1. Introduction
Adolescence is considered as a transition process from childhood to adulthood. It is a stage of life in which major changes take place over a short period of time [
1]. This process consists of three interrelated levels [
2]: biological (puberty), psychological, and social. The changes are a consequence of the developmental mechanisms and cultural demands of a specific social context, which includes defining dimensions such as social values. Due to the need to quickly adapt to these changes, various psychopathological symptoms often occur that directly affect the well-being and functioning of adolescents [
3,
4,
5]. Numerous studies have shown that 32% of the child and adolescent population suffer from some kind of anxiety disorder generated by the presence of a stressor, such as lack of self-confidence, low self-esteem, or frustration due to poor academic performance [
6,
7,
8,
9,
10]. These studies suggest that between 30% and 50% of these cases are associated to another type of disorder, such as aggressive behaviour, eating disorders, obsessive compulsive disorder, etc. [
11,
12,
13,
14]. In addition, 80% of adolescents suffering from these conditions do not receive any treatment or professional care [
15].
In many cases, these symptoms are linked to the inability of individuals to recognise their emotions or to inadequate emotion regulation [
16]. Emotions are an essential aspect of daily life and can promote or impair a person’s health and play a significant role in different cognitive processes. Therefore, the capacity to regulate or modulate emotional states is key to maintaining good mental health [
17]. Emotion regulation is defined as the use of mechanisms, skills, and strategies with the goal of maintaining, increasing, or suppressing an existing emotional state [
18]. Emotion regulation implies being aware of the state of one’s emotions and using strategies to manage mood [
19,
20]. Different studies have demonstrated that when people are unable to effectively regulate their emotions, distress may persist over time and may lead to different psychopathological symptoms and health problems in general [
21,
22,
23,
24]. Furthermore, gender has also been considered in many studies; females tend to present higher anxiety-related symptoms and a wider variety of mental disorders than males [
6,
21,
25,
26,
27,
28,
29].
The growing scientific interest in the personal and interpersonal processes and skills that facilitate emotion regulation has been highlighted by the increase in publications on these topics over the last 30 years [
30,
31,
32]. A key factor for research in this area is the availability of instruments that allow accurate assessment of the emotion regulation mechanisms.
One of the most commonly used models for understanding emotion regulation processes is that of Garnefski et al. [
19], which states that emotions evoked by a negative event can be regulated by cognitive processing. Thus, the model postulates that people can use nine emotion regulation strategies:
Blaming others (blaming another person for the occurrence of negative incidents or events),
Self-blame (blaming oneself for the experience),
Rumination (systematically thinking about the feelings and thoughts associated with the negative event),
Catastrophizing (explicitly emphasising the terror of what you have experienced),
Putting into perspective (pushing aside the severity of the event in comparison to other events),
Positive reappraisal (creating a positive appraisal of the event in terms of personal growth),
Refocus on planning (thinking about what steps to take and how to handle the negative event),
Positive refocusing (thinking about joyful and pleasant issues instead of thinking about the actual event), and
Acceptance (accepting what you experienced and resigning yourself to what has happened).
In addition, these strategies have frequently been classified into two dimensions: adaptive cognitive strategies of emotion regulation (Putting into Perspective, Acceptance, Positive Refocusing, Positive Reappraisal, and Refocus on Planning) and maladaptive cognitive strategies of emotion regulation (Rumination, Catastrophizing, Self-blame, and Blaming others).
To evaluate these nine strategies, Garnefski et al. [
19] proposed the Cognitive Emotion Regulation Questionnaire (CERQ), which is the first and only emotion regulation assessment instrument that separates cognitive regulation strategies from behavioural strategies [
33]. It is one of the most widely used instruments for the assessment of emotion regulation and has shown its usefulness in different fields, such as clinical [
34] or educational [
35,
36]. For example, Giménez et al. [
34] indicate that poor use of emotion regulation strategies is associated with greater perceived distress and the possibility of developing psychopathological symptoms. In this sense, the CERQ is a suitable instrument to study cognitive emotion regulation strategies and to understand their influence on subjective well-being and mental health.
The CERQ is a self-report instrument consisting of 36 items distributed according to the nine strategies of the model (four items for each dimension). Garnefski et al. [
19] reported that the nine factors together explained 64.6% of the variance with communalities ranging between 0.46 and 0.73. Subsequent studies confirmed the nine-dimensional structure [
37,
38] and verified the validity and reliability of the scale in different populations [
39,
40]. The instrument was also adapted in different countries such as France [
41], China [
42], and Spain [
43], where the nine-dimensional model showed a good fit to the data. The internal consistency indices (Cronbach’s alpha) found in these and other investigations [
44] typically range between 0.60 and 0.90 points.
