
Dietary Supplement Use during Pregnancy: Perceptions versus Reality

 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling Method
2.2. Recruitment
2.3. Data Collection
2.3.1. Dietary Supplements
2.3.2. Types of Dietary Supplements Used
2.3.3. Perception of Dietary Supplements
2.3.4. General Demographic Information and Pregnancy Information
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
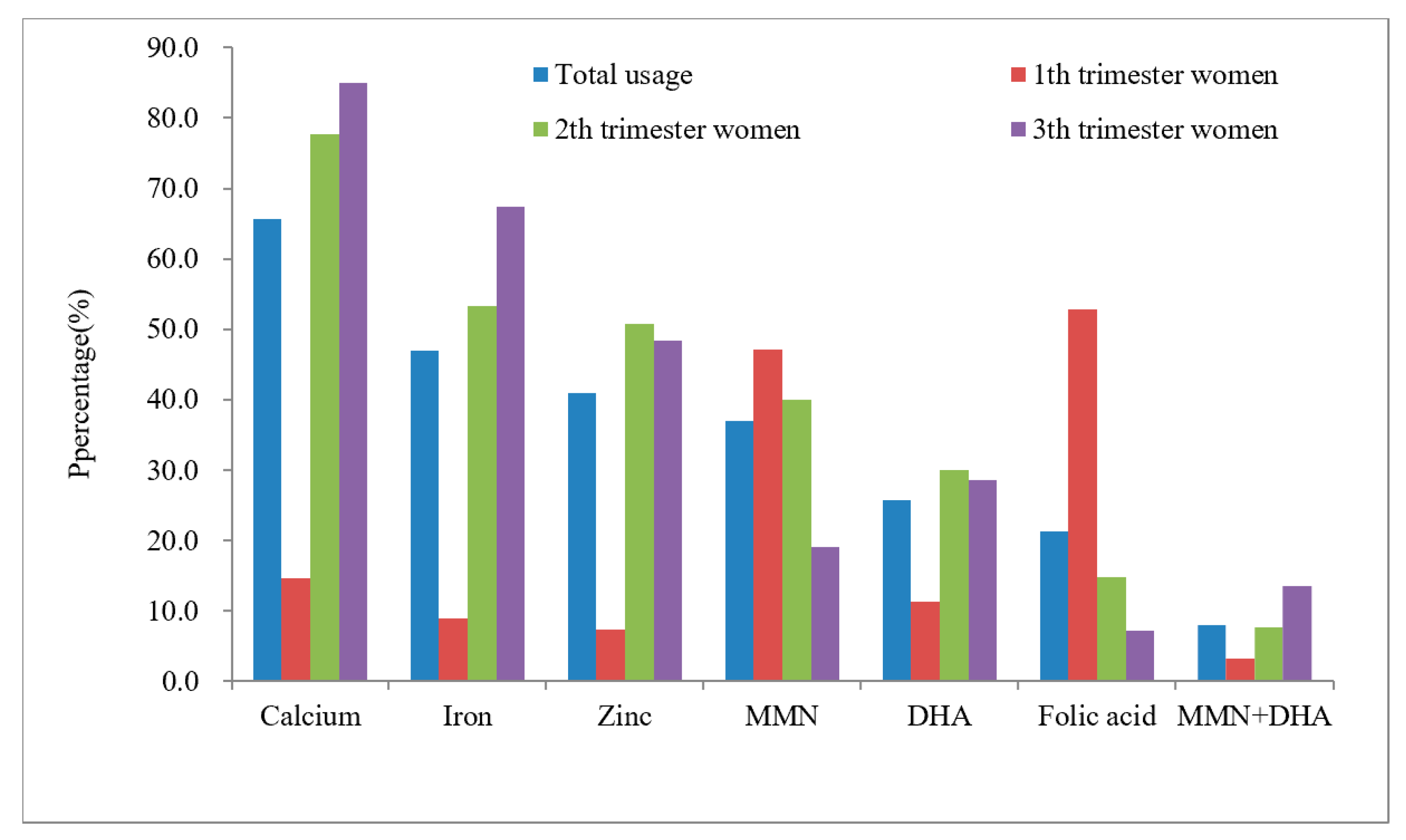
3.2. Use of Dietary Supplements
3.3. Repeated Supplementation of Nutrients
3.4. Information Sources and Purchase Channels
3.5. Pregnant Women’s Perceptions of Dietary Supplement Use
3.6. Factors Associated with the Use of Multiple Dietary Supplements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dickinson, A. History and overview of DSHEA. Fitoterapia 2011, 82, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhang, Z. Development of dietary nutrition supplementary industry (I). Fine Spec. Chem. 2019, 27, 1–10. [Google Scholar]
- Liu, H.; Zhang, S.; Zou, H.; Pan, Y.; Yang, Q.; Ouyang, Y.; Luo, J.; Lin, Q. Dietary Supplement Use Among Chinese Primary School Students: A Cross-Sectional Study in Hunan Province. Int. J. Environ. Res. Public Health 2019, 16, 374. [Google Scholar] [CrossRef] [PubMed]
- Chinese Nutrition Society. Dietary guidelines for pregnant Women. Chin. J. Perinat. Med. 2016, 19, 641–648. [Google Scholar]
- Picciano, M.F. Pregnancy and lactation: Physiological adjustments, nutritional requirements and the role of dietary supplements. J. Nutr. 2003, 133, 1997s–2002s. [Google Scholar] [CrossRef]
- Blumfield, M.L.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. A systematic review and meta-analysis of micronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2013, 71, 118–132. [Google Scholar] [CrossRef]
- Parisi, F.; Laoreti, A.; Cetin, I. Multiple micronutrient needs in pregnancy in industrialized countries. Ann. Nutr. Metab. 2014, 65, 13–21. [Google Scholar] [CrossRef]
- Kumari, S.; Garg, N.; Kumar, A.; Guru, P.K.I.; Ansari, S.; Anwar, S.; Singh, K.P.; Kumari, P.; Mishra, P.K.; Gupta, B.K.; et al. Maternal and severe anaemia in delivering women is associated with risk of preterm and low birth weight: A cross sectional study from Jharkhand, India. One Health (Amst. Neth.) 2019, 8, 100098. [Google Scholar] [CrossRef]
- Wu, G.; Imhoff-Kunsch, B.; Girard, A.W. Biological mechanisms for nutritional regulation of maternal health and fetal development. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 4–26. [Google Scholar] [CrossRef]
