
The Effect of Cone-Beam Computed Tomography (CBCT) Evaluation on Treatment Planning after Endodontic Instrument Fracture


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical and Initial Radiographic Examination
- Maxillary and mandibular molars with instrument fracture in the mesial root
- Informed consent by patients who wish to participate in the study
- Patients with a contributory severe medical history such as immunocompromised patients or patients with a history of radiation involving the jaws.
- Tooth/teeth of interest;
- Root and canal with instrument fracture;
- Location of the fragment (cervical, middle, middle-apical, apical third);
- Presence of periapical, lateral or furcation lesion;
- Presence of signs (sinus tract, swelling) and symptoms.
2.2. CBCT Examination and Imaging Protocol
2.3. Statistical Analysis
3. Results
4. Discussion
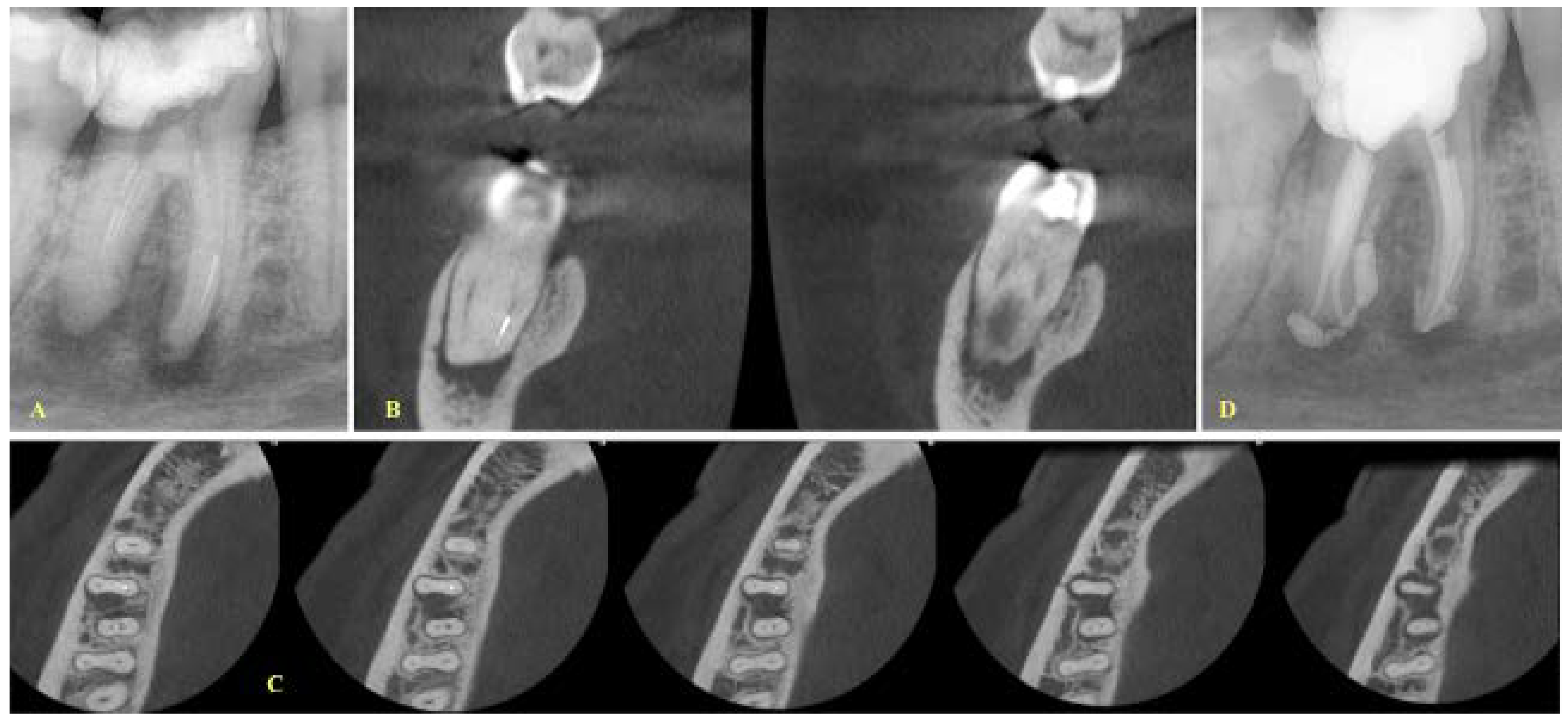
- If a lesion was present, the canals were separate and the fragment was located at the apical level, and a final treatment plan of bypassing the fragment was set (Figure 1).
