
Resilience-Building for Mental Health among Early Childhood Educators: A Systematic Review and Pilot-Study towards an EEG-VR Resilience Building Intervention

 ,
,  , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
1.1. Challenges of the Workload on Mental Health of Teachers
1.2. Role of Resilience in Supporting Early Childhood Teachers
1.3. Rationale and Objective of Review
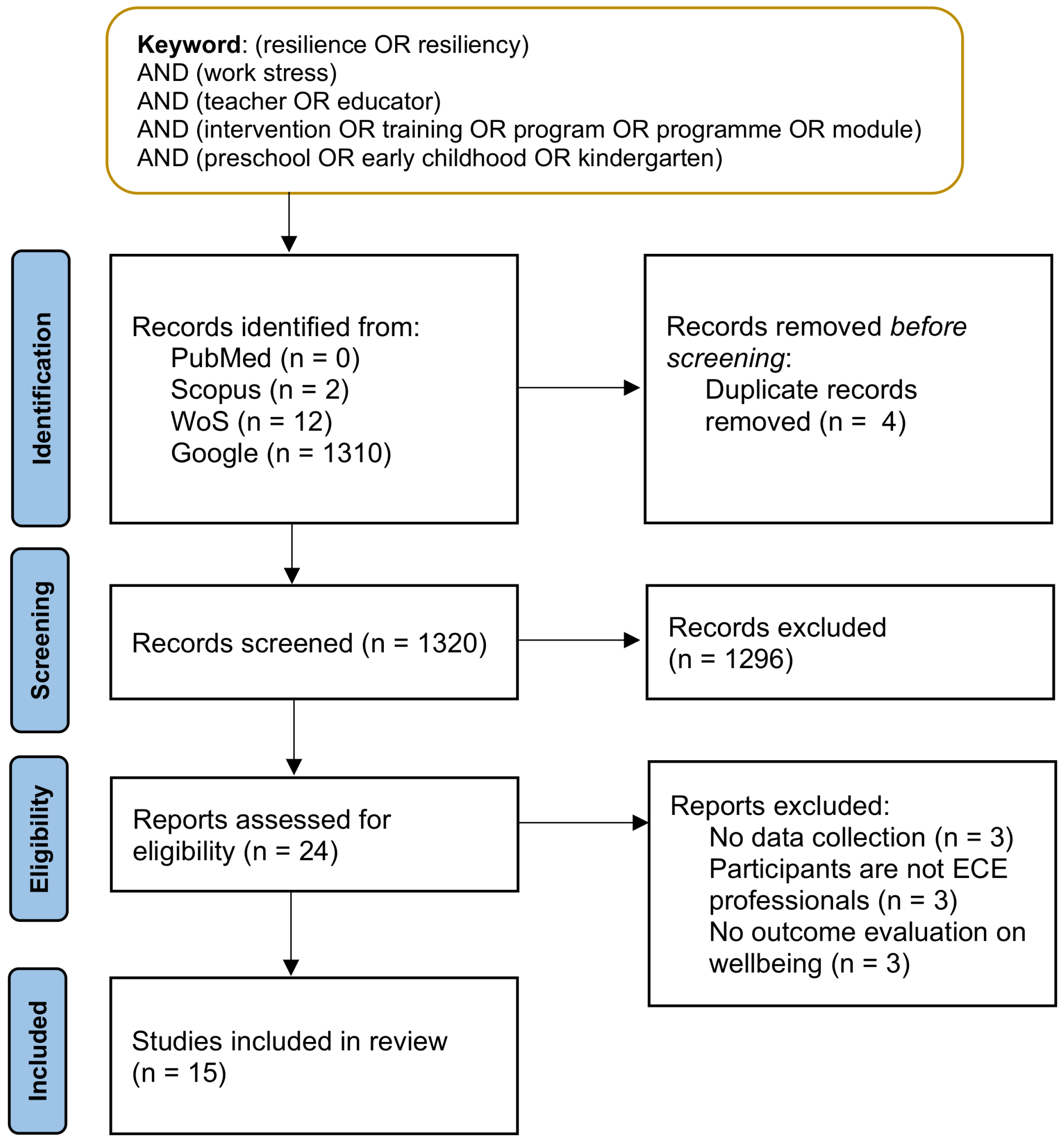
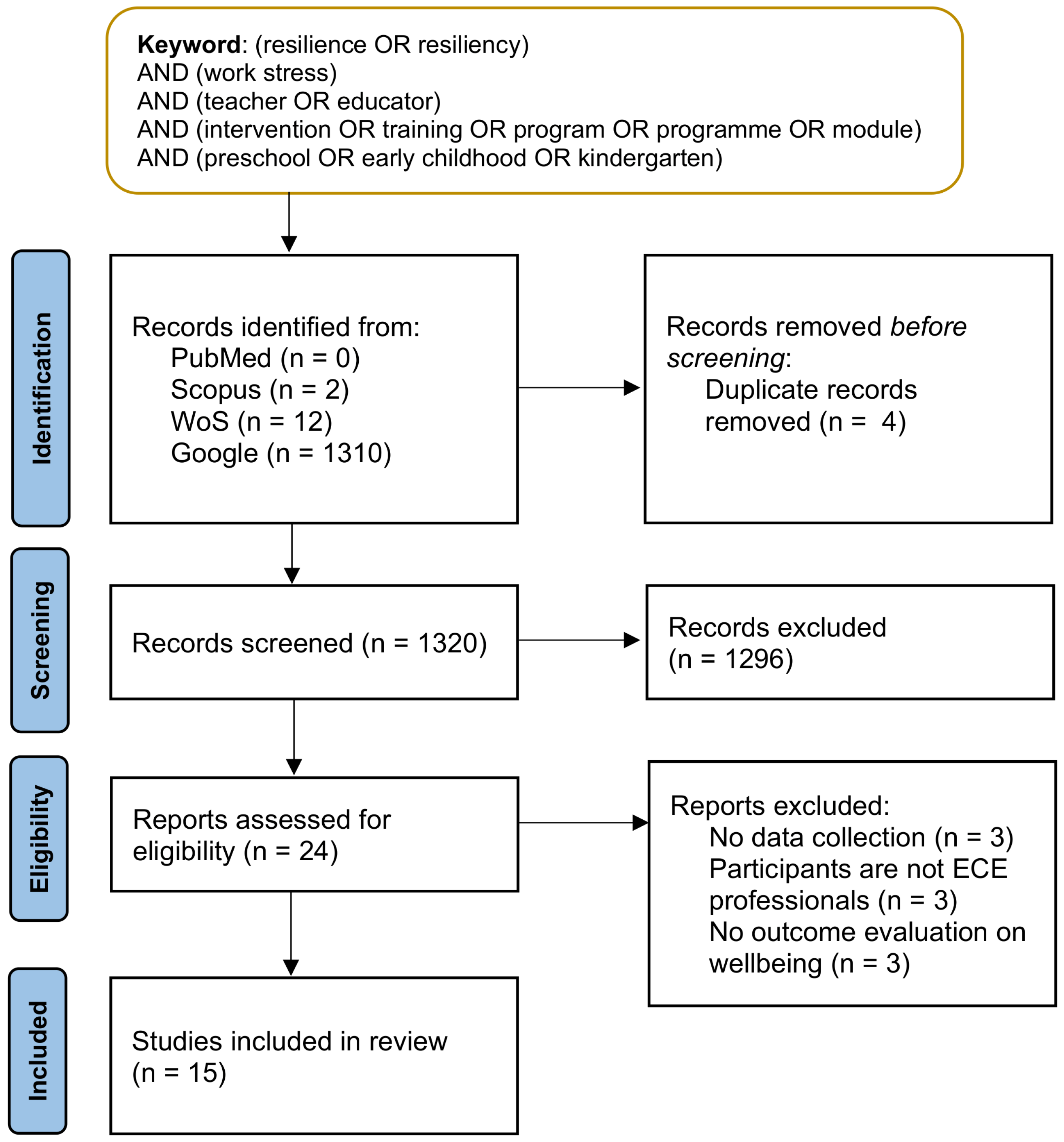
2. Methodology
2.1. Search Strategy and Eligibility Criteria
- 1.