- Oliver, E.M.; Grimshaw, K.E.; Schoemaker, A.A.; Keil, T.; McBride, D.; Sprikkelman, A.B.; Ragnarsdottir, H.S.; Trendelenburg, V.; Emmanouil, E.; Reche, M.; et al. Dietary habits and supplement use in relation to national pregnancy recommendations: Data from the EuroPrevall birth cohort. Matern. Child. Health J. 2014, 18, 2408–2425. [Google Scholar] [CrossRef]
- Titilayo, A.; Palamuleni, M.E.; Omisakin, O. Sociodemographic factors influencing adherence to antenatal iron supplementation recommendations among pregnant women in Malawi: Analysis of data from the 2010 Malawi Demographic and Health Survey. Malawi Med. J. J. Med. Assoc. Malawi 2016, 28, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Gebremedhin, S.; Samuel, A.; Mamo, G.; Moges, T.; Assefa, T. Coverage, compliance and factors associated with utilization of iron supplementation during pregnancy in eight rural districts of Ethiopia: A cross-sectional study. BMC Public Health 2014, 14, 607. [Google Scholar] [CrossRef]
- Ogundipe, O.; Hoyo, C.; Østbye, T.; Oneko, O.; Manongi, R.; Lie, R.T.; Daltveit, A.K. Factors associated with prenatal folic acid and iron supplementation among 21,889 pregnant women in Northern Tanzania: A cross-sectional hospital-based study. BMC Public Health 2012, 12, 481. [Google Scholar] [CrossRef]
- Dong, S.; Zhou, Q.; Liu, J.; Xiao, R.; Yu, H. Investigation and analysis on nutritional knowledge, attitude, practice of 377 pregnant women. Matern. Child Health Care China 2016, 31, 345–347. [Google Scholar]
- Liu, D.; Li, J.; Qu, P.; Dang, S.; Wu, X.; Zhang, R.; Yan, H.; Yan, H. Prenatal supplementations of iron, iron-containing multimicronutrients and antianemic Chinese patent medicines in women in Shaanxi province, 2010–2013. Chin. J. Epidemiol. 2017, 38, 1466–1470. [Google Scholar] [CrossRef]
- Tang, L.; Lee, A.H.; Yau, K.K.W.; Hui, Y.V.; Binns, C.W. Consumption of dietary supplements by Chinese women during pregnancy and postpartum: A prospective cohort study. Matern. Child Nutr. 2017, 13, e12435. [Google Scholar] [CrossRef]
- Shi, Y.; Chen, Y.; Zhan, Y.; Feng, Y.; Wu, S.; Wang, Y.; Yan, B.; Shen, Z.; Ma, S.; Jiang, Y.; et al. A survey of the use of nutritional supplements in 7931 women in early pregnancy. Med. J. Peking Union Med. Coll. Hosp. 2020, 11, 585–591. [Google Scholar]
- Gao, Y.; Ma, J.; Jiang, H.; Wang, Q.; Xu, M.; Yu, H. Use of dietary supplements and its influence factors in pregnant women. Chin. J. Public Health 2012, 28, 272–274. [Google Scholar]
- Keats, E.C.; Haider, B.A.; Tam, E.; Bhutta, Z.A. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 3, CD004905. [Google Scholar] [CrossRef]
- Hovdenak, N.; Haram, K. Influence of mineral and vitamin supplements on pregnancy outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 164, 127–132. [Google Scholar] [CrossRef]
