
The COVID-19 Pandemic Impacted Maternal Mental Health Differently Depending on Pregnancy Status and Trimester of Gestation

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
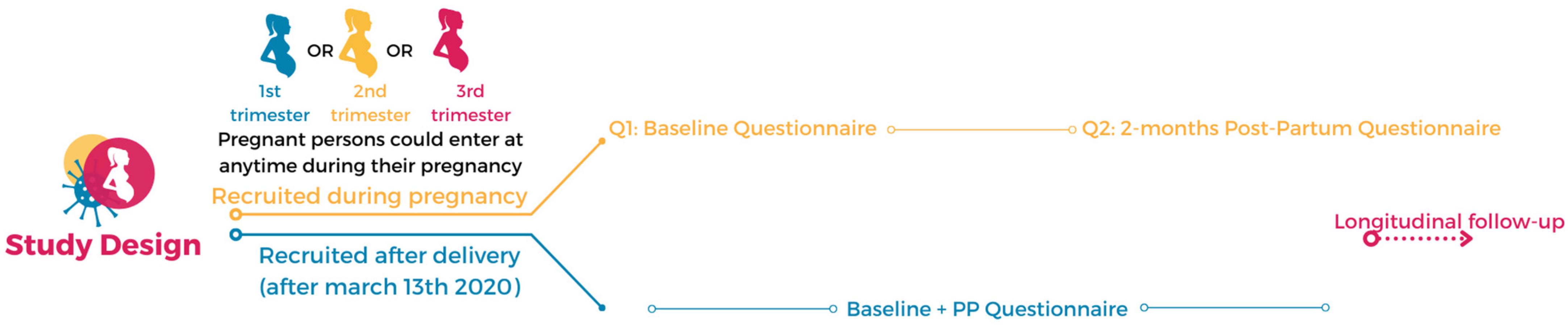
2.1. Study Design
2.2. Data Collection
2.3. Data Analyses
3. Results
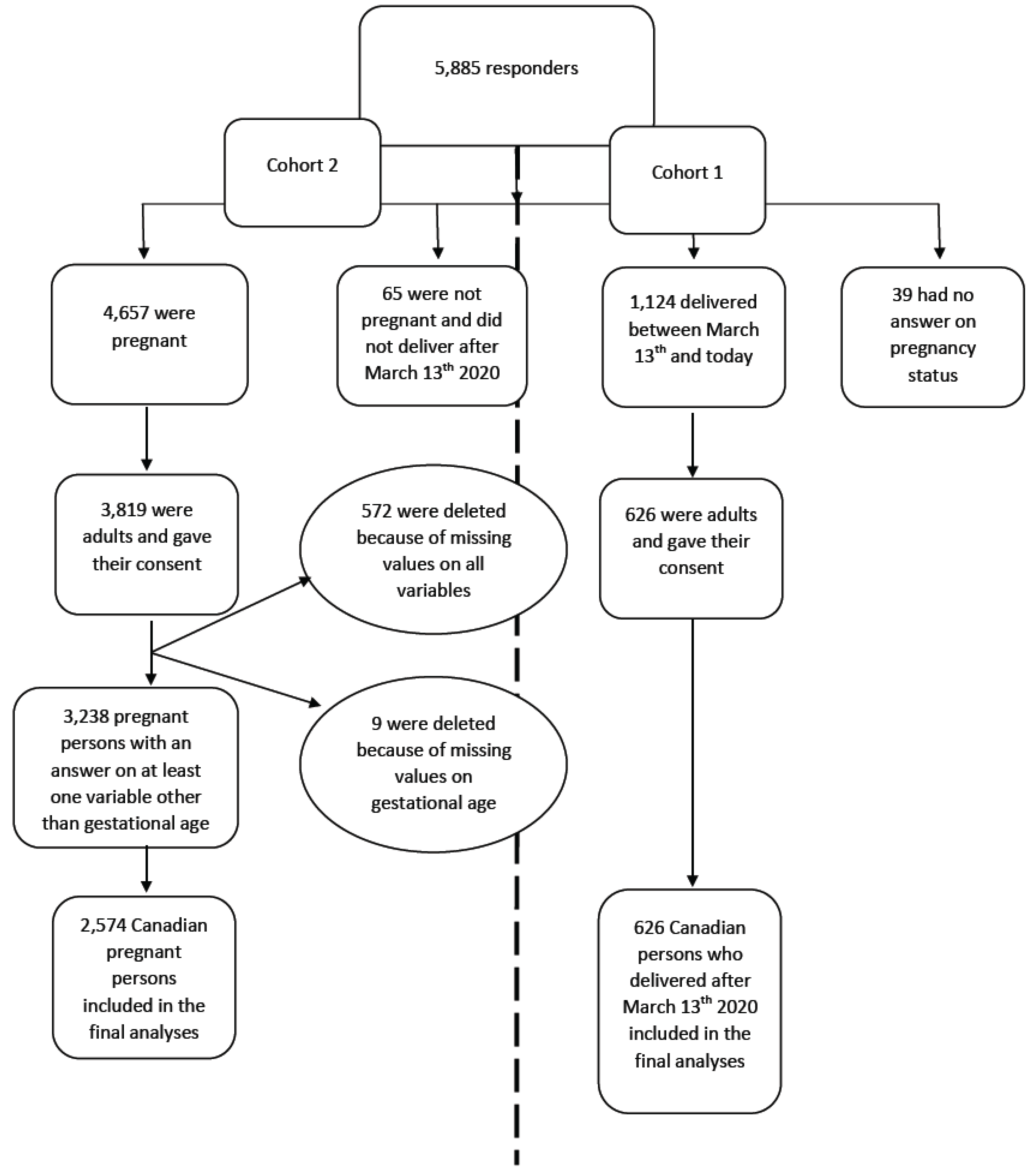
3.1. Description of the Participants
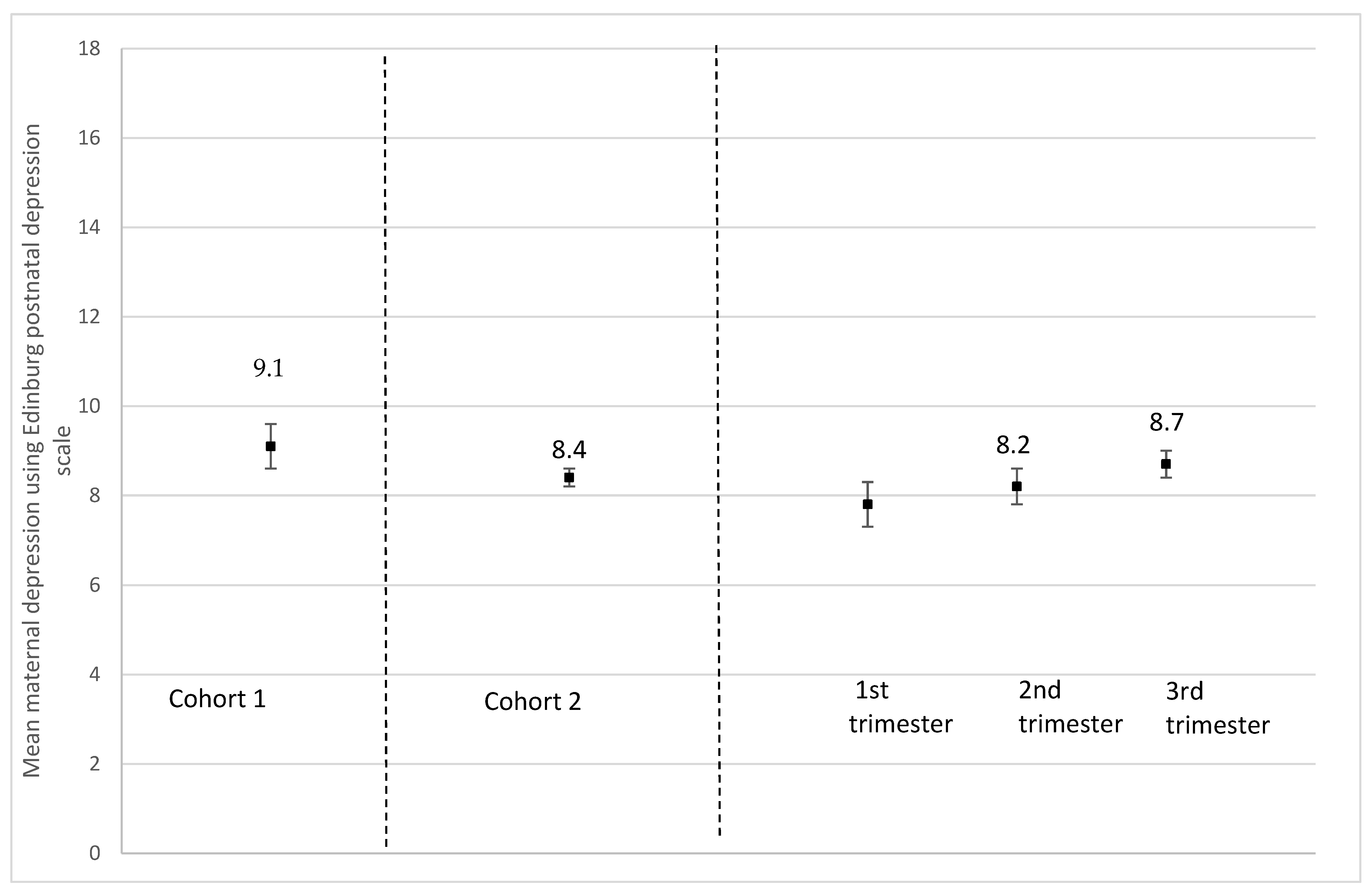
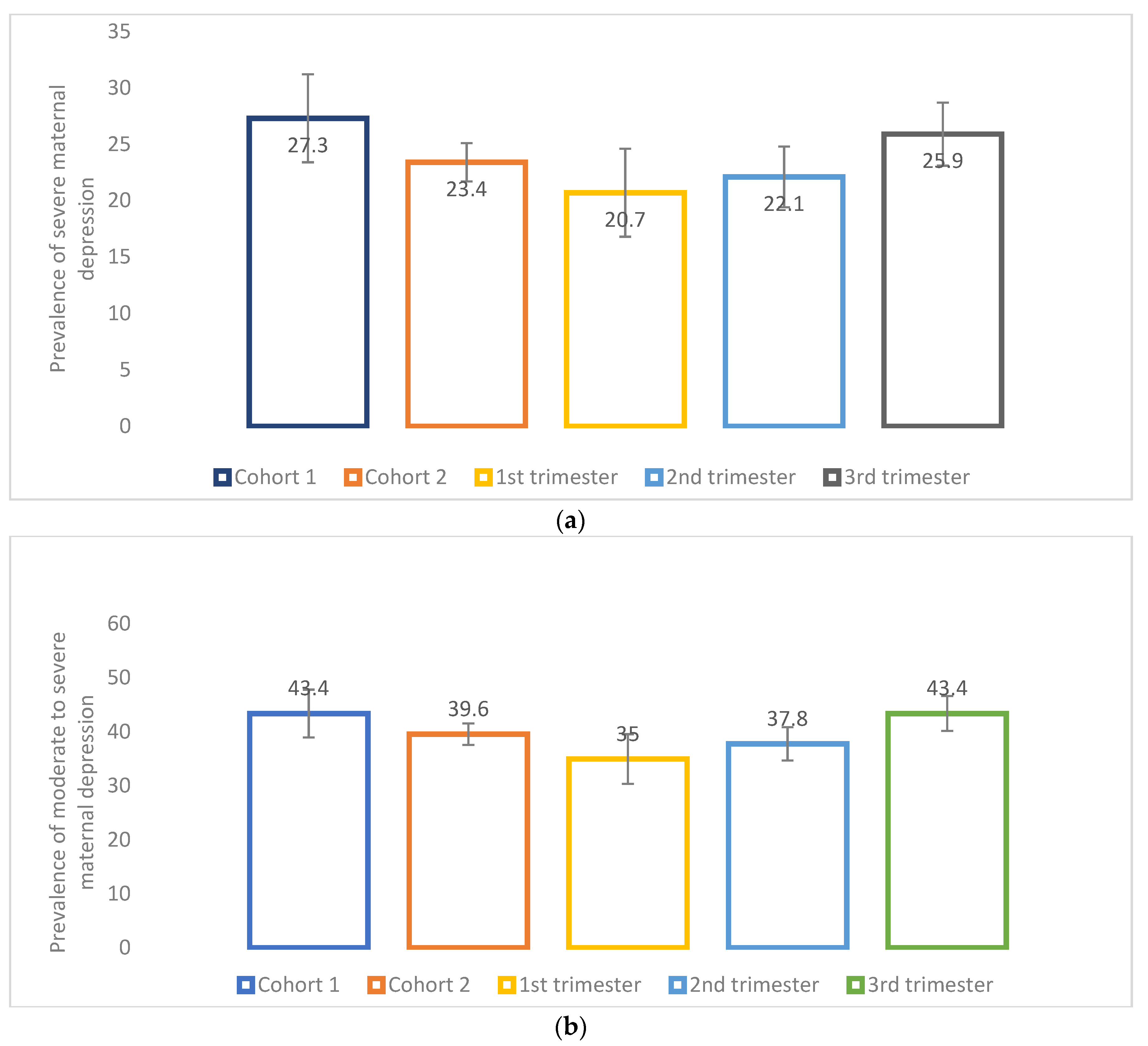
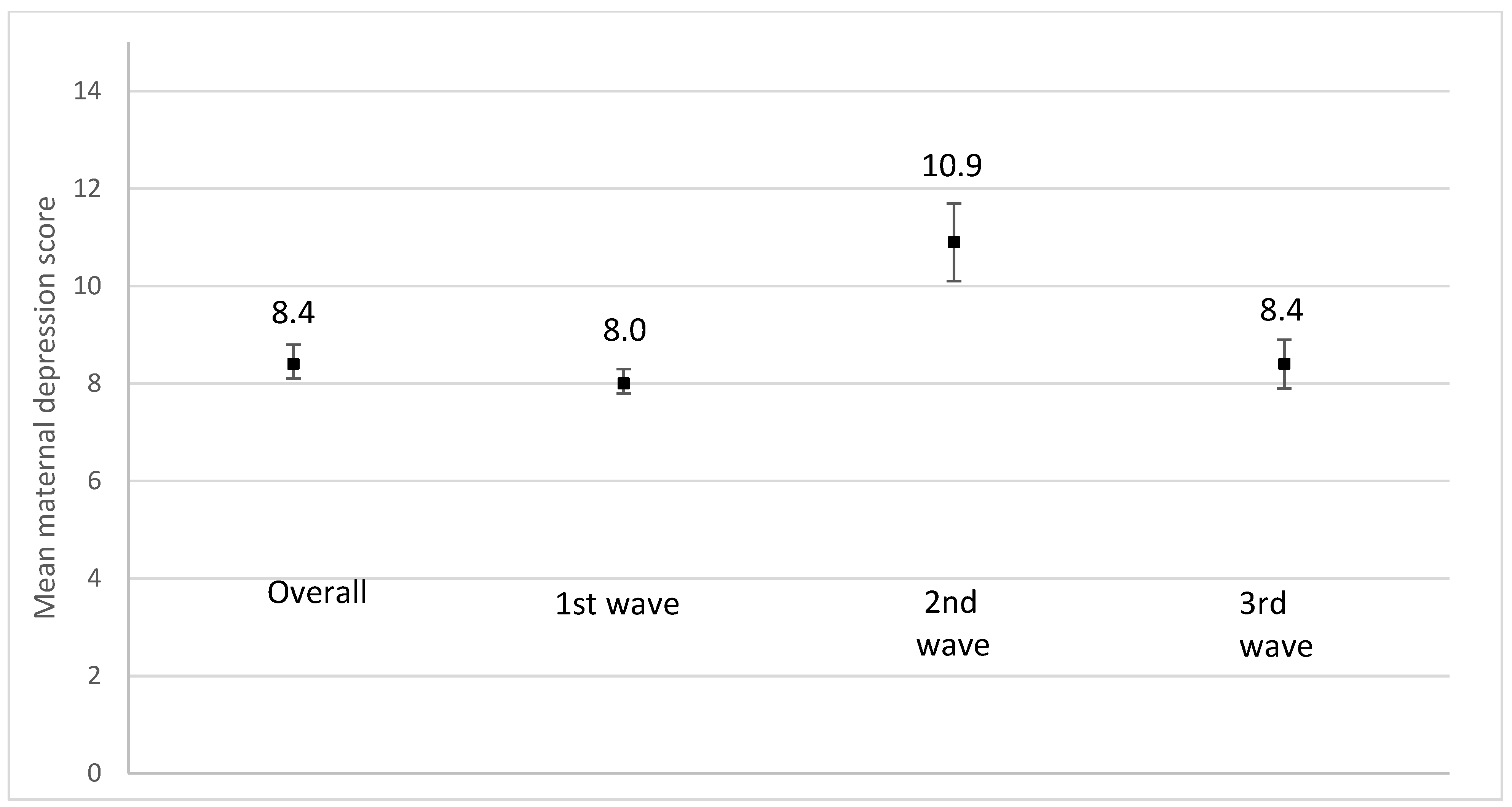
3.2. Maternal Depression
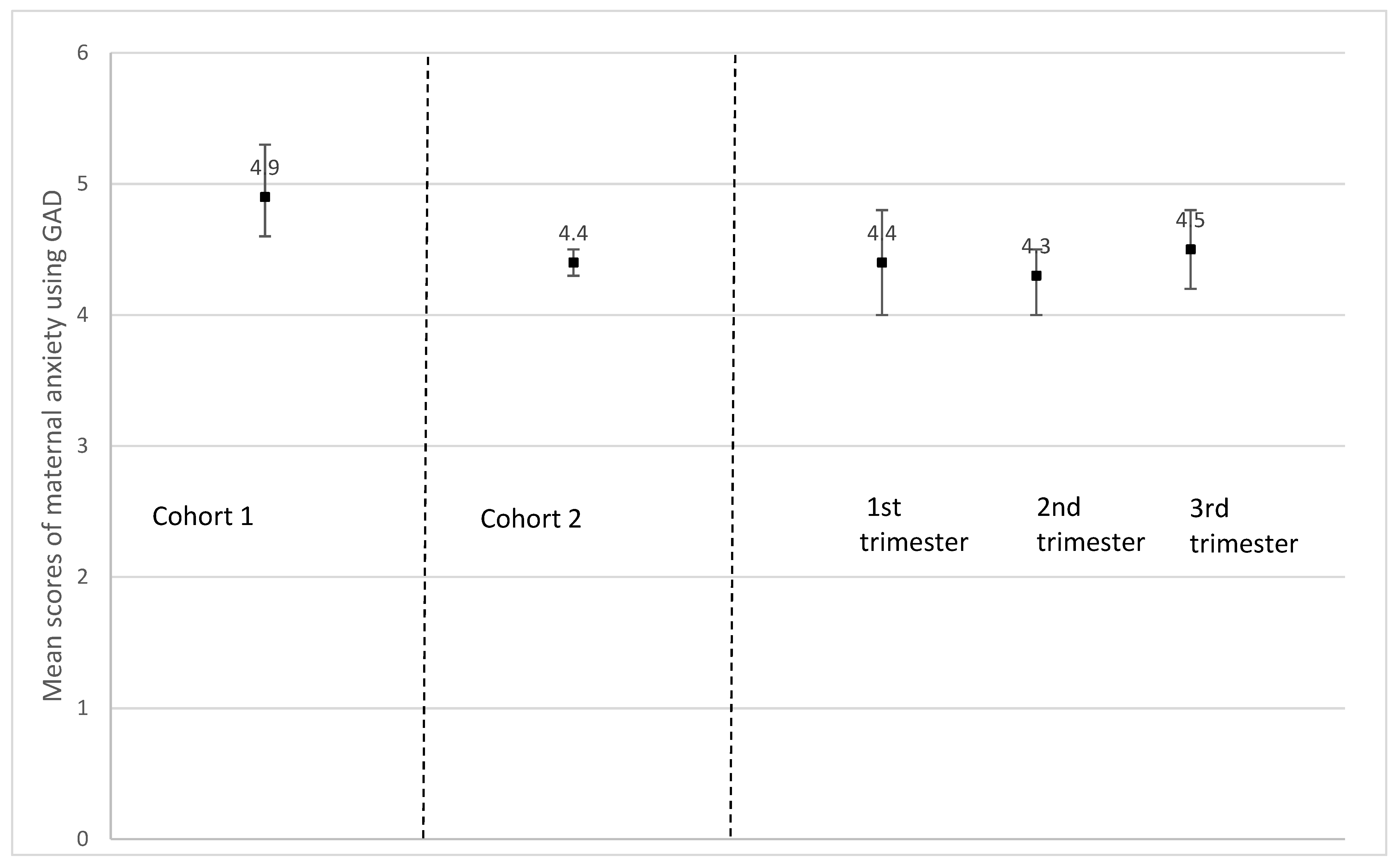
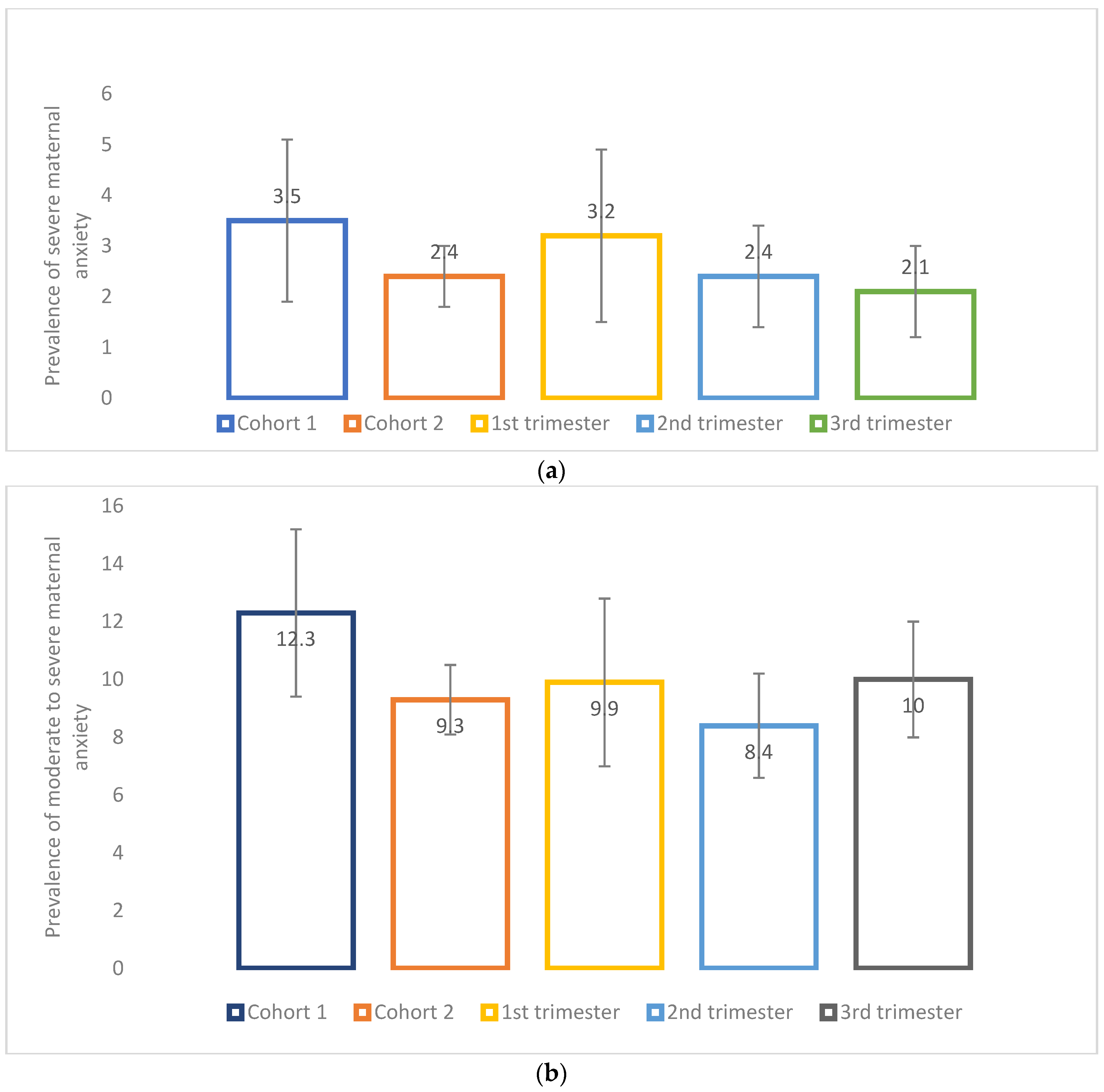
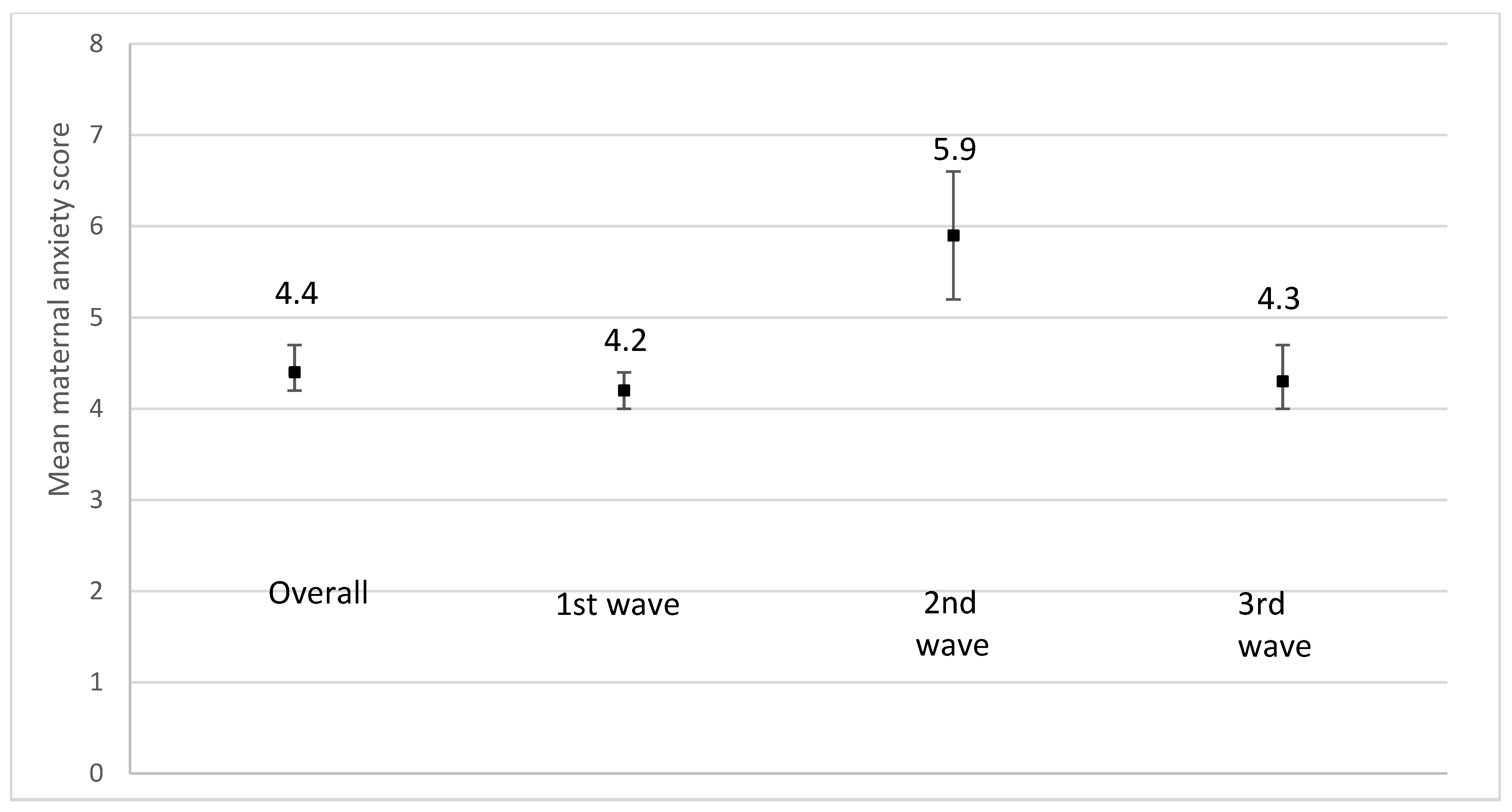
3.3. Maternal Anxiety and Overall Stress
3.4. Predictors of Severe Maternal Depression during Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grote, N.K.; Bridge, J.A.; Gavin, A.R.; Melville, J.L.; Iyengar, S.; Katon, W.J. A Meta-analysis of Depression During Pregnancy and the Risk of Preterm Birth, Low Birth Weight, and Intrauterine Growth Restriction. Arch. Gen. Psychiatry 2010, 67, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- DiGiovanni, C.; Conley, J.; Chiu, D.; Zaborski, J. Factors Influencing Compliance with Quarantine in Toronto during the 2003 SARS Outbreak. Biosecur. Bioterror. Biodef. Strat. Pract. Sci. 2004, 2, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Mappa, I.; Distefano, F.A.; Rizzo, G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: A prospectic observational study. J. Peérinat. Med. 2020, 48, 545–550. [Google Scholar] [CrossRef]
