1. Introduction
Disruptive behavioral disorders are highly prevalent among preschool children [
1], and they are one of the most common reasons for referral to mental health services at this age [
2]. If untreated, behavioral problems have a high degree of persistence [
3], and increase the risk of developing mental health problems later in life such as anxiety disorders, depression, antisocial personality disorders, and addiction [
4]. Other long-term outcomes include academic difficulties [
5], unemployment and family problems [
6], as well as criminal and violent behavior into adolescence and adulthood [
7]. These outcomes result in high costs for mental health, law enforcement, educational and social services, and add to the necessity of effective, evidence-based interventions for behavioral problems at an early stage in the child’s development.
Parent training programs, which use the parents as the primary agent of change, have proven to be the most effective method for treating young children with behavioral problems [
8]. A widely used and evidence-based parent training program is parent−child interaction therapy (PCIT) [
9], originally developed for children aged between two and seven years. The treatment is based on both attachment [
10] and social learning [
11] theory, and is aimed at improving the quality of the parent−child relationship and teaching the parent effective parenting skills to better manage their child’s behavior [
12]. Multiple studies have shown medium to large effect sizes of PCIT in reducing the child’s disruptive behavior and parenting stress and improving parenting skills [
13], with growing evidence that PCIT prevents against child maltreatment [
14,
15,
16].
Despite its effectiveness, premature attrition from treatment remains a serious problem for PCIT, with attrition rates ranging from 27% to 69% [
17,
18,
19,
20]. Largely, these high attrition rates are a result of barriers most families referred to community mental health services face, due to low socioeconomic resources [
21]. These barriers to treatment are often very pragmatic, and include limitations in transportation, provision of childcare, and disruptions in work [
22,
23]. Furthermore, other problems such as financial or parental mental health problems might complicate staying motivated for treatment [
24]. To increase the accessibility and effectiveness of PCIT for families with low resources, a home-based adaptation of PCIT has been developed [
25]. The core principles of treatment of PCIT stay intact, but the home-based adaptation provides several key advantages compared to the traditional clinic-based PCIT: it eliminates the logistical barriers, it has strong ecological value because families are observed in their natural setting, while learned skills can be generalized faster to other situations and contexts [
21,
26]. Studies on home-based PCIT have shown similar outcomes compared to clinic-based PCIT, so the advantage is mostly found in reaching families otherwise difficult to reach. However, the results on lower rates of attrition for PCIT-Home compared to PCIT-Clinic have been inconclusive [
20,
21,
27,
28,
29,
30,
31]. Furthermore, PCIT has been adapted to a time-limited version, based on the less-is-more principle of Bakermans−Kranenburg [
32], which assumes that brief interventions with a moderate number of sessions and a clear end point are more effective than interventions with a large number of sessions. In this line, Abrahamse et al. [
33] examined the effectiveness of a time-limited, home-based adaptation of PCIT, with lower rates of attrition (15%), and a potentially protective effect against child maltreatment.
Home-based and time-limited adaptations of PCIT point to the importance of understanding the mechanisms and effective elements behind PCIT so it can be adjusted to the needs of specific families to make it more effective and prevent attrition. An important aspect of PCIT and its possible effect on treatment outcomes and attrition, which has not yet been investigated, is parental mentalization [
34]—the parent’s ability to represent and hold in mind the internal states of their child. PCIT acknowledges the importance of enhancing the parent−child relationship through positive changes enacted by the parent that support a sense of security in the child. This demands of the parent to become more attuned to their child’s psychological needs and responding to such signals in a predictable, consistent, and sensitive manner [
35]. Therefore, while not specifically highlighted in PCIT, the parental ability to take the perspective of the child or ‘to mentalize about the child’ might be a key prerequisite for the positive change in the parent’s behavior and for the efficacy of PCIT. In other words, we expect that parents who are less able to understand and take the perspective of their child are less able to change their behavior accordingly, and therefore will profit less from treatment or are at risk of premature attrition. To test these hypotheses, we performed a retrospective cohort study, investigating if parental mind-mindedness, which is a form of parental mentalization, affects the outcome of PCIT.