- Bailey, R.L.; Pac, S.G.; Fulgoni, V.L., 3rd; Reidy, K.C.; Catalano, P.M. Estimation of Total Usual Dietary Intakes of Pregnant Women in the United States. JAMA Netw. Open 2019, 2, e195967. [Google Scholar] [CrossRef] [PubMed]
- Savard, C.; Lemieux, S.; Weisnagel, S.J.; Fontaine-Bisson, B.; Gagnon, C.; Robitaille, J.; Morisset, A.S. Trimester-Specific Dietary Intakes in a Sample of French-Canadian Pregnant Women in Comparison with National Nutritional Guidelines. Nutrients 2018, 10, 768. [Google Scholar] [CrossRef] [PubMed]
- Department of Disease Control, MOH; PRC. Guidelines for the Prevention and Control of Overweight and Obesity in Chinese Adults; People’s Medical Publishing House: Beijing, China, 2006. [Google Scholar]
- Wang, J.; Zhang, L.; Piao, J.; Zhang, J.; Yang, X.; Yin, S. Nutrition and health status of pregnant women in 8 provinces in China. J. Hyg. Res. 2011, 40, 201–203. [Google Scholar]
- Aronsson, C.A.; Vehik, K.; Yang, J.; Uusitalo, U.; Hay, K.; Joslowski, G.; Riikonen, A.; Ballard, L.; Virtanen, S.M.; Norris, J.M.; et al. Use of dietary supplements in pregnant women in relation to sociodemographic factors-a report from The Environmental Determinants of Diabetes in the Young (TEDDY) study. Public Health Nutr. 2013, 16, 1390–1402. [Google Scholar] [CrossRef] [PubMed]
- McAlpine, J.M.; Vanderlelie, J.J.; Vincze, L.J.; Perkins, A.V. Use of micronutrient supplements in pregnant women of south-east Queensland. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 561–567. [Google Scholar] [CrossRef]
- Hatzopoulou, K.; Filis, V.; Grammatikopoulou, M.G.; Kotzamanidis, C.; Tsigga, M. Greek pregnant women demonstrate inadequate micronutrient intake despite supplement use. J. Diet. Suppl. 2014, 11, 155–165. [Google Scholar] [CrossRef]
- Pinto, E.; Barros, H.; dos Santos Silva, I. Dietary intake and nutritional adequacy prior to conception and during pregnancy: A follow-up study in the north of Portugal. Public Health Nutr. 2009, 12, 922–931. [Google Scholar] [CrossRef]
- Ladipo, O.A. Nutrition in pregnancy: Mineral and vitamin supplements. Am. J. Clin. Nutr. 2000, 72, 280S–290S. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, Y.; Li, X. Analysis of whole blood microelements content in 3860 pregnant women with second or third trimester in Hefei city. J. Reprod. Med. 2020, 29, 770–774. [Google Scholar]
- Tabrizi, F.M.; Pakdel, F.G. Serum Level of Some Minerals during Three Trimesters of Pregnancy in Iranian Women and Their Newborns: A Longitudinal Study. Indian J. Clin. Biochem. 2014, 29, 174–180. [Google Scholar] [CrossRef]
- Bao, Q. Analysis of serum copper, zinc, calcium, iron and magnesium in 1086 pregnant women. Guangxi Med. J. 2013, 35, 780–784. [Google Scholar]