- Karam, F.; Sheehy, O.; Huneau, M.-C.; Chambers, C.; Fraser, W.D.; Johnson, D.; Kao, K.; Martin, B.; Riordan, S.H.; Roth, M.; et al. Impact of maternal prenatal and parental postnatal stress on 1-year-old child development: Results from the OTIS antidepressants in pregnancy study. Arch. Women’s Ment. Health 2016, 19, 835–843. [Google Scholar] [CrossRef]
- Laplante, D.P.; Brunet, A.; Schmitz, N.; Ciampi, A.; King, S. Project Ice Storm: Prenatal maternal stress affects cognitive and linguistic functioning in 5 1/2-year-old children. J. Am. Acad. Child. Adolesc. Psychiatry 2008, 47, 1063–1072. [Google Scholar] [CrossRef] [Green Version]
- Dancause, K.N.; Laplante, D.P.; Fraser, S.; Brunet, A.; Ciampi, A.; Schmitz, N.; King, S. Prenatal exposure to a natural disaster increases risk for obesity in 5(1/2)-year-old children. Pediatr. Res. 2012, 71, 126–131. [Google Scholar] [CrossRef]
- Liu, G.T.; Dancause, K.N.; Elgbeili, G.; Laplante, D.P.; King, S. Disaster-related prenatal maternal stress explains increasing amounts of variance in body composition through childhood and adolescence: Project Ice Storm. Environ. Res. 2016, 150, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Veru, F.; Dancause, K.; Laplante, D.P.; King, S.; Luheshi, G. Prenatal maternal stress predicts reductions in CD4+ lymphocytes, increases in innate-derived cytokines, and a Th2 shift in adolescents: Project Ice Storm. Physiol. Behav. 2015, 144, 137–145. [Google Scholar] [CrossRef]
- Laplante, D.P.; Barr, R.G.; Brunet, A.; Du Fort, G.G.; Meaney, M.L.; Saucier, J.-F.; Zelazo, P.R.; King, S. Stress During Pregnancy Affects General Intellectual and Language Functioning in Human Toddlers. Pediatr. Res. 2004, 56, 400–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laplante, D.P.; Zelazo, P.R.; Brunei, A.; King, S. Functional Play at 2 Years of Age: Effects of Prenatal Maternal Stress. Infancy 2007, 12, 69–93. [Google Scholar] [CrossRef]
