
No Excess Mortality up to 10 Years in Early Stages of Breast Cancer in Women Adherent to Oral Endocrine Therapy: A Probabilistic Graphical Modeling Approach

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data: BCStage Dataset
2.2. Synthetic Data Simulation
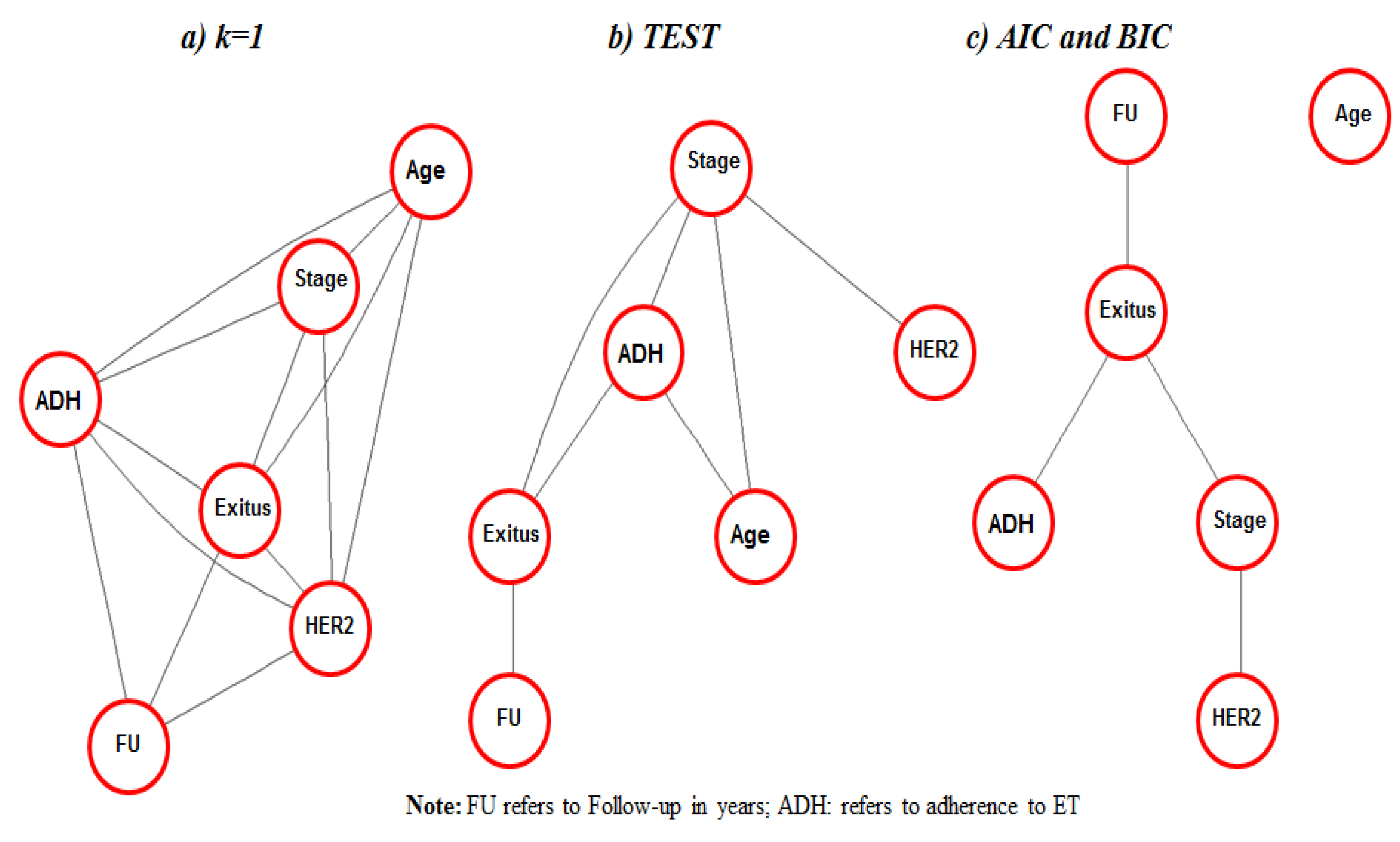
2.2.1. Fitting Graphical Models through ModGraProDep
2.2.2. ComSynSurData: Combining Synthetic Survival Datasets
- Step 0.
- Use ModGraProDep for generating the four SynDs.
- Step 1.