- Yang, K.; Cai, H.; Ao, Y. Changes and clinical significe of calcium, zinc and iron in peripheral blood of pregnant women during different pregnancy. Hainan Med. J. 2021, 32, 1692–1694. [Google Scholar]
- World Health Organization. Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. WHO Recommendation on Calcium Supplementation before Pregnancy for the Prevention of Pre-Eclampsia and Its Complications; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Liu, D.; Cheng, Y.; Dang, S.; Wang, D.; Zhao, Y.; Li, C.; Li, S.; Lei, F.; Qu, P.; Mi, B.; et al. Maternal adherence to micronutrient supplementation before and during pregnancy in Northwest China: A large-scale population-based cross-sectional survey. BMJ Open 2019, 9, e028843. [Google Scholar] [CrossRef] [PubMed]
- Haugen, M.; Brantsaeter, A.L.; Alexander, J.; Meltzer, H.M. Dietary supplements contribute substantially to the total nutrient intake in pregnant Norwegian women. Ann. Nutr. Metab. 2008, 52, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Newberry, S.J.; Chung, M.; Booth, M.; Maglione, M.A.; Tang, A.M.; O’Hanlon, C.E.; Wang, D.D.; Okunogbe, A.; Huang, C.; Motala, A.; et al. Omega-3 Fatty Acids and Maternal and Child Health: An Updated Systematic Review. Evid. Rep./Technol. Assess. 2016, 224, 1–826. [Google Scholar] [CrossRef][Green Version]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst. Rev. 2018, 11, Cd003402. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Pena-Rosas, J.P.; Fernandez-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, 2015, CD007950. [Google Scholar] [CrossRef]
- Force, U.S.P.S.T.; Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W., Jr.; Garcia, F.A.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Folic Acid Supplementation for the Prevention of Neural Tube Defects: US Preventive Services Task Force Recommendation Statement. JAMA 2017, 317, 183–189. [Google Scholar] [CrossRef]
- Nilsen, R.M.; Vollset, S.E.; Gjessing, H.K.; Magnus, P.; Meltzer, H.M.; Haugen, M.; Ueland, P.M. Patterns and predictors of folic acid supplement use among pregnant women: The Norwegian Mother and Child Cohort Study. Am. J. Clin. Nutr. 2006, 84, 1134–1141. [Google Scholar] [CrossRef]
- Zheng, L.; Huang, J.; Kong, H.; Wang, F.; Su, Y.; Xin, H. The effect of folic acid throughout pregnancy among pregnant women at high risk of pre-eclampsia: A randomized clinical trial. Pregnancy Hypertens 2020, 19, 253–258. [Google Scholar] [CrossRef]
- McNulty, H.; Rollins, M.; Cassidy, T.; Caffrey, A.; Marshall, B.; Dornan, J.; McLaughlin, M.; McNulty, B.A.; Ward, M.; Strain, J.J.; et al. Effect of continued folic acid supplementation beyond the first trimester of pregnancy on cognitive performance in the child: A follow-up study from a randomized controlled trial (FASSTT Offspring Trial). BMC Med. 2019, 17, 196. [Google Scholar] [CrossRef]