However, some studies show discrepancies with these results. For example, McKinnon et al. [
45] reported that a five-factor model provided the best fit in an adult clinical population. In relation to the Spanish population, Carvajal et al. [
33] found that reducing the scale to 27 items improved model fit. Holgado-Tello et al. [
46] supported this 27-item version of the CERQ. Also in the Spanish population, Domínguez-Sánchez et al. [
43] reported that an alternative model integrating the nine dimensions into two second-order factors (adaptive and maladaptive strategies) showed appropriate global fit indices.
The CERQ has also been adapted for children [
37], and this adaptation has received a considerable interest in various studies, [
5,
47]. However, even though Garnefski et al. [
19] indicated that the CERQ is designed as a self-report questionnaire that can be administered from 12 years of age, its properties have not yet been sufficiently explored in the Spanish-speaking adolescent population. Given the importance of cognitive emotion regulation, the CERQ could constitute a conceptually sound instrument for assessing underlying cognitive coping processes in adolescence. Therefore, the main objective of this study is to provide new empirical evidence on the validity and reliability of the CERQ in a sample of Spanish adolescents.
3. Results
The results of the CFA allowed comparison of the goodness of fit of four alternative models: two with nine factors and two with two second-order factors and nine first-order factors, with 36 and 27 items respectively. The result was extremely favourable for model 3 with nine correlated factors and 27 items. As can be observed in
Table 1, the improvement in the fit of model 3 over the other models proved conclusive.
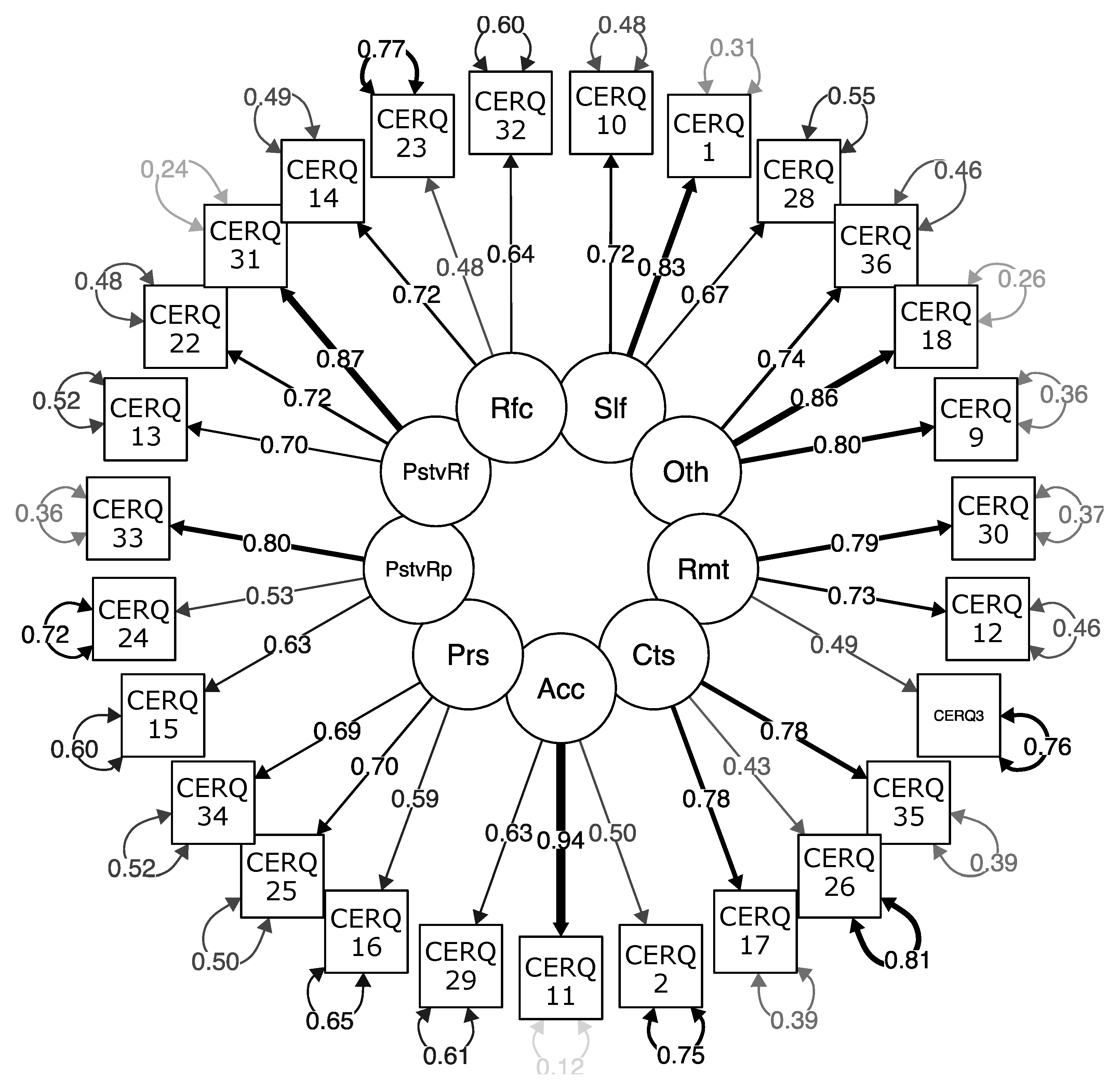
Figure 1 shows the graphical representation of the measurement model.
