
A Mixed-Methods Formative Evaluation of a Dementia-Friendly Congregation Program for Black Churches


Abstract
:1. Introduction
2. Materials and Methods
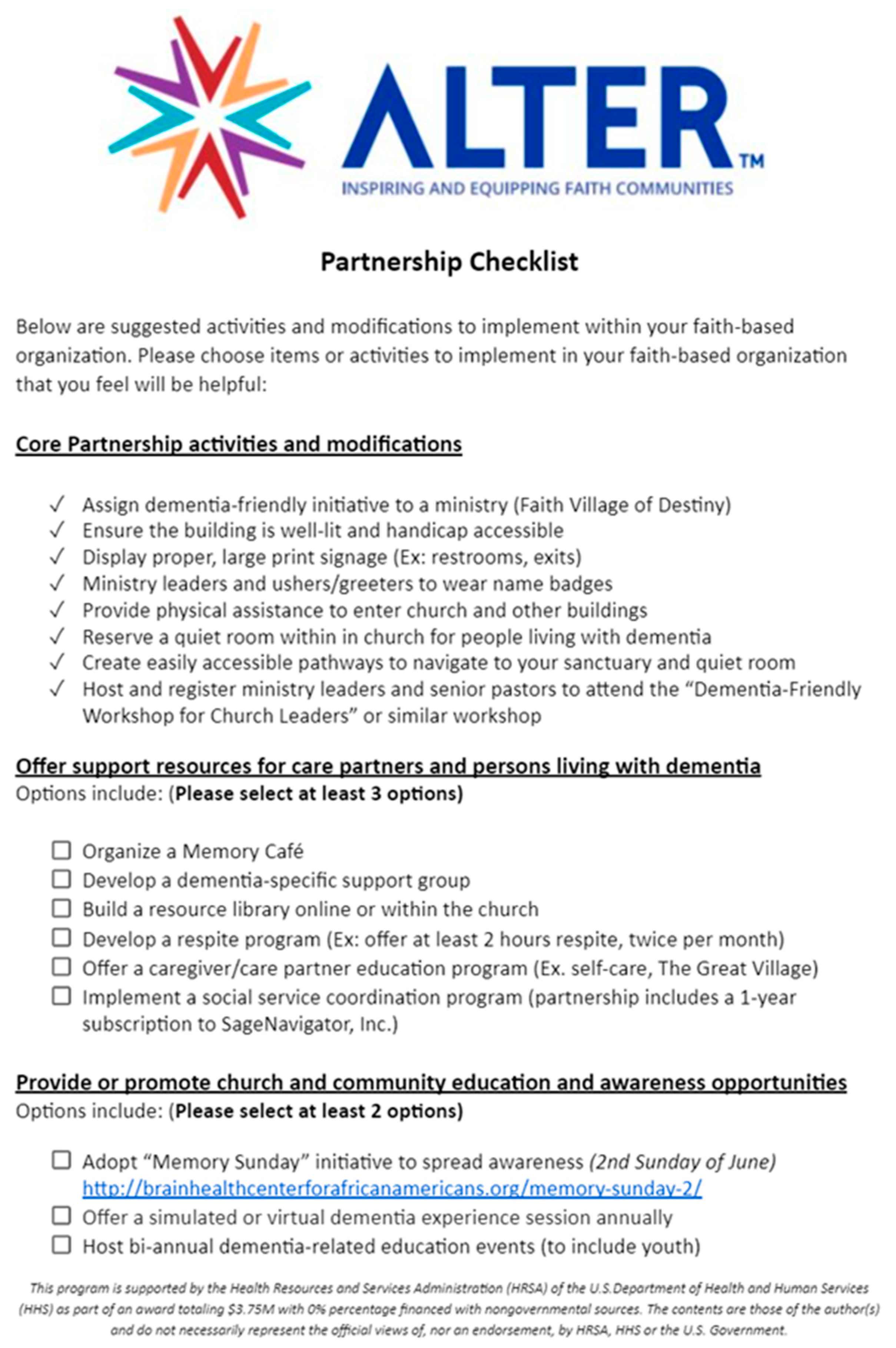
2.1. Program Description
2.2. Program Recruitment and Implementation
2.3. Evaluation Design and Measure
- How can Alter™ best support partnering churches as the program continues to enroll more churches?
