
Ecological Predictors of Older Adults’ Participation and Retention in a Physical Activity Intervention

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Literature Review
2.1. Individual-Level Factors
2.2. Ecological Factors
2.2.1. Socioeconomic Composition of the Neighborhood
2.2.2. Distance
2.2.3. Weather Conditions, Season and Holiday Periods
- (1)
- To determine whether the findings regarding individual-level factors associated with reduced participation and retention available thus far can be supported by the present study, which enrolled older German adults.
- (2)
- To identify ecological predictors and program-related determinants of overall participation and retention. Consideration will be given to the socioeconomic composition and setting (urban vs. suburban) of the participant’s neighborhood, as well as the proximity to intervention sites.
- (3)
- To determine associations of concise weather exposures and (public) holidays with weekly attendance rates in scheduled exercise classes.
3. Materials and Methods
3.1. Data and Procedures
3.1.1. Intervention Program
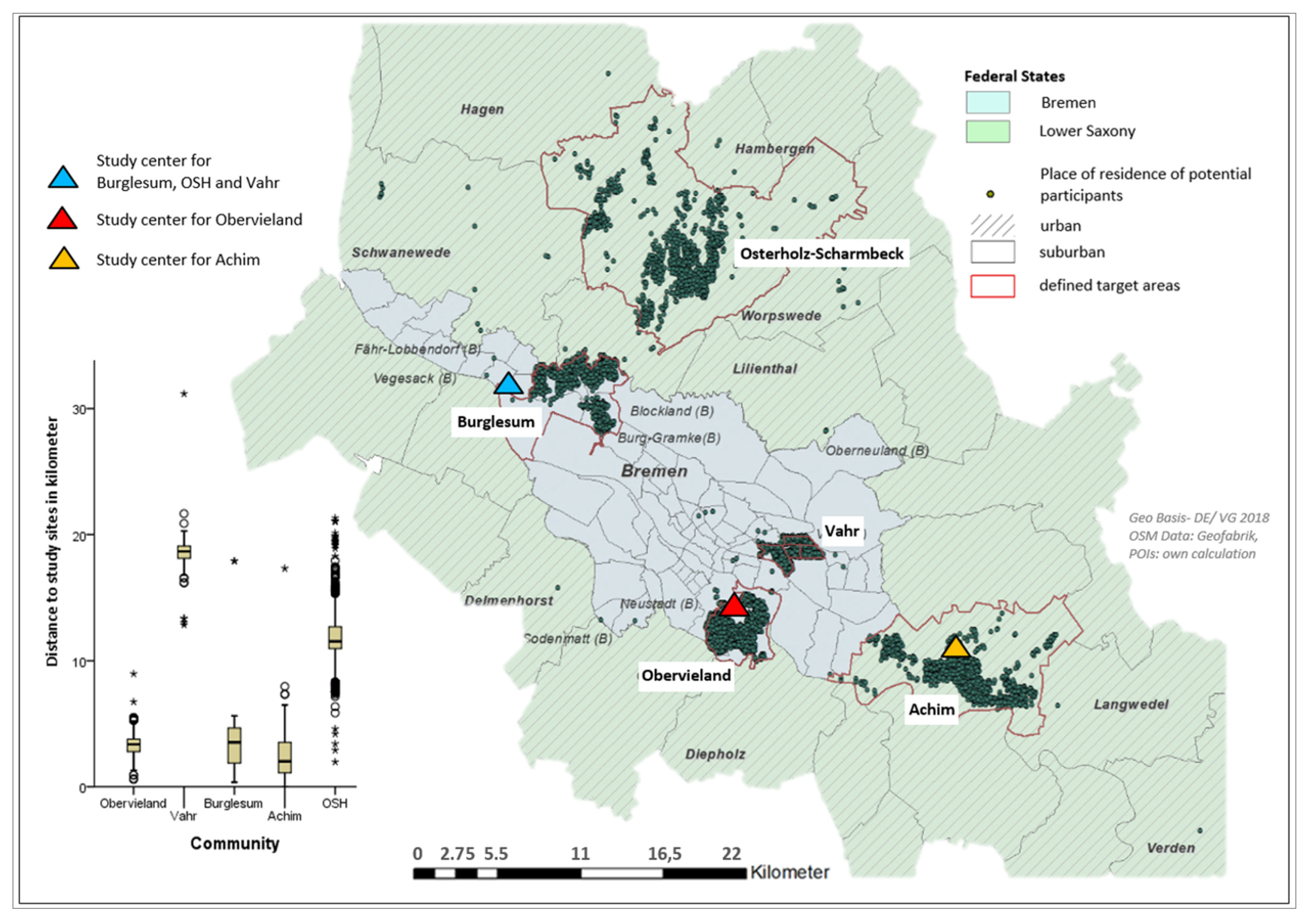
3.1.2. Ecological Data
3.2. Measures
3.2.1. Primary Outcomes
3.2.2. Potential Explanatory Variables
District Level Socio Economic Status
Proximities to Interventions Sites
Weather, Season, Public and School Holidays
Individual-Level Characteristics
3.3. Statistical Analysis
4. Results
4.1. Results Regarding Participant Enrollment
4.2. Results Regarding Retention
4.3. Survival Analysis and Stage of Dropout

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Contacted and Volunteers | Non-Responders * | Included Participants | Completed Study ** | Dropouts ** | p | V |
|---|---|---|---|---|---|---|---|
| N-Total (%) | 8474 | 6694 | 589 (7%) | 405 (68.8) | 184 (31.2) | ||
| Recruitment, n (%) | |||||||
| Contacted | 8299 | 6694 (80.7) | 459 (77.9) | 324 (70.6) | 135 (29.4) | 0.072 | 0.074 |
| Volunteers | 175 | 130 (22.1) | 81 (62.3) | 49 (37.7) | |||
| Community n (%) | |||||||
| Burglesum (urban) | 1085 (12.8) | 855 (78.8) | 87 (14.8) | 55 (63.2) | 32 (36.8) | 0.002 | 0.172 |
| Vahr (urban) | 2300 (27.1) | 1892 (82.3) | 85 (14.4) | 44 (51.8) | 41 (48.2) | ||
| Obervieland (urban) | 2257 (26.6) | 1734 (76.8) | 169 (28.7) | 121 (71.6) | 48 (28.4) | ||
| OSH (suburban) | 1457 (17.2) | 1100 (75.5) | 143 (24.3) | 108 (75.5) | 35 (24.5) | ||
| Achim (suburban) | 1375 (16.2) | 1109 (80.7) | 105 (17.8) | 77 (73.3) | 28 (26.7) | ||
| Neighborhood Settings, n (%) | |||||||
| Urban | 5642 (66.6) | 4481 (79.4) | 341 (57.9) | 220 (64.5) | 121 (35.5) | 0.009 | 0.107 |
| Suburban | 2832 (33.4) | 2209 (78.4) | 248 (42.1) | 185 (74.6) | 63 (25.4) | ||
| Missing | 4 | ||||||
| Age in years, mean (SD) | 71.4 (3.3) | 71.3 (3.2) | 71.6 (3.5) | ||||
| Age groups, n (%) | |||||||
| 60–64 | 5 (0.8) | 3 (60) | 2 (40.0) | 0.552 | 0.060 | ||
| 65–69 | 196 (33.3) | 136 (69.4) | 60 (30.6) | ||||
| 70–74 | 305 (51.8) | 215 (70.5) | 90 (29.5) | ||||
| 75–80 | 80 (13.6) | 50 (62.5) | 30 (37.5) | ||||
| Missing | 3 (0.5) | 1 (33.3) | 2 (66.7) | ||||
| Gender, n (%) | |||||||
| Male | 4146 (48.9) | 3376 (81.4) | 251 (42) | 182 (72.5) | 69 (27.5) | 0.096 | 0.069 |
| Female | 4328 (51.1) | 3314 (76.6) | 336 (58) | 223 (66.1) | 114 (33.9) | ||