- Caffrey, A.; McNulty, H.; Rollins, M.; Prasad, G.; Gaur, P.; Talcott, J.B.; Witton, C.; Cassidy, T.; Marshall, B.; Dornan, J.; et al. Effects of maternal folic acid supplementation during the second and third trimesters of pregnancy on neurocognitive development in the child: An 11-year follow-up from a randomised controlled trial. BMC Med. 2021, 19, 73. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.F.; Baron, J.A.; Sandler, R.S.; Haile, R.W.; Ahnen, D.J.; Bresalier, R.S.; McKeown-Eyssen, G.; Summers, R.W.; Rothstein, R.I.; Burke, C.A.; et al. Folic acid for the prevention of colorectal adenomas: A randomized clinical trial. JAMA 2007, 297, 2351–2359. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.B.; Dickstein, A.; Jacques, P.F.; Haggarty, P.; Selhub, J.; Dallal, G.; Rosenberg, I.H. A temporal association between folic acid fortification and an increase in colorectal cancer rates may be illuminating important biological principles: A hypothesis. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1325–1329. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.H.; Sanghvi, T.; Kim, S.S.; Tran, L.M.; Afsana, K.; Mahmud, Z.; Aktar, B.; Menon, P. Factors influencing maternal nutrition practices in a large scale maternal, newborn and child health program in Bangladesh. PLoS ONE 2017, 12, e0179873. [Google Scholar] [CrossRef]
- Kikuchi, D.; Obara, T.; Usuzaki, T.; Yonezawa, Y.; Yamashita, T.; Oyanagi, G.; Noda, A.; Ueno, F.; Murakami, K.; Matsubara, H.; et al. Evaluating folic acid supplementation among Japanese pregnant women with dietary intake of folic acid lower than 480 microg per day: Results from TMM BirThree Cohort Study. J. Matern. Fetal. Neonatal. Med. 2020, 35, 964–969. [Google Scholar] [CrossRef]
- Hu, M.; Qin, R.; Lin, X.; Ding, Y.; Xu, J.; Li, F.; Wang, Z. Study on the dietary supplements among women while pregnant and lactating from four cities of China. Matern. Child Health Care China 2019, 34, 3769–3772. [Google Scholar]
- Li, S.; Lei, F.; Zhang, R.; Liu, D.; Qu, P.; Cheng, Y.; Liu, X.; Chen, F.; Dang, S.; Yan, H. Socioeconomic disparity in the diet quality of pregnant women in Northwest China. Asia Pac. J. Clin. Nutr. 2019, 28, 330–340. [Google Scholar] [CrossRef]
- Malek, D.L.; Umberger, D.W.; Makrides, D.M.; Collins, D.C.; Zhou, D.S. Understanding motivations for dietary supplementation during pregnancy: A focus group study. Midwifery 2018, 57, 59–68. [Google Scholar] [CrossRef]
- Soltani, H.; Duxbury, A.; Rundle, R.; Marvin-Dowle, K. Dietary habits and supplementation practices of young women during pregnancy: An online cross-sectional survey of young mothers and health care professionals. BMC Nutr. 2017, 3, 19. [Google Scholar] [CrossRef]