Mind-mindedness [
36] refers to the parents’ tendency to consider and to treat their children as individuals with an independent mind, rather than as entities with needs that must be met [
37,
38]. It can be measured by observing the parent−child interaction in a ‘free play session’ and coding systematically how often the parent makes a mind-related comment about the child (e.g., the child’s emotions, desires, intentions, thoughts) [
39]. Research shows that mind-mindedness is associated with the child’s development of social understanding, parent−child secure attachment (for a review, see [
40,
41]), language development, and school readiness [
42,
43]. There is also emerging evidence that mind-mindedness protects against the development of child behavior problems [
44,
45,
46,
47,
48]. Studies investigating parenting programs aimed at increasing mind-mindedness of parents with adopted or foster children showed improvements in children’s behavioral problems, attachment, and parenting stress [
49,
50,
51]. Mind-mindedness has not been measured or investigated in PCIT before.
The Present Study
The aim of the present study was to investigate to what extent a caregiver’s use of mind-mindedness measured before the start of treatment has an effect on the outcome of both parent−child interaction therapy provided in a time-limited, home-based setting (PCIT-Home) and in a clinic-based setting (PCIT-Clinic). We expected a caregiver’s use of mind-mindedness would have a moderating effect on the outcome measures, resulting in more decrease of the child’s behavioral problems, parenting stress, and mothers’ anxious and depressive symptoms, and more improvement in parenting skills. We also expected a group effect of mind-mindedness, with mothers with a medium-high level of mind-mindedness reporting fewer behavioral problems in their children, experiencing less parenting stress and anxious and depressive symptoms, and showing better parenting skills. Furthermore, we investigated whether mind-mindedness is associated with a lower risk of premature attrition and—for the PCIT-Clinic sample only—fewer sessions.
4. Statistical Approach
The data were analyzed using IBM SPSS Statistics, version 26 (IBM Corp., Armonk, NY, USA). Both datasets contained missing data: PCIT-Home 21.1% and PCIT-Clinic 11.9% (total missing values). The missing values were completely at random, with Little’s MCAR-test for PCIT-Home χ
2 (24) = 23.63,
p = 0.483 and for PCIT-Clinic χ
2 (82) = 84.31,
p = 0.409. Therefore, conditions were met to impute the missing data. We performed multiple imputation (MI), a method which has proven appropriate with small sample sizes and large proportions of missing data of up to 50% [
69]. Using MI, we created 5 copies of the original datasets, and missing values of the outcome variables in each dataset were replaced with independent random draws from the predictive distribution of the missing values under a specific model (the imputation model). These multiple results were combined into one dataset (one for PCIT-Home and one for PCIT-Clinic), which we used for our analyses. For the analyses of moderating effect of mind-mindedness on the different treatment outcomes, series of repeated measures analysis of variance (ANOVA) were conducted. For these analyses, the percentage of appropriate mind-mindedness was divided into two groups (MM-
low and MM-
high) by median. Post hoc analyses were conducted by means of adjusted SIDAK comparisons and alpha levels were adjusted using Tukey in the correlations. We performed additional sensitivity analyses with covariates to control for confounding. The effect sizes for the repeated measures ANOVA were presented in terms of partial eta squared (
ηp2: 0.01 =
small, 0.06 =
medium, 0.14 =
large).
Spearman nonparametric correlations were computed to test the relation between mind-mindedness and dropouts and (for PCIT-Clinic only) total sessions.
Assumptions relevant to all analyses were verified. The variables ECBI Intensity, ECBI Problem, OBVL, PSI-SF, DPICS Non-Compliance, DPICS Positive Following, and DPICS Negative Leading were normally distributed, with values of skewness/SE
skew and kurtosis/SE
kurt between −1.96 and +1.96 [
70]. Outlier scores (i.e., Z-scores exceeding ± 3) were replaced with scores one unit larger than the next most extreme score [
71].We found two variable outliers for PCIT-Home (DPICS Total Praise T1; DPICS Demandingness T3) and two for PCIT-Clinic (DPICS Inappropriate Child Behavior T2; ASR T3). The outliers were winsorized, after which the data were normally distributed. We applied winsorization, as this method allows weight modification without discarding the values of outliers, does not cause a bias based on under- or overestimation (e.g., trimming) and because the nature of the population distributions was not known (e.g., robust estimation method) [
72]. No multivariate outliers were found using Mahalanobis distance.
