
Association between Clinical Use of Colchicine and Risk of Type 2 Diabetes Mellitus among Gouty Patients: A Nationwide Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
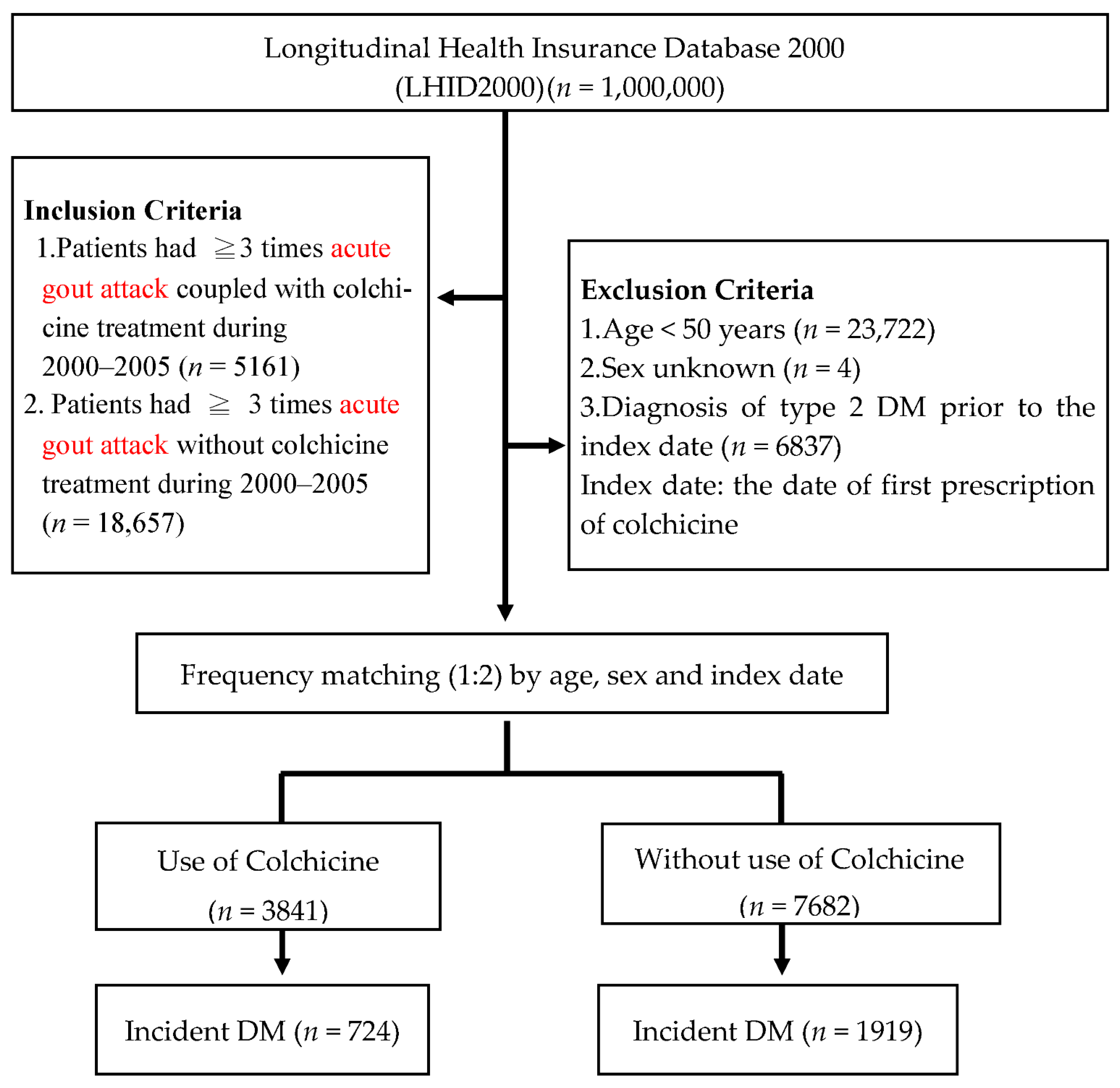
2.2. Study Design and Study Population
2.3. Ascertainment of Type 2 Diabetes Mellitus
2.4. Covariate Assessment and Adjustment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richette, P.; Bardin, T. Gout. Lancet 2010, 375, 318–328. [Google Scholar] [CrossRef]
- Kim, S.C.; Liu, J.; Solomon, D.H. Risk of incident diabetes in patients with gout: A cohort study. Arthritis Rheumatol. 2015, 67, 273–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rho, Y.H.; Lu, N.; Peloquin, C.E.; Man, A.; Zhu, Y.; Zhang, Y.; Choi, H.K. Independent—Impact of gout on the risk of diabetes mellitus among women and men: A population-based, BMI-matched cohort study. Ann. Rheum. Dis. 2016, 75, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Ford, E.S.; Li, C.; Curhan, G. Prevalence of the metabolic syndrome in patients with gout: The Third National Health and Nutrition Examination Survey. Arthritis Rheumatol. 2007, 57, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Feig, D.I.; Kang, D.H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef]
- Chiang, K.M.; Tsay, Y.C.; Vincent Ng, T.C.; Yang, H.C.; Huang, Y.T.; Chen, C.H.; Pan, W.H. Is hyperuricemia, an early-onset metabolic disorder, causally associated with cardiovascular disease events in Han Chinese? J. Clin. Med. 2019, 8, 1202. [Google Scholar] [CrossRef] [Green Version]
- Gaubert, M.; Bardin, T.; Cohen-Solal, A.; Dievart, F.; Fauvel, J.P.; Guien, R.; Sadrin, S.; Maixent, J.M.; Galinier, M.; Paganelli, F. Hyperuricemia and hypertension, coronary artery disease, kidney Disease: From concept to practice. Int. J. Mol. Sci. 2020, 21, 4066. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Yessirkepov, M.; Kitas, G.D. Colchicine as an anti-inflammatory and cardioprotective agent. Expert Opin. Drug Metab. Toxicol. 2015, 11, 1781–1794. [Google Scholar] [CrossRef]
- Kotwas, A.; Karakiewicz, B.; Zabielska, P.; Wieder-Huszla, S.; Jurczak, A. Epidemiological factors for type 2 diabetes mellitus: Evidence from the global burden of disease. Arch. Public Health 2021, 79, 110. [Google Scholar] [CrossRef]
- Spranger, J.; Kroke, A.; Möhlig, M.; Hoffmann, K.; Bergmann, M.M.; Ristow, M.; Boeing, H.; Pfeiffer, A.F.H. Inflammatory cytokines and the risk to develop type 2 diabetes: Results of the prospective population-based European prospective investigation into Cancer and nutrition (EPIC)-Potsdam study. Diabetes 2003, 52, 812–817. [Google Scholar] [CrossRef] [Green Version]
