
Intercultural Competence Predicts Intercultural Effectiveness: Test of an Integrative Framework

 and
and
Abstract
:1. Introduction
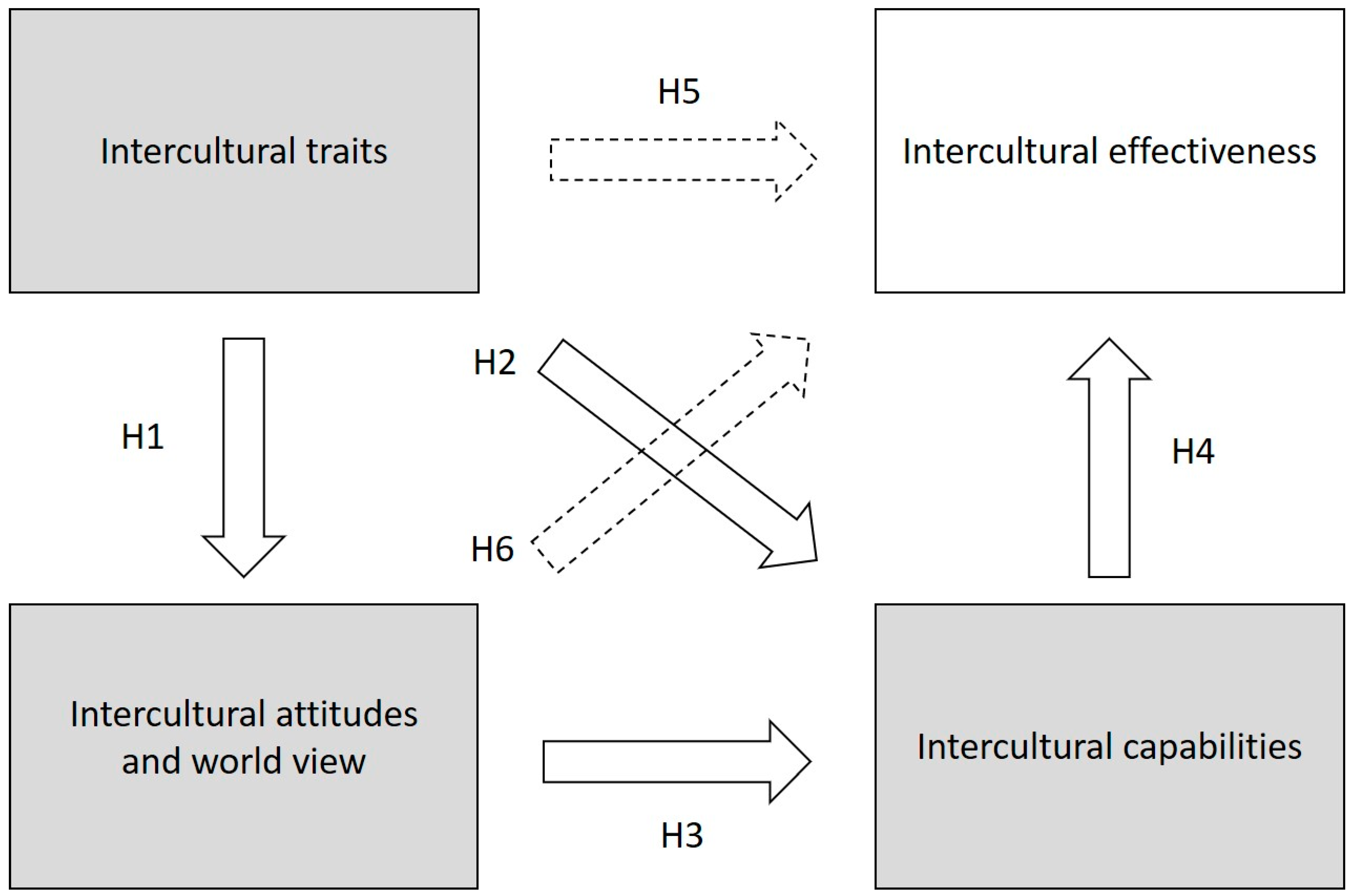
1.1. The Framework of Intercultural Competence and Intercultural Effectiveness
1.1.1. Intercultural Traits
1.1.2. Intercultural Worldviews
1.1.3. Intercultural Capabilities
1.2. Intercultural Effectiveness
1.3. Present Study
2. Materials and Method
2.1. Data and Procedure
2.2. Measures
2.2.1. Intercultural Traits
2.2.2. Intercultural Attitudes and Worldviews
2.2.3. Intercultural Capabilities
2.2.4. Intercultural Effectiveness
2.3. Analyses
3. Results
3.1. Preliminary Analysis: First Order Correlations and CFA
3.2. Model 1: Saturated Model
3.3. Model 2: Structural Model
3.4. Model 3: Structural Model with Subscales
3.5. Hypotheses Evaluation
4. Discussion
4.1. Implications for Practice
4.2. Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdallah-Pretceille, M. Interculturalism as a Paradigm for Thinking about Diversity. Intercult. Educ. 2006, 17, 475–483. [Google Scholar] [CrossRef]
- Capell, J.; Dean, E.; Veenstra, G. The Relationship between Cultural Competence and Ethnocentrism of Health Care Professionals. J. Transcult. Nurs. 2008, 19, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Egede-Nissen, V.; Sellevold, G.S.; Jakobsen, R.; Sørlie, V. Minority Healthcare Providers Experience Challenges, Trust, and Interdependency in a Multicultural Team. Nurs. Ethics 2019, 26, 1326–1336. [Google Scholar] [CrossRef] [PubMed]
- Epner, D.E.; Baile, W.F. Patient-Centered Care: The Key to Cultural Competence. Ann. Oncol. 2012, 23, iii33–iii42. [Google Scholar] [CrossRef]
- Schouten, B.C.; Meeuwesen, L. Cultural Differences in Medical Communication: A Review of the Literature. Patient Educ. Couns. 2006, 64, 21–34. [Google Scholar] [CrossRef]
- Culyer, A.J.; Wagstaff, A. Equity and Equality in Health and Health Care. J. Health Econ. 1993, 12, 431–457. [Google Scholar] [CrossRef]
- Höglund, A.T.; Carlsson, M.; Holmström, I.K.; Lännerström, L.; Kaminsky, E. From Denial to Awareness: A Conceptual Model for Obtaining Equity in Healthcare. Int. J. Equity Health 2018, 17, 9. [Google Scholar] [CrossRef] [Green Version]
- Starfield, B. Improving Equity in Health: A Research Agenda. Int. J. Health Serv. 2001, 31, 545–566. [Google Scholar] [CrossRef]
- Andia, T.S.; Lamprea, E. Is the Judicialization of Health Care Bad for Equity? A Scoping Review. Int. J. Equity Health 2019, 18, 61. [Google Scholar] [CrossRef]
- Lane, H.; Sarkies, M.; Martin, J.; Haines, T. Equity in Healthcare Resource Allocation Decision Making: A Systematic Review. Soc. Sci. Med. 2017, 175, 11–27. [Google Scholar] [CrossRef]
- Paluck, E.L.; Green, D.P. Prejudice Reduction: What Works? A Review and Assessment of Research and Practice. Annu. Rev. Psychol. 2009, 60, 339–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, E.G.; Beach, M.C.; Gary, T.L.; Robinson, K.A.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.; Feuerstein, C.; Bass, E.B.; et al. A Systematic Review of the Methodological Rigor of Studies Evaluating Cultural Competence Training of Health Professionals. Acad. Med. 2005, 80, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Cabral, A.L.L.V.; Giatti, L.; Martínez-Hernáez, Á.; Cherchiglia, M.L. Inequality in Breast Cancer Care in a Brazilian Capital City: A Comparative Analysis of Narratives. Int. J. Equity Health 2019, 18, 88. [Google Scholar] [CrossRef] [PubMed]