- Produce a partition of the cohort dataset into L subsets according to A age groups and S levels of a stratification variable, such as stage at diagnosis; then, L = A × S. For instance, if strata were stage at diagnosis with levels {I, II, III}, and three age groups were considered, then L = 3 × 3 = 9 subsets (one for each age group and stage combination). In the same line, the same partition is made for each SynD.
- Step 2.
- For each of the L subsets of the cohort data, find its “best” counterpart among the 4 × 9 = 36 subsets of SynDs by comparing survival estimates between the observed cohort and that derived from the SynDs through a scoring method.
- Step 3.
- Once L subsets of SynD are selected in each age stratum, generate a combined synthetic cohort by merging these L subsets, from which Kaplan–Meier survival estimates according to stage and corresponding age groups can be derived.
2.2.3. Scoring Method for Comparing Observed versus Predicted Survival in Step 2
2.3. Statistical Modeling of Excess Mortality
2.4. Analysis Scheme
3. Results
3.1. Data Simulation
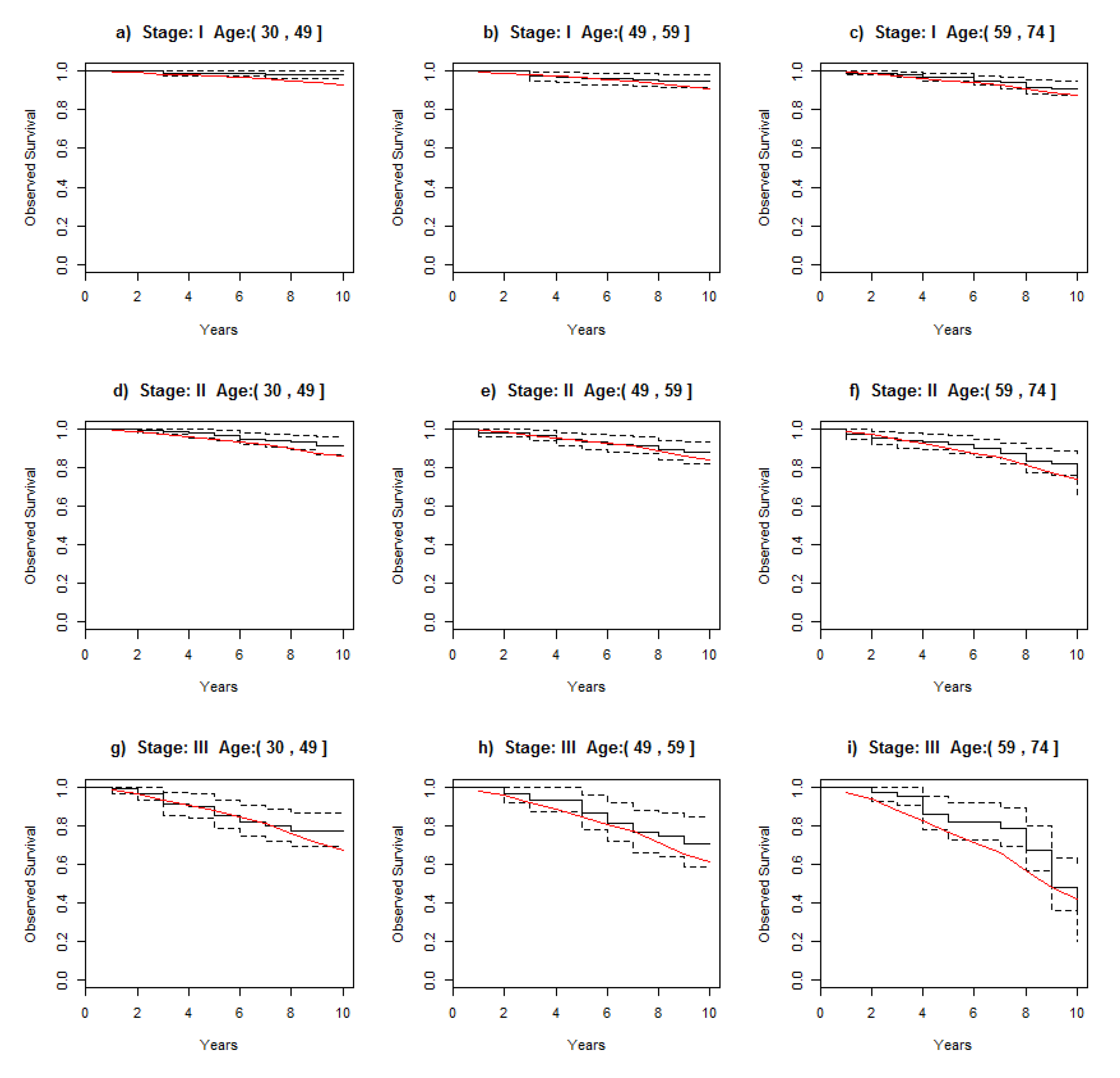
3.2. Comparing Observed Survival in the Cohort with Survival in the Combined Cohort
3.3. Survival Indicators Derived from Combined Dataset
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chirlaque, M.D.; Salmerón, D.; Galceran, J.; Ameijide, A.; Mateos, A.; Torrella, A.; Jiménez, R.; Larrañaga, N.; Marcos-Gragera, R.; Ardanaz, E.; et al. Cancer survival in adult patients in Spain. Results from nine population-based cancer registries. Clin. Transl. Oncol. 2018, 20, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Clèries, R.; Ameijide, A.; Buxó, M.; Martínez, J.M.; Marcos-Gragera, R.; Vilardell, M.-L.; Carulla, M.; Yasui, Y.; Vilardell, M.; Espinàs, J.A.; et al. Long-term crude probabilities of death among breast cancer patients by age and stage: A population-based survival study in Northeastern Spain (Girona–Tarragona 1985–2004). Clin. Transl. Oncol. 2018, 20, 1252–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hieke, S.; Kleber, M.; König, C.; Engelhardt, M.; Schumacher, M. Conditional Survival: A Useful Concept to Provide Information on How Prognosis Evolves over Time. Clin. Cancer Res. 2015, 21, 1530–1536. [Google Scholar] [CrossRef] [Green Version]
- Shack, L.; Bryant, H.; Lockwood, G.; Ellison, L.F. Conditional relative survival: A different perspective to measuring cancer outcomes. Cancer Epidemiol. 2013, 37, 446–448. [Google Scholar] [CrossRef]