- How helpful are the proposed program activities and modifications?
- How difficult is it to implement the proposed program activities and modifications at partnering churches?
- How useful are the proposed program activities and modifications?
- How did the COVID-19 pandemic impact participating churches’ ability to participate in the program fully?
2.4. Data Collection and Procedures
2.5. Statistical Analysis
2.6. Qualitative Analysis
3. Results
3.1. Church Partner Characteristics
3.2. Experience Implementing Program Activities and Modifications
3.2.1. Core Activities
3.2.2. Support Activities
3.2.3. Educational and Awareness Activities
3.2.4. Worship Modifications
3.2.5. Barriers to Implementation
3.3. Focus Group Findings
3.3.1. Barriers to Implementing Activities
“…once COVID came and then we shut everything down. So, we still have those things to do. You know? …, I think we would’ve been much further along had COVID not come.”
“well, our organization have been so focused on trying to get back in the church as well as to bring education, ah, to their, ah, constituents, um, about COVID. And so, that’s been their primary focus and how they can, you know, really not lose their members during this time. … So, they have put the dementia back on the back burner, you know, during this time because that’s been their primary focus.”Participant 4, Focus Group 2
“But right now, we just really don’t have that many, ah, people in the congregation, ah, who are actually dealing with, or living with dementia … I’m sure people will be coming or, you know, or things will be changing. So, that’s where we are in getting more things set up so that when, um, they’re needed, they will be available.”Participant 2, Focus Group 1
“[W]hen we went through our survey [a] couple weeks ago, there were some things I think I could’ve implemented that I didn’t implement… I was like, “Oh, I… We could’ve did that.”
3.3.2. Support Provided and Needed
“Keep on doing the good job that you’re doing in helping us to become, ah, great Faith Village [dementia-friendly] churches. Because, ah, it’s just a, it’s something that’s very much needed and, ah, the team has done an excellent job even, ah, with the COVID situation.”Participant 1, Focus group 1
“Because the other day we had, um, someone and, and the, the father is member of our church. He’s, he’s older, but was doing very well, but has now moved back in with his daughter. And she had, um, she’s- she’s having to work from home and just some other things. But, ah, and I was able to, ah, connect her with [program staff], and it just really helped. Because we don’t know, well, let me speak for me. I don’t know all of the ins and outs and what may be available. I know with, with some of the information, but as far as talking to someone and seeing exactly where they are and what they need, then having her there has been just a tremendous asset.”Participant 2, Focus group 1
“Because we’re dealing with people who—in most cases—are older. [They wonder,] “Okay, I’ve gotta dial a 1–800 number. What…?” The first thing that comes to their mind [is], “Okay, I may get in a loop… You know, it’s gonna be somebody who doesn’t necessarily care about me or whatever.” … but having you contact the sister the other day and being able to talk to her, letting her know you understood exactly what she was looking for, and I don’t even know if she found everything, but it was the fact that this is somebody who understands what’s happening here.”
“But I think it, it’s, you know, it’s good that we are talking and getting- getting to, to know each other… and or- or call or whatever and say, “Well, how did… how did this work for you? This is what we’re trying to do, but we’re running into a roadblock.” You know? And, and sometimes just-just having that, ah, because it’s just, it’s a lot we can do but then it’s a lot that we can’t do.”Participant 2, Focus group 1
3.3.3. Use of Program Funding
“Well, because of, ah, most of the churches been closed, ah, we haven’t used the money, ah, in The Alliance … So, um, it’s been beneficial, um, that, you know, we just hadn’t decided to use the money right now. We just doing, you know, we just doing what we do.”Participant 4, Focus Group 1
“…but in the future. the church is not that big. Obviously, um, we do not have anything that we are doing that’s costing anything right now.”Participant 1, Focus Group 2
“And the toolbox had socks; it had, um, mints, nuts, um, a puzzle, a cross--no, word, word search puzzle. It had colored pencils for the colored, um, booklets. And just so happen, I went to the Dollar Tree, and they had those inspirational coloring books, and you could download the music, there was music to go along with the coloring books.”Participant 3, Focus Group 2
4. Discussion
4.1. Adapting Health Promotion Programs Virtually
4.2. Assessing Community Organization Capacity for Programming
4.3. Developing a Program Manual
4.4. Conducting Structured Workshops for Program Implementors
4.5. Hiring Health Educators
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B. Focus Group Guide (Utilized RE-AIM Framework)
- How did your church hear about the Dementia-Friendly Faith Villages Community program? Disclaimer: Dementia-friendly faith village community will be referred to as DFFVC throughout the remainder of the focus group.