- Li, X.; Gao, R.; Dai, X.; Liu, H.; Zhang, J.; Liu, X.; Si, D.; Deng, T.; Xia, W. The association between symptoms of depression during pregnancy and low birth weight: A prospective study. BMC Pregnancy Childbirth 2020, 20, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakic Rados, S.; Tadinac, M.; Herman, R. Anxiety During Pregnancy and Postpartum: Course, Predictors and Comorbidity with Postpartum Depression. Acta Clin. Croat. 2018, 57, 39–51. [Google Scholar] [CrossRef]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X.; et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 223, 240.e1–240.e9. [Google Scholar] [CrossRef]
- Statistics Canada. Survey on COVID-19 and Mental Health, September to December 2020. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/210318/dq210318a-eng.htm (accessed on 22 November 2021).
- Ceulemans, M.; Foulon, V.; Ngo, E.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’Shaughnessy, F.; Passier, A.; et al. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic—A multinational cross-sectional study. Acta Obstet. Gynecol. Scand. 2021, 100, 1219–1229. [Google Scholar] [CrossRef]
- Kajdy, A.; Feduniw, S.; Ajdacka, U.; Modzelewski, J.; Baranowska, B.; Sys, D.; Pokropek, A.; Pawlicka, P.; Kaźmierczak, M.; Rabijewski, M.; et al. Risk factors for anxiety and depression among pregnant women during the COVID-19 pandemic: A web-based cross-sectional survey. Medicine 2020, 99, e21279. [Google Scholar] [CrossRef]