- Cronin, K.A.; Feuer, E.J. Cumulative cause-specific mortality for cancer patients in the presence of other causes: A crude analogue of relative survival. Stat. Med. 2000, 19, 1729–1740. [Google Scholar] [CrossRef]
- He, V.Y.F.; Condon, J.R.; Baade, P.D.; Zhang, X.; Zhao, Y. Different survival analysis methods for measuring long-term outcomes of Indigenous and non-Indigenous Australian cancer patients in the presence and absence of competing risks. Popul. Health Metr. 2017, 15, 1. [Google Scholar] [CrossRef] [Green Version]
- Maso, L.D.; Guzzinati, S.; Buzzoni, C.; Capocaccia, R.; Serraino, D.; Caldarella, A.; Tos, A.P.D.; Falcini, F.; Autelitano, M.; Masanotti, G.; et al. Long-term survival, prevalence, and cure of cancer: A population-based estimation for 818,902 Italian patients and 26 cancer types. Ann. Oncol. 2014, 25, 2251–2260. [Google Scholar] [CrossRef]
- Maso, L.D.; Panato, C.; Tavilla, A.; Guzzinati, S.; Serraino, D.; Mallone, S.; Botta, L.; Boussari, O.; Capocaccia, R.; Colonna, M.; et al. Cancer cure for 32 cancer types: Results from the EUROCARE-5 study. Int. J. Epidemiol. 2020, 49, 1517–1525. [Google Scholar] [CrossRef]
- Freedman, R.A.; Keating, N.L.; Lin, N.U.; Winer, E.P.; Vaz-Luis, I.; Lii, J.; Exman, P.; Barry, W.T. Breast cancer-specific survival by age: Worse outcomes for the oldest patients. Cancer 2018, 124, 2184–2191. [Google Scholar] [CrossRef] [Green Version]
- Munzone, E.; Colleoni, M. Optimal management of luminal breast cancer: How much endocrine therapy is long enough? Ther. Adv. Med. Oncol. 2018, 10, 1758835918777437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Font, R.; Alfons, J.; Agustí, E.; Angel, B.; Jaume, I.; Saladie, F. Influence of adherence to adjuvant endocrine therapy on disease-free and overall survival: A population-based study in Catalonia, Spain. Breast Cancer Res. Treat. 2019, 175, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Vilardell, M.; Buxó, M.; Clèries, R.; Martínez, J.M.; Garcia, G.; Ameijide, A.; Font, R.; Civit, S.; Marcos-Gragera, R.; Vilardell, M.L.; et al. Missing data imputation and synthetic data simulation through modeling graphical probabilistic dependencies between variables (ModGraProDep): An application to breast cancer survival. Artif. Intell. Med. 2020, 107, 101875. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Generating survival times to simulate Cox proportional hazards models with time-varying covariates. Stat. Med. 2012, 31, 3946–3958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, C.; Thompson, S.G. The importance of varying the event generation process in simulation studies of statistical methods for recurrent events. Stat. Med. 2006, 25, 165–179. [Google Scholar] [CrossRef]