To test whether our samples had enough power to discern significant change between pre-, post-, and follow-up tests, we performed a power analysis using the program G*Power [
73]. We calculated power separately for PCIT-Home and PCIT-Clinic. Because we expected different correlations between the observational instrument (DPICS) and the questionnaires (ECBI, OBVL, PSI-SF, ASR), we also conducted separate calculations for these instruments. The power analysis was conducted for a repeated measures ANOVA with three repeated measures. We assumed an effect size of 0.30, an alpha of 0.05, and a power of 0.80. For the PCIT-Home sample, the mean correlation of the observational instrument was 0.30 between the pre-, post-, and follow-up tests, and for the questionnaires the mean correlation was 0.65. The power analyses indicated that a sample size of 20 children for the observational instrument, and a sample size of 12 children for the questionnaires, would be adequate to detect a significant difference between pre-, post-, and follow-up tests. For the PCIT-Clinic sample, the mean correlation of the observational instrument was 0.25 between the pre-, post-, and follow-up tests, and for the questionnaires the mean correlation was 0.50. Respectively, sample sizes of 22 children and of 16 children would be adequate to detect a significant difference between pre-, post-, and follow-up tests.
5. Results
5.1. Preliminary Analyses
We investigated whether mind-mindedness was correlated with the outcome variables at T1. For PCIT-Home, mind-mindedness was only significantly positively correlated with the parental DPICS subcategory ‘positive following’, r(18) = 0.53, p = 0.019. Mind-mindedness was not significantly related to all other outcome variables (ECBI Intensity, ECBI Problem, OBVL, DPICS subcategories ‘inappropriate behavior’, ‘child compliance, ‘negative leading’, ‘praise’, and ‘demandingness’). In the PCIT-Clinic sample, mind-mindedness was not significantly correlated to any of the outcome variables (ECBI Intensity, ECBI Problem, PSI-SF, ASR, and all the DPICS subcategories).
We also checked whether mind-mindedness was associated with mothers’ and child characteristics. In the PCIT-Home sample, mind-mindedness was significantly positively correlated with mothers’ educational level, r(17) = 0.47, p = 0.048, to family income, r(18) = 0.56, p = 0.012, and to relationship of the mother to the child, with foster mothers showing higher levels of mind-mindedness than biological mothers, r(18) = 0.49, p = 0.033. We found no significant correlations of mind-mindedness with mothers’ or child characteristics in the PCIT-Clinic sample.
5.2. Moderating and Group Effects of Mind-Mindedness
We examined the effect of parental level of mind-mindedness before the intervention (