- Dovidio, J.F.; Fiske, S.T. Under the Radar: How Unexamined Biases in Decision-Making Processes in Clinical Interactions Can Contribute to Health Care Disparities. Am. J. Public Health 2012, 102, 945–952. [Google Scholar] [CrossRef]
- Johnson-Askew, W.L.; Gordon, L.; Sockalingam, S. Practice Paper of the American Dietetic Association: Addressing Racial and Ethnic Health Disparities. J. Am. Diet. Assoc. 2011, 111, 446–456. [Google Scholar] [CrossRef]
- Çingöl, N.; Karakaş, M.; Çelebi, E.; Zengin, S. Determining the Effect of an Intercultural Nursing Course on Empathic Skill and Intercultural Sensitivity Levels: An Intervention Study. Nurse Educ. Today 2021, 99, 104782. [Google Scholar] [CrossRef]
- Raval, V.V.; Ovia, T.; Freeman, M.; Raj, S.P.; Daga, S.S. Discourses about Race in the United States: A Thematic Analysis of Short Essays. Int. J. Intercult. Relat. 2021, 83, 98–113. [Google Scholar] [CrossRef]
- Leung, K.; Ang, S.; Tan, M.L. Intercultural Competence. Annu. Rev. Organ. Psychol. Organ. Behav. 2014, 1, 489–519. [Google Scholar] [CrossRef] [Green Version]
- Brottman, M.R.; Char, D.M.; Hattori, R.A.; Heeb, R.; Taff, S.D. Toward Cultural Competency in Health Care. Acad. Med. 2020, 95, 803–813. [Google Scholar] [CrossRef]
- Dias, D.; Zhu, C.J.; Samaratunge, R. Examining the Role of Cultural Exposure in Improving Intercultural Competence: Implications for HRM Practices in Multicultural Organizations. Int. J. Hum. Resour. Manag. 2020, 31, 1359–1378. [Google Scholar] [CrossRef]
- Herrera, C.J.; Owens, G.P. Multicultural Personality and Posttraumatic Stress in U.S. Service Members. J. Clin. Psychol. 2015, 71, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Van der Zee, K.I.; van Oudenhoven, J.P. The Multicultural Personality Questionnaire: A Multidimensional Instrument of Multicultural Effectiveness. Eur. J. Personal. 2000, 14, 291–309. [Google Scholar] [CrossRef]
- Den Dekker, W. Global Mindset and Cross-Cultural Behavior: Improving Leadership Effectiveness; MacMillan Publishers Ltd.: London, UK, 2016. [Google Scholar]
- Gielen, J.; van den Branden, S.; Broeckaert, B. The Operationalisation of Religion and World View in Surveys of Nurses’ Attitudes toward Euthanasia and Assisted Suicide. Med. Health Care Philos. 2009, 12, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Piekut, A. Survey Nonresponse in Attitudes towards Immigration in Europe. J. Ethn. Migr. Stud. 2021, 47, 1136–1161. [Google Scholar] [CrossRef]
- Manroop, L.; Boekhorst, J.A.; Harrison, J.A. The Influence of Cross-Cultural Differences on Job Interview Selection Decisions. Int. J. Hum. Resour. Manag. 2013, 24, 3512–3533. [Google Scholar] [CrossRef]
- Wang, C.; Shakespeare-Finch, J.; Dunne, M.P.; Hou, X.-Y.; Khawaja, N.G. How Much Can Our Universities Do in the Development of Cultural Intelligence? A Cross-Sectional Study among Health Care Students. Nurse Educ. Today 2021, 103, 104956. [Google Scholar] [CrossRef]
- Connor-Smith, J.K.; Flachsbart, C. Relations between Personality and Coping: A Meta-Analysis. J. Personal. Soc. Psychol. 2007, 93, 1080–1107. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, M.A.; Harrison, D.A.; Gregersen, H.; Black, J.S.; Ferzandi, L.A. You Can Take It with You: Individual Differences and Expatriate Effectiveness. J. Appl. Psychol. 2006, 91, 109–125. [Google Scholar] [CrossRef]
- Van der Zee, K.I.; van Oudenhoven, J.P. The Multicultural Personality Questionnaire: Reliability and Validity of Self- and Other Ratings of Multicultural Effectiveness. J. Res. Personal. 2001, 35, 278–288. [Google Scholar] [CrossRef]