- Sato, Y.; Nakanishi, T.; Chiba, T.; Yokotani, K.; Ishinaga, K.; Takimoto, H.; Itoh, H.; Umegaki, K. Prevalence of inappropriate dietary supplement use among pregnant women in Japan. Asia Pac. J. Clin. Nutr. 2013, 22, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.A.; Avorn, J. Internet marketing of herbal products. JAMA 2003, 290, 1505–1509. [Google Scholar] [CrossRef] [PubMed]
- Han, T.; Dong, J.; Zhang, J.; Zhang, C.; Wang, Y.; Zhang, Z.; Xiang, M. Nutrient supplementation among pregnant women in China: An observational study. Public Health Nutr. 2021, 1–6. [Google Scholar] [CrossRef]
- Toda, M.; Uneyama, C. Current Problems Associated with Overseas Health Products. Yakugaku Zasshi J. Pharm. Soc. Jpn. 2018, 138, 1531–1536. [Google Scholar] [CrossRef]
- Dong, C.X.; Yin, S.A. The ten-year retrospect of nutrition and health status of pregnant women in China. Chin. J. Prev. Med. 2018, 52, 94–100. [Google Scholar] [CrossRef]
- Beluska-Turkan, K.; Korczak, R.; Hartell, B.; Moskal, K.; Maukonen, J.; Alexander, D.E.; Salem, N.; Harkness, L.; Ayad, W.; Szaro, J.; et al. Nutritional Gaps and Supplementation in the First 1000 Days. Nutrients 2019, 11, 2891. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Types of Dietary Supplements Used (n,%) | ||||||
|---|---|---|---|---|---|---|
| Characteristics | n (%) | 0 | 1–3 | 4–6 | χ2 | p |
| Total | 572 (100%) | 30 (5.2) | 372 (65.0) | 170 (29.8) | ||
| Age (years) * | 7.796 | 0.091 | ||||
| ≤25 | 74 (13.0) | 8 (10.8) | 51 (68.9) | 15 (20.3) | ||
| 26–35 | 437 (76.6) | 20 (4.6) | 284 (65.0) | 133 (30.4) | ||
| 36–45 | 59 (10.4) | 2 (3.4) | 36 (61.0) | 21 (35.6) | ||
| Educational level * | 14.072 | 0.005 | ||||
| Junior high school and below | 33 (5.8) | 4 (12.1) | 25 (75.8) | 4 (12.1) | ||
| High school | 74 (13.0) | 7 (9.5) | 51 (68.9) | 16 (21.6) | ||
| Bachelor degree and above | 461 (81.2) | 19 (4.2) | 292 (63.3) | 150 (32.5) | ||
| Employed during pregnancy * | 2.256 | 0.314 | ||||
| Yes | 484 (85.1) | 23 (4.8) | 314 (64.9) | 147 (30.3) | ||
| No | 85 (14.9) | 7 (8.2) | 56 (65.9) | 22 (25.9) | ||
| Household register * | 1.328 | 0.515 | ||||
| Rural area | 269 (47.2) | 17 (6.3) | 175 (65.1) | 77 (28.6) | ||
| Urban | 301 (52.8) | 13 (4.3) | 195 (64.8) | 93 (30.9) | ||
| Income (RMB/month) * | 12.480 | 0.014 | ||||
| 2000–5999 | 97 (17.4) | 8 (8.2) | 71 (73.2) | 18 (18.6) | ||
| 6000–9999 | 213 (38.2) | 15 (7.0) | 128 (60.1) | 70 (32.9) | ||
| ≥10,000 | 247 (44.4) | 7 (2.8) | 161 (65.2) | 79 (32.0) | ||
| Pre-pregnancy BMI * | 3.311 | 0.507 | ||||
| Underweight | 97 (17.1) | 3 (3.1) | 59 (60.8) | 35 (36.1) | ||
