M.; Amin-Kotb, K.; Gellert, P.; Balke, K.; Kuhlmey, A.; Schnitzer, S. Associations between informal caregivers’ burden and educational level. GeroPsych 2019, 32, 19. [Google Scholar] [CrossRef]
- Jedro, C.; Holmberg, C.; Tille, F.; Widmann, J.; Schneider, A.; Stumm, J.; Dopfmer, S.; Kuhlmey, A.; Schnitzer, S. The Acceptability of Task-Shifting from Doctors to Allied Health Professionals. Dtsch Arztebl. Int. 2020, 117, 583–590. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n = 6110 * | % [95% CI] | ||
|---|---|---|---|
| Age | 18–64 | 4294 | 70.3 [69.1; 71.4] |
| 65+ | 1815 | 29.7 [28.6; 30.9] | |
| Sex | female | 3196 | 52.3 [51.1; 53.6] |
| male | 2914 | 47.7 [46.4; 48.9] | |
| Education | low | 4122 | 68.3 [67.1; 69.4] |
| high | 1916 | 31.7 [30.6; 32.9] | |
| Partnership | yes | 4341 | 71.4 [70.2; 72.5] |
| no | 1741 | 28.6 [27.5; 29.8] | |
| Region | East Germany | 1063 | 17.4 [16.5; 18.4] |
| West Germany | 5047 | 82.6 [81.6; 83.5] | |
| Urban/Rural | rural | 1781 | 31.2 [30.0; 32.4] |
| town | 2603 | 45.6 [44.3; 46.9] | |
| big city | 1326 | 23.2 [22.1; 24.3] | |
| Chronic Illness | yes | 2885 | 47.6 [46.3; 48.8] |
| no | 3177 | 52.4 [51.2; 53.7] | |
| Subjective health | excellent/very good/good | 4716 | 77.9 [76.8; 78.9] |
| less well/bad | 1342 | 22.1 [21.1; 23.2] |
| No Experience with Patient Navigation | Experience with Patient Navigation | |||||
|---|---|---|---|---|---|---|
| M1a. Application | M2a. Information | M3a. Emotional | M1b. Application | M2b. Information | M3b. Emotional | |
| OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | |
| Age | ||||||
| 18–64 | 1.33 [1.02, 1.74] | 1.15 [0.78, 1.69] | 1.33 [0.97, 1.81] | 4.68 [1.86, 11.80] | 0.56 [0.22, 1.40] | 0.64 [0.19, 2.17] |
| 65+ | 1 | 1 | 1 | 1 | 1 | 1 |
| Sex | ||||||
| female | 1 | 1 | 1 | 1 | 1 | 1 |
| male | 1.55 [1.20, 2.00] | 0.98 [0.69, 1.40] | 0.66 [0.49, 0.89] | 0.48 [0.21, 1.07] | 1.55 [0.68, 3.51] | 1.27 [0.47, 3.45] |
| Education | ||||||
| low | 1 | 1 | 1 | 1 | 1 | 1 |
| high | 1.01 [0.76, 1.35] | 1.55 [1.06, 2.27] | 0.92 [0.66, 1.27] | 0.56 [0.22, 1.45] | 0.73 [0.27, 1.99] | 3.31 [1.05, 10.41] |
| Partnership | ||||||
| yes | 1.75 [1.32, 2.32] | 0.82 [0.56, 1.21] | 0.53 [0.39, 0.71] | 0.53 [0.23, 1.24] | 1.66 [0.68, 4.07] | 0.98 [0.33, 2.97] |
| no | 1 | 1 | 1 | 1 | 1 | 1 |
| Region | ||||||
| West Germany | 1.40 [1.02, 1.92] | 0.70 [0.46, 1.06] | 0.75 [0.53, 1.07] | 0.38 [0.14, 1.01] | 3.59 [1.06, 12.18] | 0.90 [0.27, 2.97] |
| East Germany | 1 | 1 | 1 | 1 | 1 | 1 |
| Urban/rural | ||||||
| rural ≤ 5000 | 1.33 [0.94, 1.88] | 0.85 [0.52, 1.41] | 0.84 [0.56, 1.26] | 0.29 [0.10, 0.89] | 1.03 [0.32, 3.24] | 3.15 [0.67, 14.67] |
| town 5001–100,000 | 0.81 [0.59, 1.12] | 1.14 [0.74, 1.76] | 1.27 [0.89, 1.83] | 0.36 [0.13, 0.98] | 1.65 [0.59, 4.65] | 1.82 [0.46, 7.25] |
| big city | 1 | 1 | 1 | 1 | 1 | 1 |
| Chronic illness | ||||||
| yes | 1.68 [1.29, 2.20] | 0.91 [0.63, 1.32] | 0.66 [0.49, 0.89] | 4.99 [2.01, 12.42] | 0.54 [0.21, 1.41] | 0.37 [0.12, 1.17] |
| no | 1 | 1 | 1 | 1 | 1 | 1 |
| Subjective health | ||||||
| less well/bad | 1.00 [0.74, 1.37] | 0.54 [0.32, 0.89] | 1.30 [0.92, 1.84] | 0.60 [0.26, 1.39] | 1.46 [0.60, 3.53] | 0.89 [0.28, 2.90] |
| excellent/very good/good | 1 | 1 | 1 | 1 | 1 | 1 |
| R² (Nagelkerke) | 0.073 | 0.037 | 0.061 | 0.047 | 0.122 | 0.148 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnitzer, S.; Kohl, R.; Fügemann, H.; Gödde, K.; Stumm, J.; Engelmann, F.; Grittner, U.; Rieckmann, N. Patient Navigation—Who Needs What? Awareness of Patient Navigators and Ranking of Their Tasks in the General Population in Germany. Int. J. Environ. Res. Public Health 2022, 19, 2846. https://doi.org/10.3390/ijerph19052846
Schnitzer S, Kohl R, Fügemann H, Gödde K, Stumm J, Engelmann F, Grittner U, Rieckmann N. Patient Navigation—Who Needs What? Awareness of Patient Navigators and Ranking of Their Tasks in the General Population in Germany. International Journal of Environmental Research and Public Health. 2022; 19(5):2846. https://doi.org/10.3390/ijerph19052846
Chicago/Turabian StyleSchnitzer, Susanne, Raphael Kohl, Hella Fügemann, Kathrin Gödde, Judith Stumm, Fabian Engelmann, Ulrike Grittner, and Nina Rieckmann. 2022. "Patient Navigation—Who Needs What? Awareness of Patient Navigators and Ranking of Their Tasks in the General Population in Germany" International Journal of Environmental Research and Public Health 19, no. 5: 2846. https://doi.org/10.3390/ijerph19052846