- Why did your church decide to participate in the program?
- What were your churches first impressions of the DFFVC program?
- Do you see this program helping other churches?
- What attracted you to the program or the concept of dementia-friendly churches?
- Can you all describe what the “Dementia-friendly faith villages community program” means to everyone’s respective church?
- 4.
- Can you express to me how the program has helped/assisted your congregation and the church with creating a dementia-friendly church?
- Do you feel the church is more educated?
- How do you feel the church is more aware?
- Explain why or/and example.
- 5.
- What elements of the program allow the church to continue to implement and modify the space into a dementia-friendly environment?
- Structure, experience with staff, support
- 6.
- Is there something you would change about the dementia-friendly community program?
- How would the changes you suggest impact the church members affected by dementia?
- What would you like to see change within your church as a result of creating a dementia-friendly space?
- 7.
- Are there ways in which this program has had a positive impact on your church and church members?
- Persons experiencing Dementia
- Caregivers
- Other congregants
- 8.
- Did implementing the DFFVC program present any challenges?
- What aspects of the program are challenging?
- Have there been challenges implementing the program? Why have you not implemented anything?
- What other factors made it challenging? (i.e., Financial strain?)
- What aspects have negatively impacted the church, caregivers, and/or persons living with dementia?
- 9.
- How does the dementia-friendly program align with your churches’ mission?
- Have you had to adjust your mission to fulfill the requirements of the dementia-friendly program?
- Have you changed the dementia-friendly program to align with your churches mission?
- How have you used the DFFVC program’s framework to make decisions for your churches when it comes to providing support and an appropriate worship experience for persons with dementia and their caregivers?
- 10.
- What have you seen as a result of implementing the DFFVC program?
- Tell me about a time when you saw the program help someone or someone expressed gratitude about the program?
- Any Success stories from anything you have implemented?
- What is the program doing well?
- 11.
- We are always looking to expand the number of churches within our network. How do you think this program would benefit future churches?
- 12.
- Do you feel the money received from the program to implement the dementia-friendly modifications assist your church effectively?
- Explain why and how?
- What are additional costs the church had to take on that the scholarship did not cover?
- 13.
- How do your churches plan to maintain the program in the next 2–3 years?
- What is sustainable about the program?
- What do you feel you will be able to maintain?
- What factors may hinder the maintenance of the program?
- 14.
- What are additional ways we can support your church in creating a dementia-friendly space?