| Season, n (%) | |||||||
| Fall/winter | 1872 (28) | 165 (28) | 135 (81.8) | 30 (18.2) | 0.001 | 0.176 | |
| Spring/summer | 4822 (72) | 424 (72) | 270 (63.7) | 154 (36.3) | |||
| Level of education, n (%) | |||||||
| ISCED low, moderate | 308 (52.3) | 201 (65.3) | 107 (34.7) | 0.019 | 0.098 | ||
| ISCED high | 261 (44.3) | 194 (74.3) | 67 (25.7) | ||||
| Missing | 20 (3.4) | 10 (50) | 10 (50) | ||||
| Employment status, n (%) | |||||||
| Employed or retired but working | 113 (19.2) | 71 (62.8) | 42 (37.2) | 0.070 | 0.076 | ||
| Retired or other | 454 (77.1) | 325 (71.6) | 129 (28.4) | ||||
| Missing | 22 (3.7) | 9 (41) | 13 (59) | ||||
| Household income, n (%) | |||||||
| Low | 164 (27.8) | 109 (66.5) | 55 (33.5) | 0.299 | 0.067 | ||
| Middle | 168 (28.5) | 118 (70.2) | 50 (29.8) | ||||
| High | 203 (34.5) | 150 (73.9) | 53 (26.1) | ||||
| Missing | 54 (9.2) | 28 (51.9) | 26 (48.1) | ||||
| Subjective health status n (%) | |||||||
| Excellent or very good | 144 (24.5) | 116 (80.6) | 28 (19.4) | 0.001 | 0.188 | ||
| Good | 333 (56.6) | 234 (70.3) | 99 (29.7) | ||||
| Less good or poor | 87 (14.7) | 46 (52.9) | 41 (41.1) | ||||
| Missing | 25 (4.2) | 9 (39) | 16 (64) | ||||
| District level SES, n (%) | |||||||
| First quartile (low) | 3779 (44.6) | 2904 (76.8) | 366 (62.1) | 262 (71.6) | 104 (28.4) | 0.011 | 0.138 |
| Second quartile (moderate) | 1911 (22.6) | 1509 (79) | 109 (18.5) | 76 (69.7) | 33 (30.3) | ||
| Third quartile (high) | 625 (7.4) | 482 (77.1) | 32 (5.4) | 14 (43.8) | 18 (56.3) | ||
| Fourth quartile (very high) | 2102 (24.8) | 1774 (84.4) | 75 (12.7) | 49 (65.3) | 26 (34.7) | ||
| Missing | 57 (0.7) | 25 (43.8) | 7 (1.2) | 4 (57.1) | 3 (42.9) | ||
| Distance to intervention sites in meters, n (%) | |||||||
| <800 (very low) | 102 (17.3) | 62 (60.8) | 40 (39.2) | 0.118 | 0.112 | ||
| 800–1599 (low) | 161 (27.3) | 115 (71.4) | 46 (28.6) | ||||
| 1600–3499 (moderate) | 203 (34.5) | 143 (70.4) | 60 (29.6) | ||||
| 3500–5000 (high) | 51 (8.7) | 40 (78.4) | 11 (21.6) | ||||
| >5000 (very high) | 72 (12.2) | 45 (62.5) | 27 (37.5) | ||||
| Missing | |||||||
4.4. Attendance in Weekly Onsite Classes
5. Discussion
5.1. Principal Findings
5.2. Individual-Level Factors Associated with Participation and Dropout
5.3. Ecological Predictors Associated with Response, Participation and Dropout
5.4. Factors Associated with Recruitment and Study Design
5.5. Impact of Season, Weather Conditions and Holiday Periods
5.6. Strengths and Limitations
6. Conclusions
Supplementary Materials
 rainfall > 15 l/m2,
rainfall > 15 l/m2,  temperature > 30.
temperature > 30.  :wind speed > 7, IG1a: web-based intervention with subjective PA self-monitoring, first group, IG1b: web-based intervention with subjective PA self-monitoring, second group, IG2a: web-based intervention with subjective and objective PA self-monitoring, first (only) group. Table S1: Number and type of weather expositions by different groups and communities. Note: * The number of groups in each community varied according to the total number of participants in that community. The target group size was about 20 participants. ** Those who left the study before the first class were not included.