- The study must include training or interventions to develop resilience or psychosocial well-being of professionals in an ECE setting to withstand or recover from stress or adversity faced at work;
- 2.
- The study must involve data collection involving in-service teachers working in ECE settings;
- 3.
- The study must evaluate the outcome of the intervention based on changes in well-being, mental health, or performance outcomes of participants;
- 4.
- The study is originally written in the English language.
2.2. Study Selection
3. Results
3.1. Overview of Interventions in Selected Studies
3.2. Duration and Frequency of Intervention
3.3. Interventions Based on Needs Assessment
3.4. Participant Characteristics
3.5. Instruments for Resilience, Well-Being, and Work Stress Measures
4. Key Findings and Proposed Direction
4.1. Key Findings of Systematic Review
4.1.1. Psychological Assessment as a Main Measure for Well-Being and Mental Health
4.1.2. Concerns of Response Bias in Self-Report Assessments
4.1.3. Challenges in the Group-Approach Intervention: Lengthy Period and Attrition
4.1.4. Balancing between Multi-Centre and Needs-Based Interventions
4.2. Proposed Direction for Resilience-Building and Work Stress-Management Programs through Physiological Measures
5. Pilot Study towards an EEG-VR Resilience-Building Intervention
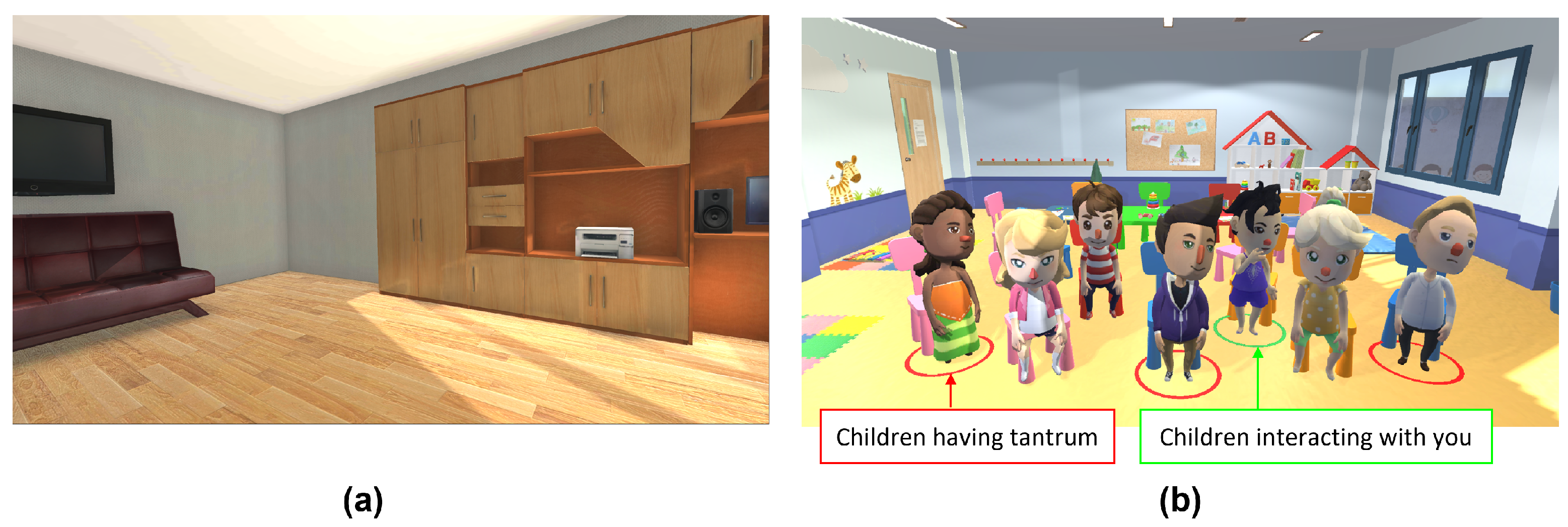
5.1. Setup of Virtual Classroom
- 1.
- 2 minutes of resting condition in a virtual enclosed room;
- 2.
- 4 minutes of mental task condition in a virtual classroom;
- 3.
- 2 minutes of resting condition in a virtual enclosed room;
- 4.
- 4 minutes of mental task condition in a virtual classroom.