- Ali, S.H.; Foreman, J.; Capasso, A.; Jones, A.M.; Tozan, Y.; DiClemente, R.J. Social media as a recruitment platform for a nationwide online survey of COVID-19 knowledge, beliefs, and practices in the United States: Methodology and feasibility analysis. BMC Med. Res. Methodol. 2020, 20, 116. [Google Scholar] [CrossRef]
- Shrestha, S.D.; Pradhan, R.; Tran, T.; Gualano, R.C.; Fisher, J. Reliability and validity of the Edinburgh Postnatal Depression Scale (EPDS) for detecting perinatal common mental disorders (PCMDs) among women in low-and lower-middle-income countries: A systematic review. BMC Pregnancy Childbirth 2016, 16, 72. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, M.A.; Zamorano, E.; Garcia-Campayo, J.; Pardo, A.; Freire, O.; Rejas, J. Validity of the GAD-7 scale as an outcome measure of disability in patients with generalized anxiety disorders in primary care. J. Affect. Disord. 2011, 128, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Society of Obstetricians and Gynaecologists of Canada. SOGC Statement on the COVID-19 Vaccines and Rare Adverse Outcomes of Thrombosis Associated with Low Platelets. 2021. Available online: https://www.sogc.org/en/content/featured-news/SOGC_Statement_on_the_COVID-19_vaccines_and_rare_adverse_outcomes_of_%20thrombosis.aspx (accessed on 22 November 2021).
- García, F.E.; Barraza-Peña, C.G.; Wlodarczyk, A.; Alvear-Carrasco, M.; Reyes-Reyes, A. Psychometric properties of the Brief-COPE for the evaluation of coping strategies in the Chilean population. Psicol Reflex Crit. 2018, 31, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Eberhard-Gran, M.; Tambs, K.; Opjordsmoen, S.; Skrondal, A.; Eskild, A. Depression during pregnancy and after delivery: A repeated measurement study. J. Psychosom. Obstet. Gynecol. 