:wind speed > 7, IG1a: web-based intervention with subjective PA self-monitoring, first group, IG1b: web-based intervention with subjective PA self-monitoring, second group, IG2a: web-based intervention with subjective and objective PA self-monitoring, first (only) group. Table S1: Number and type of weather expositions by different groups and communities. Note: * The number of groups in each community varied according to the total number of participants in that community. The target group size was about 20 participants. ** Those who left the study before the first class were not included. Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hupin, D.; Roche, F.; Gremeaux, V.; Chatard, J.C.; Oriol, M.; Gaspoz, J.M.; Barthelemy, J.C.; Edouard, P. Even a low-dose of moderate-to-vigorous physical activity reduces mortality by 22% in adults aged ≥ 60 years: A systematic review and meta-analysis. Br. J. Sport. Med. 2015, 49, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Barnett, D.W.; Barnett, A.; Nathan, A.; Van Cauwenberg, J.; Cerin, E. Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C.; Lancet Physical Activity Series 2 Executive Committee. Scaling up physical activity interventions worldwide: Stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef] [Green Version]
- Pfeifer, K.; Rütten, A. Nationale Empfehlungen für Bewegung und Bewegungsförderung. Gesundheitswesen 2017, 79, S2–S3. [Google Scholar] [CrossRef] [Green Version]
- Finger, J.D.; Mensink, G.; Lange, C.; Manz, K. Gesundheitsfördernde körperliche Aktivität in der Freizeit bei Erwachsenen in Deutschland. J. Health Monit. 2017, 2, 37–44. [Google Scholar]
- WHO. Global Recommendations on Physical Activty for Health; WHO: Geneva, Switzerland, 2010; Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 18 February 2022).
- Van Der Bij, A.K.; Laurant, M.G.; Wensing, M. Effectiveness of physical activity interventions for older adults: A review. Am. J. Prev. Med. 2002, 22, 120–133. [Google Scholar] [CrossRef]
- Sully, B.G.; Julious, S.A.; Nicholl, J. A reinvestigation of recruitment to randomised, controlled, multicenter trials: A review of trials funded by two UK funding agencies. Trials 2013, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e402. [Google Scholar] [CrossRef]
- Wichmann, F.; Brand, T.; Gansefort, D.; Darmann-Finck, I. Ready to participate? Using qualitative data to typify older adults’ reasons for (non-) participation in a physical activity promotion intervention. BMC Public Health 2019, 19, 1327. [Google Scholar] [CrossRef] [Green Version]
- Guertler, D.; Vandelanotte, C.; Kirwan, M.; Duncan, M.J. Engagement and nonusage attrition with a free physical activity promotion program: The case of 10,000 steps Australia. J. Med. Internet Res. 2015, 17, e4339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, R.M.; Atkins, C.J. Selective attrition causes overestimates of treatment effects in studies of weight loss. Addict. Behav. 1987, 12, 297–302. [Google Scholar] [CrossRef]
- Martin, K.A.; Sinden, A.R. Who will stay and who will go? A review of older adults’ adherence to randomized controlled trials of exercise. J. Aging Phys. Act. 2001, 9, 91–114. [Google Scholar] [CrossRef] [Green Version]
- Gul, R.B.; Ali, P.A. Clinical trials: The challenge of recruitment and retention of participants. J. Clin. Nurs. 2010, 19, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Hawley-Hague, H.; Horne, M.; Campbell, M.; Demack, S.; Skelton, D.A.; Todd, C. Multiple levels of influence on older adults’ attendance and adherence to community exercise classes. Gerontologist 2014, 54, 599–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killingback, C.; Tsofliou, F.; Clark, C. Older people’s adherence to community-based group exercise programmes: A multiple-case study. BMC Public Health 2017, 17, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carstensen, L.L. Evidence for a life-span theory of socioemotional selectivity. Curr. Dir. Psychol. Sci. 1995, 4, 151–156. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Social cognition models and health behaviour: A structured review. Psychol. Health 2000, 15, 173–189. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [Green Version]
- Barton, H.; Grant, M. A health map for the local human habitat. J. R. Soc. Promot. Health 2006, 126, 252. [Google Scholar] [CrossRef]
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jancey, J.; Lee, A.; Howat, P.; Clarke, A.; Wang, K.; Shilton, T. Reducing attrition in physical activity programs for older adults. J. Aging Phys. Act. 2007, 15, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Martin, A.D.; Taunton, J.E.; Rhodes, E.C.; Donnelly, M.; Elliot, J. Factors associated with exercise adherence among older adults. Sport. Med. 1999, 28, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Chatfield, M.D.; Brayne, C.E.; Matthews, F.E. A systematic literature review of attrition between waves in longitudinal studies in the elderly shows a consistent pattern of dropout between differing studies. J. Clin. Epidemiol. 2005, 58, 13–19. [Google Scholar] [CrossRef]
- Van Beijsterveldt, C.; Van Boxtel, M.; Bosma, H.; Houx, P.; Buntinx, F.; Jolles, J. Predictors of attrition in a longitudinal cognitive aging study: The Maastricht Aging Study (MAAS). J. Clin. Epidemiol. 2002, 55, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Brassington, G.S.; Atienza, A.A.; Perczek, R.E.; DiLorenzo, T.M.; King, A.C. Intervention-related cognitive versus social mediators of exercise adherence in the elderly. Am. J. Prev. Med. 2002, 23, 80–86. [Google Scholar] [CrossRef]
- McAuley, E.; Jerome, G.J.; Elavsky, S.; Marquez, D.X.; Ramsey, S.N. Predicting long-term maintenance of physical activity in older adults. Prev. Med. 2003, 37, 110–118. [Google Scholar] [CrossRef]