- Moriña, D.; Navarro, A. The R Package survsim for the Simulation of Simple and Complex Survival Data. J. Stat. Soft. 2014, 59, 1–20. Available online: https://www.jstatsoft.org/index.php/jss/article/view/v059i02 (accessed on 18 January 2022). [CrossRef] [Green Version]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. {SMOTE}: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Han, H.; Wang, W.; Mao, B. Borderline-SMOTE: A New Over-Advances in Intelligent Computing. In Proceedings of the International Conference on Intelligent Computing, ICIC 2005, Hefei, China, 23–26 August 2005; Lecture Notes in Computer Science, Sampling Method in Imbalanced Data Sets Learning. Huang, D.S., Zhang, X.P., Huang, G.B., Eds.; Springer: Berlin, Germany, 2005; Volume 3644. [Google Scholar] [CrossRef]
- Barua, S.; Islam, M.M.; Yao, X.; Murase, K. MWMOTE—Majority weighted minority oversampling technique for imbalanced data set learning. IEEE Trans. Knowl. Data Eng. 2014, 26, 405–425. [Google Scholar] [CrossRef]
- Pearl, J. Probabilistic Reasoning in Intelligent Systems: Networks of Plausible Inference; Morgan-Kauffman Publishers: Los Altos, CA, USA, 1988. [Google Scholar] [CrossRef]
- Lauritzen, S.L.; Spiegelhalter, D.J. Local computations with probabilities on graphical structures and their application to expert systems (with discussion). Ann. Math. Artif. Intell. 1988, 50, 157–224. [Google Scholar] [CrossRef]
- Højsgaard, S.; Edwards, D.; Lauritzen, S. Graphical Models with R.; Springer: New York, NY, USA; Dordrecht, The Netherlands; Heidelberg, Germany; London, UK, 2012. [Google Scholar]
- Ameijide, A.; Clèries, R.; Carulla, M.; Buxó, M.; Marcos-Gragera, R.; Martínez, J.M.; Vilardell, M.L.; Espinàs, J.A.; Borras, J.M.; Izquierdo, Á.; et al. Cause-specific mortality after a breast cancer diagnosis: A cohort study of 10,195 women in Girona and Tarragona. Clin. Transl. Oncol. 2019, 21, 1014–1025. [Google Scholar] [CrossRef] [Green Version]
- Singletary, S.E.; Connolly, J.L. Breast cancer staging: Working with the sixth edition of the AJCC Cancer Staging Manual. CA Cancer J. Clin. 2006, 56, 37–47, Quiz 50, 51. [Google Scholar] [CrossRef] [PubMed]
- Højsgaard, S. Graphical Independence Networks with the gRain Package for R. J. Stat. Soft. 2012, 46, 1–26. Available online: https://www.jstatsoft.org/index.php/jss/article/view/v046i10 (accessed on 18 January 2022).