2004, 25, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Bérard, A.; Sheehy, O.; Zhao, J.-P.; Chambers, C.; Roth, M.; Bozzo, P.; Johnson, D.; Kao, K.; Lavigne, S.; Wolfe, L.; et al. Impact of antidepressant use, discontinuation, and dosage modification on maternal depression during pregnancy. Eur. Neuropsychopharmacol. 2019, 29, 803–812. [Google Scholar] [CrossRef]
- Krubiner, C.B.; Faden, R.R.; Karron, R.A.; Little, M.O.; Lyerly, A.D.; Abramson, J.S.; Beigi, R.H.; Cravioto, A.R.; Durbin, A.P.; Gellin, B.G.; et al. Pregnant women & vaccines against emerging epidemic threats: Ethics guidance for preparedness, research, and response. Vaccine 2019, 39, 85–120. [Google Scholar] [CrossRef] [PubMed]
- Onoye, J.M.; Shafer, L.A.; Goebert, D.A.; Morland, L.A.; Matsu, C.R.; Hamagami, F. Changes in PTSD symptomatology and mental health during pregnancy and postpartum. Arch. Women’s Ment. Health 2013, 16, 453–463. [Google Scholar] [CrossRef]
- Yim, I.S.; Glynn, L.M.; Schetter, C.D.; Hobel, C.J.; Chicz-DeMet, A.; Sandman, C.A. Risk of Postpartum Depressive Symptoms With Elevated Corticotropin-Releasing Hormone in Human Pregnancy. Arch. Gen. Psychiatry 2009, 66, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Poliquin, V.; Castillo, E.; Boucoiran, I.; Wong, J.; Watson, H.; Yudin, M.; Money, D.; Van Schalkwyk, J.; Elwood, C.; on behalf of the Infectious Disease Committee of the Society of Obstetricians and Gynaecologists of Canada. SOGC Statement on COVID-19 Vaccination in Pregnancy. 2021. Available online: https://sogc.org/common/Uploaded%20files/Latest%20News/SOGC_Statement_COVID-19_Vaccination_in_Pregnancy.pdf (accessed on 22 November 2021).