- Chinn, D.J.; White, M.; Howel, D.; Harland, J.O.; Drinkwater, C.K. Factors associated with non-participation in a physical activity promotion trial. Public Health 2006, 120, 309–319. [Google Scholar] [CrossRef]
- Lakerveld, J.; IJzelenberg, W.; Van Tulder, M.W.; Hellemans, I.M.; Rauwerda, J.A.; Van Rossum, A.C.; Seidell, J.C. Motives for (not) participating in a lifestyle intervention trial. BMC Med. Res. Methodol. 2008, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Picorelli, A.M.; Pereira, L.S.; Pereira, D.S.; Felício, D.; Sherrington, C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: A systematic review. J. Physiother. 2014, 60, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Resnick, B.; Spellbring, A.M. Understanding what motivates older adults to exercise. J. Gerontol. Nurs. 2000, 26, 34–42. [Google Scholar] [CrossRef]
- Manaf, H. Barriers to participation in physical activity and exercise among middle-aged and elderly individuals. Singap. Med. J. 2013, 54, 581–586. [Google Scholar]
- Forsat, N.D.; Palmowski, A.; Palmowski, Y.; Boers, M.; Buttgereit, F. Recruitment and retention of older people in clinical research: A systematic literature review. J. Am. Geriatr. Soc. 2020, 68, 2955–2963. [Google Scholar] [CrossRef]
- Elzen, H.; Slaets, J.P.; Snijders, T.A.; Steverink, N. Do older patients who refuse to participate in a self-management intervention in the Netherlands differ from older patients who agree to participate? Aging Clin. Exp. Res. 2008, 20, 266–271. [Google Scholar] [CrossRef] [Green Version]
- Bentley, C.L.; Powell, L.; Potter, S.; Parker, J.; Mountain, G.A.; Bartlett, Y.K.; Farwer, J.; O’Connor, C.; Burns, J.; Cresswell, R.L. The use of a smartphone app and an activity tracker to promote physical activity in the management of chronic obstructive pulmonary disease: Randomized controlled feasibility study. JMIR MHealth uHealth 2020, 8, e16203. [Google Scholar] [CrossRef]
- Jacomb, P.A.; Jorm, A.F.; Korten, A.E.; Christensen, H.; Henderson, A.S. Predictors of refusal to participate: A longitudinal health survey of the elderly in Australia. BMC Public Health 2002, 2, 4. [Google Scholar] [CrossRef]
- Wichmann, F.; Pischke, C.R.; Jurgens, D.; Darmann-Finck, I.; Koppelin, F.; Lippke, S.; Pauls, A.; Peters, M.; Voelcker-Rehage, C.; Muellmann, S. Requirements for (web-based) physical activity interventions targeting adults above the age of 65 years-qualitative results regarding acceptance and needs of participants and non-participants. BMC Public Health 2020, 20, 907. [Google Scholar] [CrossRef]
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- King, A.C.; Blair, S.N.; Bild, D.E.; Dishman, R.K.; Dubbert, P.M.; Marcus, B.H.; Oldridge, N.B.; Paffenbarger, R.S.; Powell, K.E.; Yeager, K.K. Determinants of physical activity and interventions in adults. Med. Sci. Sport. Exerc. 1992, 24, S221–S236. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.-M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Humpel, N.; Owen, N.; Leslie, E. Environmental factors associated with adults’ participation in physical activity: A review. Am. J. Prev. Med. 2002, 22, 188–199. [Google Scholar] [CrossRef]
- Owen, N.; Humpel, N.; Leslie, E.; Bauman, A.; Sallis, J.F. Understanding environmental influences on walking: Review and research agenda. Am. J. Prev. Med. 2004, 27, 67–76. [Google Scholar] [CrossRef]
- Kamphuis, C.B.M.; Van Lenthe, F.J.; Giskes, K.; Huisman, M.; Brug, J.; Mackenbach, J.P. Socioeconomic Status, Environmental and Individual Factors, and Sports Participation. Med. Sci. Sport. Exerc. 2008, 40, 71–81. [Google Scholar] [CrossRef]
- Knechel, N.A. The challenges of enrolling older adults into intervention studies. Yale J. Biol. Med. 2013, 86, 41. [Google Scholar]
- Martinez, I.L.; Kim, K.; Tanner, E.; Fried, L.P.; Seeman, T. Ethnic and class variations in promoting social activities among older adults. Act. Adapt. Aging 2009, 33, 96–119. [Google Scholar] [CrossRef]
- Franke, T.; Sims-Gould, J.; Chaudhury, H.; Winters, M.; McKay, H. Re-framing mobility in older adults: An adapted comprehensive conceptual framework. Qual. Res. Sport Exerc. Health 2020, 12, 336–349. [Google Scholar] [CrossRef]
- Boyette, L.W.; Lloyd, A.; Boyette, J.E.; Watkins, E.; Furbush, L.; Dunbar, S.B.; Brandon, L.J. Personal characteristics that influence exercise behavior of older adults. J. Rehabil. Res. Dev. 2002, 39, 95–104. [Google Scholar]
- Van Lenthe, F.J.; Brug, J.; Mackenbach, J.P. Neighbourhood inequalities in physical inactivity: The role of neighbourhood attractiveness, proximity to local facilities and safety in the Netherlands. Soc. Sci. Med. 2005, 60, 763–775. [Google Scholar] [CrossRef]
- Liljas, A.E.; Walters, K.; Jovicic, A.; Iliffe, S.; Manthorpe, J.; Goodman, C.; Kharicha, K. Strategies to improve engagement of ‘hard to reach’older people in research on health promotion: A systematic review. BMC Public Health 2017, 17, 349. [Google Scholar] [CrossRef] [Green Version]
- Wahl, H.-W.; Lang, F.R. Aging in context across the adult life course: Integrating physical and social environmental research perspectives. Annu. Rev. Gerontol. Geriatr. 2003, 23, 1–33. [Google Scholar]
- Odierna, D.H.; Bero, L.A. Retaining participants in outpatient and community-based health studies: Researchers and participants in their own words. SAGE Open 2014, 4, 2158244014554391. [Google Scholar] [CrossRef]
- Cherubini, A.; Signore, S.D.; Ouslander, J.; Semla, T.; Michel, J.P. Fighting against age discrimination in clinical trials. J. Am. Geriatr. Soc. 2010, 58, 1791–1796. [Google Scholar] [CrossRef]
- Roigk, P.; Kampe, K.; Rapp, K.; Rupp, K.; Pfeiffer, K. Teilnahmebereitschaft und Adhärenz von Teilnehmern an “Trittsicher” -Bewegungskursen. Physioscience 2019, 15, 53–62. [Google Scholar] [CrossRef]
