
Can Rehabilitation in Nature Improve Self-Perceived Interpersonal Problems? A Matched-Control Study

 ,
,
Abstract
:1. Background
1.1. A Nature-Based Rehabilitation Program
1.2. Aim
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. The Intervention
The Wildman Programme
2.4. Treatment as Usual (TAU)
2.5. Outcome: Inventory of Interpersonal Problems (IIP)
2.6. Statistical Analysis
3. Results
3.1. Demographics
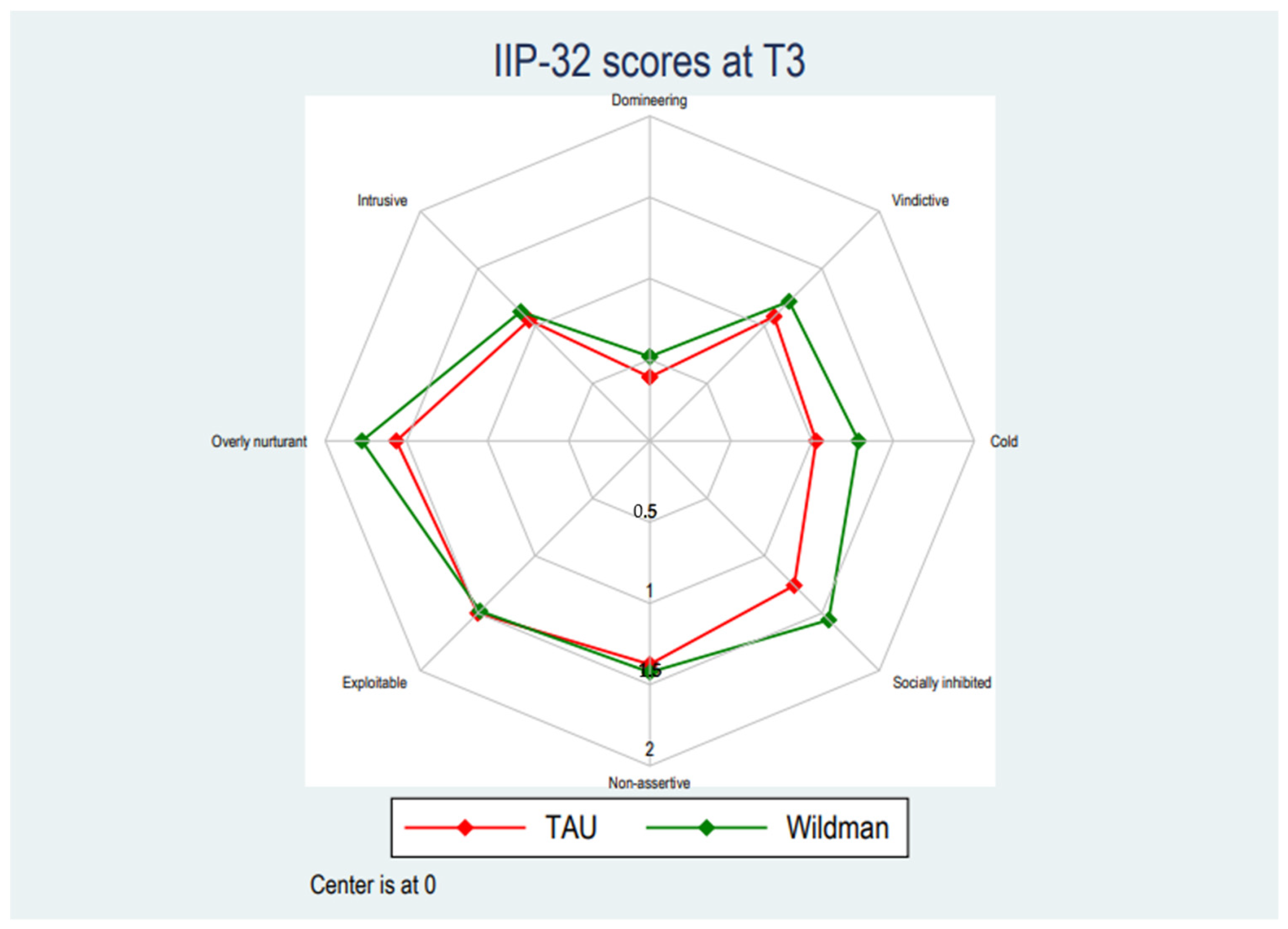
3.2. Effects of Intervention on Self-Perceived Interpersonal Problems
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grahn, P.; Stigsdotter, U.K. The relation between perceived sensory dimensions of urban green space and stress restoration. Landsc. Urban Plan. 2010, 94, 264–275. [Google Scholar] [CrossRef]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, R.; Kaplan, S. The Experience of Nature. A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Bratman, G.N.; Hamilton, J.P.; Daily, G.C. The impacts of nature experience on human cognitive function and mental health. Ann. N. Y. Acad. Sci. 2012, 1249, 118–136. [Google Scholar] [CrossRef]
- Berman, M.G.; Jonides, J.; Kaplan, S. The Cognitive Benefits of Interacting With Nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef]
- Cole, D.N.; Hall, T.E. Experiencing the Restorative Components of Wilderness Environments: Does Congestion Interfere and Does Length of Exposure Matter? Environ. Behav. 2010, 42, 806–823. [Google Scholar] [CrossRef] [Green Version]
- Hartig, T.; Mang, M.; Evans, G.W. Restorative Effects of Natural Environment Experiences. Environ. Behav. 1991, 23, 3–26. [Google Scholar] [CrossRef]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Horowitz, L.M.; Rosenberg, S.E.; Bartholomew, K. Interpersonal problems, attachment styles, and outcome in brief dynamic psychotherapy. J. Consult. Clin. Psychol. 1993, 61, 549. [Google Scholar] [CrossRef]
- Russell, K.C.; Hendee, J.C.; Phillips-Miller, D. Wilderness therapy as an intervention and treatment for adolescents with behavioral problems. Wild Sci. Time Chang. 2000, 15, 136–141. [Google Scholar]
- Annerstedt, M.; Währborg, P. Nature-assisted therapy: Systematic review of controlled and observational studies. Scand. J. Public Health 2011, 39, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (Forest Bathing) and Nature Therapy on Mental Health: A Systematic Review and Meta-analysis. Int. J. Ment. Heal. Addict. 2020, 20, 337–361. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological Effects of Nature Therapy: A Review of the Research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef]
- Mau, M.; Aaby, A.; Klausen, S.; Roessler, K. Are Long-Distance Walks Therapeutic? A Systematic Scoping Review of the Conceptualization of Long-Distance Walking and Its Relation to Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 7741. [Google Scholar] [CrossRef] [PubMed]