- MSSS. COVID-19 ARNm: Vaccins à ARN Messager Contre la COVID-19. 2021. Available online: https://www.msss.gouv.qc.ca/professionnels/vaccination/piq-vaccins/covid-19-vaccin-a-arn-messager-contre-la-covid-19/ (accessed on 22 November 2021).
- Kalin, N.H. The Critical Relationship Between Anxiety and Depression. Am. J. Psychiatry 2020, 177, 365–367. [Google Scholar] [CrossRef]
- Hammen, C.; Kim, E.Y.; Eberhart, N.K.; Brennan, P.A. Chronic and acute stress and the prediction of major depression in women. Depress. Anxiety 2009, 26, 718–723. [Google Scholar] [CrossRef] [Green Version]
- Weaver, A.; Himle, J.A.; Taylor, R.J.; Matusko, N.N.; Abelson, J.M. Urban vs Rural Residence and the Prevalence of Depression and Mood Disorder Among African American Women and Non-Hispanic White Women. JAMA Psychiatry 2015, 72, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women Who Delivered (Cohort 1) n = 626 | Women Currently Pregnant (Cohort 2) n = 2574 | p-Value + | First Trimester n = 504 | Second Trimester n = 1032 | Third Trimester n = 1038 | p-Value / | |
|---|---|---|---|---|---|---|---|
| Age at recruitment (mean, SD), years | 33.2 (4.5) | 32.2 (4.3) | <0.0001 | 32.2 (4.3) | 32.3 (4.4) | 32.1 (4.2) | 0.7320 |
| Missing | 4 | 8 | 1 | 2 | 5 | ||
| Gestational age at recruitment (SD), weeks | 38.9 (1.9) | 24.5 (9.7) | <0.0001 | 9.8 (3.0) | 22.1 (4.0) | 34.1 (3.3) | <0.0001 |
| Missing | |||||||
| Prenatal care follow-up * | |||||||
| Family physician | 201 (32.8) | 906 (35.5) | 0.2179 | 196 (39.4) | 385 (37.6) | 325 (31.6) | 0.0023 |
| Obstetrician/Gynaecologist | 426 (69.6) | 1570 (61.5) | 0.0002 | 275 (55.2) | 614 (59.9) | 681 (66.1) | <0.0001 |
| Midwife | 47 (7.7) | 308 (12.1) | 0.0020 | 65 (13.1) | 118 (11.5) | 125 (12.1) | 0.6847 |
| Missing | 14 | 21 | 6 | 7 | 8 | ||
| Pre-pregnancy body mass index, kg/m2 | 0.9147 | ||||||
| Mean (SD) | 25.1 (5.) | 25.0 (5.8) | 0.6556 | 24.9 (5.7) | 25.0 (5.8) | 25.1 (5.7) | |
| Missing | 7 | 26 | 2 | 12 | 12 | ||
| Pregnancy body mass index, kg/m2 | <0.0001 | ||||||
| Mean (SD) | 30.1 (5.5) | 27.6 (5.9) | <0.0001 | 25.5 (5.8) | 27.0 (5.7) | 29.2 (5.8) | |
| Missing | 14 | 58 | 13 | 22 | 23 | ||
| Education, years | 0.7740 | ||||||
| Mean (SD) | 17.4 (3.2) | 16.9 (4.5) | 0.0042 | 16.9 (4.7) | 17.0 (4.4) | 16.9 (4.5) | |
| Missing | 39 | 98 | 21 | 32 | 45 | ||
| Ethnicity-Caucasian/White | 540 (90.9) | 2242 (90.8) | 0.9377 | 434 (90.8) | 901 (90.5) | 907 (91.2) | 0.8662 |
| Missing | 32 | 105 | 26 | 36 | 43 | ||
| Marital status–Living alone | 20 (3.4) | 52 (2.1) | 0.0661 | 10 (2.1) | 19 (1.9) | 23 (2.3) | 0.8139 |
| Missing | 30 | 86 | 21 | 27 | 38 | ||
| Annual household income, CAN$ | 0.2549 | 0.3405 | |||||
| <30,000 | 27 (4.8) | 69 (2.9) | 4 (0.8) | 36 (3.8) | 29 (3.1) | ||
| 30,001–60,000 | 49 (8.7) | 239 (10.1) | 54 (11.5) | 91 (9.5) | 94 (9.9) | ||
| 60,001–90,000 | 83 (14.7) | 374 (15.8) | 78 (16.6) | 150 (15.7) | 146 (15.4) | ||
| 90,001–120,000 | 143 (25.4) | 606 (25.5) | 126 (26.7) | 250 (26.2) | 230 (24.3) | ||
| 120,001–150,000 | 101 (17.9) | 429 (18.1) | 81 (17.2) | 175 (18.3) | 173 (18.3) | ||
| 150,001–180,000 | 65 (11.5) | 299 (12.6) | 56 (11.9) | 117 (12.3) | 126 (13.3) | ||
| >180,000 | 96 (17.0) | 356 (15.0) | 72 (15.3) | 136 (14.2) | 148 (15.7) | ||
| Missing | 62 | 202 | 33 | 77 | 92 | ||
| Area of residence | 0.2757 | 0.9796 | |||||
| Urban | 268 (45.0) | 1065 (42.9) | 208 (43.1) | 432 (43.2) | 425 (42.6) | ||
| Suburban | 260 (43.6) | 1073 (43.3) | 212 (43.9) | 431 (43.1) | 430 (43.1) | ||
| Rural | 68 (11.4) | 343 (13.8) | 63 (13.0) | 138 (13.7) | 142 (14.3) | ||
| Missing | 30 | 93 | 21 | 31 | 41 | ||
| Recruitment period - | <0.0001 | ||||||
| 1st COVID wave | - | - | - | 341 (67.7) | 714 (69.2) | 771 (74.3) | |
| 2nd COVID wave | - | - | - | 67 (13.3) | 95 (9.2) | 54 (5.2) | |
| 3rd COVID wave | - | - | - | 96 (19.0) | 223 (21.6) | 213 (20.5) |
| Variable | No Depression n = 1693 (%) | Severe Depression + n = 511 (%) | Unadjusted OR (95%CI) | Adjusted OR * (95%CI) |
|---|---|---|---|---|
| Recruitment trimester of pregnancy | ||||
| 1st trimester | 316 (18.7) | 80 (15.7) | Reference | Reference |
| 2nd trimester | 713 (42.1) | 201 (39.3) | 1.11 (0.83; 1.49) | 1.29 (0.85; 1.95) |
| 3rd trimester | 664 (39.2) | 230 (45.0) | 1.37 (1.03; 1.82) | 1.48 (0.97; 2.27) |
| Maternal anxiety /, mean (SD) | 3.1 (2.7) | 8.7 (4.3) | 1.63 (1.55; 1.71) | 1.51 (1.44; 1.59) |
| Maternal stress -, mean (SD) | 4.1 (1.9) | 6.2 (1.7) | 1.86 (1.74; 2.00) | 1.35 (1.24; 1.48) |
| Maternal age at recruitment, years | 32.3 (4.2) | 32.4 (4.2) | 1.00 (0.98; 1.03) | 1.00 (0.97; 1.04) |
| Education, years | 17.2 (4.3) | 16.4 (5.0) | 0.96 (0.94; 0.98) | 1.00 (0.97; 1.03) |
| Ethnicity/Race | ||||
| Caucasian | 1552 (91.7) | 464 (90.8) | Reference | Reference |
| Others | 141 (8.3) | 47 (9.2) | 1.12 (0.79; 1.58) | 0.86 (0.51; 1.45) |
| Annual household income, CAD | ||||
| <30,000 | 33 (1.9) | 24 (4.7) | Reference | Reference |
| 30,001–60,000 | 147 (8.7) | 71 (13.9) | 0.66 (0.37; 1.21) | 0.57 (0.23; 1.37) |
| 60,001–90,000 | 267 (15.8) | 75 (14.7) | 0.39 (0.22; 0.69) | 0.38 (0.16; 0.92) |