- Belza, B.; Chiang, K.-C.; Seman, L.; Tsai, J.H.-C. Peer Reviewed: “It Is Our Exercise Family”: Experiences of Ethnic Older Adults in a Group-Based Exercise Program. Prev. Chronic Dis. 2008, 5, A05. [Google Scholar]
- Knox, P.L. The intraurban ecology of primary medical care: Patterns of accessibility and their policy implications. Environ. Plan. A 1978, 10, 415–435. [Google Scholar] [CrossRef]
- Basche, M.; Barón, A.E.; Eckhardt, S.G.; Balducci, L.; Persky, M.; Levin, A.; Jackson, N.; Zeng, C.; Vranas, P.; Steiner, J.F. Barriers to enrollment of elderly adults in early-phase cancer clinical trials. J. Oncol. Pract. 2008, 4, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.K.; Tobin, J.D.; Brant, L.J. Factors affecting attrition in the Baltimore Longitudinal Study of Aging. Exp. Gerontol. 1986, 21, 329–340. [Google Scholar] [CrossRef]
- Farber, S.; Páez, A.; Mercado, R.G.; Roorda, M.; Morency, C. A time-use investigation of shopping participation in three Canadian cities: Is there evidence of social exclusion? Transportation 2011, 38, 17–44. [Google Scholar] [CrossRef]
- Follmer, R.; Gruschwitz, D.; Jesske, B.; Quandt, S.; Lenz, B.; Nobis, C.; Mehlin, M. Mobilität in Deutschland 2008: Ergebnisbericht; Technical Report; Federal Ministry for Transport, Building and Urban Development, INFAS, DLR: Berlin, Germany, 2010. [Google Scholar]
- Van den Berg, P.; Arentze, T.; Timmermans, H. Estimating social travel demand of senior citizens in the Netherlands. J. Transp. Geogr. 2011, 19, 323–331. [Google Scholar] [CrossRef]
- Scheiner, J. Interrelations between travel mode choice and trip distance: Trends in Germany 1976–2002. J. Transp. Geogr. 2010, 18, 75–84. [Google Scholar] [CrossRef]
- Tucker, P.; Gilliland, J. The effect of season and weather on physical activity: A systematic review. Public Health 2007, 121, 909–922. [Google Scholar] [CrossRef]
- Díaz, J.; Garcia, R.; De Castro, F.V.; Hernández, E.; López, C.; Otero, A. Effects of extremely hot days on people older than 65 years in Seville (Spain) from 1986 to 1997. Int. J. Biometeorol. 2002, 46, 145–149. [Google Scholar]
- Clarke, P.J.; Yan, T.; Keusch, F.; Gallagher, N.A. The Impact of Weather on Mobility and Participation in Older U.S. Adults. Am. J. Public Health 2015, 105, 1489–1494. [Google Scholar] [CrossRef]
- Böcker, L.; Priya Uteng, T.; Liu, C.; Dijst, M. Weather and daily mobility in international perspective: A cross-comparison of Dutch, Norwegian and Swedish city regions. Transp. Res. Part D Transp. Environ. 2019, 77, 491–505. [Google Scholar] [CrossRef]
- Böcker, L.; Dijst, M.; Prillwitz, J. Impact of everyday weather on individual daily travel behaviours in perspective: A literature review. Transp. Rev. 2013, 33, 71–91. [Google Scholar] [CrossRef]
- Tu, W.; Stump, T.E.; Damush, T.M.; Clark, D.O. The effects of health and environment on exercise-class participation in older, urban women. J. Aging Phys. Act. 2004, 12, 480–496. [Google Scholar] [CrossRef]
- Chan, C.B.; Ryan, D.A.; Tudor-Locke, C. Relationship between objective measures of physical activity and weather: A longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Tulloch, H.; Sweet, S.N.; Fortier, M.; Capstick, G.; Kenny, G.P.; Sigal, R.J. Exercise facilitators and barriers from adoption to maintenance in the diabetes aerobic and resistance exercise trial. Can. J. Diabetes 2013, 37, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Bogart, L.M.; Uyeda, K. Community-based participatory research: Partnering with communities for effective and sustainable behavioral health interventions. Health Psychol. 2009, 28, 391–393. [Google Scholar] [CrossRef] [Green Version]
- Burton, E.; Hill, A.-M.; Pettigrew, S.; Lewin, G.; Bainbridge, L.; Farrier, K.; Airey, P.; Hill, K.D. Why do seniors leave resistance training programs? Clin. Interv. Aging 2017, 12, 585. [Google Scholar] [CrossRef] [Green Version]
- Dolansky, M.A.; Stepanczuk, B.; Charvat, J.M.; Moore, S.M. Women’s and men’s exercise adherence after a cardiac event: Does age make a difference? Res. Gerontol. Nurs. 2010, 3, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Forberger, S.; Bammann, K.; Bauer, J.; Boll, S.; Bolte, G.; Brand, T.; Hein, A.; Koppelin, F.; Lippke, S.; Meyer, J.; et al. How to Tackle Key Challenges in the Promotion of Physical Activity among Older Adults (65+): The AEQUIPA Network Approach. Int. J. Environ. Res Public Health 2017, 14, 379. [Google Scholar] [CrossRef] [Green Version]
- Muellmann, S.; Bragina, I.; Voelcker-Rehage, C.; Rost, E.; Lippke, S.; Meyer, J.; Schnauber, J.; Wasmann, M.; Toborg, M.; Koppelin, F. Development and evaluation of two web-based interventions for the promotion of physical activity in older adults: Study protocol for a community-based controlled intervention trial. BMC Public Health 2017, 17, 512. [Google Scholar] [CrossRef] [Green Version]
- Muellmann, S.; Buck, C.; Voelcker-Rehage, C.; Bragina, I.; Lippke, S.; Meyer, J.; Peters, M.; Pischke, C.R. Effects of two web-based interventions promoting physical activity among older adults compared to a delayed intervention control group in Northwestern Germany: Results of the PROMOTE community-based intervention trial. Prev. Med. Rep. 2019, 15, 100958. [Google Scholar] [CrossRef]
- Gansefort, D.; Brand, T.; Princk, C.; Zeeb, H. Community readiness for the promotion of physical activity in older adults—A cross-sectional comparison of rural and urban communities. Int. J. Environ. Res. Public Health 2018, 15, 453. [Google Scholar] [CrossRef] [Green Version]
- Climate Data Center. Data Portal. Available online: https://cdc.dwd.de/portal/ (accessed on 18 February 2022).
- Schulferien.org. Schulferien, Kalender, Feiertage. Available online: https://www.schulferien.org/deutschland/ (accessed on 18 February 2022).