Appendix C

{kind=link}
{kind=link}
| Evaluation Survey Components | Assign to a Ministry | Building Is Well-Lit | Large Print Signage | Badges for Support Staff | Physical Support | Quiet Room/Space | Accessible Pathways | Church Leaders Workshop |
|---|---|---|---|---|---|---|---|---|
| Implementation status | ||||||||
| Not Selected | -- | -- | -- | -- | -- | -- | -- | -- |
| Selected to Implement and NOT Implemented | 1 | 1 | 4 | 1 | 4 | 3 | 3 | |
| Selected to Implement and Implemented | 8 | 7 | 7 | 4 | 7 | 4 | 5 | 5 |
| Level of helpfulness | ||||||||
| Completely helpful | 4 | 4 | 5 | 3 | 5 | 2 | 2 | 4 |
| Very helpful | 2 | 3 | 1 | 1 | 1 | 1 | 1 | 1 |
| Moderately helpful | 2 | -- | -- | -- | 1 | -- | -- | -- |
| Slightly helpful | -- | -- | 2 | -- | -- | -- | -- | -- |
| Not helpful at all | -- | -- | -- | -- | -- | -- | -- | -- |
| Level of difficulty | ||||||||
| Not Difficult at All | 7 | 7 | 7 | 4 | 6 | 3 | 5 | 4 |
| Slightly Difficult | -- | -- | -- | 1 | -- | -- | -- | |
| Moderately Difficult | 1 | -- | -- | -- | -- | -- | -- | -- |
| Very Difficult | -- | -- | -- | -- | -- | -- | -- | -- |
| Extremely Difficult (not able to implement) | -- | -- | -- | -- | -- | -- | -- | -- |
| Utility | ||||||||
| Extensively Utilizing | 1 | -- | -- | 4 | 5 | 1 | 1 | 2 |
| Utilizing | 3 | -- | -- | -- | -- | -- | -- | 3 |
| Moderately Utilizing | 1 | -- | -- | -- | 1 | 1 | -- | -- |
| Somewhat Utilizing | 3 | -- | -- | -- | -- | -- | 1 | -- |
| Not Utilizing | -- | -- | -- | -- | 1 | 1 | 3 | -- |
Appendix D
| Evaluation Survey Components | Memory Café | Support Group | Resource Library | Respite Care | Educational Events | Social Service Coordination |
|---|---|---|---|---|---|---|
| Implementation status | ||||||
| Not Selected to Implement | 3 | 4 | 1 | 6 | -- | 5 |
| Selected to Implement and NOT Implemented | 5 | 2 | 3 | 1 | 4 | 2 |
| Selected to Implement and Implemented | -- | 2 | 4 | 1 | 4 | 1 |
| Level of helpfulness | ||||||
| Completely helpful | -- | -- | 3 | -- | 1 | -- |
| Very helpful | -- | 1 | -- | -- | 3 | 1 |
| Moderately helpful | -- | 1 | 1 | -- | -- | |
| Slightly helpful | -- | -- | -- | -- | -- | |
| Not helpful at all | -- | -- | -- | -- | -- | |
| Level of difficulty | ||||||
| Not Difficult at All | -- | 2 | 4 | 1 | 3 | -- |
| Slightly Difficult | -- | -- | -- | -- | -- | 1 |
| Moderately Difficult | -- | -- | -- | -- | 1 | -- |
| Very Difficult | -- | -- | -- | -- | -- | -- |
| Extremely Difficult (not able to implement) | -- | -- | -- | -- | -- | -- |
| Utility | ||||||
| Extensively Utilizing | -- | -- | -- | -- | 1 | -- |
| Utilizing | -- | -- | -- | -- | -- | -- |
| Moderately Utilizing | -- | -- | 3 | -- | 1 | 1 |
| Somewhat Utilizing | -- | 1 | 1 | -- | 2 | -- |
| Not Utilizing | -- | 1 | -- | 1 | -- | -- |
Appendix E
| Evaluation Survey Components | Memory Sunday | Dementia Education with Youth | Dementia Resources and Education on Social Media/Website | Virtual Dementia Experience |
|---|---|---|---|---|
| Implementation status | ||||
| Not Selected to Implement | 2 | 4 | 1 | 6 |
| Selected to Implement and NOT Implemented | 2 | 3 | 1 | 2 |
| Selected to Implement and Implemented | 4 | 1 | 6 | -- |
| Level of helpfulness | ||||
| Completely helpful | 2 | -- | 3 | -- |
| Very helpful | 1 | -- | 2 | -- |
| Moderately helpful | 1 | -- | -- | -- |
| Slightly helpful | -- | -- | -- | -- |
| Not helpful at all | -- | 1 | 1 | -- |
| Level of difficulty | ||||
| Not Difficult at All | 4 | -- | 4 | -- |
| Slightly Difficult | -- | -- | 1 | -- |
| Moderately Difficult | -- | 1 | 1 | -- |
| Very Difficult | -- | -- | -- | -- |
| Extremely Difficult (not able to implement) | -- | -- | -- | -- |
| Utility | ||||
| Extensively Utilizing | -- | -- | 3 | -- |