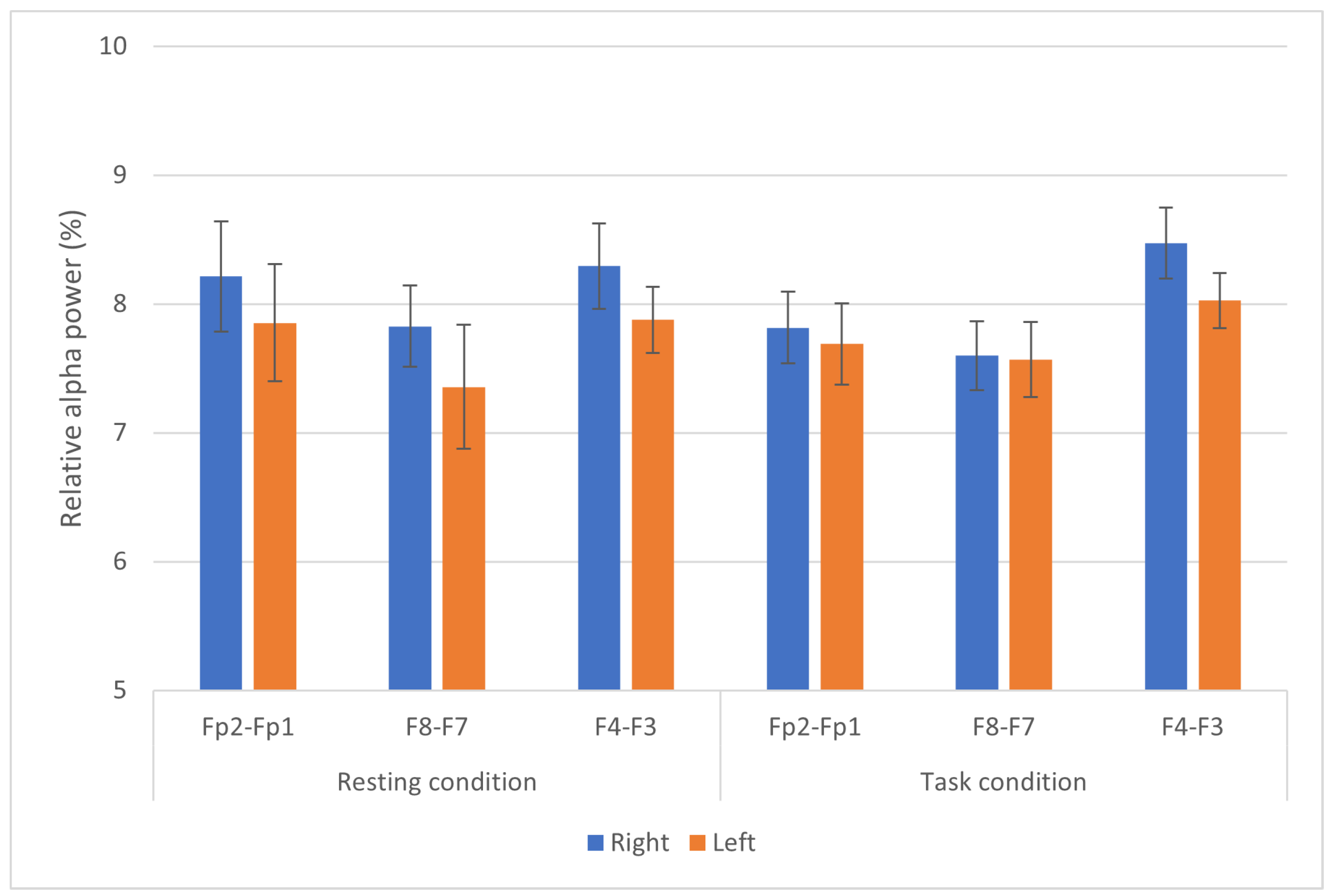
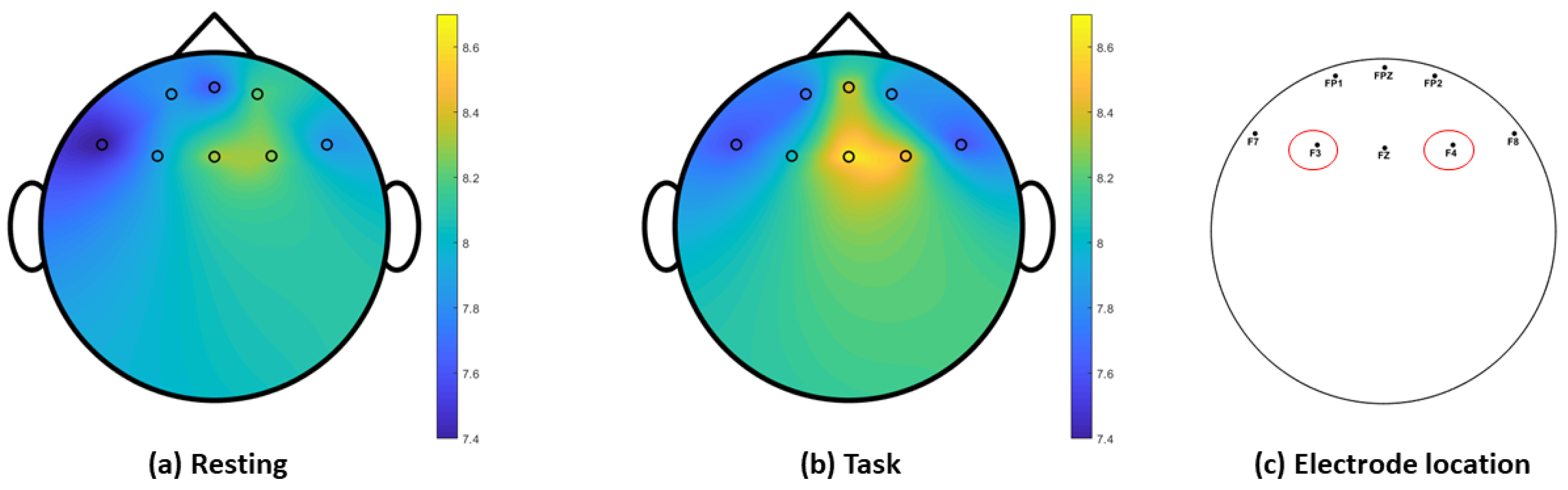
5.2. EEG Recording and Processing
- 1.
- Band-pass filtering between 1 and 45 Hz EEG signals to remove power-line noise;
- 2.
- 3.
- 4.
- Computation of relative alpha power [87] for both resting and task conditions.
- 5.