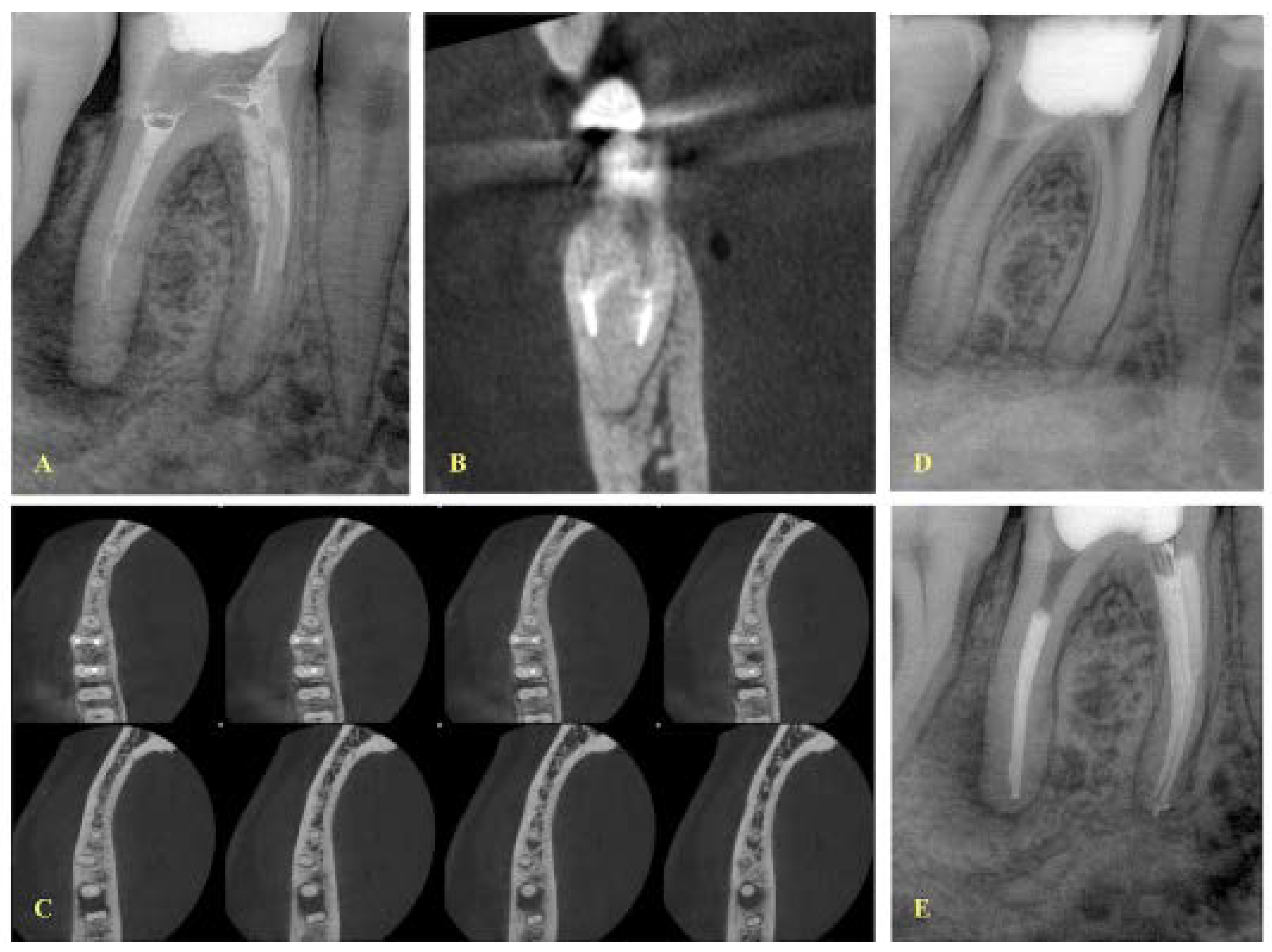
- If the fragment was located at the middle level, the canals were separate and the curvature was not severe as indicated after evaluation of the coronal CBCT images; then, a removal attempt was made, especially in cases where the length of the fragment was short (Figure 2).