- Van der Zee, K.; van Oudenhoven, J.P. Culture Shock or Challenge? The Role of Personality as a Determinant of Intercultural Competence. J. Cross-Cult. Psychol. 2013, 44, 928–940. [Google Scholar] [CrossRef]
- Bakker, W.; van der Zee, K.; van Oudenhoven, J.P. Personality and Dutch Emigrants’ Reactions to Acculturation Strategies. J. Appl. Soc. Psychol. 2006, 36, 2864–2891. [Google Scholar] [CrossRef]
- Van Oudenhoven, J.P.; van der Zee, K.I. Predicting Multicultural Effectiveness of International Students: The Multicultural Personality Questionnaire. Int. J. Intercult. Relat. 2002, 26, 679–694. [Google Scholar] [CrossRef]
- Van Oudenhoven, J.P.; Mol, S.; van der Zee, K.I. Study of the Adjustment of Western Expatriates in Taiwan ROC with the Multicultural Personality Questionnaire. Asian J. Soc. Psychol. 2003, 6, 159–170. [Google Scholar] [CrossRef]
- Van der Zee, K.; van Oudenhoven, J.P.; Ponterotto, J.G.; Fietzer, A.W. Multicultural Personality Questionnaire: Development of a Short Form. J. Personal. Assess. 2013, 95, 118–124. [Google Scholar] [CrossRef]
- Summerfield, L.P.; Prado-Gascó, V.; Giménez-Espert, M.D.C.; Mesa-Gresa, P. The Multicultural Personality Questionnaire (SF-40): Adaptation and Validation of the Spanish Version. Int. J. Environ. Res. Public Health 2021, 18, 2426. [Google Scholar] [CrossRef]
- Hampson, S.E.; Goldberg, L.R. A First Large Cohort Study of Personality Trait Stability over the 40 Years between Elementary School and Midlife. J. Personal. Soc. Psychol. 2006, 91, 763–779. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, J.G.; Gray, E.K.; Haig, J.R.; Mroczek, D.K.; Watson, D. Differential Stability and Individual Growth Trajectories of Big Five and Affective Traits during Young Adulthood. J. Personal. 2008, 76, 276–304. [Google Scholar] [CrossRef] [Green Version]
- Horverak, J.G.; Sandal, G.M.; Bye, H.H.; Pallesen, S. Managers’ Selection Preferences: The Role of Prejudice and Multicultural Personality Traits in the Assessment of Native and Immigrant Job Candidates. Eur. Rev. Appl. Psychol. 2013, 63, 267–275. [Google Scholar] [CrossRef]
- Nesdale, D.; de Vries Robbé, M.; van Oudenhoven, J.P. Intercultural Effectiveness, Authoritarianism, and Ethnic Prejudice. J. Appl. Soc. Psychol. 2012, 42, 1173–1191. [Google Scholar] [CrossRef]
- Ang, S.; van Dyne, L.; Koh, C. Personality Correlates of the Four-Factor Model of Cultural Intelligence. Group Organ. Manag. 2006, 31, 100–123. [Google Scholar] [CrossRef]
- Ward, C.; Fischer, R. Personality, Cultural Intelligence, and Cross-Cultural Adaptation. In Handbook on Cultural Intelligence: Theory, Measurement and Applications; Sharpe: New York, NY, USA, 2008; pp. 159–176. [Google Scholar]
- Michael Paige, R.; Jacobs-Cassuto, M.; Yershova, Y.A.; DeJaeghere, J. Assessing Intercultural Sensitivity: An Empirical Analysis of the Hammer and Bennett Intercultural Development Inventory. Int. J. Intercult. Relat. 2003, 27, 467–486. [Google Scholar] [CrossRef]
- Bennett, M.J. Developmental Model of Intercultural Sensitivity. In The International Encyclopedia of Intercultural Communication; Wiley: Hoboken, NJ, USA, 2017. [Google Scholar]
- Bizumic, B.; Duckitt, J. What Is and Is Not Ethnocentrism? A Conceptual Analysis and Political Implications. Political Psychol. 2012, 33, 887–909. [Google Scholar] [CrossRef]
- Kirillova, K.; Lehto, X.; Cai, L. Volunteer Tourism and Intercultural Sensitivity: The Role of Interaction with Host Communities. J. Travel Tour. Mark. 2015, 32, 382–400. [Google Scholar] [CrossRef]