- Mau, M.; Nielsen, D.S.; Jakobsen, I.S.; Klausen, S.H.; Roessler, K.K. Mental movements: How long-distance walking influences reflection processes among middle-age and older adults. Scand. J. Psychol. 2021, 62, 365–373. [Google Scholar] [CrossRef]
- Duvall, J. Enhancing the benefits of outdoor walking with cognitive engagement strategies. J. Environ. Psychol. 2011, 31, 27–35. [Google Scholar] [CrossRef]
- Høegmark, S.; Elmose Andersen, T.; Grahn, P.; Kaya Roessler, K. The wildman programme. A nature-based rehabilitation programme enhancing quality of life for men on long-term sick leave: Study protocol for a matched controlled study in Denmark. Int. J. Environ. Res. Public Health 2020, 17, 3368. [Google Scholar] [CrossRef]
- Høegmark, S.; Andersen, T.E.; Grahn, P.; Mejldal, A.; Roessler, K.K. The Wildman Programme—Rehabilitation and Reconnection with Nature for Men with Mental or Physical Health Problems—A Matched-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 11465. [Google Scholar] [CrossRef]
- Høegmark, S.; Andersen, T.E.; Grahn, P.; Roessler, K.K. The Wildman Programme–Experiences from a first implementation of a nature-based intervention designed for men with stress and chronic illnesses. Complement. Ther. Clin. Pract. 2022, 101535. [Google Scholar] [CrossRef]
- Smith, J.A.; Watkins, D.C.; Griffith, D.M. Equity, gender and health: New directions for global men’s health pro-motion. Health Promot. J. Aust. 2020, 31, 161–165. [Google Scholar] [CrossRef] [Green Version]
- Ragonese, C.; Shand, T.; Barker, G. Masculine Norms and Men’s Health: Making the Connections; Promun-do-US: Washington, DC, USA, 2019. [Google Scholar]
- Madsen, S.A. Men as patients: Understanding and communicating with men. Trends Urol. Men’s Health 2015, 6, 22–26. [Google Scholar] [CrossRef]
- Ragonese, C.; Barker, G. Understanding masculinities to improve men’s health. Lancet 2019, 394, 198–199. [Google Scholar] [CrossRef]
- Gibson, R. Natural environmental psychology. In Environmental Psychology. Principles and Practice, 5th ed.; Optimal Books: Victoria, BC, Canada, 2014; pp. 381–419. [Google Scholar]
- Roessler, K.K. A corrective emotional experience-or just a bit of exercise? The relevance of interpersonal learning in Exercise on prescription. Scand. J. Psychol. 2011, 52, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Pálsdóttir, A.M.; Persson, D.; Persson, B.; Grahn, P. The Journey of Recovery and Empowerment Embraced by Nature—Clients’ Perspectives on Nature-Based Rehabilitation in Relation to the Role of the Natural Environment. Int. J. Environ. Res. Public Health 2014, 11, 7094–7115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leavell, M.A.; Leiferman, J.A.; Gascon, M.; Braddick, F.; Gonzalez, J.C.; Litt, J.S. Nature-Based Social Prescribing in Urban Settings to Improve Social Connectedness and Mental Well-being: A Review. Curr. Environ. Health Rep. 2019, 6, 297–308. [Google Scholar] [CrossRef]