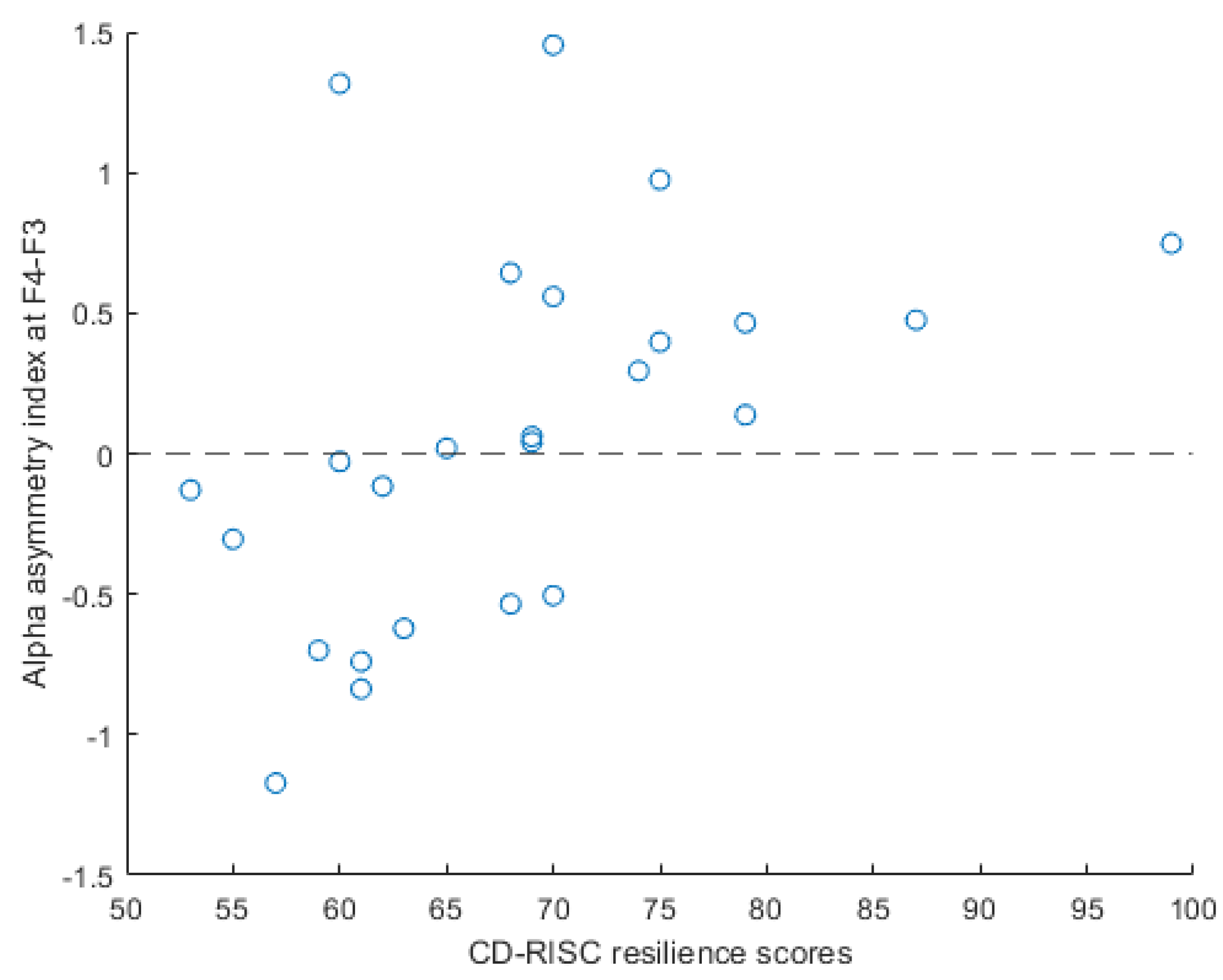
5.3. Statistical Analysis
5.4. Preliminary Findings
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harnois, G.; Gabriel, P. Mental Health and Work: Impact, Issues and Good Practices; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Feltoe, G.; Beamish, W.; Davies, M. Secondary School Teacher Stress and Coping: Insights from Queensland, Australia. Int. J. Arts Sci. 2016, 9, 597–608. [Google Scholar]
- Fink, G. Stress: Concepts, Cognition, Emotion, and Behavior: Handbook of Stress Series, Volume 1; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Kassim, M.S.A.; Ismail, A.; Ismail, R. A Review of Occupational Stress Prevalence and its Predictors among Selected Working Populations in Malaysia. Malays. J. Public Health Med. 2018, 18, 1–6. [Google Scholar]
- Menon, J. Depression on the Rise as Malaysians Burn Out from sTress, Expert Warns. MalayMail. 2016. Available online: https://www.malaymail.com/news/malaysia/2016/03/24/depression-on-the-rise-as-malaysians-burn-out-from-stress-expert-warns/1086087 (accessed on 14 August 2019).
- Badawy, S.M. Egyptian Teachers’ Burnout: The Role of Work Environment Characteristics and Job Stress. J. Bus. Manag. Sci. 2015, 3, 101–110. [Google Scholar] [CrossRef]
- Desouky, D.; Allam, H. Occupational stress, anxiety and depression among Egyptian teachers. J. Epidemiol. Glob. Health 2017, 7, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Jepson, E.; Forrest, S. Individual contributory factors in teacher stress: The role of achievement striving and occupational commitment. Br. J. Educ. Psychol. 2006, 76, 183–197. [Google Scholar] [CrossRef]
- Johnson, S.; Cooper, C.; Cartwright, S.; Donald, I.; Taylor, P.; Millet, C. The experience of work-related stress across occupations. J. Manag. Psychol. 2005, 20, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Rentner, D.S.; Kober, N.; Frizzell, M.; Ferguson, M. Listen to Us: Teacher Views and Voices; Center on Education Policy: Washington, DC, USA, 2016. [Google Scholar]
- Kwon, K.A.; Jeon, S.; Jeon, L.; Castle, S. The role of teachers’ depressive symptoms in classroom quality and child developmental outcomes in Early Head Start programs. Learn. Individ. Differ. 2019, 74, 101748. [Google Scholar] [CrossRef]
- Linnan, L.; Arandia, G.; Bateman, L.A.; Vaughn, A.; Smith, N.; Ward, D. The Health and Working Conditions of Women Employed in Child Care. Int. J. Env. Res Public Health 2017, 14, 1–14. [Google Scholar] [CrossRef]
- Whitaker, R.C.; Dearth-Wesley, T.; Gooze, R.A. Workplace stress and the quality of teacher-children relationships in Head Start. Early Child. Res. Q. 2015, 30, 57–69. [Google Scholar] [CrossRef]
- Hall-Kenyon, K.M.; Bullough, R.V.; MacKay, K.L.; Marshall, E.E. Preschool Teacher Well-Being: A Review of the Literature. Early Child. Educ. J. 2014, 42, 153–162. [Google Scholar] [CrossRef]
- Sandilos, L.E.; Cycyk, L.M.; Hammer, C.S.; Sawyer, B.E.; López, L.; Blair, C. Depression, Control, and Climate: An Examination of Factors Impacting Teaching Quality in Preschool Classrooms. Early Educ. Dev. 2015, 26, 1111–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, E.; Fung, L.; Chow, L. Sources and Manifestations of Stress in Female Kindergarten Teachers. Int. Educ. J. 2006, 7, 364–370. [Google Scholar]
- Zinsser, K.M.; Christensen, C.G.; Torres, L. She’s supporting them; who’s supporting her? Preschool center-level social-emotional supports and teacher well-being. J. Sch. Psychol. 2016, 59, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Mantzicopoulos, P. Conflictual relationships between kindergarten children and their teachers: Associations with child and classroom context variables. J. Sch. Psychol. 2005, 43, 425–442. [Google Scholar] [CrossRef]
- Sandilos, L.E.; Goble, P.; Rimm-Kaufman, S.E.; Pianta, R.C. Does professional development reduce the influence of teacher stress on teacher-child interactions in pre-kindergarten classrooms? Early Child. Res. Q. 2018, 42, 280–290. [Google Scholar] [CrossRef]
- Mustafa, L.M.; Azman, M.N.A. Preschool Education in Malaysia: Emerging Trends and Implications for the Future. Am. J. Econ. 2013, 3, 347–351. [Google Scholar] [CrossRef]
- Ambotang, A.S.; Hashim, M.H.M. The Relation of Work Environment and Stress in Classroom Management among Preschool Teachers. J. Techno-Soc. 2010, 2, 69–81. [Google Scholar]
- Majzub, R.M. Critical Issues in Preschool Education in Malaysia. In Recent Advances in Educational Technologies; WSEAS Press: Cambridge, MA, USA, 2013; pp. 150–155. [Google Scholar]
- Cumming, T.; Logan, H.; Wong, S. A critique of the discursive landscape: Challenging the invisibility of early childhood educators’ well-being. Contemp. Issues Early Child. 2020, 21, 96–110. [Google Scholar] [CrossRef]