- Donath, M.Y.; Shoelson, S.E. Type 2 diabetes as an inflammatory disease. Nat. Rev. Immunol. 2011, 11, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Das, U.N. Colchicine in diabetes mellitus. J. Assoc. Phys. India 1993, 41, 213. [Google Scholar]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in patients with chronic coronary disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.Y.; Chen, Y.J.; Ho, H.J.; Hsu, Y.C.; Kuo, K.N.; Wu, M.S.; Lin, J.T. Association between nucleoside analogues and risk of hepatitis B virus-related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, M.N.; Wang, S.M.; Chen, P.C.; Chen, Y.Y.; Wang, J.D. Population-based case-control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J. Natl. Cancer Inst. 2010, 102, 179–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.L.; Kao, Y.H.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef]
- Kao, W.H.; Hong, J.H.; See, L.C.; Yu, H.P.; Hsu, J.T.; Chou, I.J.; Chou, W.C.; Chiou, M.J.; Wang, C.C.; Kuo, C.F. Validity of cancer diagnosis in the National Health Insurance database compared with the linked National Cancer Registry in Taiwan. Pharmacoepidemiol. Drug Saf. 2018, 27, 1060–1066. [Google Scholar] [CrossRef]
- Gau, C.S.; Chang, I.S.; Lin Wu, F.L.; Yu, H.; Huang, Y.W.; Chi, C.L.; Chien, S.Y.; Lin, K.M.; Liu, M.Y.; Wang, H.P. Usage of the claim database of national health insurance—Programme for analysis of cisapride-erythromycin co-medication in Taiwan. Pharmacoepidemiol. Drug Saf. 2007, 16, 86–95. [Google Scholar] [CrossRef]
- Gill, R.; Schumacher, M. A simple test of the proportional hazards assumption. Biometrika 1987, 74, 289–300. [Google Scholar] [CrossRef]
- Petersen, K.F.; Dufour, S.; Befroy, D.; Garcia, R.; Shulman, G.I. Impaired mitochondrial activity in the insulin-resistant offspring of patients with type 2 diabetes. N. Engl. J. Med. 2004, 350, 664–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, B.B.; Schmidt, M.I.; Pankow, J.S.; Ballantyne, C.M.; Couper, D.; Vigo, A.; Hoogeveen, R.; Folsom, A.R.; Heiss, G.; Atherosclerosis Risk in Communities Study. Low-grade systemic inflammation and the development of type 2 diabetes: The atherosclerosis risk in communities study. Diabetes 2003, 52, 1799–1805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luc, K.; Schramm-Luc, A.; Guzik, T.J.; Mikolajczyk, T.P. Oxidative stress and inflammatory markers in prediabetes and diabetes. J. Physiol. Pharmacol. 2019, 70, 809–824. [Google Scholar]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Osanik, T.; Golawski, M.; Lewandowski, P.; Pawlas, N. “Obesity and insulin resistance” is the component of the metabolic syndrome most strongly associated with stress. Antioxidants 2022, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; McGee, D.L. Diabetes and cardiovascular disease. JAMA 1979, 241, 2035–2038. [Google Scholar] [CrossRef]