- Hammer, M.R. The Developmental Paradigm for Intercultural Competence Research. Int. J. Intercult. Relat. 2015, 48, 12–13. [Google Scholar] [CrossRef]
- Hammer, M.R. Additional Cross-Cultural Validity Testing of the Intercultural Development Inventory. Int. J. Intercult. Relat. 2011, 35, 474–487. [Google Scholar] [CrossRef]
- Kaya, Y.; Arslan, S.; Erbaş, A.; Yaşar, B.N.; Küçükkelepçe, G.E. The Effect of Ethnocentrism and Moral Sensitivity on Intercultural Sensitivity in Nursing Students, Descriptive Cross-Sectional Research Study. Nurse Educ. Today 2021, 100, 104867. [Google Scholar] [CrossRef]
- Ng, K.-Y.; van Dyne, L.; Ang, S. From Experience to Experiential Learning: Cultural Intelligence as a Learning Capability for Global Leader Development. Acad. Manag. Learn. Educ. 2009, 8, 511–526. [Google Scholar] [CrossRef] [Green Version]
- Young, C.A.; Haffejee, B.; Corsun, D.L. The Relationship between Ethnocentrism and Cultural Intelligence. Int. J. Intercult. Relat. 2017, 58, 31–41. [Google Scholar] [CrossRef]
- Early, P.; Ang, S. Cultural Intelligence: Individual Interactions across Cultures; Stanford University Press: Redwood, CA, USA, 2003. [Google Scholar]
- Herrmann, E.; Call, J.; Hernàndez-Lloreda, M.V.; Hare, B.; Tomasello, M. Humans Have Evolved Specialized Skills of Social Cognition: The Cultural Intelligence Hypothesis. Science 2007, 317, 1360–1366. [Google Scholar] [CrossRef] [Green Version]
- Peterson, B. Cultural Intelligence: A Guide to Working with People from Other Cultures; Intercultural Press: London, UK, 2004. [Google Scholar]
- Andresen, M.; Bergdolt, F. A Systematic Literature Review on the Definitions of Global Mindset and Cultural Intelligence—Merging Two Different Research Streams. Int. J. Hum. Resour. Manag. 2017, 28, 170–195. [Google Scholar] [CrossRef]
- Schwarzenthal, M.; Juang, L.P.; Schachner, M.K.; van de Vijver, F.J.R. A Multimodal Measure of Cultural Intelligence for Adolescents Growing up in Culturally Diverse Societies. Int. J. Intercult. Relat. 2019, 72, 109–121. [Google Scholar] [CrossRef]
- Van Dyne, L.; Ang, S.; Ng, K.Y.; Rockstuhl, T.; Tan, M.L.; Koh, C. Sub-Dimensions of the Four Factor Model of Cultural Intelligence: Expanding the Conceptualization and Measurement of Cultural Intelligence. Soc. Personal. Psychol. Compass 2012, 6, 295–313. [Google Scholar] [CrossRef]
- Chen, X.; Gabrenya, W.K. In Search of Cross-Cultural Competence: A Comprehensive Review of Five Measurement Instruments. Int. J. Intercult. Relat. 2021, 82, 37–55. [Google Scholar] [CrossRef]
- Schwarzenthal, M.; Schachner, M.K.; Juang, L.P.; van de Vijver, F.J.R. Reaping the Benefits of Cultural Diversity: Classroom Cultural Diversity Climate and Students’ Intercultural Competence. Eur. J. Soc. Psychol. 2020, 50, 323–446. [Google Scholar] [CrossRef]
- Harrison, R.; Walton, M.; Chauhan, A.; Manias, E.; Chitkara, U.; Latanik, M.; Leone, D. What Is the Role of Cultural Competence in Ethnic Minority Consumer Engagement? An Analysis in Community Healthcare. Int. J. Equity Health 2019, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Schei, V.; Selart, M. Hype or Hope? A New Look at the Research on Cultural Intelligence. Int. J. Intercult. Relat. 2018, 66, 148–171. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Cognitive Theory: An Agentic Perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandura, A. Social Cognitive Theory of Self-Regulation. Organ. Behav. Hum. Decis. Processes 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Talsma, K.; Schüz, B.; Schwarzer, R.; Norris, K. I Believe, Therefore I Achieve (and Vice Versa): A Meta-Analytic Cross-Lagged Panel Analysis of Self-Efficacy and Academic Performance. Learn. Individ. Differ. 2018, 61, 136–150. [Google Scholar] [CrossRef]