- Jones, C.; Johnstone, M.; Hadley, F.; Waniganayake, M. Early childhood educators’ workplace well-being: It’s everyone’s right! Australas. J. Early Child. 2020, 45, 322–335. [Google Scholar] [CrossRef]
- Faulkner, M.; Gerstenblatt, P.; Lee, A.; Vallejo, V.; Travis, D. Childcare providers: Work stress and personal well-being. J. Early Child. Res. 2014, 14, 280–293. [Google Scholar] [CrossRef]
- Ismail, F.L.M.; Ismail, A.; Aziz, M.A.A.; Aziz, S.A.; Sharom, N.Q.; Ramlan, S.R. Service Quality of Public Preschool Education in Malaysia: Perceptions of Parents. Sains Insani 2018, 3, 28–37. [Google Scholar] [CrossRef]
- Grining, C.L.; Raver, C.C.; Champion, K.; Sardin, L.; Metzger, M.; Jones, S.M. Understanding and Improving Classroom Emotional Climate and Behavior Management in the “Real World”: The Role of Head Start Teachers’ Psychosocial Stressors. Early Educ. Dev. 2010, 21, 65–94. [Google Scholar] [CrossRef]
- Jennings, P.A.; Greenberg, M.T. The Prosocial Classroom: Teacher Social and Emotional Competence in Relation to Student and Classroom Outcomes. Rev. Educ. Res. 2009, 79, 491–525. [Google Scholar] [CrossRef]
- Cumming, T. Early Childhood Educators’ Well-Being: An Updated Review of the Literature. Early Child. Educ. J. 2017, 45, 583–593. [Google Scholar] [CrossRef]
- Gu, Q.; Day, C. Teachers resilience: A necessary condition for effectiveness. Teach. Teach. Educ. 2007, 23, 1302–1316. [Google Scholar] [CrossRef]
- Mansfield, C.F.; Beltman, S.; Broadley, T.; Weatherby-Fell, N. Building resilience in teacher education: An evidenced informed framework. Teach. Teach. Educ. 2016, 54, 77–87. [Google Scholar] [CrossRef]
- Kalisch, R.; Müller, M.B.; Tüscher, O. A conceptual framework for the neurobiological study of resilience. Behav. Brain Sci. 2015, 38, e92. [Google Scholar] [CrossRef]
- Gibbs, S.; Miller, A. Teachers’ resilience and well-being: A role for educational psychology. Teach. Teach. 2014, 20, 609–621. [Google Scholar] [CrossRef]
- Yao, Z.F.; Hsieh, S. Neurocognitive Mechanism of Human Resilience: A Conceptual Framework and Empirical Review. Int. J. Environ. Res. Public Health 2019, 16, 5123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhove, A.J.; Herian, M.N.; Perez, A.L.U.; Harms, P.D.; Lester, P.B. Can resilience be developed at work? A meta-analytic review of resilience-building programme effectiveness. J. Occup. Organ. Psychol. 2020, 89, 278–307. [Google Scholar] [CrossRef] [Green Version]
- Bokaba, J.N. The Development of a Personal Growth Programme to Address the Emotional Needs of Early Childhood Development Practitioners in Previously Disadvantaged Communities. Master’s Thesis, University of Pretoria, Pretoria, South Africa, 2011. [Google Scholar]
- Júníusdóttir, H.L. Enhancing Preschool Employees’ Wellbeing by Promoting Exercise Engagement during Working Hours. Master’s Thesis, Lund University, Lund, Sweden, 2015. [Google Scholar]
- Lepore, C.E. The Prevention of Preschool Teacher Stress: Using Mixed Methods to Examine the Impact of Reflective Supervision. Ph.D. Thesis, University of California, Oakland, CA, USA, 2015. [Google Scholar]
- Christian, E.M. The Effectiveness of the ACHIEVER Adult Resilience Curriculum in Promoting Teacher Wellbeing. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2017. [Google Scholar]
- Nilsson, M.; Andersson, I.; Blomqvist, K. Coexisting Needs: Paradoxes in Collegial Reflection–The Development of a Pragmatic Method for Reflection. Educ. Res. Int. 2017, 2017, 4851067. [Google Scholar] [CrossRef] [Green Version]
- Fulchini, A. Exploring Stress for Novice Teachers’ in Low Socio-Economic Elementary Schools Through Breathing Biofeedback. Ph.D. Thesis, University of Central Florida, Orlando, FL, USA, 2018. [Google Scholar]
- Killion, S.K. The Intersection of Mindfulness, Teacher Efficacy and School Climate: A Pilot Study. Ph.D. Thesis, University of Denver, Denver, CO, USA, 2019. [Google Scholar]
- Coggin, K.R. The Relationship between Mindfulness and School Leader Stress. Ph.D. Thesis, Texas A&M University, College Station, TX, USA, 2019. [Google Scholar]
- Lang, S.N.; Jeon, L.; Sproat, E.B.; Brothers, B.E.; Buettner, C.K. Social Emotional Learning for Teachers (SELF-T): A Short-term, Online Intervention to Increase Early Childhood Educators’ Resilience. Early Educ. Dev. 2020, 31, 1112–1132. [Google Scholar] [CrossRef]
- Hatton-Bowers, H.; Howell Smith, M.; Huynh, T.; Bash, K.; Durden, T.; Anthony, C.; Foged, J.; Lodl, K. “I Will Be Less Judgmental, More Kind, More Aware, and Resilient!”: Early Childhood Professionals’ Learnings from an Online Mindfulness Module. Early Child. Educ. J. 2020, 48, 379–391. [Google Scholar] [CrossRef]