- Graf, E.; Schmoor, C.; Sauerbrei, W.; Schumacher, M. Assessment and comparison of prognostic classification schemes for survival data. Stat. Med. 1999, 18, 2529–2545. [Google Scholar] [CrossRef]
- Haider, H.; Hoehn, B.; Davis, S.; Greiner, R. Effective ways to build and evaluate individual survival distributions. J. Mach. Learn. Res. 2020, 21, 1–63. [Google Scholar]
- Pohar Perme, M.; Estève, J.; Rachet, B. Analysing population-based cancer survival—Settling the controversies. BMC Cancer 2016, 16, 933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seppä, K.; Hakulinen, T.; Läärä, E.; Pitkäniemi, J. Comparing net survival estimators of cancer patients. Stat. Med. 2016, 35, 1866–1879. [Google Scholar] [CrossRef]
- Clèries, R.; Buxó, M.; Yasui, Y.; Marcos-Gragera, R.; Martinez, J.M.; Ameijide, A.; Galceran, J.; Borras, J.M.; Izquierdo, Á. Estimating long-term crude probability of death among young breast cancer patients: A Bayesian approach. Tumori 2016, 102, 555–561. [Google Scholar] [CrossRef] [Green Version]
- Lunn, D.J.; Thomas, A.; Best, N.; Spiegelhalter, D. WinBUGS—A Bayesian modelling framework: Concepts, structure, and extensibility. Stat. Comput. 2000, 10, 325–337. [Google Scholar] [CrossRef]
- Sturtz, S.; Ligges, U.; Gelman, A. R2WinBUGS: A Package for Running WinBUGS from R. J. Stat. Soft. 2005, 12, 1–16. Available online: https://www.jstatsoft.org/index.php/jss/article/view/v012i03 (accessed on 18 January 2022). [CrossRef] [Green Version]
- Wang, S.; Liu, Y.; Feng, Y.; Zhang, J.; Swinnen, J.; Li, Y.; Ni, Y. A review on curability of cancers: More efforts for novel therapeutic options are needed. Cancers 2019, 11, 1782. [Google Scholar] [CrossRef] [Green Version]
- Mariotto, A.B.; Noone, A.-M.; Howlader, N.; Cho, H.; Keel, G.E.; Garshell, J.; Woloshin, S.; Schwartz, L.M. Cancer survival: An overview of measures, uses, and interpretation. J. Natl. Cancer Inst. Monogr. 2014, 2014, 145–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.; Abraham, J.H.; Rhodes, L.; Roberts, R. Use of the word “cure” in oncology. J. Oncol. Pract. 2013, 9, e136–e140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariotto, A.B.; Zou, Z.; Zhang, F.; Howlader, N.; Kurian, A.W.; Etzioni, R. Can we use survival data from cancer registries to learn about disease recurrence? The case of breast cancer. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1332–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Maaren, M.C.; Strobbe, L.J.A.; Smidt, M.L.; Moossdorff, M.; Poortmans, P.M.P.; Siesling, S. Ten-year conditional recurrence risks and overall and relative survival for breast cancer patients in the Netherlands: Taking account of event-free years. Eur. J. Cancer 2018, 102, 82–94. [Google Scholar] [CrossRef]
- Van Maaren, M.C.; De Munck, L.; Strobbe, L.J.; Sonke, G.; Westenend, P.; Smidt, M.L.; Poortmans, P.M.; Siesling, S. Ten-year recurrence rates for breast cancer subtypes in the Netherlands: A large population-based study. Int. J. Cancer 2018, 144, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Männle, H.; Siebers, J.W.; Momm, F.; Münstedt, K. Impact of patients’ refusal to undergo adjuvant treatment measures on survival. Breast Cancer Res. Treat. 2020, 185, 239–246. [Google Scholar] [CrossRef]