| Utilizing | 1 | -- | 1 | -- |
| Moderately Utilizing | 1 | 1 | 1 | -- |
| Somewhat Utilizing | -- | -- | -- | -- |
| Not Utilizing | 1 | -- | 1 | -- |
Appendix F
| Evaluation Survey Components | Shorten Service Length to 75 min. or Less | Simplify Sermons | Include Familiar Bible Verses | Support Staff Present | Increase Amount of Music | Modify Worship Service Order of Flow |
|---|---|---|---|---|---|---|
| Implementation status | ||||||
| Not Selected to Implement | -- | 1 | 5 | 7 | 3 | 3 |
| Selected to Implement and NOT Implemented | -- | 1 | -- | 1 | -- | -- |
| Selected to Implement and Implemented | 8 | 6 | 3 | -- | 5 | 5 |
| Level of helpfulness | ||||||
| Completely helpful | 4 | 3 | 2 | -- | 3 | 4 |
| Very helpful | 1 | 2 | 1 | -- | 2 | 1 |
| Moderately helpful | 1 | 1 | -- | -- | -- | -- |
| Slightly helpful | -- | -- | -- | -- | -- | -- |
| Not helpful at all | ||||||
| Level of difficulty | ||||||
| Not Difficult at All | 4 | 6 | 3 | -- | 4 | 3 |
| Slightly Difficult | 2 | -- | -- | -- | 1 | 1 |
| Moderately Difficult | -- | -- | -- | -- | -- | -- |
| Very Difficult | -- | -- | -- | -- | -- | -- |
| Extremely Difficult (not able to implement) | ||||||
| Utility | ||||||
| Extensively Utilizing | 6 | 4 | 3 | -- | 3 | 5 |
| Utilizing | -- | -- | -- | -- | -- | -- |
| Moderately Utilizing | -- | 1 | -- | -- | 2 | -- |
| Somewhat Utilizing | -- | 1 | -- | -- | -- | -- |
| Not Utilizing | -- | -- | -- | -- | -- | -- |
References
- Alzheimer’s Association. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. J. Alzheimers Assoc. 2021, 17, 327–406. [Google Scholar] [CrossRef] [PubMed]
- Matthews, K.A.; Xu, W.; Gaglioti, A.H.; Holt, J.B.; Croft, J.B.; Mack, D.; McGuire, L.C. Racial and ethnic estimates of Alzheimer’s disease and related dementias in the United States (2015–2060) in adults aged ≥65 years. Alzheimers Dement. 2019, 15, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Laditka, S.B.; Laditka, J.N.; Liu, R.; Price, A.E.; Friedman, D.B.; Wu, B.; Bryant, L.L.; Corwin, S.K.; Ivey, S.L. How do older people describe others with cognitive impairment? A multiethnic study in the United States. Ageing Soc. 2013, 33, 369–392. [Google Scholar] [CrossRef] [Green Version]
- Vickrey, B.G.; Strickland, T.L.; Fitten, L.J.; Adams, G.R.; Ortiz, F.; Hays, R.D. Ethnic variations in dementia caregiving experiences: Insights from focus groups. J. Hum. Behav. Soc. Environ. 2007, 15, 233–249. [Google Scholar] [CrossRef]
- Epps, F.; Foster, K.; Alexander, K.; Brewster, G.; Chester, M.; Thornton, J.; Aycock, D. Perceptions and attitudes toward dementia in predominantly African American congregants. J. Appl. Gerontol. 2021, 40, 0733464820987350. [Google Scholar] [CrossRef]
- Epps, F.; Alexander, K.; Brewster, G.S.; Parker, L.J.; Chester, M.; Tomlinson, A.; Adkins, A.; Zingg, S.; Thornton, J. Promoting dementia awareness in African American faith communities. Public Health Nurs. 2020, 37, 715–721. [Google Scholar] [CrossRef]
- Epps, F.; Williams, I.C. The importance of religiosity to the well-being of African American older adults living with dementia. J. Appl. Gerontol. 2020, 39, 509–518. [Google Scholar] [CrossRef]
- Weisman de Mamani, A.; Weintraub, M.J.; Maura, J.; Martinez de Andino, A.; Brown, C.A. The interplay among mindfulness, caregiver burden, and mental health in family members of individuals with dementia. Prof. Psychol. Res. Pract. 2018, 49, 116. [Google Scholar] [CrossRef]
- Parrill, R.; Kennedy, B.R. Partnerships for health in the African American community: Moving toward community-based participatory research. J. Cult. Divers. 2011, 18, 150–154. [Google Scholar]