- Susman-Stillman, A.; Lim, S.; Meuwissen, A.; Watson, C. Reflective Supervision/Consultation and Early Childhood Professionals’ Well-Being: A Qualitative Analysis of Supervisors’ Perspectives. Early Educ. Dev. 2020, 31, 1151–1168. [Google Scholar] [CrossRef]
- Bayly, B.L.; Dizon, E.; Shrestha, G.; Smith, C.L.; Tekle, S.; Rhoades Cooper, B. Leveraging self-determination theory to understand which preschool teachers benefit most from a professional development intervention. J. Early Child. Teach. Educ. 2020, 1–19. [Google Scholar] [CrossRef]
- Pianta, R.; Burchinal, M. National Center for Research on Early Childhood Education Teacher Professional Development Study (2007–2011); Technical Report; Inter-University Consortium for Political and Social Research: Ann Arbor, MI, USA, 2016. [Google Scholar] [CrossRef]
- Hepburn, S.J.; Carroll, A.; McCuaig-Holcroft, L. A Complementary Intervention to Promote Wellbeing and Stress Management for Early Career Teachers. Int. J. Environ. Res. Public Health 2021, 18, 6320. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.R.; Evarrs, S.; Knotek, S. The Impact of Behavioral Activation on Teacher Stress and Burnout: A Multiple Probe Single Case Design. Ph.D. Thesis, The University of North Carolina at Chapel Hill, Ann Arbor, MI, USA, 2021. [Google Scholar]
- Lejuez, C.W.; Hopko, D.R.; Acierno, R.; Daughters, S.B.; Pagoto, S.L. Ten Year Revision of the Brief Behavioral Activation Treatment for Depression: Revised Treatment Manual. Behav Modif 2011, 35, 111–161. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.T.; Carl, E.; Cuijpers, P.; Karyotaki, E.; Smits, J.A.J. Looking beyond depression: A meta-analysis of the effect of behavioral activation on depression, anxiety, and activation. Psychol. Med. 2020, 51, 1491–1504. [Google Scholar] [CrossRef] [PubMed]
- Mechelke, K.K.; Bloomberg, L. Strengthening Teachers’ Relationship-Building Skills: A Single Qualitative Case Study of a One-Day Enneagram Training. Ph.D. Thesis, Northcentral University, Ann Arbor, MI, USA, 2021. [Google Scholar]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Parker, P.D.; Martin, A.J.; Colmar, S.; Liem, G.A. Teachers’ workplace well-being: Exploring a process model of goal orientation, coping behavior, engagement, and burnout. Teach. Teach. Educ. 2012, 28, 503–513. [Google Scholar] [CrossRef]
- Berry, B. A Quantitative Study of Optimistic Explanatory Style as a Theoretical Pathway to Teacher Self-Efficacy. Ph.D. Thesis, Northcentral University, School of Psychology, San Diego, CA, USA, 2018. [Google Scholar]
- Arnsten, A.F.T. Stress weakens prefrontal networks: Molecular insults to higher cognition. Nat Neurosci. 2015, 18, 1376–1385. [Google Scholar] [CrossRef]
- Ursin, H.; Eriksen, H.R. The cognitive activation theory of stress. Psychoneuroendocrinology 2004, 29, 567–592. [Google Scholar] [CrossRef]
- Franklin, T.; Saab, B.; Mansuy, I. Neural Mechanisms of Stress Resilience and Vulnerability. Neuron 2012, 75, 747–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keynan, J.N.; Cohen, A.; Jackont, G.; Green, N.; Goldway, N.; Davidov, A.; Meir-Hasson, Y.; Raz, G.; Intrator, N.; Fruchter, E.; et al. Electrical fingerprint of the amygdala guides neurofeedback training for stress resilience. Nat. Hum. Behav. 2019, 3, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Peres, J.F.; Foerster, B.; Santana, L.G.; Fereira, M.D.; Nasello, A.G.; Savoia, M.; Moreira-Almeida, A.; Lederman, H. Police officers under attack: Resilience implications of an fMRI study. J. Psychiatr. Res. 2011, 45, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Reynaud, E.; Guedj, E.; Souville, M.; Trousselard, M.; Zendjidjian, X.; Khoury-Malhame, M.E.; Fakra, E.; Nazarian, B.; Blin, O.; Canini, F.; et al. Relationship between emotional experience and resilience: An fMRI study in fire-fighters. Neuropsychologia 2013, 51, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Mandrick, K.; Peysakhovich, V.; Rémy, F.; Lepron, E.; Causse, M. Neural and psychophysiological correlates of human performance under stress and high mental workload. Biol. Psychol. 2016, 121, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebner, K.; Singewald, N. Individual differences in stress susceptibility and stress inhibitory mechanisms. Curr. Opin. Behav. Sci. 2017, 14, 54–64. [Google Scholar] [CrossRef]
- Kong, F.; Wang, X.; Hu, S.; Liu, J. Neural correlates of psychological resilience and their relation to life satisfaction in a sample of healthy young adults. NeuroImage 2015, 123, 165–172. [Google Scholar] [CrossRef]
- Perez, B.Z.; Marin, M.M.; Perez, E.I. Developing a Virtual Environment for Safety Training. In Proceedings of the Electronics, Robotics and Automotive Mechanics Conference, Cuernavaca, Mexico, 25–28 September 2007; pp. 545–550. [Google Scholar] [CrossRef]