- Roca-Barceló, A.; Viñas, G.; Pla, H.; Carbó, A.; Comas, R.; Izquierdo, Á.; Pinheiro, P.S.; Vilardell, L.; Solans, M.; Marcos-Gragera, R. Mortality of women with ductal carcinoma in situ of the breast: A population-based study from the Girona province, Spain (1994–2013). Clin. Transl. Oncol. 2018, 21, 891–899. [Google Scholar] [CrossRef] [Green Version]
- Azim, H.H.A.; Michiels, S.; Bedard, P.; Singhal, S.K.; Criscitiello, C.; Ignatiadis, M.; Haibe-Kains, B.; Piccart-Gebhart, M.; Sotiriou, C.; Loi, S. Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin. Cancer Res. 2012, 18, 1341–1351. [Google Scholar] [CrossRef] [Green Version]
- He, X.M.; Zou, D.H. The association of young age with local recurrence in women with early-stage breast cancer after breast-conserving therapy: A meta-analysis. Sci. Rep. 2017, 7, 11058. [Google Scholar] [CrossRef]
- Johansson, A.L.V.; Trewin, C.B.; Hjerkind, K.V.; Ellingjord-Dale, M.; Johannesen, T.B.; Ursin, G. Breast cancer-specific survival by clinical subtype after 7 years follow-up of young and elderly women in a nationwide cohort. Int. J. Cancer 2019, 144, 1251–1261. [Google Scholar] [CrossRef]
- Johansson, A.L.V.; Trewin, C.B.; Fredriksson, I.; Reinertsen, K.V.; Russnes, H. In modern times, how important are breast cancer stage, grade and receptor subtype for survival: A population-based cohort study. Breast Cancer Res. 2021, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Sahli, Z.; Wang, Y.; Wolff, A.C.; Cope, L.M.; Umbricht, C.B. Young age at diagnosis is associated with worse prognosis in the Luminal A breast cancer subtype: A retrospective institutional cohort study. Breast Cancer Res. Treat. 2018, 172, 689–702. [Google Scholar] [CrossRef]
- Partridge, A.H.; Hughes, M.E.; Warner, E.T.; Ottesen, R.A.; Wong, Y.-N.; Edge, S.B.; Theriault, R.L.; Blayney, D.W.; Niland, J.C.; Winer, E.P.; et al. Subtype-dependent relationship between young age at diagnosis and breast cancer survival. J. Clin. Oncol. 2016, 34, 3308–3314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huiart, L.; Ferdynus, C.; Giorgi, R. A meta-regression analysis of the available data on adherence to adjuvant hormonal therapy in breast cancer: Summarizing the data for clinicians. Breast Cancer Res. Treat. 2013, 138, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Condorelli, R.; Vaz-Luis, I. Managing side effects in adjuvant endocrine therapy for breast cancer. Expert Rev. Anticancer Ther. 2018, 18, 1101–1112. [Google Scholar] [CrossRef]
- Francis, P.A.; Pagani, O.; Fleming, G.F.; Walley, B.A.; Colleoni, M.; Láng, I.; Gómez, H.L.; Tondini, C.A.; Ciruelos, E.; Burstein, H.J.; et al. Tailoring Adjuvant Endocrine Therapy for Premenopausal Breast Cancer. N. Engl. J. Med. 2018, 379, 122–137. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HER2− (N = 1736; 75.6%) | HER2+ (561; 24.4%) | Total (N = 2297; 100%) | ||
|---|---|---|---|---|
| Registry | Girona | 876 (50.5%) | 301 (53.6%) | 1176 (51.2%) |
| Tarragona | 860 (49.5%) | 260 (46.4%) | 1121 (48.8%) | |
| Age | Mean (SD) | 55.6 (10.6) | 54.3 (10.7) | 55.3 (10.6%) |
| ≤49 years | 556 (32.0%) | 196 (35.0%) | 751 (32.7%) | |