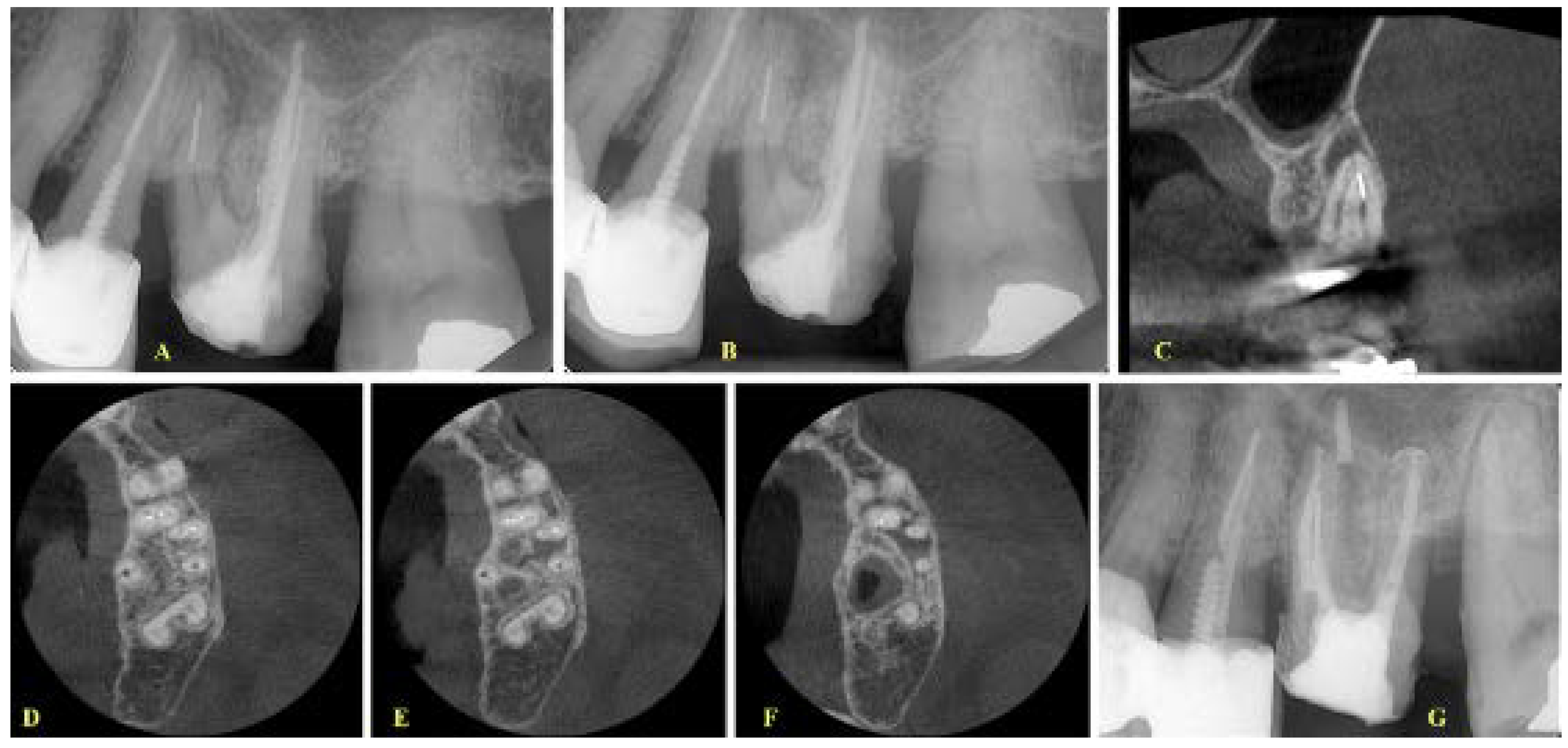
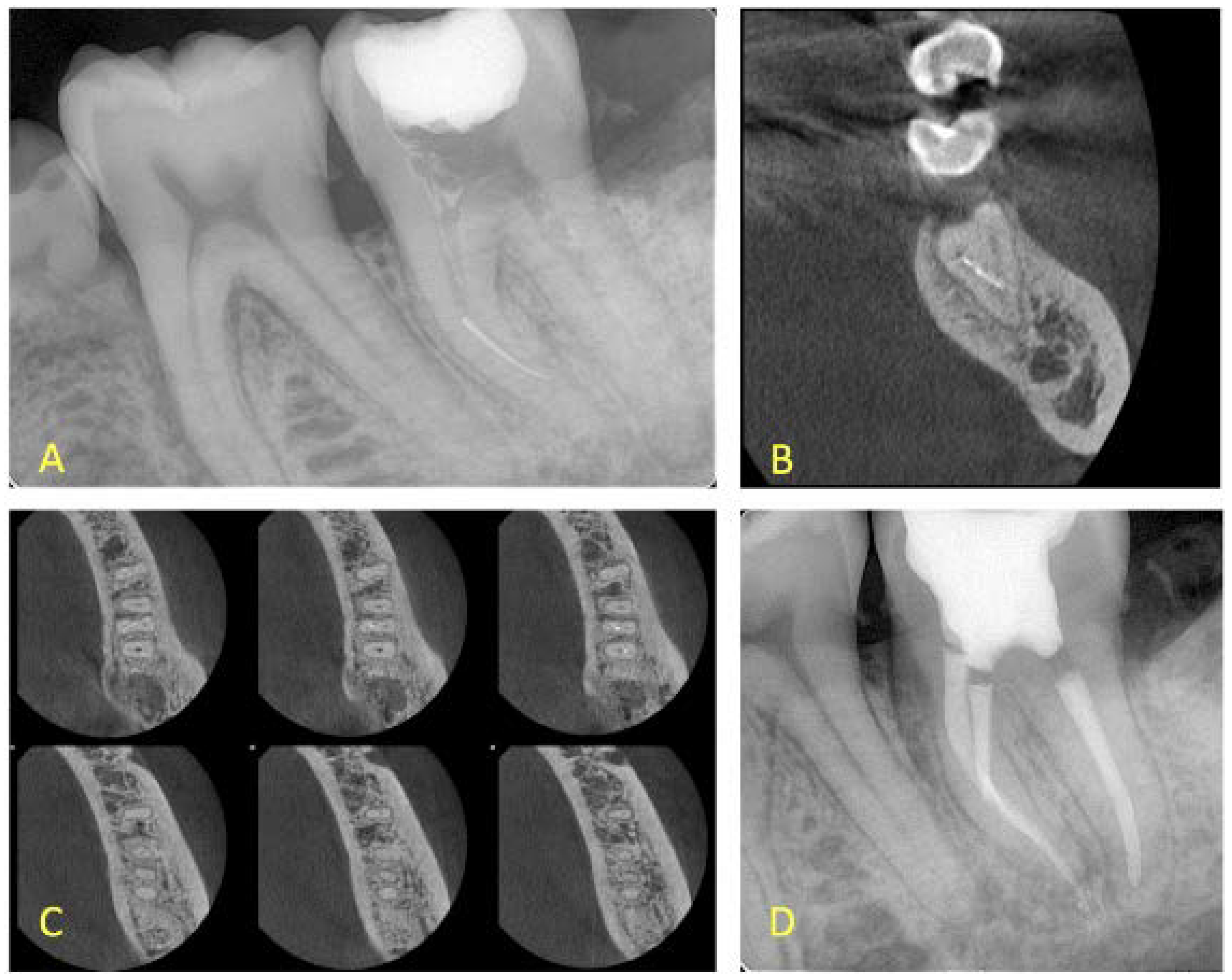
- In cases where the canals were merging, then a final treatment plan of leaving the fragment in situ was set, irrespective of the presence or absence of lesions (Figure 3 and Figure 4). The only occasion that would induce a modification to this treatment plan (i.e., leave the fragment in situ) was to conclude, after CBCT assessment and evaluation of canal curvature, that the removal of the fragment located at the middle level of the root would not be of a high difficulty degree procedure (Figure 5).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parashos, P.; Messer, H.H. Rotary NiTi instrument fracture and its consequences. J. Endod. 2006, 32, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Hülsmann, M.; Schinkel, I. Influence of several factors on the success or failure of removal of fractured instruments from the root canal. Endod. Dent. Traumatol. 1999, 15, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Spili, P.; Parashos, P.; Messer, H.H. The impact of instrument fracture on outcome of endodontic treatment. J. Endod. 2005, 31, 845–850. [Google Scholar] [CrossRef]
- Tzanetakis, G.N.; Kontakiotis, E.G.; Maurikou, D.V.; Marzelou, M.P. Prevalence and management of instrument fracture in the postgraduate endodontic program at the Dental School of Athens: A five-year retrospective clinical study. J. Endod. 2008, 34, 675–678. [Google Scholar] [CrossRef]
- Ungerechts, C.; Bårdsen, A.; Fristad, I. Instrument fracture in root canals—Where, why, when and what? A study from a student clinic. Int. Endod. J. 2014, 47, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Peng, P.; Cheung, G.S. Factors associated with the removal of fractured NiTi instruments from root canal systems. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 605–610. [Google Scholar] [CrossRef]
- Verma, P.; Love, R.M. A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int. Endod. J. 2011, 44, 210–217. [Google Scholar] [CrossRef]