- Williams, L.F.; Cousin, L. ‘A charge to keep I have’: Black pastors’ perceptions of their influence on health behaviors and outcomes in their churches and communities. J. Relig. Health 2021, 60, 1069–1082. [Google Scholar] [CrossRef]
- Sattin, R.W.; Williams, L.B.; Dias, J.; Garvin, J.T.; Marion, L.; Joshua, T.V.; Kriska, A.; Kramer, M.K.; Venkat Narayan, K.M. Community trial of a faith-based lifestyle intervention to prevent diabetes among African-Americans. J. Community Health 2016, 41, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler-Ajibade, P.; Booth, W.; Burwell, C. Partnering with the Black church: Recipe for promoting heart health in the stroke belt. Assoc. Black Nurs. Fac. J. 2012, 23, 34–37. [Google Scholar]
- Collins, W. The role of African American churches in promoting health among congregations. Soc. Work Christ. 2015, 42, 2. [Google Scholar]
- Fleming, R.; Bennett, K.; Preece, T.; Phillipson, L. The development and testing of the dementia friendly communities environment assessment tool (DFC EAT). Int. Psychogeriatr. 2017, 29, 303–311. [Google Scholar] [CrossRef]
- Su, D.; Garg, A.; Wiens, J.; Meyer, E.; Cai, G. Assessing health needs in African American churches: A mixed-methods study. J. Relig. Health 2021, 60, 1179–1197. [Google Scholar] [CrossRef] [PubMed]
- Epps, F.; Moore, M.; Chester, M.; Gore, J.; Sainz, M.; Adkins, A.; Clevenger, C.; Aycock, D. The Alter program: A nurse-led, dementia-friendly program for African American faith communities and families living with dementia. Nurs. Adm. Q. 2022, 46, 72–80. [Google Scholar] [CrossRef]
- Eccles, M.P.; Mittman, B.S. Welcome to implementation science. Implement. Sci. 2006, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Jull, J.; Giles, A.; Graham, I.D. Community-based participatory research and integrated knowledge translation: Advancing the co-creation of knowledge. Implement. Sci. 2017, 12, 150. [Google Scholar] [CrossRef] [Green Version]
- Stetler, C.B.; Legro, M.W.; Wallace, C.M.; Bowman, C.; Guihan, M.; Hagedorn, H.; Kimmel, B.; Sharp, N.D.; Smith, J.L. The role of formative evaluation in implementation research and the queri experience. J. Gen. Intern. Med. 2006, 21 (Suppl. 2), S1–S8. [Google Scholar] [CrossRef]
- Janus, M.; Brinkman, S. Evaluating early childhood education and care programs. In International Encyclopedia of Education, 3rd ed.; Peterson, P., Baker, E., McGaw, B., Eds.; Elsevier: Oxford, UK, 2010; pp. 25–31. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Harden, S.M.; Gaglio, B.; Rabin, B.; Smith, M.L.; Porter, G.C.; Ory, M.G.; Estabrooks, P.A. RE-AIM planning and evaluation framework: Adapting to new science and practice with a 20-year review. Front. Public Health 2019, 7, 64. [Google Scholar] [CrossRef] [Green Version]
- Holtrop, J.S.; Rabin, B.A.; Glasgow, R.E. Qualitative approaches to use of the RE-AIM framework: Rationale and methods. BMC Health Serv. Res. 2018, 18, 177. [Google Scholar] [CrossRef] [PubMed]
- Corbie-Smith, G.; Goldmon, M.; Isler, M.R.; Washington, C.; Ammerman, A.; Green, M.; Bunton, A. Partnerships in health disparities research and the roles of pastors of Black churches: Potential conflict, synergy, and expectations. J. Natl. Med. Assoc. 2010, 102, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Sands, L.P.; Albert, S.M.; Suitor, J.J. Understanding and addressing older adults’ needs during COVID-19. Innov. Aging 2020, 4, igaa019. [Google Scholar] [CrossRef] [PubMed]
- Vincenzo, J.L.; Hergott, C.; Schrodt, L.; Rohrer, B.; Brach, J.; Tripken, J.; Shirley, K.D.; Sidelinker, J.C.; Shubert, T.E. Capitalizing on virtual delivery of community programs to support health and well-being of older adults. Phys. Ther. 2021, 101, pzab001. [Google Scholar] [CrossRef]