| 50–59 years | 502 (28.9%) | 178 (31.7%) | 680 (29.6%) | |
| 60–74 years | 678 (39.1%) | 187 (33.3%) | 866 (37.7%) | |
| Stage at diagnosis | I | 769 (44.3%) | 195 (34.7%) | 997 (43.4%) |
| II | 641 (36.9%) | 257 (45.9%) | 898 (39.1%) | |
| III | 326 (18.8%) | 109 (19.5%) | 402 (17.5%) | |
| Deceased (%) | 11.9 | 10.9 | 11.7 | |
| Follow-up in years, mean (SD) | 9.2 (1.7) | 9.3 (1.5) | 9.2 (1.6) | |
| Adherence to ET | No: ≤80% | 234 (13.4%; 24.9% b) | 75 (13.5%; 24.8% b) | 309 (13.5%; 24.9% b) |
| Yes: >80% | 706 (40.7%; 75.1% b) | 228 (40.6%; 75.2% b) | 934 (40.6%; 75.1% b) | |
| Total a | 940 (54.1%; 100.0% b) | 303 (54.0%; 100.0% b) | 1243 (54.1%; 100.0 b) | |
| Missing c | 796 (45.9%; - ) | 258 (45.9%; - ) | 1054 (45.9%; - ) | |
| Distribution of BC Cases in Cohort after Imputation of Adherence to ET when Missing | ||||
| Adherence to ET | HER2− (N = 1736; 75.6%) | HER2+ (N = 561; 24.4%) | Total (N = 2297; 100%) | |
| GMK1 d | No: ≤80% | 426 (24.5%) | 126 (22.4%) | 552 (24.0%) |
| Yes: >80% | 1310 (74.5%) | 435 (77.6%) | 1745 (76.0%) | |
| Total | 1736 (100.0%) | 561(100.0%) | 2297 (100.0%) | |
| GMAIC e | No: ≤80% | 420 (24.2%) | 120 (21.4%) | 540 (23.5%) |
| Yes: >80% | 1316 (74.8%) | 441 (78.6%) | 1745 (76.5%) | |
| Total | 1736 (100.0%) | 561(100.0%) | 2297 (100.0%) | |
| GMBIC f | No: ≤80% | 420 (24.2%) | 120 (21.4%) | 540 (23.5%) |
| Yes: >80% | 1316 (74.8%) | 441 (78.6%) | 1745 (76.5%) | |
| Total | 1736 (100.0%) | 561(100.0%) | 2297 (100.0%) | |
| GMTEST g | No: ≤80% | 424 (24.4%) | 121 (21.5%) | 545 (23.7%) |
| Yes: >80% | 1312 (74.6%) | 440 (78.5%) | 1752 (76.3%) | |
| Total | 1736 (100.0%) | 561(100.0%) | 2297 (100.0%) | |
| Synthetic Dataset | ||||
|---|---|---|---|---|
| Derived from GMk1 | Derived from GMTest | Derived from GMAIC | Derived from GMBIC | |
| Stage I | ||||
| ≤49 years | 0.0149 | 0.0146 | 0.0142 | 0.0143 |
| 50–59 years | 0.0432 | 0.0433 | 0.0433 | 0.0433 |
| 60–74 years | 0.0471 | 0.0485 | 0.0482 | 0.0482 |
| Stage II | ||||
| ≤49 years | 0.0484 | 0.0486 | 0.0485 | 0.0485 |
| 50–59 years | 0.0703 | 0.0707 | 0.0706 | 0.0706 |
| 60–74 years | 0.0943 | 0.0986 | 0.0982 | 0.0984 |
| Stage III | ||||
| ≤49 years | 0.1183 | 0.1188 | 0.1185 | 0.1185 |
| 50–59 years | 0.1437 | 0.1431 | 0.1427 | 0.1426 |
| 60–74 years | 0.1722 | 0.2020 | 0.1960 | 0.1965 |
| OS(5) (%) | OS(10) (%) | PCa(10) (%) | POC(10) (%) | EM(5) (%) | ||
|---|---|---|---|---|---|---|
| Adherent | N * | Me(95% CI) | Me(95% CI) | Me(95% CI) | Me(95% CI) | Me(95% CI) |
| Stage I | ||||||
| ≤49 years | 72,817 | 98.3 (98.2; 98.4) | 95.7 (95.5; 95.9) | 1.8 (1.6; 1.9) | 2.5 (2.5; 2.5) | 1.1 (1.0; 1.3) |
| 50–59 years | 92,526 | 98.4 (98.3; 98.5) | 96.0 (95.9; 96.2) | 0.2 (0.1; 0.3) | 3.8 (3.6; 3.9) | 0.0 (−0.1; 0.1) |
| 60–74 years | 167,001 | 97.3 (97.2; 97.3) | 92.9 (92.7; 93.1) | 0.2 (0.1; 0.3) | 6.9 (6.7; 7.1) | 0.0 (−0.1; 0.1) |
| Stage II | ||||||
| ≤49 years | 98,722 | 95.9 (95.7; 96.1) | 89.0 (88.8; 89.3) | 8.7 (8.4; 8.9) | 2.3 (2.0; 2.6) | 5.8 (5.5; 6.2) |
| 50–59 years | 92,612 | 96.5 (96.4; 96.6) | 90.6 (90.4; 90.9) | 3.4 (3.1; 3.6) | 6.0 (5.9; 6.1) | 2.3 (2.1; 2.6) |
| 60–74 years | 92,919 | 91.9 (91.7; 92.1) | 78.6 (78.3; 79.0) | 0.6 (0.4; 0.9) | 20.8 (20.3; 21.1) | 0.0 (−0.4; 0.4) |