| Healthy weight | 402 (70.9) | 23 (5.7) | 267 (66.4) | 112 (27.9) | ||
| Overweight/Obese | 68 (12.0) | 4 (5.9) | 43 (63.2) | 21 (30.9) | ||
| Gestational stage | 48.037 | <0.001 | ||||
| First trimester | 123 (21.5) | 4 (3.3) | 112 (91.1) | 7 (5.6) | ||
| Second trimester | 323 (56.5) | 19 (5.9) | 188 (58.2) | 116 (35.9) | ||
| Third trimester | 126 (22.0) | 7 (5.6) | 72 (57.1) | 47 (37.3) | ||
| Number of fetuses | 3.685 | 0.148 | ||||
| 1 | 543 (94.9) | 30 (5.5) | 356 (65.6) | 157 (28.9) | ||
| ≥2 | 29 (5.1) | 0 (0.0) | 16 (55.2) | 13 (44.8) | ||
| Way of pregnancy * | 9.887 | 0.005 | ||||
| Natural | 503 (90.6) | 29 (5.8) | 332 (66.0) | 142 (28.2) | ||
| ART | 52 (9.4) | 1 (1.9) | 25 (48.1) | 26 (50.0) | ||
| Number of pregnancies * | 17.673 | 0.001 | ||||
| 1 | 273 (48.7) | 5 (1.8) | 189 (69.2) | 79 (28.9) | ||
| 2 | 150 (26.7) | 15 (10.0) | 96 (64.0) | 39 (26.0) | ||
| ≥3 | 138 (24.6) | 10 (7.2) | 79 (57.3) | 49 (35.5) | ||
| Number of deliveries * | 8.649 | 0.072 | ||||
| 0 | 351 (62.0) | 13 (3.7) | 225 (64.1) | 113 (32.2) | ||
| 1 | 194 (34.3) | 14 (7.2) | 129 (66.5) | 51 (26.3) | ||
| ≥2 | 21 (3.7) | 3 (14.3) | 14 (66.7) | 4 (19.0) | ||
| Number of abortions * | 14.551 | 0.005 | ||||
| 0 | 378 (67.1) | 15 (4.0) | 261 (69.0) | 102 (27.0) | ||
| 1 | 122 (21.7) | 13 (10.7) | 71 (58.2) | 38 (31.1) | ||
| ≥2 | 63 (11.2) | 2 (3.2) | 34 (54.0) | 27 (42.8) | ||
| Number of antenatal visits * | 33.833 | <0.001 | ||||
| ≤5 | 284 (54.0) | 18 (6.3) | 211 (74.3) | 55 (19.4) | ||
| 6 to 10 | 192 (36.5) | 4 (2.1) | 116 (60.4) | 72 (37.5) | ||
| ≥10 | 50 (9.5) | 3 (6.0) | 22 (44.0) | 25 (50.0) | ||
| Planned pregnancy * | 0.826 | 0.662 | ||||
| Yes | 373 (65.8) | 17 (4.6) | 243 (65.1) | 113 (30.3) | ||
| No | 194 (34.2) | 12 (6.2) | 127 (65.5) | 55 (28.3) | ||
| Iron deficiency anemia * | 8.948 | 0.010 | ||||
| Yes | 84 (14.7) | 0 (0.0) | 52 (61.9) | 32 (38.1) | ||
| No | 487 (85.3) | 30 (6.2) | 320 (65.7) | 137 (28.1) | ||
| Hypothyroidism * | 12.368 | 0.002 | ||||
| Yes | 72 (12.6) | 1 (1.4) | 37 (51.4) | 34 (47.2) | ||
| No | 499 (87.4) | 29 (5.8) | 335 (67.1) | 135 (27.1) | ||
| Variable | n | (%) | |
|---|---|---|---|
| Information sources for DS | |||
| Doctor | 400 | 69.9 | |
| Family or friends | 286 | 50.0 | |
| Network knowledge | 272 | 47.6 | |
| Newspaper or magazine | 118 | 20.6 | |
| Advertising | 43 | 7.6 | |
| Purchase channels | |||
| Hospitals | 415 | 72.6 | |
| Pharmacies | 258 | 45.1 | |
| Overseas Daigou or online purchases | 182 | 31.8 | |
| Community | 29 | 5.1 | |
| Other places | 22 | 3.8 |
| Item | Approval (%) |
|---|---|
| DS can prevent nutrition-related diseases during pregnancy. | 89.2 |
| DS can improve/treat nutrition-related diseases during pregnancy. | 78.7 |