- Grajewski, D.; Górski, F.; Hamrol, A.; Zawadzki, P. Immersive and Haptic Educational Simulations of Assembly Workplace Conditions. Procedia Comput. Sci. 2015, 75, 359–368. [Google Scholar] [CrossRef] [Green Version]
- binti Sulaiman, S.; Ali, S.S.A.; Adil, S.H.; Ebrahim, M.; Raza, K. Virtual Reality Training and Skill Enhancement for Offshore Workers. In Proceedings of the 2020 International Conference on Computational Intelligence (ICCI), Bandar Seri Iskandar, Malaysia, 8–9 October 2020; pp. 287–292. [Google Scholar] [CrossRef]
- Allanson, J.; Mariani, J. Mind over virtual matter: Using virtual environments for neurofeedback training. In Proceedings of the IEEE Virtual Reality (Cat. No. 99CB36316), Houston, TX, USA, 13–17 March 1999; pp. 270–273. [Google Scholar] [CrossRef]
- Wiederhold, B.K.; Jang, D.P.; Kim, S.I.; Wiederhold, M.D. Physiological Monitoring as an Objective Tool in Virtual Reality Therapy. CyberPsychol. Behav. 2002, 5, 77–84. [Google Scholar] [CrossRef]
- Hoffman, H.G. Virtual Reality Therapy. Sci. Am. 2004, 291, 58–65. [Google Scholar] [CrossRef]
- Randeniya, N.; Ranjha, S.; Kulkarni, A.; Lu, G. Virtual Reality Based Maintenance Training Effectiveness Measures—A Novel Approach for Rail Industry. In Proceedings of the 2019 IEEE 28th International Symposium on Industrial Electronics (ISIE), Vancouver, BC, Canada, 12–14 June 2019; pp. 1605–1610. [Google Scholar] [CrossRef]
- Abu Hasan, R.; Sulaiman, S.; Ashykin, N.N.; Abdullah, M.N.; Hafeez, Y.; Ali, S.S.A. Workplace Mental State Monitoring during VR-Based Training for Offshore Environment. Sensors 2021, 21, 4885. [Google Scholar] [CrossRef]
- Wan, B.; Wang, Q.; Su, K.; Dong, C.; Song, W.; Pang, M. Measuring the Impacts of Virtual Reality Games on Cognitive Ability Using EEG Signals and Game Performance Data. IEEE Access 2021, 9, 18326–18344. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.; Smeets, T.; Giesbrecht, T.; Quaedflieg, C.W.; Smulders, F.T.; Meijer, E.H.; Merckelbach, H.L. The role of frontal EEG asymmetry in post-traumatic stress disorder. Biol. Psychol. 2015, 108, 62–77. [Google Scholar] [CrossRef]
- Brouwer, A.M.; Neerincx, M.A.; Kallen, V.; van der Leer, L.; ten Brinke, M. EEG Alpha Asymmetry, Heart Rate Variability and Cortisol in Response to Virtual Reality Induced Stress. J. Cybertherapy Rehabil. 2011, 4, 27–40. [Google Scholar]
- Pascalis, V.D.; Cozzuto, G.; Caprara, G.V.; Alessandri, G. Relations among EEG-alpha asymmetry, BIS/BAS, and dispositional optimism. Biol. Psychol. 2013, 94, 198–209. [Google Scholar] [CrossRef]
- Quaedflieg, C.; Meyer, T.; Smulders, F.; Smeets, T. The functional role of individual-alpha based frontal asymmetry in stress responding. Biol. Psychol. 2015, 104, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Behavior, U.H. Frontal Asymmetry 101—How to Get Insights on Motivation and Emotions from EEG; Technical Report; iMotions: Boston, MA, USA, 2017. [Google Scholar]
- Gabard-Durnam, L.J.; Mendez Leal, A.S.; Wilkinson, C.L.; Levin, A.R. The Harvard Automated Processing Pipeline for Electroencephalography (HAPPE): Standardized Processing Software for Developmental and High-Artifact Data. Front. Neurosci. 2018, 12, 97. [Google Scholar] [CrossRef] [PubMed]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, I.; Haufe, S.; Tangermann, M. Automatic Classification of Artifactual ICA-Components for Artifact Removal in EEG Signals. Behav. Brain Funct. 2011, 7, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayser, J.; Tenke, C.E. Principal components analysis of Laplacian waveforms as a generic method for identifying ERP generator patterns: I. Evaluation with auditory oddball tasks. Clin. Neurophysiol. 2006, 117, 348–368. [Google Scholar] [CrossRef] [PubMed]
- Kayser, J.; Tenke, C.E. Principal components analysis of Laplacian waveforms as a generic method for identifying ERP generator patterns: II. Adequacy of low-density estimates. Clin. Neurophysiol. 2006, 117, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Kayser, J. Current Source Density (CSD) Interpolation Using Spherical Splines—CSD Toolbox (Version 1.1); New York State Psychiatric Institute, Division of Cognitive Neuroscience: New York, NY, USA, 2009; Available online: http://psychophysiology.cpmc.columbia.edu/Software/CSDtoolbox (accessed on 1 January 2020).
- Li, G.; Huang, S.; Xu, W.; Jiao, W.; Jiang, Y.; Gao, Z.; Zhang, J. The impact of mental fatigue on brain activity: A comparative study both in resting state and task state using EEG. BMC Neurosci. 2020, 21, 20. [Google Scholar] [CrossRef]
- Davidson, J.R. Connor-Davidson Resilience Scale (CD-RISC) © Manual. Available online: www.cdrisc.com (accessed on 1 January 2020).