| Stage III | ||||||
| ≤49 years | 40,968 | 87.8 (87.5; 88.1) | 69.6 (69.1; 70.1) | 27.9 (27.3; 28.4) | 2.5 (2.5; 2.6) | 19.7 (19.1; 20.2) |
| 50–59 years | 36,659 | 88.0 (87.7; 88.3) | 69.5 (68.9; 70.1) | 24.8 (24.2; 25.4) | 5.7 (5.7; 5.8) | 17.9 (17.3; 18.6) |
| 60–74 years | 41,335 | 78.8 (78.4; 79.2) | 47.3 (46.7; 47.9) | 28.1 (27.5; 28.8) | 24.6 (24.5; 24.7) | 25.4 (24.5; 26.3) |
| Overall | 735,559 | 94.5 (94.4; 94.6) | 85.7 (85.6; 85.8) | 0.9 (0.8; 1.0) | 13.5 (13.3; 13.6) | 0.5 (0.4; 0.7) |
| Nonadherent | ||||||
| Stage I | ||||||
| ≤49 years | 34,356 | 96.5 (96.3; 96.7) | 90.8 (90.4; 91.2) | 7.1 (6.7; 7.5) | 2.2 (2.2; 2.2) | 4.6 (4.3; 5.0) |
| 50–59 years | 29,888 | 92.8 (92.5; 93.1) | 81.5 (80.9; 82.0) | 13.1 (12.6; 13.7) | 5.4 (5.4; 5.4) | 9.0 (8.5; 9.6) |
| 60–74 years | 33,313 | 87.7 (87.3; 88.0) | 68.8 (68.2; 69.5) | 7.4 (6.8; 8.0) | 23.9 (23.2; 24.1) | 5.4 (4.6; 6.1) |
| Stage II | ||||||
| ≤49 years | 49,897 | 94.7 (94.5; 94.9) | 85.9 (85.5; 86.3) | 11.9 (11.5; 12.3) | 2.1 (2.1; 2.1) | 8.0 (7.6; 8.4) |
| 50–59 years | 28,269 | 87.2 (86.8; 87.6) | 66.6 (65.9; 67.4) | 28.0 (27.3; 28.7) | 5.3 (5.3; 5.4) | 20.8 (20.1; 21.6) |
| 60–74 years | 26,084 | 85.6 (85.2; 86.0) | 62.7 (61.9; 63.4) | 13.9 (13.0; 14.7) | 23.5 (23.4; 23.6) | 11.9 (10.9; 12.9) |
| Stage III | ||||||
| ≤49 years | 16,468 | 77.6 (77.0; 78.2) | 46.3 (45.3; 47.3) | 49.8 (48.9; 50.7) | 3.9 (3.8; 4.0) | 39.5 (38.3; 40.7) |
| 50–59 years | 14,953 | 78.0 (77.3; 78.6) | 46.5 (45.5; 47.5) | 47.0 (46.1; 47.9) | 6.5 (6.4; 6.6) | 38.0 (36.8; 39.3) |
| 60–74 years | 13,020 | 72.2 (71.4; 72.9) | 31.3 (30.2; 32.3) | 41.1 (40.1; 42.0) | 27.7 (27.4; 28) | 43.9 (42.1; 45.7) |
| Overall | 246,248 | 88.5 (88.4; 88.6) | 70.5 (70.3; 70.8) | 19.6 (19.4; 19.9) | 9.8 (9.6; 9.9) | 14.5 (14.3; 14.8) |
| Overall difference Adherent vs. nonadherent ** | 6.0 | 15.2 | −18.7 | 3.7 | −14.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clèries, R.; Buxó, M.; Vilardell, M.; Ameijide, A.; Martínez, J.M.; Font, R.; Marcos-Gragera, R.; Puigdemont, M.; Viñas, G.; Carulla, M.; et al. No Excess Mortality up to 10 Years in Early Stages of Breast Cancer in Women Adherent to Oral Endocrine Therapy: A Probabilistic Graphical Modeling Approach. Int. J. Environ. Res. Public Health 2022, 19, 3605. https://doi.org/10.3390/ijerph19063605
Clèries R, Buxó M, Vilardell M, Ameijide A, Martínez JM, Font R, Marcos-Gragera R, Puigdemont M, Viñas G, Carulla M, et al. No Excess Mortality up to 10 Years in Early Stages of Breast Cancer in Women Adherent to Oral Endocrine Therapy: A Probabilistic Graphical Modeling Approach. International Journal of Environmental Research and Public Health. 2022; 19(6):3605. https://doi.org/10.3390/ijerph19063605
Chicago/Turabian StyleClèries, Ramon, Maria Buxó, Mireia Vilardell, Alberto Ameijide, José Miguel Martínez, Rebeca Font, Rafael Marcos-Gragera, Montse Puigdemont, Gemma Viñas, Marià Carulla, and et al. 2022. "No Excess Mortality up to 10 Years in Early Stages of Breast Cancer in Women Adherent to Oral Endocrine Therapy: A Probabilistic Graphical Modeling Approach" International Journal of Environmental Research and Public Health 19, no. 6: 3605. https://doi.org/10.3390/ijerph19063605