- Geyer, S. Einzelindikator oder index? Masse sozialer Differenzierung im Vergleich. Gesundheitswesen 2008, 70, 281–288. [Google Scholar] [CrossRef]
- Kukulska, A.; Salata, T.; Cegielska, K.; Szylar, M. Methodology of evaluation and correction of geometric data topology in QGIS software. Acta Sci. Polonorum. Form. Circumiectus 2018, 17, 137–150. [Google Scholar] [CrossRef]
- Peters, M.; Muellmann, S.; Christianson, L.; Stalling, I.; Bammann, K.; Drell, C.; Forberger, S. Measuring the association of objective and perceived neighborhood environment with physical activity in older adults: Challenges and implications from a systematic review. Int. J. Health Geogr. 2020, 19, 47. [Google Scholar] [CrossRef]
- Villanueva, K.; Knuiman, M.; Nathan, A.; Giles-Corti, B.; Christian, H.; Foster, S.; Bull, F. The impact of neighborhood walkability on walking: Does it differ across adult life stage and does neighborhood buffer size matter? Health Place 2014, 25, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Davern, M.; Gunn, L.; Whitzman, C.; Higgs, C.; Giles-Corti, B.; Simons, K.; Villanueva, K.; Mavoa, S.; Roberts, R.; Badland, H. Using spatial measures to test a conceptual model of social infrastructure that supports health and wellbeing. Cities Health 2017, 1, 194–209. [Google Scholar] [CrossRef] [Green Version]
- Buck, C.; Dreger, S.; Pigeot, I. Anonymisation of address coordinates for microlevel analyses of the built environment: A simulation study. BMJ Open 2015, 5, e006481. [Google Scholar] [CrossRef] [Green Version]
- DWD. Warnkriterien. Available online: https://www.dwd.de/DE/wetter/warnungen_aktuell/kriterien/warnkriterien.html?nn=508722 (accessed on 18 February 2022).
- Bundesamt, S. Demographische Standards Ausageb 2016 Statistik und Wissenschaft; Statistisches Bundesamt: Wiesbaden, Germany, 2016; Volume 17. [Google Scholar]
- Bertelsmann Stiftung, Sozialplanung Für Senioren. Fragebogen TF 1 Demografische und Sozio-Kulturelle Daten. Available online: http://www.sozialplanung-senioren.de/frageboegen-bausteine/frageboegen-nach-themenfeldern/index.html?L=0%2F%2F%2F%2F%27tyl (accessed on 18 February 2022).
- Robert-Koch-Institut. Studie zur Gesundheit Erwachsener in Deutschland (DEGS): Gesundheitsfragebogen ab 65 Jahren; Bundesministerium für Gesundheit und Robert Koch-Institut: Berlin, Germany, 2009. [Google Scholar]
- Boehle, M. Armutsmessung mit dem Mikrozensus: Methodische Aspekte und Umsetzung für Querschnitts-und Trendanalysen; GESIS Papers 2015/16; GESIS-Leibniz-Institut für Sozialwissenschaften: Mannheim, Germany, 2015. [Google Scholar]
- Morfeld, M.; Kirchberger, I.; Bullinger, M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche Version des Short Form-36 Health Survey; Hogrefe: Göttingen, Germany, 2011. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Schmidt, J.A.; Gruman, C.; King, M.B.; Wolfson, L.I. Attrition in an exercise intervention: A comparison of early and later dropouts. J. Am. Geriatr. Soc. 2000, 48, 952–960. [Google Scholar] [CrossRef]
- Davies, C.A.; Spence, J.C.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W.K. Meta-analysis of internet-delivered interventions to increase physical activity levels. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 52. [Google Scholar] [CrossRef] [Green Version]
- Ryan, C.; Bergin, M.; Wells, J.S.G. Theoretical Perspectives of Adherence to Web-Based Interventions: A Scoping Review. Int. J. Behav. Med. 2018, 25, 17–29. [Google Scholar] [CrossRef]
- Verheijden, M.W.; Jans, M.P.; Hildebrandt, V.H.; Hopman-Rock, M. Rates and determinants of repeated participation in a web-based behavior change program for healthy body weight and healthy lifestyle. J. Med. Internet Res. 2007, 9, e1. [Google Scholar] [CrossRef] [Green Version]