- Lee, J.K.; Yoo, Y.J.; Perinpanayagam, H.; Ha, B.H.; Lim, S.M.; Oh, S.R.; Gu, Y.; Chang, S.W.; Zhu, Q.; Kum, K.Y. Three-dimensional modelling and concurrent measurements of root anatomy in mandibular first molar mesial roots using micro-computed tomography. Int. Endod. J. 2015, 48, 380–389. [Google Scholar] [CrossRef]
- Spagnuolo, G.; Ametrano, G.; D’Antò, V.; Formisano, A.; Simeone, M.; Riccitiello, F.; Amato, M.; Rengo, S. Microcomputed tomography analysis of mesiobuccal orifices and major apical foramen in first maxillary molars. Open Dent. J. 2012, 6, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Panitvisai, P.; Parunnit, P.; Sathorn, C.; Messer, H.H. Impact of a retained instrument on treatment outcome: A systematic review and meta-analysis. J. Endod. 2010, 36, 775–780. [Google Scholar] [CrossRef]
- Nevares, G.; Cunha, R.S.; Zuolo, M.L.; Bueno, C.E. Success rates for removing or bypassing fractured instruments: A prospective clinical study. J. Endod. 2012, 38, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Souter, N.J.; Messer, H.H. Complications associated with fractured file removal using an ultrasonic technique. J. Endod. 2005, 31, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Madarati, A.A.; Hunter, M.J.; Dummer, P.M. Management of intracanal separated instruments. J. Endod. 2013, 39, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE) developed by. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Salehi, S.K.; Horner, K. Impact of cone beam computed tomography (CBCT) on diagnostic thinking in endodontics of posterior teeth: A before-after study. J. Dent. 2016, 53, 57–63. [Google Scholar] [CrossRef]
- Ee, J.; Fayad, M.; Johnson, B. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J. Endod. 2014, 40, 910–916. [Google Scholar] [CrossRef]
- Mota de Almeida, F.J.; Knutsson, K.; Flygare, L. The impact of cone beam computed tomography on the choice of endodontic diagnosis. Int. Endod. J. 2015, 48, 564–572. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, G.; Abella, F.; Duràn-Sindreu, F.; Patel, S.; Roig, M. Influence of cone-beam computed tomography in clinical decision-making among specialists. J. Endod. 2017, 43, 194–199. [Google Scholar] [CrossRef]