- Grundy, S.M.; Benjamin, I.J.; Burke, G.L.; Chait, A.; Eckel, R.H.; Howard, B.V.; Mitch, W.; Smith, S.C., Jr.; Sowers, J.R. Diabetes and cardiovascular disease: A statement for health professionals from the American Heart Association. Circulation 1999, 100, 1134–1146. [Google Scholar] [CrossRef] [Green Version]
- Jakubiak, G.K.; Pawlas, N.; Cieslar, G.; Stanke, A. Pathogenesis and clinical significance of in-stent restenosis in patients with diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Andreu, J.M.; Timasheff, S.N. Interaction of tubulin with single ring analogue of colchicine. Biochemistry 1982, 21, 534–543. [Google Scholar] [CrossRef]
- Niggli, V. Signaling to migration in neutrophils: Importance of localized pathways. Int. J. Biochem. Cell. Biol. 2003, 35, 1619–1638. [Google Scholar] [CrossRef]
- Kamanli, A.; Nazıroglu, M.; Aydilek, N.; Hacievliyagil, C. Plasma lipid peroxidation and antioxidant levels in patients with rheumatoid arthritis. Cell Biochem. Funct. 2004, 22, 53–57. [Google Scholar] [CrossRef]
- Sahin, M.; Uguz, A.C.; Demirkan, H.; Naziroglu, M. Colchicine modulates oxidative stress in serum and leucocytes from remission patients with family Mediterranean fever through regulation of Ca2+ release and the antioxidant system. J. Membrane Biol. 2011, 240, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Zălar, D.M.; Pop, C.; Buzdugan, E.; Kiss, B.; Stefan, M.G.; Ghibu, S.; Crisan, D.; Buruiană-Simic, A.; Grozav, A.; Borda, H.M.; et al. Effects of colchicine in a rat model of diet-induced hyperlipidemia. Antioxidants 2022, 11, 230. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Sawhney, M.; Zhao, Y.; Carpio, G.R.; Fonseca, V.; Shi, L. Association between colchicine and risk of diabetes among the veterans affairs population with gout. Clin. Ther. 2015, 37, 1206–1215. [Google Scholar] [CrossRef] [PubMed]
- Demidowich, A.P.; Levine, J.A.; Onyekaba, G.I.; Khan, S.M.; Chen, K.Y.; Brady, S.M.; Broadney, M.M.; Yanovski, J.A. Effects of colchicine in adults with metabolic syndrome: A pilot randomized controlled trial. Diabetes Obes. Metab. 2019, 21, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Hyman, J. The limitations of using insurance data for research. J. Am. Dent. Assoc. 2015, 146, 283–285. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Without Colchicine (n = 7682) | With Colchicine (n = 3841) | p Value |
|---|---|---|---|
| Age (years) | 1.000 | ||
| 50–59 | 2432 (31.7%) | 1216 (31.7%) | |
| 60–69 | 2340 (30.5%) | 1170 (30.5%) | |
| ≥70 | 2910 (37.9%) | 1455 (37.9%) | |
| Sex | |||
| Female | 1168 (15.2%) | 584 (15.2%) | 1.000 |
| Male | 6514 (84.8%) | 3257 (84.8%) | |
| Comorbidities | |||
| Heart failure | 572 (7.4%) | 387 (10.1%) | <0.001 |
| Chronic liver disease | 1633 (21.3%) | 713 (18.6%) | <0.001 |