- Cai, Z.; Fan, X.; Du, J. Gender and attitudes toward technology use: A meta-analysis. Comput. Educ. 2017, 105, 1–13. [Google Scholar] [CrossRef]
- Rosenbloom, S. Sustainability and automobility among the elderly: An international assessment. Transportation 2001, 28, 375–408. [Google Scholar] [CrossRef]
- Rosenbloom, S.; Waldorf, B. Older travelers: Does place or race make a difference? Transp. Res. Circ. 2001, E-C026, 103–120. [Google Scholar]
- Warren-Findlow, J.; Prohaska, T.R.; Freedman, D. Challenges and opportunities in recruiting and retaining underrepresented populations into health promotion research. Gerontologist 2003, 43, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Oenema, A.; Brug, J.; Dijkstra, A.; de Weerdt, I.; de Vries, H. Efficacy and use of an internet-delivered computer-tailored lifestyle intervention, targeting saturated fat intake, physical activity and smoking cessation: A randomized controlled trial. Ann. Behav. Med. 2008, 35, 125–135. [Google Scholar] [CrossRef]
- Boulton, E.R.; Horne, M.; Todd, C. Multiple influences on participating in physical activity in older age: Developing a social ecological approach. Health Expect. 2018, 21, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Giles-Corti, B.; Donovan, R.J. The relative influence of individual, social and physical environment determinants of physical activity. Soc. Sci. Med. 2002, 54, 1793–1812. [Google Scholar] [CrossRef]
- Bartsch, A. As time goes by: What changes and what remains the same in entertainment experience over the life span? J. Commun. 2012, 62, 588–608. [Google Scholar] [CrossRef] [Green Version]
- Hendricks, J.; Cutler, S.J. Volunteerism and socioemotional selectivity in later life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2004, 59, S251–S257. [Google Scholar] [CrossRef] [Green Version]
- Wong, D.W.S. The modifiable areal unit problem (MAUP). In WorldMinds: Geographical Perspectives on 100 Problems; Springer: Dordrecht, The Netherlands, 2004; pp. 571–575. [Google Scholar]
- Chan, Y. Biostatistics 104: Correlational analysis. Singapore Med. J. 2003, 44, 614–619. [Google Scholar]


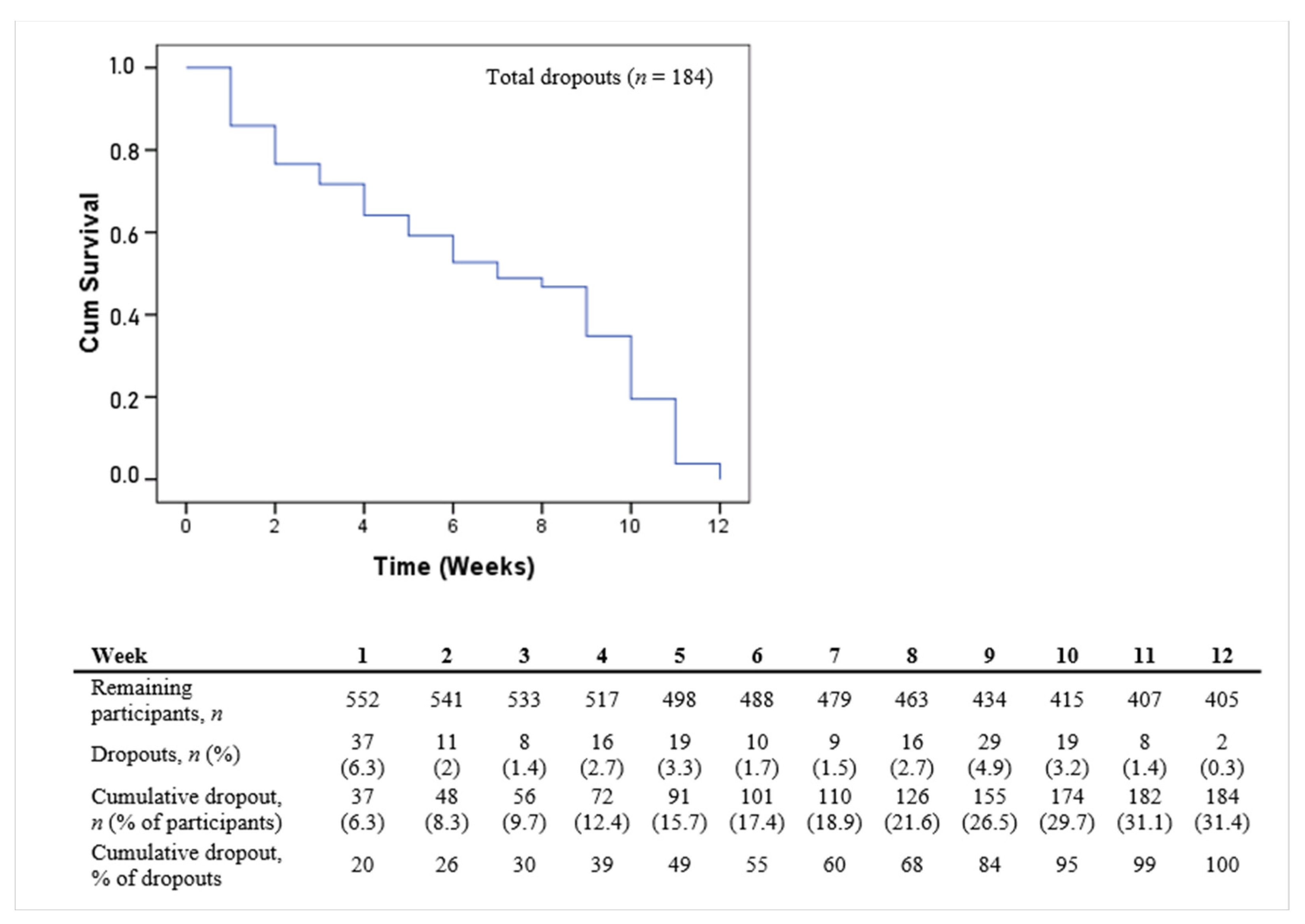
 censored data = end of observation period (week twelve).
censored data = end of observation period (week twelve).
censored data = end of observation period (week twelve).
censored data = end of observation period (week twelve). rainfall > 15 l/m2, temperature > 30. IG1a: web-based intervention with subjective PA self-monitoring, first group, IG1b: web-based intervention with subjective PA self-monitoring, second group, IG2a: web-based intervention with subjective and objective PA self-monitoring, first (only) group.
rainfall > 15 l/m2, temperature > 30. IG1a: web-based intervention with subjective PA self-monitoring, first group, IG1b: web-based intervention with subjective PA self-monitoring, second group, IG2a: web-based intervention with subjective and objective PA self-monitoring, first (only) group.
rainfall > 15 l/m2, temperature > 30. IG1a: web-based intervention with subjective PA self-monitoring, first group, IG1b: web-based intervention with subjective PA self-monitoring, second group, IG2a: web-based intervention with subjective and objective PA self-monitoring, first (only) group.
rainfall > 15 l/m2, temperature > 30. IG1a: web-based intervention with subjective PA self-monitoring, first group, IG1b: web-based intervention with subjective PA self-monitoring, second group, IG2a: web-based intervention with subjective and objective PA self-monitoring, first (only) group.