- Rodríguez, G.; Patel, S.; Durán-Sindreu, F.; Roig, M.; Abella, F. Influence of cone-beam computed tomography on endodontic retreatment strategies among general dental practitioners and endodontists. J. Endod. 2017, 43, 1433–1437. [Google Scholar] [CrossRef]
- Viana Wanzeler, A.M.; Montagner, F.; Vieira, H.T.; Dias da Silveira, H.L.; Arús, N.A.; Vizzotto, M.B. Can cone-beam computed tomography change endodontists’ level of confidence in diagnosis and treatment planning? a before and after study. J. Endod. 2020, 46, 283–288. [Google Scholar] [CrossRef]
- Baratto-Filho, F.; Vavassori de Freitas, J.; Fagundes Tomazinho, F.S.; Leão Gabardo, M.C.; Mazzi-Chaves, J.F.; Damião Sousa-Neto, M. Cone-Beam Computed Tomography Detection of Separated Endodontic Instruments. J. Endod. 2020, 46, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Venezia, N.B.; Kamburoglu, K.; Meirowitz, A.; Ziv-Baran, T. A comparison of cone-beam computed tomography with periapical radiography in the detection of separated instruments retained in the apical third of root canal-filled teeth. J. Endod. 2016, 42, 1035–1039. [Google Scholar] [CrossRef] [PubMed]
- Ramos Brito, A.C.; Verner, F.S.; Junqueira, R.B.; Yamasaki, M.C.; Queiroz, P.M.; Freitas, D.Q. Detection of fractured endodontic instruments in root canals: Comparison between different digital radiography systems and cone-beam computed tomography. J. Endod. 2017, 43, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.D.; Brasil, D.M.; Queiroz, P.M.; Verner, F.S.; Junqueira, R.B.; Freitas, D.Q. Use of the metal artefact reduction tool in the identification of fractured endodontic instruments in cone-beam computed tomography. Int. Endod. J. 2020, 53, 506–512. [Google Scholar] [CrossRef]
- Rosado, L.P.L.; Fagundes, F.B.; Freitas, D.Q.; Oliveira, M.L.; Neves, F.S. Influence of the Intracanal Material and Metal Artifact Reduction Tool in the Detection of the Second Mesiobuccal Canal in Cone-beam Computed Tomographic Examinations. J. Endod. 2020, 46, 1067–1073. [Google Scholar] [CrossRef]