Global alpha ordinal reliability values [
60] of α = 0.83 and McDonald’s omega values [
61,
62] of ω = 0.82 were obtained. Both values are adequate. Good internal consistency indices were obtained for
adaptive strategies (α1 = 0.87; ω1 = 0.9) and for
maladaptive strategies (α2 = 0.82; ω2 = 0.89).
The composite reliability (CR) analysis of each latent variable provides an indicator of the reliability of the construct [
63]. In all cases, CR was higher than 0.70 (CR1 = 0.78; CR2 = 0.84; CR3 = 0.79; CR4 = 0.71; CR5 = 0.74; CR6 = 0.71; CR7 = 0.79; CR8 = 0.81; and CR9 = 0.74). Therefore, it can be concluded that the indicators of the nine factors are a reliable measurement of the construct. Average variance extracted (AVE) showed values higher than or extremely close to 0.5 in all cases (AVE1 = 0.55; AVE2 = 0.64, AVE3 = 0.47, AVE4 = 0.47, AVE5 = 0.51; AVE6 = 0.44, AVE7 = 0.44, AVE8 = 0.58, and AVE9 = 0.48). Thus, it can be concluded that a substantial amount of the variance of the indicators is explained by the construct compared with the error of the measurement. All these indicators constitute evidence of reliability in the operationalisation of the nine latent variables of the scale.
The reliability of each indicator can be checked using the R2 values, which indicate the proportion of variance of each indicator that explains the latent variable (high R2 values indicate that the indicator is reliable). The most reliable indicator for the acceptance factor was item 11 (I think that I have to accept the situation; R2 = 0.88). The most reliable indicator for the positive refocusing factor was item 31 (I think of pleasant things that have nothing to do with it; R2 = 0.757). The most reliable indicator for the positive reappraisal factor was item 31 I look for the positive sides to the matter (R2 = 0.639). The item 29 I feel that others are responsible for what has happened proved to be the most reliable indicator for the blaming others factor (R2 = 0.735). The item 1 I feel that I am the one to blame for it proved to be the most reliable indicator for the self-blame factor (R2 = 0.694).
Regarding convergent validity (e.g., the indicators of each latent variable have a high shared variance),
Table 2 and
Table 3 indicate that (a) the factor loadings of all of the indicators proved significant; (b) all but three indicators (
I often think about how I feel about what I have experienced—λ = 0.493;
I often think that what I have experienced is the worst that can happen to a person—λ = 0.435;
I think about how to change the situation—λ = 0.478) higher than 0.5; and (c) the AVE of the saturations of the items in each factor are all those which are higher or extremely close to 0.5.
The evidence of discriminant validity demonstrates that each of the constructs analysed is unique and different from other constructs. To test discriminant validity, four approaches were used [
53]. First, the correlation between each pair of factors was set to 1, and the fit of the resulting models was compared to the fit of the original model of nine correlated factors and 27 items. The results showed that this model was significantly superior to the models in which the correlation between each pair of factors was set to 1 (
Table A1). Second, the confidence interval test [
64] demonstrated that the confidence interval of the correlations between the factors does not contain 1 (
Table 4). Third, it was verified that the HTMT ratio [
65] of the correlations between the indicators of different factors (heterotrait-heteromethod correlations–HT) and between the correlations of the indicators of the same factor (monotrait-heteromethod correlations–MT) is less than 0.9 (F1–F2, HT/MT = 0.771; F1–F3, HT/MT = 0.693; F2–F3, HT/MT = 0.835).