- Holt, D.T.; Vardaman, J.M. Toward a comprehensive understanding of readiness for change: The case for an expanded conceptualization. J. Change Manag. 2013, 13, 9–18. [Google Scholar] [CrossRef]
- Walker, T.J.; Brandt, H.M.; Wandersman, A.; Scaccia, J.; Lamont, A.; Workman, L.; Dias, E.; Diamond, P.M.; Craig, D.W.; Fernandez, M.E. Development of a comprehensive measure of organizational readiness (motivation × capacity) for implementation: A study protocol. Implement. Sci. Commun. 2020, 1, 103. [Google Scholar] [CrossRef]
- Gilmore, G.D. Needs and Capacity Assessment Strategies for Health Education and Health Promotion, 4th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2011; Available online: https://www.amazon.com/Capacity-Assessment-Strategies-Education-Promotion/dp/1449646441 (accessed on 24 February 2022).
- Goldberg, J.M.; Sklad, M.; Elfrink, T.R.; Schreurs, K.M.; Bohlmeijer, E.T.; Clarke, A.M. Effectiveness of interventions adopting a whole school approach to enhancing social and emotional development: A meta-analysis. Eur. J. Psychol. Educ. 2019, 34, 755–782. [Google Scholar] [CrossRef] [Green Version]
- Stanhope, K.K.; Bettermann, E.; Stevenson, E.C.H.; Julius, S.D.; Kafi, A.; Kay, C.; Gazmararian, J.A. Feasibility of a multicomponent program to promote physical activity and nutrition in Georgia low-income early care and education settings. Child. Obes. 2018, 14, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Bruening, R.A.; Coronado, F.; Auld, M.E.; Benenson, G.; Simone, P.M. Health education workforce: Opportunities and challenges. Prev. Chronic. Dis. 2018, 15, 180045. [Google Scholar] [CrossRef]
- Hassan, E. Recall bias can be a threat to retrospective and prospective research designs. Internet J. Epidemiol. 2006, 3, 4. [Google Scholar] [CrossRef]
| Evaluation Question | Domain Assessed |
|---|---|
| Main: How can Alter™ best support partnering churches as the program continues to enroll more churches? | Focus group data about support from staff and the overall percentages of the activities and modifications |
| Sub: How helpful are the proposed program activities and modifications? | Percentage of activities identified as helpful to church and congregation members |
| Sub: How difficult is it to implement the proposed program activities and modifications at partnering churches? | Percentage of activities identified as difficult to implement for the church |
| Sub: How useful are the proposed program activities and modifications? | Percentage of activities identified as being used and how often they were used |
| Main: How did the COVID-19 pandemic impact participating churches’ ability to participate in the program fully? | Content analysis of survey short answer responses and focus groups. Number of times COVID-19 is referenced as impacting program activities or modifications |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gore, J.; Toliver, J.; Moore, M.A.; Aycock, D.; Epps, F. A Mixed-Methods Formative Evaluation of a Dementia-Friendly Congregation Program for Black Churches. Int. J. Environ. Res. Public Health 2022, 19, 4498. https://doi.org/10.3390/ijerph19084498
Gore J, Toliver J, Moore MA, Aycock D, Epps F. A Mixed-Methods Formative Evaluation of a Dementia-Friendly Congregation Program for Black Churches. International Journal of Environmental Research and Public Health. 2022; 19(8):4498. https://doi.org/10.3390/ijerph19084498
Chicago/Turabian StyleGore, Janelle, Jamilla Toliver, Miranda A. Moore, Dawn Aycock, and Fayron Epps. 2022. "A Mixed-Methods Formative Evaluation of a Dementia-Friendly Congregation Program for Black Churches" International Journal of Environmental Research and Public Health 19, no. 8: 4498. https://doi.org/10.3390/ijerph19084498