- Özer, S.Y.; Özkan, G.; Çetin, E.; Özkan, H.D. A comparative study of cone-beam computed tomography and periapical radiographs in decision-making after endodontic instrument fractures. Int. J. Artif. Organs 2017, 40, 510–514. [Google Scholar] [CrossRef]
- Chogle, S.; Zuaitar, M.; Sarkis, R.; Saadoun, M.; Mecham, A.; Zhao, Y. The recommendation of cone-beam computed tomography and its effect on endodontic diagnosis and treatment planning. J. Endod. 2020, 46, 162–168. [Google Scholar] [CrossRef]
- Madarati, A.A.; Qualtrough, A.J.; Watts, D.C. Vertical fracture resistance of roots after ultrasonic removal of fractured instruments. Int. Endod. J. 2010, 43, 424–429. [Google Scholar] [CrossRef]
- de Pablo, O.V.; Estevez, R.; Péix Sánchez, M.; Heilborn, C.; Cohenca, N. Root anatomy and canal configuration of the permanent mandibular first molar: A systematic review. J. Endod. 2010, 36, 1919–1931. [Google Scholar] [CrossRef]
- Gao, Y.; Shen, Y.; Zhou, X.; Haapasalo, M. Remaining root dentin thickness in mesiobuccal canals of maxillary first molars after attempted removal of broken instrument fragments. Aust. Endod. J. 2015, 41, 122–127. [Google Scholar] [CrossRef]
- Greenland, S. On sample-size and power calculations for studies using confidence intervals. Am. J. Epidemiol. 1988, 128, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.H.; Bates, M.N. Confidence limit analyses should replace power calculations in the interpretation of epidemiologic studies. Epidemiology 1992, 3, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Abdinian, M.; Moshkforoush, S.; Hemati, H.; Soltani, P.; Moshkforoushan, M.; Spagnuolo, G. Comparison of Cone Beam Computed Tomography and Digital Radiography in Detecting Separated Endodontic Files and Strip Perforation. Appl. Sci. 2020, 10, 8726. [Google Scholar] [CrossRef]
- Venskutonis, T.; Plotino, G.; Juodzbalys, G.; Mickevičienė, L. The importance of cone-beam computed tomography in the management of endodontic problems: A review of the literature. J. Endod. 2014, 40, 1895–1901. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Change in Treatment Planning | p-Value | ||||||
|---|---|---|---|---|---|---|---|
| No | Yes | Total | |||||
| N | % | N | % | N | % | ||