| Response | Dropout from the Study and Attendance in Weekly Onsite Classes | |||
|---|---|---|---|---|
| N | Characteristics | Data Source | Characteristics | Data Source |
| Individual level | Age | Registration office | Age | Telephone interviews |
| Gender | Registration office | Gender | Telephone interviews | |
| Residential address | Registration office | Residential address | Registration office | |
| Level of education | Questionnaire | |||
| Employment status | Questionnaire | |||
| Household income | Questionnaire | |||
| Perceived health | Questionnaire | |||
| Ecological level | Neighborhood SES | Statistical offices 1 | Neighborhood SES | Statistical offices 1 |
| Proximity | Geocoded home addresses | Proximity | Geocoded home addresses | |
| Geocoded study center | Geocoded intervention sites | |||
| OSM street network data | OSM street network data | |||
| Weather 2 | GWS/CDC | |||
| Season | Study Data | |||
| Public/school holidays 2 | schulferien.org | |||
| Characteristics | Univariate HR (SE), 95% CI | p | Multivariate HR Beginning Model (SE), 95% CI | p | Multivariate HR Final Model * (SE), 95% CI | p |
|---|---|---|---|---|---|---|
| Community | ||||||
| Obervieland (urban) | Reference | 0.001 | Reference | 0.011 | Reference | 0.003 |
| Vahr (urban) | 1.987 (0.213), 1.309–3.015 | 0.001 | 1.878 (0.253), 1.144–3.080 | 0.013 | 1.803 (0.227), 1.155–2.815 | 0.009 |
| Burglesum (urban) | 1.278 (0.228), 0.817–1.998 | 0.283 | 1.258 (0.282), 0.724–2.187 | 0.415 | 1.356 (0.252), 0.828–2.221 | 0.226 |
| Achim (suburban) | 0.923 (0.238), 0.579–1.407 | 0.735 | 0.671 (0.308), 0.367–1.227 | 0.195 | 0.777 (0.265), 0.426–1.306 | 0.341 |
| OSH (suburban) | 0.837 (0.222), 0.541–1.293 | 0.422 | 0.663 (0.295), 0.372–1.120 | 0.163 | 0.816 (0.235), 0.515–1.295 | 0.388 |
| Intervention Group | ||||||
| CG | reference | 0.001 | reference | 0.001 | reference | 0.001 |
| IG1 | 1.437 (0.201), 0.696–2.130 | 0.072 | 1.770 (0.232), 1.123–2.790 | 0.014 | 1.149 (0.229), 1.149–2.822 | 0.010 |
| IG2 | 2.057 (0.194), 1.406–3.009 | 0.001 | 2.767 (0.223), 1.786–4.286 | 0.001 | 2.666 (0.219), 1.737–4.093 | 0.001 |
| Level of education | ||||||
| Low/moderate | reference | reference | reference | |||
| High | 0.683 (0.156), 0.503–0.927 | 0.014 | 0.693 (0.171), 0.495–0.969 | 0.032 | 0.674 (0.165), 0.488–0.931 | 0.017 |
| Subjective health status | ||||||
| Excellent or very good | reference | 0.292 | reference | 0.001 | reference | 0.001 |
| Good | 0.852 (0.195), 0.581–1.250 | 0.414 | 1.692 (0.224), 1.092–2.623 | 0.019 | 1.658 (0.222), 1.072–2.563 | 0.023 |
| Less good or poor | 0.740 (0.193), 0.507–1.079 | 0.117 | 2.510 (0.263), 1.500–4.200 | 0.001 | 2.644 (0.259), 1.590–4.396 | 0.001 |
| Employment status | ||||||
| Employed or retired but working | reference | reference | ||||
| Retired or other | 0.745 (0.178), 0.526–1.056 | 0.098 | 0.772 (0.190), 0.532–1.120 | 0.173 | ||
| District level SES | ||||||
| First quartile (low) | reference | 0.027 | reference | 0.854 | ||
| Second quartile (moderate) | 1.116 (0.200), 0.754–1.651 | 0.583 | 0.813 (0.258), 0.490–1.349 | 0.424 | ||
| Third quartile (high) | 2.143(0.255), 1.299–3.536 | 0.003 | 0.909 (0.358), 0.451–1.832 | 0.789 | ||
| Fourth quartile (very high) | 1.253 (0.219), 0.815–1.926 | 0.304 | 0.987 (0.299), 0.544–1.758 | 0.978 | ||
| Gender | ||||||
| Male | reference | reference | ||||
| Female | 1.319 (0.153), 0.978–1.778 | 0.070 | 1.212 (0.137), 0.863–1.702 | 0.267 | ||
| Distance to intervention sites in meters | ||||||
| <800 (very low) | reference | 0.150 | reference | 0.297 | ||
| 800–1599 (low) | 0.696 (0.216), 0.455–1.063 | 0.093 | 0.670 (0.246), 0.414–1.087 | 0.105 | ||
| 1600–3499 (moderate) | 0.726 (0.204), 0.486–1.083 | 0.117 | 0.858 (0.237), 0.539–1.367 | 0.520 | ||
| 3500–5000 (high) | 0.493 (0.341), 0.253–0.962 | 0.038 | 0.771 (0.389), 0.360–1.652 | 0.503 | ||
| >5000 (very high) | 0.951 (0.249), 0.583–1.549 | 0.839 | 1.216 (0.299), 0.677–2.184 | 0.513 | ||
| Neighborhood setting ** | ||||||
| Urban | reference | |||||
| Suburban | 0.676 (0.155), 0.498–0.917 | 0.012 | ||||
| Age (years) | ||||||
| 60 < 65 | reference | 0.548 | ||||
| 65 < 70 | 0.873 (0.719), 0.213–3.572 | 0.850 | ||||
| 70 < 75 | 0.850 (0.715). 0.209–3.450 | 0.820 | ||||
| 75 < 80 | 1.131 (0.730). 0.270–4.735 | 0.866 | ||||
| Recruitment | ||||||
| Contacted | reference | |||||
| Volunteers | 1.312 (0.167), 0.946–1.820 | 0.103 | ||||
| Household income | ||||||
| Low | reference | 0.948 | ||||
| Middle | 0.939 (0.197), 0.637–1.382 | 0.748 | ||||
| High | 0.979 (0.195), 0.668–1.434 | 0.914 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peters, M.; Ratz, T.; Wichmann, F.; Lippke, S.; Voelcker-Rehage, C.; Pischke, C.R. Ecological Predictors of Older Adults’ Participation and Retention in a Physical Activity Intervention. Int. J. Environ. Res. Public Health 2022, 19, 3190. https://doi.org/10.3390/ijerph19063190
Peters M, Ratz T, Wichmann F, Lippke S, Voelcker-Rehage C, Pischke CR. Ecological Predictors of Older Adults’ Participation and Retention in a Physical Activity Intervention. International Journal of Environmental Research and Public Health. 2022; 19(6):3190. https://doi.org/10.3390/ijerph19063190
Chicago/Turabian StylePeters, Manuela, Tiara Ratz, Frauke Wichmann, Sonia Lippke, Claudia Voelcker-Rehage, and Claudia R. Pischke. 2022. "Ecological Predictors of Older Adults’ Participation and Retention in a Physical Activity Intervention" International Journal of Environmental Research and Public Health 19, no. 6: 3190. https://doi.org/10.3390/ijerph19063190
APA StylePeters, M., Ratz, T., Wichmann, F., Lippke, S., Voelcker-Rehage, C., & Pischke, C. R. (2022). Ecological Predictors of Older Adults’ Participation and Retention in a Physical Activity Intervention. International Journal of Environmental Research and Public Health, 19(6), 3190. https://doi.org/10.3390/ijerph19063190