- Castelo, N.; White, K.; Goode, M.R. Exposure to nature promotes self-transcendence and prosocial behavior. J. Environ. Psychol. 2021, 76, 101639. [Google Scholar] [CrossRef]
- Rehabilitation International Denmark. 2004. Available online: https://www.rehabiliteringsforum.dk/in-english/ (accessed on 10 January 2022). (In English).
- Roessler, K.K.; Glintborg, D.; Ravn, P.; Birkebaek, C.; Andersen, M. Supportive relationships—Psychological effects of group counselling in women with polycystic ovary syndrome (PCOS). Commun. Med. 2013, 9, 125–131. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Gu, Y.; Luo, Y.-J.; Cacioppo, J.T. The Mental Representation of Social Connections: Generalizability Extended to Beijing Adults. PLoS ONE 2012, 7, e44065. [Google Scholar] [CrossRef]
- Monsen, J.T.; Hagtvet, K.A.; Havik, O.E.; Eilertsen, D.E. Circumplex structure and personality disorder correlates of the Interpersonal Problems Model (IIP-C): Construct validity and clinical implications. Psychol. Assess. 2006, 18, 165–173. [Google Scholar] [CrossRef]
- Huber, D.; Henrich, G.; Klug, G. The Inventory of Interpersonal Problems (IIP): Sensitivity to change. Psychother. Res. 2007, 17, 474–481. [Google Scholar] [CrossRef]
- Horowitz, L.M. Interpersonal Formulations of Psychopathology; American Psychological Association: Washington, DC, USA, 2004. [Google Scholar]
- McEvoy, P.M.; Burgess, M.M.; Page, A.C.; Nathan, P.; Fursland, A. Interpersonal problems across anxiety, depression, and eating disorders: A transdiagnostic examination. Br. J. Clin. Psychol. 2012, 52, 129–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarquhar, T.; Luyten, P.; Fonagy, P. Changes in interpersonal problems in the psychotherapeutic treatment of depression as measured by the Inventory of Interpersonal Problems: A systematic review and meta-analysis. J. Affect. Disord. 2018, 226, 108–123. [Google Scholar] [CrossRef] [PubMed]
- Viana, A.G.; Stevens, E.N. Interpersonal difficulties as an underlying mechanism in the anxiety-depression asso-ciation. Behav. Chang. 2013, 30, 273–282. [Google Scholar] [CrossRef]