- Zimmermann, J.; Greischel, H.; Jonkmann, K. The Development of Multicultural Effectiveness in International Student Mobility. High. Educ. 2020, 82, 171–192. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Efficacy of the Theory of Planned Behaviour: A Meta-Analytic Review. Br. J. Soc. Psychol. 2001, 40, 471–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Earley, P.C.; Peterson, R.S. The Elusive Cultural Chameleon: Cultural Intelligence as a New Approach to Intercultural Training for the Global Manager. Acad. Manag. Learn. Educ. 2004, 3, 100–115. [Google Scholar] [CrossRef] [Green Version]
- MacNab, B.R.; Worthley, R. Individual Characteristics as Predictors of Cultural Intelligence Development: The Relevance of Self-Efficacy. Int. J. Intercult. Relat. 2012, 36, 62–71. [Google Scholar] [CrossRef]
- Quine, A.; Hadjistavropoulos, H.D.; Alberts, N.M. Cultural Self-Efficacy of Canadian Nursing Students Caring for Aboriginal Patients with Diabetes. J. Transcult. Nurs. 2012, 23, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Briones, E.; Tabernero, C.; Tramontano, C.; Caprara, G.V.; Arenas, A. Development of a Cultural Self-Efficacy Scale for Adolescents (CSES-A). Int. J. Intercult. Relat. 2009, 33, 301–312. [Google Scholar] [CrossRef]
- Berhanu, R.D.; Tesema, A.A.; Deme, M.B.; Kanfe, S.G. Perceived Transcultural Self-Efficacy and Its Associated Factors among Nurses in Ethiopia: A Cross-Sectional Study. PLoS ONE 2021, 16, e0254643. [Google Scholar] [CrossRef]
- Capone, V.; Petrillo, G. Patient’s Communication Perceived Self-Efficacy Scale (PCSS): Construction and Validation of a New Measure in a Socio-Cognitive Perspective. Patient Educ. Couns. 2014, 95, 340–347. [Google Scholar] [CrossRef]
- Tam, C.C.; Li, X.; Benotsch, E.G.; Lin, D. A Resilience-Based Intervention Programme to Enhance Psychological Well-Being and Protective Factors for Rural-to-Urban Migrant Children in China. Appl. Psychol. Health Well-Being 2020, 12, 53–76. [Google Scholar] [CrossRef]
- Oolders, T.; Chernyshenko, O.S.; Stark, S. Cultural Intelligence as a Mediator of Relationships between Openness to Experience and Adaptive Performance. In Handbook on Cultural Intelligence: Theory, Measurement and Applications; Psychology Faculty Publications: London, UK; New York, NY, USA, 2008; pp. 145–158. [Google Scholar]
- Ramalu, S.S.; Shamsudin, F. Mohd.; Subramania, C. The Mediating Effect of Cultural Intelligence on the Relationship between Openness Personality and Job Performance among Expatriates on International Assignments. Int. Bus. Manag. 2012, 6, 601–610. [Google Scholar] [CrossRef]
- Greipp, M.E. Culture, Age and Gender: Effects on Quality of Predicted Self and Colleague Reactions. Int. J. Nurs. Stud. 1996, 33, 83–97. [Google Scholar] [CrossRef]
- Logan, S.; Steel, Z.; Hunt, C. Intercultural Willingness to Communicate within Health Services: Investigating Anxiety, Uncertainty, Ethnocentrism and Help Seeking Behaviour. Int. J. Intercult. Relat. 2016, 54, 77–86. [Google Scholar] [CrossRef]
- Academic Ranking of World Universities. Available online: https://www.shanghairanking.com/ (accessed on 30 December 2021).