| 90,001–120,000 | 416 (24.6) | 138 (27.0) | 0.46 (0.26; 0.80) | 0.47 (0.20; 1.10) |
| 120,001–150,000 | 311 (18.4) | 89 (17.4) | 0.39 (0.22; 0.70) | 0.43 (0.18; 1.03) |
| 150,001–180,000 | 232 (13.7) | 61 (11.9) | 0.36 (0.20; 0.66) | 0.43 (0.17; 1.07) |
| >180,000 | 287 (16.9) | 53 (10.4) | 0.25 (0.14; 0.46) | 0.26 (0.10; 0.66) |
| Area of residence | ||||
| Urban | 735 (43.4) | 207 (40.5) | Reference | Reference |
| Suburban | 733 (43.3) | 223 (43.6) | 1.08 (0.87; 1.34) | 0.89 (0.65; 1.22) |
| Rural | 225 (13.3) | 81 (15.9) | 1.28 (0.95; 1.72) | 1.64 (1.08; 2.49) |
| Current number of children | ||||
| 0 | 881 (52.0) | 232 (45.4) | Reference | Reference |
| 1 | 583 (34.4) | 209 (40.9) | 0.74 (0.59; 0.91) | 0.76 (0.55; 1.05) |
| ≥2 | 229 (13.6) | 70 (13.7) | 0.85 (0.63; 1.16) | 0.98 (0.63; 1.53) |
| Marital status–Living alone | ||||
| No | 1663 (98.2) | 497 (97.3) | Reference | Reference |
| Yes | 30 (1.8) | 14 (2.7) | 1.56 (0.82; 2.97) | 1.77 (0.67; 4.72) |
| Pre-pregnancy body mass index, mean (SD) | 24.9 (5.7) | 25.8 (6.0) | 1.03 (1.01; 1.04) | 1.01 (0.99; 1.04) |
| Coffee intake | ||||
| No | 588 (34.7) | 162 (31.7) | Reference | Reference |
| Yes | 1105 (65.3) | 349 (68.3) | 1.15 (0.93; 1.42) | 1.24 (0.92; 1.67) |
| Smoking | ||||
| No | 1667 (98.5) | 495 (96.9) | Reference | Reference |
| Yes | 26 (1.5) | 16 (3.1) | 2.07 (1.10; 3.89) | 0.96 (0.31; 2.94) |
| Alcohol | ||||
| No | 1626 (96.0) | 491 (96.1) | Reference | Reference |
| Yes | 67 (4.0) | 20 (3.9) | 0.99 (0.59; 1.65) | 0.62 (0.28; 1.39) |
| Cannabis use | ||||
| No | 1681 (99.3) | 501 (98.0) | Reference | Reference |
| Yes | 12 (0.7) | 10 (2.0) | 2.80 (1.20; 6.51) | 0.75 (0.14; 3.93) |
| Physical activity | ||||
| No change | 509 (30.1) | 119 (23.3) | Reference | Reference |
| Start/Increase | 298 (17.6) | 66 (12.9) | 0.95 (0.68; 1.32) | 0.99 (0.63; 1.57) |
| Stop/Decrease | 886 (52.3) | 326 (63.8) | 1.57 (1.24; 1.99) | 1.21 (0.87; 1.70) |
| Multivitamin use during pregnancy | ||||
| No | 194 (11.5) | 67 (13.1) | Reference | Reference |
| Yes | 1499 (88.5) | 444 (86.9) | 0.86 (0.64; 1.16) | 1.03 (0.67; 1.59) |
| Asthma | ||||
| No | 1522 (89.9) | 445 (87.1) | Reference | Reference |
| Yes | 171 (10.1) | 66 (12.9) | 1.32 (0.98; 1.79) | 0.84 (0.54; 1.32) |
| Diabetes | ||||
| No | 1616 (95.5) | 475 (92.9) | Reference | Reference |
| Yes | 77 (4.5) | 36 (7.1) | 1.59 (1.06; 2.40) | 0.93 (0.51; 1.72) |
| Hypertension | ||||
| No | 1651 (97.5) | 484 (94.7) | Reference | Reference |
| Yes | 42 (2.5) | 27 (5.3) | 2.19 (1.34; 3.59) | 1.32 (0.65; 2.68) |
| Nausea | ||||
| No | 1351 (79.8) | 378 (74.0) | Reference | Reference |
| Yes | 342 (20.2) | 133 (26.0) | 1.39 (1.10; 1.75) | 1.27 (0.92; 1.77) |
| Thyroid disease | ||||
| No | 1477 (87.2) | 454 (88.8) | Reference | Reference |
| Yes | 216 (12.8) | 57 (11.2) | 0.86 (0.63; 1.17) | 0.64 (0.42; 1.00) |
| Anemia | ||||
| No | 1530 (90.4) | 437 (85.5) | Reference | Reference |
| Yes | 163 (9.6) | 74 (14.5) | 1.59 (1.18; 2.14) | 1.47 (0.97; 2.23) |
| Concerns about reduced access to preferred medications | ||||
| Not at all concerned | 951 (56.2) | 195 (38.2) | Reference | Reference |
| A little concerned | 368 (21.7) | 131 (25.6) | 1.74 (1.35; 2.23) | 1.33 (0.93; 1.91) |
| Moderately/Very concerned | 374 (22.1) | 185 (36.2) | 2.41 (1.91; 3.05) | 1.31 (0.92; 1.87) |
| Concerns about unavailability of primary health care provider for hospital birth | ||||
| Not at all concerned | 137 (8.1) | 24 (4.7) | Reference | Reference |
| A little concerned | 324 (19.1) | 61 (11.9) | 1.08 (0.64; 1.80) | 1.15 (0.56; 2.36) |
| Moderately/Very concerned | 1232 (72.8) | 426 (83.4) | 1.97 (1.26; 3.09) | 0.99 (0.51; 1.94) |
| Concerns about a possible separation from baby after delivery | ||||
| Not at all concerned | 238 (14.1) | 35 (6.9) | Reference | Reference |
| A little concerned | 326 (19.2) | 64 (12.5) | 1.34 (0.86; 2.08) | 0.62 (0.32; 1.18) |
| Moderately/Very concerned | 1129 (66.7) | 412 (80.6) | 2.48 (1.71; 3.60) | 0.70 (0.36; 1.35) |
| Concerns about a shorter stay in hospital after delivery | ||||
| Not at all concerned | 639 (37.7) | 131 (25.6) | Reference | Reference |
| A little concerned | 430 (25.4) | 102 (20.0) | 1.16 (0.87; 1.54) | 0.97 (0.64; 1.45) |
| Moderately/Very concerned | 624 (36.9) | 278 (54.4) | 2.17 (1.72; 2.75) | 0.98 (0.67; 1.43) |
| Concerns about adequate opportunity for skin-to skin contact with newborn | ||||
| Not at all concerned | 336 (19.9) | 47 (9.2) | Reference | Reference |
| A little concerned | 385 (22.7) | 93 (18.2) | 1.73 (1.18; 2.53) | 1.75 (0.94; 3.27) |
| Moderately/Very concerned | 972 (57.4) | 371 (72.6) | 2.73 (1.97; 3.79) | 1.45 (0.75; 2.80) |
| Concerns about insufficient opportunity to initiate breastfeeding | ||||
| Not at all concerned | 444 (26.2) | 82 (16.1) | Reference | Reference |
| A little concerned | 357 (21.1) | 82 (16.1) | 1.24 (0.89; 1.74) | 0.79 (0.46; 1.35) |
| Moderately/Very concerned | 892 (52.7) | 347 (67.8) | 2.11 (1.61; 2.75) | 0.79 (0.47; 1.33) |
| Concerns about no visit from family and friends after delivery | ||||
| Not at all concerned | 356 (21.0) | 74 (14.5) | Reference | Reference |