- Smith, E.E.; Reznik, S.J.; Stewart, J.L.; Allen, J.J.B. Assessing and conceptualizing frontal EEG asymmetry: An updated primer on recording, processing, analyzing, and interpreting frontal alpha asymmetry. Int. J. Psychophysiol. 2017, 111, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Zhang, Y.; Ge, Y.; Zheng, Y.; Sun, X.; Zhang, K. Asymmetric hemisphere activation in tenderness: Evidence from EEG signals. Sci. Rep. 2018, 8, 8029. [Google Scholar] [CrossRef] [PubMed]
- Zotev, V.; Yuan, H.; Misaki, M.; Phillips, R.; Young, K.D.; Feldner, M.T.; Bodurka, J. Correlation between amygdala BOLD activity and frontal EEG asymmetry during real-time fMRI neurofeedback training in patients with depression. Neuroimage Clin. 2016, 11, 224–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafeez, Y.; Ali, S.S.A.; Hasan, R.A.; Adil, S.H.; Moinuddin, M.; Ebrahim, M.; Yusoff, M.S.B.; Amin, H.; Al-Saggaf, U. Development of Enhanced Stimulus Content to Improve the Treatment Efficacy of EEG-Based Frontal Alpha Asymmetry Neurofeedback for Stress Mitigation. IEEE Access 2021, 9, 130638–130648. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approach | Study Location | Participants | Program | Instruments and Measures | Outcome of Intervention |
|---|---|---|---|---|---|
| Group, with facilitator [36] | Schools with Head Start program in 5 residential areas | ECE teachers | Personal Growth Programme designed by identified needs |
|
|
| Group [37] | Two preschools integrating employee exercise in work routine | Voluntary employees | Exercise program, 20 min group outdoor activity |
|
|
| Group [38] | Five early childhood care centres serving homeless or low-income families. | Experienced (>2 years of RS) and new (<1 year RS) teachers | Reflective supervision |
| Compared to novice group, experienced group had:
|
| Group [39] | Six elementary schools in a large urban district | Teachers between kindergarten and 5th grade | ACHIEVER Resilience Curriculum |
| Compared to control group, intervention group significantly improved in:
|
| Group [40] | One school from preschool to sixth grade classes | Teachers from preschool to sixth grade | Collegial reflection |
|
|
| Individual [41] | One low-SES public elementary school | Novice elementary teachers, within 5 years in-service | Breathing Biofeedback; 29 days of wearing Spire device |
|
|
| Mixed [42] | 5 public schools, urban district | Teachers between preschool and 5th grade | MindUP curriculum, modified version |
| At post-measure, participants significantly improved in:
|
| Individual [43] | K-12 public schools across 20 regions in Texas | School principals | Mindfulness Coach smartphone application, self-guided |
| Non-significant changes in group between pre- and post-measure
|
| Individual [44] | 18 centre-based childcare programs | Early childhood teachers | SELF-T, Self-paced online course |
| At post-measure, participants significantly improved in:
|
| Individual [45] | Four program types: Centre, Home, School-aged, Prekindergarten/Preschools | Early childhood professionals; direct- and indirect care | 2 h Online module: Mindful Practice for ECE Professionals: Begin the Journey; Online module |
|
|
| Mixed, with facilitator [46] | 38 state organizations for infant mental health | Reflective supervisors for ECE professionals | Reflective supervision/consultation | Online survey with 38 questions, including 4 open-ended questions—Demographics, training in becoming provider, perception of intervention effects | Themes observed on the effects of intervention:
|
| One-to-one, with facilitator [47] | 200 ECE centres | Preschool teachers | MyTeachingPartner, video and coaching |
|
|
| Mixed [49] | 49 schools with prekindergarten to grade 12 levels | Teachers with 1–5 years in service | Yoga-based intervention; home practice and group practice |
| Comparing before and after the intervention:
|
| One-to-one, with facilitator [50] | Public schools in areas with shortages of teacher placements | High-stress and emotionally exhausted teachers | Behavioural Activation Intervention, virtual meetings on Zoom |
| Throughout intervention:
|
| Mixed, with facilitator [53] | One private school with K-12 grade | Teachers with different expertise and >1 year experience (5 kindergarten) | One-day Enneagram training, with journaling and focus group discussion |
| Qualitative analysis on practicing learnt:
|
| Duration per Session | Frequency of Session | Period of Intervention | Conducted Needs Assessment | Recruited Participant | Analysed Participant |
|---|---|---|---|---|---|
| Unclear [36] | 3 sessions | Continuous | Yes | 65 | 6 interviewed |
| 20–30 min [37] | Two days per week | Continuous | Yes | Varied | 6 interviewed |
| 45–90 mins [38] | Weekly or biweekly | Continuous | No | 37 | 37 |
| 2–2.5 h [39] | Weekly | 8 weeks | Yes | 67 | 67 |
| 30 min [40] | Weekly (14 meetings) | 4 months | Yes | 21 | 3 interviews + 31 returned open-mail questions) |
| 6 h [41] | Daily | 29 days | No | 13 | 9 |
| 45–60 min [42] | Weekly | 4 weeks | No | 35 | 29 |
| No restriction [43] | Daily | 4 weeks | No | 224 | 53 |
| No restriction [44] | 3 h to complete | 2 weeks | No | 63 | 63 (32 returned activity packet feedback) |
| No restriction [45] | 2 h to complete | — | No | 680, direct | 548 |
| No restriction, but consistent [46] | Weekly or monthly | Continuous | No | 210 | 97 |
| Unclear [47] | Unclear | Continuous | No | 427+69 | 401 |
| Varied between sessions [49] | Weekly | 6 Weeks | No | 51 | 24 (17 with salivary data) |
| 45 + 30 min [50] | Weekly + Daily | 2 weeks | Yes | 6 | 3 |
| No restriction [53] | Daily + 6 h training | 4 weeks | No | 16 | 16 |
| Characteristics (N = 25) | Frequency | |
|---|---|---|
| Gender | Females | 24 |
| Male | 1 | |
| Age | 18–24 | 2 |
| 25–34 | 13 | |
| 35–49 | 9 | |
| 50–64 | 1 | |
| Marital Status | Single | 4 |
| Married | 20 | |
| Divorced | 1 | |
| Level of education | High school | 6 |
| College or Pre-university | 3 | |
| Diploma or Bachelor’s degree | 9 | |
| Master’s degree | 7 | |
| Length of working experience | <1 year | 2 |
| 1–5 years | 4 | |
| 5–10 years | 11 | |
| 10–15 years | 5 | |
| >15 years | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu Hasan, R.; Yusoff, M.S.B.; Tang, T.B.; Hafeez, Y.; Mustafa, M.C.; Dzainudin, M.; Bacotang, J.; Al-Saggaf, U.M.; Ali, S.S.A. Resilience-Building for Mental Health among Early Childhood Educators: A Systematic Review and Pilot-Study towards an EEG-VR Resilience Building Intervention. Int. J. Environ. Res. Public Health 2022, 19, 4413. https://doi.org/10.3390/ijerph19074413
Abu Hasan R, Yusoff MSB, Tang TB, Hafeez Y, Mustafa MC, Dzainudin M, Bacotang J, Al-Saggaf UM, Ali SSA. Resilience-Building for Mental Health among Early Childhood Educators: A Systematic Review and Pilot-Study towards an EEG-VR Resilience Building Intervention. International Journal of Environmental Research and Public Health. 2022; 19(7):4413. https://doi.org/10.3390/ijerph19074413
Chicago/Turabian StyleAbu Hasan, Rumaisa, Muhamad Saiful Bahri Yusoff, Tong Boon Tang, Yasir Hafeez, Mazlina Che Mustafa, Masayu Dzainudin, Juppri Bacotang, Ubaid M. Al-Saggaf, and Syed Saad Azhar Ali. 2022. "Resilience-Building for Mental Health among Early Childhood Educators: A Systematic Review and Pilot-Study towards an EEG-VR Resilience Building Intervention" International Journal of Environmental Research and Public Health 19, no. 7: 4413. https://doi.org/10.3390/ijerph19074413
APA StyleAbu Hasan, R., Yusoff, M. S. B., Tang, T. B., Hafeez, Y., Mustafa, M. C., Dzainudin, M., Bacotang, J., Al-Saggaf, U. M., & Ali, S. S. A. (2022). Resilience-Building for Mental Health among Early Childhood Educators: A Systematic Review and Pilot-Study towards an EEG-VR Resilience Building Intervention. International Journal of Environmental Research and Public Health, 19(7), 4413. https://doi.org/10.3390/ijerph19074413