- The Labor Market from a Gender Point of View. Available online: https://statbel.fgov.be/nl/visuals/arbeid-en-gender (accessed on 30 December 2021).
- Living Together in Diversity. Available online: http://www.samenleven-in-diversiteit.vlaanderen.be/ (accessed on 30 December 2021).
- European Social Survey 2002/2003: Technical Report. Available online: http://www.europeansocialsurvey.org (accessed on 16 June 2020).
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.r-project.org/ (accessed on 30 December 2021).
- The Lavaan Project. Available online: https://lavaan.ugent.be/ (accessed on 30 December 2021).
- Ullman, J.B.; Bentler, P.M. Structural Equation Modeling. In Handbook of Psychology, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kaniskan, B.; Mccoach, D.B. The Performance of RMSEA in Models with Small Degrees of Freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Measuring Model Fit. Available online: http://www.davidakenny.net/cm/fit.htm (accessed on 30 December 2021).
- Gumber, A.; Gumber, L. Improving Prevention, Monitoring and Management of Diabetes among Ethnic Minorities: Contextualizing the Six G’s Approach. BMC Res. Notes 2017, 10, 774. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| M | SD | EC-ER | MPQ-CE | MPQ-FX | MPQ-SI | MPQ-ES | MPQ-OP | CSE-process | CSE-mix | CSE-cope | CSE-US | CSE-LAN | CSE | CQ-MOT | CQ-COG | CQ-META | CQ-BEH | CQ | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EC-ER | 39.99 | 8.2 | 1 | 0.181 ** | 0.153 ** | 0.066 | 0.066 | 0.398 ** | 0.308 ** | 0.296 ** | 0.021 | 0.362 ** | 0.075 * | 0.319 ** | 0.470 ** | 0.121 ** | 0.256 ** | 0.194 ** | 0.371 ** |
| MPQ-CE | 33.42 | 3.44 | 1 | −0.070 * | 0.261 ** | −0.062 | 0.387 ** | 0.338 ** | 0.265 ** | 0 | 0.303 ** | 0.127 ** | 0.302 ** | 0.415 ** | 0.144 ** | 0.229 ** | 0.238 ** | 0.366 ** | |
| MPQ-FX | 19.62 | 5.66 | 1 | 0.099 ** | 0.257 ** | 0.148 ** | 0.064 | 0.141 ** | 0.003 | 0.108 ** | 0.043 | 0.113 ** | 0.101 ** | 0.05 | −0.025 | −0.047 | 0.033 | ||
| MPQ-SI | 26.58 | 5.13 | 1 | 0.273 ** | 0.275 ** | 0.224 ** | 0.288 ** | 0.037 | 0.130 ** | 0.134 ** | 0.249 ** | 0.145 ** | 0.112 ** | 0.081* | 0.022 | 0.136 ** | |||
| MPQ-ES | 24.66 | 5.71 | 1 | 0.218 ** | 0.108 ** | 0.173 ** | 0.141 ** | 0.062 | 0.101 ** | 0.180 ** | 0.073 * | 0.116 ** | −0.052 | −0.146 ** | 0.01 | ||||
| MPQ-OP | 27.63 | 4.22 | 1 | 0.503 ** | 0.434 ** | 0.145 ** | 0.365 ** | 0.298 ** | 0.512 ** | 0.518 ** | 0.303 ** | 0.291 ** | 0.167 ** | 0.471 ** | |||||
| CSE-process | 18.06 | 2.67 | 1 | 0.521 ** | 0.152 ** | 0.498 ** | 0.358 ** | 0.721 ** | 0.538 ** | 0.386 ** | 0.238 ** | 0.187 ** | 0.502 ** | ||||||
| CSE-mix | 3.52 | 4.45 | 1 | 0.306 ** | 0.446 ** | 0.349 ** | 0.829 ** | 0.559 ** | 0.230 ** | 0.191 ** | 0.158 ** | 0.414 ** | |||||||
| CSE-cope | 11.61 | 3.42 | 1 | 0.111 ** | 0.147 ** | 0.534 ** | 0.132 ** | 0.147 ** | −0.033 | −0.045 | 0.083 * | ||||||||