| A little concerned | 348 (20.6) | 81 (15.8) | 1.12 (0.79; 1.59) | 0.88 (0.54; 1.43) |
| Moderately/Very concerned | 989 (58.4) | 356 (69.7) | 1.73 (1.31; 2.29) | 0.95 (0.63; 1.43) |
| Concerns about reduction of optimal postnatal care | ||||
| Not at all concerned | 339 (20.0) | 38 (7.4) | Reference | Reference |
| A little concerned | 421 (24.9) | 77 (15.1) | 1.63 (1.08; 2.47) | 1.25 (0.71; 2.20) |
| Moderately/Very concerned | 933 (55.1) | 396 (77.5) | 3.79 (2.65; 5.40) | 1.49 (0.86; 2.58) |
| Concerns about less access to lactation support after discharge from hospital | ||||
| Not at all concerned | 497 (29.4) | 83 (16.2) | Reference | Reference |
| A little concerned | 424 (25.0) | 94 (18.4) | 1.33 (0.96; 1.83) | 1.33 (0.83; 2.12) |
| Moderately/Very concerned | 772 (45.6) | 334 (65.4) | 2.59 (1.99; 3.38) | 1.56 (0.98; 2.46) |
| Concerns about birth complications due to contracting COVID-19 | ||||
| Not at all concerned | 242 (14.3) | 34 (6.7) | Reference | Reference |
| A little concerned | 500 (29.5) | 86 (16.8) | 1.22 (0.80; 1.87) | 0.83 (0.43; 1.62) |
| Moderately/Very concerned | 951 (56.2) | 391 (76.5) | 2.93 (2.01; 4.27) | 0.66 (0.33; 1.29) |
| Concerns about possible exposure to COVID-19 during pregnancy | ||||
| Not at all concerned | 121 (7.1) | 13 (2.5) | Reference | Reference |
| A little concerned | 469 (27.7) | 64 (12.5) | 1.27 (0.68; 2.38) | 0.59 (0.23; 1.49) |
| Moderately/Very concerned | 1103 (65.2) | 434 (85.0) | 3.66 (2.04; 6.56) | 0.67 (0.26; 1.74) |
| Concerns about possible exposure to COVID-19 during labour/delivery or shortly thereafter | ||||
| Not at all concerned | 164 (9.7) | 17 (3.3) | Reference | Reference |
| A little concerned | 505 (29.8) | 69 (13.5) | 1.32 (0.75; 2.31) | 0.74 (0.29; 1.87) |
| Moderately/Very concerned | 1024 (60.5) | 425 (83.2) | 4.00 (2.40; 6.68) | 0.93 (0.35; 2.46) |
| Concerns about baby being infected with COVID-19 after birth | ||||
| Not at all concerned | 91 (5.4) | 6 (1.2) | Reference | Reference |
| A little concerned | 379 (22.4) | 62 (12.1) | 2.48 (1.04; 5.91) | 2.45 (0.67; 8.96) |
| Moderately/Very concerned | 1223 (72.2) | 443 (86.7) | 5.49 (2.39; 12.64) | 1.61 (0.44; 5.98) |
| Concerns about being infected with COVID-19 and unable to care for newborn | ||||
| Not at all concerned | 156 (9.2) | 14 (2.7) | Reference | Reference |
| A little concerned | 427 (25.2) | 61 (11.9) | 1.59 (0.87; 2.93) | 1.72 (0.65; 4.51) |
| Moderately/Very concerned | 1110 (65.6) | 436 (85.3) | 4.38 (2.51; 7.65) | 2.12 (0.78; 5.79) |
| Work from home | ||||
| No | 1036 (61.2) | 313 (61.2) | Reference | Reference |
| Yes | 657 (38.8) | 198 (38.8) | 1.00 (0.81; 1.22) | 0.98 (0.73; 1.32) |
| Loss of job | ||||
| No | 1580 (93.3) | 444 (86.9) | Reference | Reference |
| Yes | 113 (6.7) | 67 (13.1) | 2.11 (1.53; 2.91) | 1.30 (0.80; 2.11) |
| Decreased take-home pay due to the COVID-19 pandemic | ||||
| No | 1335 (78.9) | 379 (74.2) | Reference | Reference |
| Yes | 358 (21.1) | 132 (25.8) | 1.30 (1.03; 1.63) | 1.15 (0.83; 1.60) |
| Change in daily routine | ||||
| No change | 52 (3.1) | 12 (2.4) | Reference | Reference |
| Mild | 259 (15.3) | 43 (8.4) | 0.72 (0.36; 1.46) | 0.55 (0.21; 1.43) |
| Moderate/severe | 1382 (81.6) | 456 (89.2) | 1.43 (0.76; 2.70) | 0.57 (0.23; 1.40) |
| Change in medical health care access | ||||
| No change | 640 (37.8) | 125 (24.4) | Reference | Reference |
| Mild | 855 (50.5) | 262 (51.3) | 1.57 (1.24; 1.99) | 1.12 (0.81; 1.54) |
| Moderate/severe | 198 (11.7) | 124 (24.3) | 3.21 (2.39; 4.31) | 1.32 (0.87; 2.01) |
| Change in access to family, extended family and non-family social support | ||||
| No change | 71 (4.2) | 14 (2.7) | Reference | Reference |
| Mild | 781 (46.1) | 119 (23.3) | 0.77 (0.42; 1.42) | 1.13 (0.45; 2.82) |
| Moderate/severe | 841 (49.7) | 378 (74.0) | 2.28 (1.27; 4.10) | 1.68 (0.68; 4.14) |
| Recruitment time (month and year) | - | - | - | 1.04 (1.01; 1.07) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bérard, A.; Gorgui, J.; Tchuente, V.; Lacasse, A.; Gomez, Y.-H.; Côté, S.; King, S.; Muanda, F.; Mufike, Y.; Boucoiran, I.; et al. The COVID-19 Pandemic Impacted Maternal Mental Health Differently Depending on Pregnancy Status and Trimester of Gestation. Int. J. Environ. Res. Public Health 2022, 19, 2926. https://doi.org/10.3390/ijerph19052926
Bérard A, Gorgui J, Tchuente V, Lacasse A, Gomez Y-H, Côté S, King S, Muanda F, Mufike Y, Boucoiran I, et al. The COVID-19 Pandemic Impacted Maternal Mental Health Differently Depending on Pregnancy Status and Trimester of Gestation. International Journal of Environmental Research and Public Health. 2022; 19(5):2926. https://doi.org/10.3390/ijerph19052926
Chicago/Turabian StyleBérard, Anick, Jessica Gorgui, Vanina Tchuente, Anaïs Lacasse, Yessica-Haydee Gomez, Sylvana Côté, Suzanne King, Flory Muanda, Yves Mufike, Isabelle Boucoiran, and et al. 2022. "The COVID-19 Pandemic Impacted Maternal Mental Health Differently Depending on Pregnancy Status and Trimester of Gestation" International Journal of Environmental Research and Public Health 19, no. 5: 2926. https://doi.org/10.3390/ijerph19052926