Fourth, Fornell and Larcker’s criterion [
63] states that AVE from each factor higher than the square of the correlations between each pair of factors can be considered as evidence of discriminant validity. This criterion is fulfilled in all but two cases (
Table 5). Specifically, AVE of factors 6 (Perspective, AVE = 0.444) and 7 (Reappraisal, AVE = 0.440) was lower than the coefficient of determination between them both (ρ2 = 0.513). Likewise, AVE of factors 7 (Reappraisal, AVE = 0.440) and 9 (Planning, AVE = 0.482) was lower than the coefficient of determination between them both (ρ2 = 0.673).
4. Discussion
The main objective of this study is to provide new empirical evidence on the validity and reliability of the CERQ [
19,
31] in a sample of Spanish adolescents. The CERQ is an emotion regulation assessment tool that allows discrimination between cognitive and behavioural strategies [
33]. Prior studies have shown empirical evidence of the psychometric properties of the CERQ in the Spanish population [
32,
33,
43,
46,
66,
67]. However, less attention has been paid to its properties in the adolescent population. For this reason, the psychometric properties of the CERQ were analysed in a sample of students from the city of Valladolid (Spain).
According to some proposals in the literature, four models were estimated through CFA. The results obtained suggest the reduction of the scale to 27 items (model 3) distributed in nine factors (strategies). The nine-dimensional structure coincides with that originally proposed by Garnefski et al. [
19]. However, the number of items suggested in the results differs from the original instrument and rather supports the proposal of Carvajal et al. [
33]. In this sense, these authors recommend adapting the Spanish version to a shorter version called CERQ-S-27 and another even shorter version of 18 factors (ERQ-short), which has already been validated in other countries [
38,
48,
50,
68,
69,
70,
71,
72]. Given that the sample used in the present study is also Spanish, it is reasonable that the results regarding the number of items are more similar to previous studies carried out in this country.
Regarding the grouping into functional/adaptive and dysfunctional/maladaptive strategies, the results suggest the importance of maintaining the multidimensionality of the CERQ. Thus, it is recommended not to merge the scores of the different strategies as reported in other studies [
36,
39,
49]. However, the fit of model 4 (27 items with two second-order factors and nine first-order factors) has also demonstrated appropriate global fit indices which should be considered in future research. Although it is better to address the scales separately, using them as a whole may have interesting implications in certain specific contexts, as already pointed out by Domínguez-Sánchez et al. [
43] and D’Augerot et al. [
36].
The results suggest that the nine subscales of the CERQ present adequate internal consistency, sufficient reliability and adequate construct reliability. Furthermore, sufficient evidence of convergent validity and discriminant validity was obtained. However, discriminant validity points to the possible convenience of merging some factors (Perspective-Appraisal-Planning), but this would require a much larger sample and a theory to support this hypothesis.
In short, these results confirm the need for further research on the dimensionality of the CERQ and cognitive emotion regulation strategies. Psychometric properties were generally similar to those of the original Spanish adaptation, confirming the validity of the short 27-item version. This conclusion has been reached not only in studies with national sampling, but also in other international research, such as the Italian [
73] or German [
74] adaptations.
Finally, the results of the present study should be interpreted in light of certain limitations. First, the sample was non-probabilistic, limiting the generalizability of the results. It would be of great interest to employ a random sampling method to be able to generalise the results. Second, the exclusive use of self-report methods also imply the possibility of assessment bias [
75]. Third, because there are few studies on the CERQ functioning in adolescent populations, comparison of the findings was limited. Finally, although the number of participants was sufficient to perform the CFA and achieve the objective of the study, a larger sample would improve the accuracy of the results and give them greater scope. Moreover, a larger number of participants would enable additional analyses such as a gender factorial invariance analysis. As females tend to present a higher prevalence of anxiety-related symptoms and a wider variety of mental disorders than males [
6,
21,
25,
26,
27,
28,
29,
34,
35], examining validity and reliability of the CERQ across gender would be of great interest. It is expected that future studies may address this limitation.





{kind=link}