| Tooth (molar) | 0.25 * | ||||||
| Mandibular (mesial root) | 14 | 38.9 | 22 | 61.1 | 36 | 100.0 | |
| Maxillary (mesiobuccal root) | 9 | 56.3 | 7 | 43.7 | 16 | 100.0 | |
| Canal location | 0.01 # | ||||||
| Mesiobuccal (mandibular) | 12 | 48.0 | 13 | 52.0 | 25 | 100.0 | |
| One Mesiobuccal (maxillary) 1 | 9 | 69.2 | 4 | 30.8 | 13 | 100.0 | |
| Mesiobuccal & mesiolingual (mandibular) 2 | 1 | 100.0 | 0 | 0.0 | 1 | 100.0 | |
| Mesiolingual (mandibular) | 1 | 10.0 | 9 | 90.0 | 10 | 100.0 | |
| Single canal (maxillary) 3 | 0 | 0.0 | 3 | 100.0 | 3 | 100.0 | |
| Location (across root length) | <0.01 # | ||||||
| Cervical | 2 | 100.0 | 0 | 0.0 | 2 | 100.0 | |
| Middle | 12 | 92.3 | 1 | 7.7 | 13 | 100.0 | |
| Middle-apical | 4 | 40.0 | 6 | 60.0 | 10 | 100.0 | |
| Apical | 5 | 18.5 | 22 | 81.5 | 27 | 100.0 | |
| Canal merge | 0.26 # | ||||||
| No | 11 | 52.4 | 10 | 47.6 | 21 | 100.0 | |
| Yes | 12 | 42.9 | 16 | 57.1 | 28 | 100.0 | |
| Single canal | 0 | 0.0 | 3 | 100.0 | 3 | 100.0 | |
| Presence of lesion | 0.71 # | ||||||
| No | 3 | 33.3 | 6 | 66.7 | 9 | 100.0 | |
| Yes | 20 | 46.5 | 23 | 53.5 | 43 | 100.0 | |
| Presence of symptoms | 0.63 * | ||||||
| No | 5 | 38.5 | 8 | 61.5 | 13 | 100.0 | |
| Yes | 18 | 46.2 | 21 | 53.8 | 39 | 100.0 | |
| Total | 23 | 44.2 | 29 | 55.8 | 52 | 100.0 | |
| Conventional Periapical Radiography AssessmentN (%) | Total | p-Value * | ||||
|---|---|---|---|---|---|---|
| Retain Instrument w/o Bypass | Removal of Instrument | Bypass of Instrument | <0.001 | |||
| CBCT assessment N (%) | Retain instrument w/o bypass | 0 (0.0) | 4 (16.0) | 18 (66.7) | 22 (42.3) | |
| Removal of instrument | 0 (0.0) | 19 (76.0) | 5 (18.5) | 24 (46.2) | ||
| Bypass of instrument | 0 (0.0) | 2 (8.0) | 4 (14.8) | 6 (11.5) | ||
| Total | 0 (0.0) | 25 (100.0) | 27 (100.0) | 52 (100.0) | ||
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95%CI | p-Value | Odds Ratio | 95%CI | p-Value | |
| Tooth/jaw | 0.25 | |||||
| Mandibular | Reference | |||||
| Maxillary | 0.49 | 0.15, 1.63 | ||||
| Location of breakage | <0.001 | <0.001 | ||||
| More cervically | Reference | Reference | ||||