- Jakobsen, I.S.; Madsen, L.M.R.; Mau, M.; Hjemdal, O.; Friborg, O. The relationship between resilience and loneliness elucidated by a Danish version of the resilience scale for adults. BMC Psychol. 2020, 8, 131. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J.; Hawkley, L.C.; Cacioppo, J.T. On the Reciprocal Association Between Loneliness and Subjective Well-being. Am. J. Epidemiol. 2012, 176, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Mueller, S.E.; Degen, B.; Petitjean, S.; Wiesbeck, G.A.; Walter, M. Gender Differences in Interpersonal Problems of Alcohol-Dependent Patients and Healthy Controls. Int. J. Environ. Res. Public Health 2009, 6, 3010–3022. [Google Scholar] [CrossRef]
- Falkum, E.; Vaglum, P. The relationship between interpersonal problems and occupational stress in physicians. Gen. Hosp. Psychiatry 2005, 27, 285–291. [Google Scholar] [CrossRef]
- Harper, N.J.; Russell, K.C.; Cooley, R.; Cupples, J. Catherine Freer Wilderness Therapy Expeditions: An Exploratory Case Study of Adolescent Wilderness Therapy, Family Functioning, and the Maintenance of Change. Child Care Q. 2007, 36, 111–129. [Google Scholar] [CrossRef]
- Horowitz, L.M.; Rosenberg, S.E.; Baer, B.A.; Ureño, G. Inventory of interpersonal problems: Psychometric properties and clinical applications. J. Consult. Clin. Psychol. 1988, 56, 885–892. [Google Scholar] [CrossRef]
- Alden, L.E.; Wiggins, J.S.; Pincus, A.L. Construction of circumplex scales for the inventory of interpersonal problems. J. Personal. Assess. 1990, 55, 521–536. [Google Scholar] [CrossRef]
- American Medical Association. ICD-10-CM 2019 The Complete Official Codebook; American Medical Association: Chicago, IL, USA, 2020. [Google Scholar]
- Soldz, S.; Budman, S.; Demby, A.; Merry, J. A short form of the inventory of interpersonal problems circumplex scales. Assessment 1995, 2, 53–63. [Google Scholar] [CrossRef]
- Gurtman, M.B. Interpersonal problems and the psychotherapy context: The construct validity of the Inventory of Interpersonal Problems. Psychol. Assess. 1996, 8, 241–255. [Google Scholar] [CrossRef]
- George, D.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference. 11.0 Update, 4th ed.; Allyn & Bacon: Boston, MA, USA, 2003. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Atchley, R.A.; Strayer, D.L.; Atchley, P. Creativity in the Wild: Improving Creative Reasoning through Immersion in Natural Settings. PLoS ONE 2012, 7, e51474. [Google Scholar] [CrossRef] [PubMed]
- Burns, G.W. Naturally happy, naturally healthy: The role of the natural environment in well-being. Sci. Well-Being 2005, 404–432. [Google Scholar] [CrossRef]
- Roessler, K.K.; Mau, M.; Ekstrøm, C.T. Interpersonal problems of alcohol use disorder patients undergoing a physical exercise intervention—A randomised controlled trial. Nord. Psychol. 2017, 70, 1–11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Treatment as Usual | The Wildman Programme | p | |
|---|---|---|---|---|
| Age | Mean (SD) | 57.55 (10.70) | 54.60 (13.67) | 0.23 |
| Education | Lower secondary or less | 6 (15.8%) | 18 (16.7%) | 0.95 |