| CSE-US | 18.31 | 3.09 | 1 | 0.296 ** | 0.682 ** | 0.524 ** | 0.390 ** | 0.233 ** | 0.204 ** | 0.502 ** | |||||||||
| CSE-LAN | 9.51 | 2.56 | 1 | 0.587 ** | 0.240 ** | 0.315 ** | 0.156 ** | 0.076 * | 0.302 ** | ||||||||||
| CSE | 88.02 | 11.05 | 1 | 0.598 ** | 0.413 ** | 0.226 ** | 0.169 ** | 0.524 ** | |||||||||||
| CQ-MOT | 23.31 | 3.17 | 1 | 0.279 ** | 0.311 ** | 0.270 ** | 0.668 ** | ||||||||||||
| CQ-COG | 17.17 | 3.99 | 1 | 0.186 ** | 0.155 ** | 0.651 ** | |||||||||||||
| CQ-META | 21.16 | 3.34 | 1 | 0.557 ** | 0.731 ** | ||||||||||||||
| CQ-BEH | 21.4 | 2.9 | 1 | 0.682 ** | |||||||||||||||
| CQ | 83.05 | 9.13 | 1 |
| H | Regression | E | SE | z | p | ML |
|---|---|---|---|---|---|---|
| EC-ER | ~ | |||||
| H1 | MPQ-CE | 0.18 | 0.11 | 1.55 | 0.121 | 0.06 |
| H1 | MPQ-FX | 0.22 | 0.06 | 3.43 | 0.001 | 0.11 |
| H1 | MPQ-SI | −0.12 | 0.07 | −1.67 | 0.096 | −0.06 |
| H1 | MPQ-ES | −0.05 | 0.07 | −0.77 | 0.441 | −0.03 |
| H1 | MPQ-OP | 0.99 | 0.09 | 10.66 | 0.000 | 0.38 |
| CQ | ~ | |||||
| H2 | MPQ-CE | 0.17 | 0.03 | 6.03 | 0.000 | 0.20 |
| H2 | MPQ-FX | −0.01 | 0.02 | −0.62 | 0.537 | −0.02 |
| H2 | MPQ-SI | 0.00 | 0.02 | −0.06 | 0.952 | 0.00 |
| H2 | MPQ-ES | −0.03 | 0.02 | −1.81 | 0.070 | −0.06 |
| H2 | MPQ-OP | 0.24 | 0.03 | 9.33 | 0.000 | 0.33 |
| CQ | ~ | |||||
| H3 | EC-ER | 0.06 | 0.01 | 6.69 | 0.000 | 0.21 |
| CSE-TOT | ~ | |||||
| H4 | CQ | 0.40 | 0.04 | 10.79 | 0.000 | 0.35 |
| H5 | MPQ-CE | 0.05 | 0.03 | 1.56 | 0.120 | 0.05 |
| H5 | MPQ-FX | 0.02 | 0.02 | 0.92 | 0.358 | 0.03 |
| H5 | MPQ-SI | 0.06 | 0.02 | 2.95 | 0.003 | 0.09 |
| H5 | MPQ-ES | 0.06 | 0.02 | 2.99 | 0.003 | 0.09 |
| H5 | MPQ-OP | 0.22 | 0.03 | 7.48 | 0.000 | 0.26 |
| H6 | EC-ER | 0.02 | 0.01 | 2.07 | 0.038 | 0.06 |
| H | Regression | E | SE | z | p | ML |
|---|---|---|---|---|---|---|
| EC-ER | ~ | |||||
| H1 | MPQ-FX | 0.19 | 0.06 | 3.01 | 0.003 | 0.10 |
| H1 | MPQ-OP | 1.00 | 0.08 | 12.07 | 0.000 | 0.38 |
| CQ | ~ | |||||
| H2 | MPQ-CE | 0.19 | 0.03 | 6.69 | 0.000 | 0.21 |
| H2 | MPQ-OP | 0.22 | 0.02 | 9.08 | 0.000 | 0.31 |
| CQ | ~ | |||||
| H3 | EC-ER | 0.06 | 0.01 | 6.70 | 0.000 | 0.21 |
| CSE | ~ | |||||
| H4 | CQ | 0.42 | 0.04 | 11.35 | 0.000 | 0.36 |
| H5 | MPQ-SI | 0.07 | 0.02 | 3.38 | 0.001 | 0.10 |
| H5 | MPQ-ES | 0.05 | 0.02 | 3.02 | 0.003 | 0.09 |
| H5 | MPQ-OP | 0.23 | 0.03 | 8.26 | 0.000 | 0.27 |
| H6 | EC-ER | 0.02 | 0.01 | 2.19 | 0.029 | 0.07 |
| H | Regression | E | SE | z | p | ML |
|---|---|---|---|---|---|---|
| EC-ER | ~ | |||||
| H1 | MPQ-OP | 1.00 | 0.08 | 12.07 | 0.000 | 0.38 |
| H1 | MPQ-FX | 0.19 | 0.06 | 3.01 | 0.003 | 0.10 |
| CQ-MOT | ~ | |||||
| H2 | MPQ-CE | 0.30 | 0.04 | 8.40 | 0.000 | 0.24 |
| H2 | MPQ-OP | 0.30 | 0.03 | 9.67 | 0.000 | 0.30 |
| H3 | EC-ER | 0.12 | 0.01 | 1.51 | 0.000 | 0.31 |
| CQ-COG | ~ | |||||