| In the case of good nutrition and health during pregnancy, there is no need to DS. | 34.8 |
| In the case of malnutrition symptoms/disease during pregnancy, it is necessary to use DS. | 96.0 |
| Before taking DS, it is important to have a basic understanding/knowledge of DS. | 94.1 |
| Before taking DS, it is important to consult a professional nutritionist or obstetrician. | 92.3 |
| DS can cause nausea, vomiting, and symptoms of constipation and indigestion. | 36.7 |
| Taking DS during pregnancy is very important. | 84.3 |
| I can judge from the nutrition label of the DS whether it is suitable for my own use. | 53.3 |
| Variables | β | Wald χ2 | OR (95% CI) | p |
|---|---|---|---|---|
| Educational level (vs. Junior high school and below) | 11.338 | |||
| High school | 1.090 | 2.362 | 2.975 (0.741, 11.947) | 0.124 |
| Bachelor degree and above | 1.899 | 7.894 | 6.680 (1.776, 25.124) | 0.005 |
| Gestational stage (vs. First trimester) | 24.765 | |||
| Second trimester | 2.156 | 24.713 | 8.633 (3.690, 20.195) | <0.001 |
| Third trimester | 1.987 | 16.105 | 7.293 (2.764, 19.248) | <0.001 |
| ART conception vs. Natural conception | 1.278 | 9.298 | 3.588 (1.578, 8.158) | 0.002 |
| Number of antenatal visits (vs. ≤5) | 7.142 | |||
| 6 to 10 | 0.510 | 4.467 | 1.665 (1.038, 2.671) | 0.035 |
| ≥11 | 1.004 | 5.921 | 2.728 (1.216, 6.124) | 0.015 |
| Hypothyroidism (yes vs. no) | 0.658 | 4.956 | 1.931 (1.082, 3.446) | 0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, C.; Luo, J.; Yang, G.; Sun, M.; Liu, H.; Yang, Q.; Ouyang, Y.; Xi, Y.; Yong, C.; Khan, M.J.; et al. Dietary Supplement Use during Pregnancy: Perceptions versus Reality. Int. J. Environ. Res. Public Health 2022, 19, 4063. https://doi.org/10.3390/ijerph19074063
Xiang C, Luo J, Yang G, Sun M, Liu H, Yang Q, Ouyang Y, Xi Y, Yong C, Khan MJ, et al. Dietary Supplement Use during Pregnancy: Perceptions versus Reality. International Journal of Environmental Research and Public Health. 2022; 19(7):4063. https://doi.org/10.3390/ijerph19074063
Chicago/Turabian StyleXiang, Caihong, Jing Luo, Guilian Yang, Minghui Sun, Hanmei Liu, Qiping Yang, Yufeng Ouyang, Yue Xi, Cuiting Yong, Muhammad Jamal Khan, and et al. 2022. "Dietary Supplement Use during Pregnancy: Perceptions versus Reality" International Journal of Environmental Research and Public Health 19, no. 7: 4063. https://doi.org/10.3390/ijerph19074063
APA StyleXiang, C., Luo, J., Yang, G., Sun, M., Liu, H., Yang, Q., Ouyang, Y., Xi, Y., Yong, C., Khan, M. J., & Lin, Q. (2022). Dietary Supplement Use during Pregnancy: Perceptions versus Reality. International Journal of Environmental Research and Public Health, 19(7), 4063. https://doi.org/10.3390/ijerph19074063