| Upper secondary | 13 (34.2%) | 39 (36.1%) | ||
| Short cycle tertiary/bachelor | 13 (34.2%) | 38 (35.2%) | ||
| Master’s or above | 6 (15.8%) | 13 (12.0%) | ||
| Employment | Unemployed | 3 (7.9%) | 20 (18.7%) | 0.13 |
| Employed | 13 (34.2%) | 21 (19.6%) | ||
| Flex/ressource | 1 (2.6%) | 12 (11.2%) | ||
| Retired | 12 (31.6%) | 28 (26.2%) | ||
| Other | 9 (23.7%) | 26 (24.3%) | ||
| Marital status | Alone | 8 (21.1%) | 28 (25.7%) | 0.57 |
| Cohabiting | 30 (78.9%) | 81 (74.3%) | ||
| Parental status | Yes | 32 (84.2%) | 91 (83.5%) | 0.92 |
| No | 6 (15.8%) | 18 (16.5%) | ||
| Baseline (T1) | Post-Treatment (T2) | Follow-Up (T3) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| IIP Subscale | TAU | The Wildman Programme | p | TAU | The Wildman Programme | p | TAU | The Wildman Programme | p |
| Domineering | 0.37 (0.55) | 0.64 (0.64) | 0.02 | 0.30 (0.46) | 0.46 (0.57) | 0.17 | 0.39 (0.34) | 0.52 (0.57) | 0.29 |
| Vindictive | 1.22 (1.09) | 1.28 (1.00) | 0.76 | 1.01 (1.07) | 1.42 (1.11) | 0.072 | 1.08 (0.97) | 1.21 (1.10) | 0.59 |
| Cold | 1.35 (1.15) | 1.35 (0.93) | 0.99 | 1.07 (0.84) | 1.29 (0.99) | 0.30 | 1.02 (0.92) | 1.29 (1.14) | 0.28 |
| Socially inhibited | 1.40 (1.02) | 1.44 (0.97) | 0.87 | 1.25 (0.94) | 1.45 (0.98) | 0.34 | 1.26 (1.04) | 1.56 (1.24) | 0.28 |
| Non-assertive | 1.41 (0.95) | 1.48 (0.96) | 0.73 | 1.19 (1.00) | 1.51 (0.91) | 0.12 | 1.38 (1.05) | 1.42 (0.93) | 0.82 |
| Exploitable | 1.47 (0.73) | 1.59 (0.80) | 0.40 | 1.29 (0.78) | 1.49 (0.70) | 0.19 | 1.50 (0.80) | 1.48 (0.68) | 0.91 |
| Overly nurturant | 1.70 (1.00) | 1.81 (0.86) | 0.50 | 1.55 (0.79) | 1.81 (0.79) | 0.12 | 1.56 (0.84) | 1.77 (0.86) | 0.29 |
| Intrusive | 0.96 (0.65) | 1.21 (0.73) | 0.07 | 1.02 (0.83) | 1.26 (0.74) | 0.15 | 1.05 (0.67) | 1.13 (0.70) | 0.65 |
| Total | 1.25 (0.70) | 1.37 (0.55) | 0.34 | 1.11 (0.64) | 1.30 (0.57) | 0.17 | 1.14 (0.54) | 1.26 (0.63) | 0.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mau, M.; Vang, M.L.; Mejldal, A.; Høegmark, S.; Roessler, K.K. Can Rehabilitation in Nature Improve Self-Perceived Interpersonal Problems? A Matched-Control Study. Int. J. Environ. Res. Public Health 2022, 19, 3622. https://doi.org/10.3390/ijerph19063622
Mau M, Vang ML, Mejldal A, Høegmark S, Roessler KK. Can Rehabilitation in Nature Improve Self-Perceived Interpersonal Problems? A Matched-Control Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3622. https://doi.org/10.3390/ijerph19063622
Chicago/Turabian StyleMau, Martin, Maria L. Vang, Anna Mejldal, Simon Høegmark, and Kirsten K. Roessler. 2022. "Can Rehabilitation in Nature Improve Self-Perceived Interpersonal Problems? A Matched-Control Study" International Journal of Environmental Research and Public Health 19, no. 6: 3622. https://doi.org/10.3390/ijerph19063622