| Apically | 11.31 | 3.07, 41.76 | 11.31 | 3.07, 41.76 | ||
| Canal merge | 0.51 | |||||
| No | Reference | |||||
| Yes | 1.47 | 0.47, 4.57 | ||||
| Lesion | 0.47 | |||||
| No | Reference | |||||
| Yes | 0.58 | 0.13, 2.60 | ||||
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95%CI | p-Value | Odds Ratio | 95%CI | p-Value | |
| Tooth/jaw | 0.02 | 0.05 | ||||
| Mandibular | Reference | Reference | ||||
| Maxillary | 6.88 | 1.33, 35.58 | 7.26 | 0.99, 53.19 | ||
| Location of breakage | 0.002 | 0.003 | ||||
| More cervically | Reference | Reference | ||||
| Apically | 0.12 | 0.03, 0.45 | 0.03 | 0.003, 0.30 | ||
| Canal merge | 0.01 | 0.01 | ||||
| No | Reference | Reference | ||||
| Yes | 0.20 | 0.06, 0.71 | 0.05 | 0.01, 0.52 | ||
| Lesion | 0.48 | |||||
| No | Reference | |||||
| Yes | 1.69 | 0.39, 7.26 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalogeropoulos, K.; Xiropotamou, A.; Koletsi, D.; Tzanetakis, G.N. The Effect of Cone-Beam Computed Tomography (CBCT) Evaluation on Treatment Planning after Endodontic Instrument Fracture. Int. J. Environ. Res. Public Health 2022, 19, 4088. https://doi.org/10.3390/ijerph19074088
Kalogeropoulos K, Xiropotamou A, Koletsi D, Tzanetakis GN. The Effect of Cone-Beam Computed Tomography (CBCT) Evaluation on Treatment Planning after Endodontic Instrument Fracture. International Journal of Environmental Research and Public Health. 2022; 19(7):4088. https://doi.org/10.3390/ijerph19074088
Chicago/Turabian StyleKalogeropoulos, Konstantinos, Alexandra Xiropotamou, Despina Koletsi, and Giorgos N. Tzanetakis. 2022. "The Effect of Cone-Beam Computed Tomography (CBCT) Evaluation on Treatment Planning after Endodontic Instrument Fracture" International Journal of Environmental Research and Public Health 19, no. 7: 4088. https://doi.org/10.3390/ijerph19074088
APA StyleKalogeropoulos, K., Xiropotamou, A., Koletsi, D., & Tzanetakis, G. N. (2022). The Effect of Cone-Beam Computed Tomography (CBCT) Evaluation on Treatment Planning after Endodontic Instrument Fracture. International Journal of Environmental Research and Public Health, 19(7), 4088. https://doi.org/10.3390/ijerph19074088