| Chronic kidney disease | 539 (7.0%) | 573 (14.9%) | <0.001 |
| Hyperlipidemia | 1789 (23.3%) | 787 (20.5%) | 0.001 |
| Hypertension | 4993 (65.0%) | 2639 (68.7%) | <0.001 |
| Ischemic heart disease | 2475 (32.2%) | 1289 (33.6%) | 0.148 |
| NAFLD | 214 (2.8%) | 106 (2.8%) | 0.936 |
| COPD | 2076 (27.0%) | 1030 (26.8%) | 0.812 |
| Co-medications | |||
| NSAIDs | 4742 (61.7%) | 1892 (49.3%) | <0.001 |
| Corticosteroids | 1353 (17.6%) | 516 (13.4%) | <0.001 |
| Allopurinol | 503 (6.5%) | 646 (16.8%) | <0.001 |
| Benzbromarone | 780 (10.2%) | 686 (17.9%) | <0.001 |
| Sulfinpyrazone | 60 (0.8%) | 54 (1.4%) | 0.001 |
| Diuretics | 2901 (37.8%) | 1836 (47.8%) | <0.001 |
| Beta-blockers | 4455 (58.0%) | 2409 (62.7%) | <0.001 |
| Calcium channel blockers | 2382 (31.0%) | 1464 (38.1%) | <0.001 |
| Statins | 2346 (30.5%) | 1334 (34.7%) | <0.001 |
| Variable | No. of Subjects | No. of DM Cases | Cumulative Incidence (%) | Adjusted HR (95% CI) |
|---|---|---|---|---|
| Overall | ||||
| Without Colchicine | 7682 | 1919 | 25.0 | 1.00 |
| With Colchicine | 3841 | 724 | 18.8 | 0.74 (0.36–0.87) |
| Variable | No. of Subjects | No. of DM Cases | Cumulative Incidence (%) | Adjusted HR (95% CI) |
|---|---|---|---|---|
| Gender | ||||
| Males | ||||
| Without colchicine | 6514 | 1535 | 23.6 | 1.00 |
| With colchicine | 3257 | 564 | 17.3 | 0.72 (0.32–1.18) |
| Females | ||||
| Without colchicine | 1168 | 384 | 32.9 | 1.00 |
| With colchicine | 584 | 160 | 27.4 | 0.81 (0.23–0.96) |
| Age | ||||
| 50–64 | ||||
| Without colchicine | 3581 | 1069 | 29.9 | 1.00 |
| With colchicine | 1789 | 374 | 20.9 | 0.76 (0.23–1.12) |
| ≥65 | ||||
| Without colchicine | 4101 | 850 | 20.7 | 1.00 |
| With colchicine | 2052 | 350 | 17.0 | 0.82 (0.31–0.92) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, C.-C.; Chen, Y.-C.; Lin, M.-H.; Wu, W.-T.; Liu, F.-C.; Chen, H.-C.; Chou, Y.-C.; Sun, C.-A. Association between Clinical Use of Colchicine and Risk of Type 2 Diabetes Mellitus among Gouty Patients: A Nationwide Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 3395. https://doi.org/10.3390/ijerph19063395
Chu C-C, Chen Y-C, Lin M-H, Wu W-T, Liu F-C, Chen H-C, Chou Y-C, Sun C-A. Association between Clinical Use of Colchicine and Risk of Type 2 Diabetes Mellitus among Gouty Patients: A Nationwide Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3395. https://doi.org/10.3390/ijerph19063395
Chicago/Turabian StyleChu, Chen-Chih, Yong-Chen Chen, Ming-Hsun Lin, Wen-Tung Wu, Feng-Cheng Liu, Hsiang-Cheng Chen, Yu-Ching Chou, and Chien-An Sun. 2022. "Association between Clinical Use of Colchicine and Risk of Type 2 Diabetes Mellitus among Gouty Patients: A Nationwide Cohort Study" International Journal of Environmental Research and Public Health 19, no. 6: 3395. https://doi.org/10.3390/ijerph19063395