| H2 | MPQ-OP | 0.38 | 0.04 | 9.24 | 0.000 | 0.30 |
| CQ-META | ~ | |||||
| H2 | MPQ-CE | 0.17 | 0.04 | 3.85 | 0.000 | 0.13 |
| H2 | MPQ-OP | 0.17 | 0.03 | 5.02 | 0.000 | 0.16 |
| H3 | EC-ER | 0.07 | 0.01 | 4.85 | 0.000 | 0.17 |
| CQ-BEH | ~ | |||||
| H2 | MPQ-CE | 0.23 | 0.04 | 6.23 | 0.000 | 0.21 |
| H3 | EC-ER | 0.05 | 0.01 | 4.57 | 0.000 | 0.15 |
| SE-process | ~ | |||||
| H4 | CQ-MOT | 0.31 | 0.03 | 9.77 | 0.000 | 0.31 |
| H4 | CQ-COG | 0.16 | 0.02 | 7.49 | 0.000 | 0.21 |
| H5 | MPQ-CE | 0.11 | 0.04 | 3.17 | 0.002 | 0.09 |
| H5 | MPQ-OP | 0.25 | 0.03 | 7.53 | 0.000 | 0.25 |
| SE-mix | ~ | |||||
| H4 | CQ-MOT | 0.47 | 0.03 | 14.51 | 0.000 | 0.45 |
| H5 | MPQ-OP | 0.15 | 0.03 | 4.63 | 0.000 | 0.14 |
| H5 | MPQ-SI | 0.14 | 0.02 | 6.39 | 0.000 | 0.17 |
| SE-cope | ~ | |||||
| H4 | CQ-MOT | 0.16 | 0.06 | 2.95 | 0.003 | 0.10 |
| H4 | CQ-COG | 0.13 | 0.04 | 3.15 | 0.002 | 0.10 |
| H5 | MPQ-ES | 0.11 | 0.04 | 2.74 | 0.006 | 0.09 |
| SE-US | ~ | |||||
| H4 | CQ-MOT | 0.38 | 0.04 | 9.85 | 0.000 | 0.33 |
| H4 | CQ-COG | 0.24 | 0.03 | 9.26 | 0.000 | 0.26 |
| H5 | MPQ-CE | 0.15 | 0.04 | 3.54 | 0.000 | 0.11 |
| H6 | EC-ER | 0.07 | 0.01 | 5.14 | 0.000 | 0.16 |
| SE-LA | ~ | |||||
| H4 | CQ-COG | 0.30 | 0.04 | 7.15 | 0.000 | 0.23 |
| H5 | MPQ-OP | 0.36 | 0.05 | 6.68 | 0.000 | 0.22 |
| CQ-MOT | CQ-COG | CQ-META | CQ-BEH | EC-ER | SE-Process | SE-Mix | SE-Cope | SE-US | SE-LAN | |
|---|---|---|---|---|---|---|---|---|---|---|
| R2 | 0.397 | 0.092 | 0.116 | 0.076 | 0.167 | 0.384 | 0.361 | 0.035 | 0.339 | 0.135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schelfhout, S.; Vandecasteele, R.; De Maesschalck, S.; D’hondt, F.; Willems, S.; Derous, E. Intercultural Competence Predicts Intercultural Effectiveness: Test of an Integrative Framework. Int. J. Environ. Res. Public Health 2022, 19, 4490. https://doi.org/10.3390/ijerph19084490
Schelfhout S, Vandecasteele R, De Maesschalck S, D’hondt F, Willems S, Derous E. Intercultural Competence Predicts Intercultural Effectiveness: Test of an Integrative Framework. International Journal of Environmental Research and Public Health. 2022; 19(8):4490. https://doi.org/10.3390/ijerph19084490
Chicago/Turabian StyleSchelfhout, Stijn, Robin Vandecasteele, Stéphanie De Maesschalck, Fanny D’hondt, Sara Willems, and Eva Derous. 2022. "Intercultural Competence Predicts Intercultural Effectiveness: Test of an Integrative Framework" International Journal of Environmental Research and Public Health 19, no. 8: 4490. https://doi.org/10.3390/ijerph19084490
APA StyleSchelfhout, S., Vandecasteele, R., De Maesschalck, S., D’hondt, F., Willems, S., & Derous, E. (2022). Intercultural Competence Predicts Intercultural Effectiveness: Test of an Integrative Framework. International Journal of Environmental Research and Public Health, 19(8), 4490. https://doi.org/10.3390/ijerph19084490