high versus
low) as between factors in the outcome measures of the PCIT intervention, by performing a series of repeated measures ANOVA, with the PCIT intervention (pre-, post- and follow-up) as within factors.
Table 2 and
Table 3 present the repeated measures ANOVA results:
F-values for simple, group, and interaction effects with related effect sizes (partial eta squared). The median of mother’s percentage of appropriate mind-mindedness was 3.1 for the PCIT-Home and 2.3 for the PCIT-Clinic sample. The descriptive statistics are presented in the
Appendix A,
Table A1 and
Table A2.
5.2.1. PCIT-Home Sample
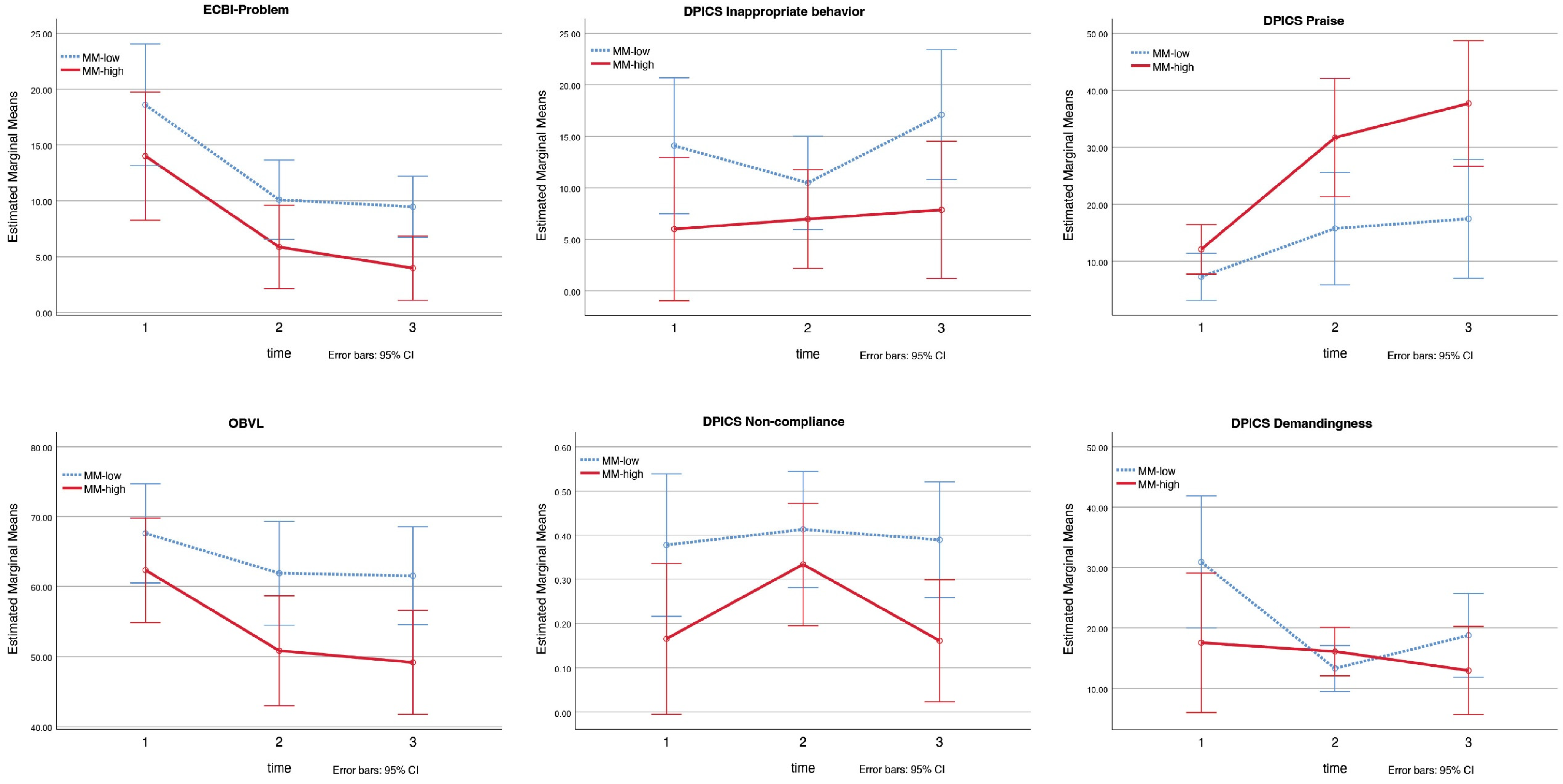
Table 2 shows the results of the repeated measures ANOVA for the PCIT-Home sample. A significant intervention effect of PCIT-Home was found for all outcome variables, except for the DPICS child subcategories ‘inappropriate behavior’ and ‘non-compliance’.
We found significant group effects of mind-mindedness for ECBI Problem,
F = 4.81,
ηp2 = 0.22,
p = 0.043, OBVL,
F = 4.56,
ηp2 = 0.21,
p = 0.048, the DPICS child subcategories ‘inappropriate behavior’,
F = 6.62,
ηp2 = 0.28,
p = 0.020 and ‘non-compliance’,
F = 10.47,
ηp2 = 0.38,
p = 0.005, and for the DPICS parental subcategory ‘praise’,
F = 8.43,
ηp2 = 0.33,
p = 0.010 (see
Figure 1). Compared to mothers with a medium-low level of mind-mindedness, mothers with a medium-high level of mind-mindedness reported lower scores on the ECBI Problem and OBVL, expressed higher levels of ‘praise’, and their children showed less ‘inappropriate behavior’ and ‘non-compliance’ on the DPICS at pre-, post-, and follow-up measurements. The group effects for ECBI Intensity and the DPICS parental subcategories ‘positive following’, ‘negative leading’, and ‘demandingness’ were not significant (see
Table 2 for
F,
ηp2,
p values).
A significant interaction effect of mind-mindedness was found for the DPICS parent subcategory ‘demandingness’,
F = 3.82,
ηp2 = 0.18,
p = 0.032 (see
Figure 1). Adjusted SIDAK comparisons showed that mothers with a medium-low level of mind-mindedness displayed significant less ‘demandingness’ at post-measurement than before the intervention (
Mpre = 30.90,
SE = 5.18,
Mpost = 13.30,
SE = 1.80),
p = 0.002. The interaction effects for the other variables (ECBI Intensity, ECBI Problem, OBVL, DPICS child subcategories ‘inappropriate behavior’ and ‘non-compliance’, DPICS parental subcategories ‘positive following’, ‘negative leading’, and ‘praise’) were not significant (see
Table 2 for
F,
ηp2,
p values).
5.2.2. PCIT-Clinic Sample
Table 3 presents the results of the repeated measures ANOVA for the PCIT-Clinic sample. A significant intervention effect of PCIT-Clinic was found for all outcome variables.
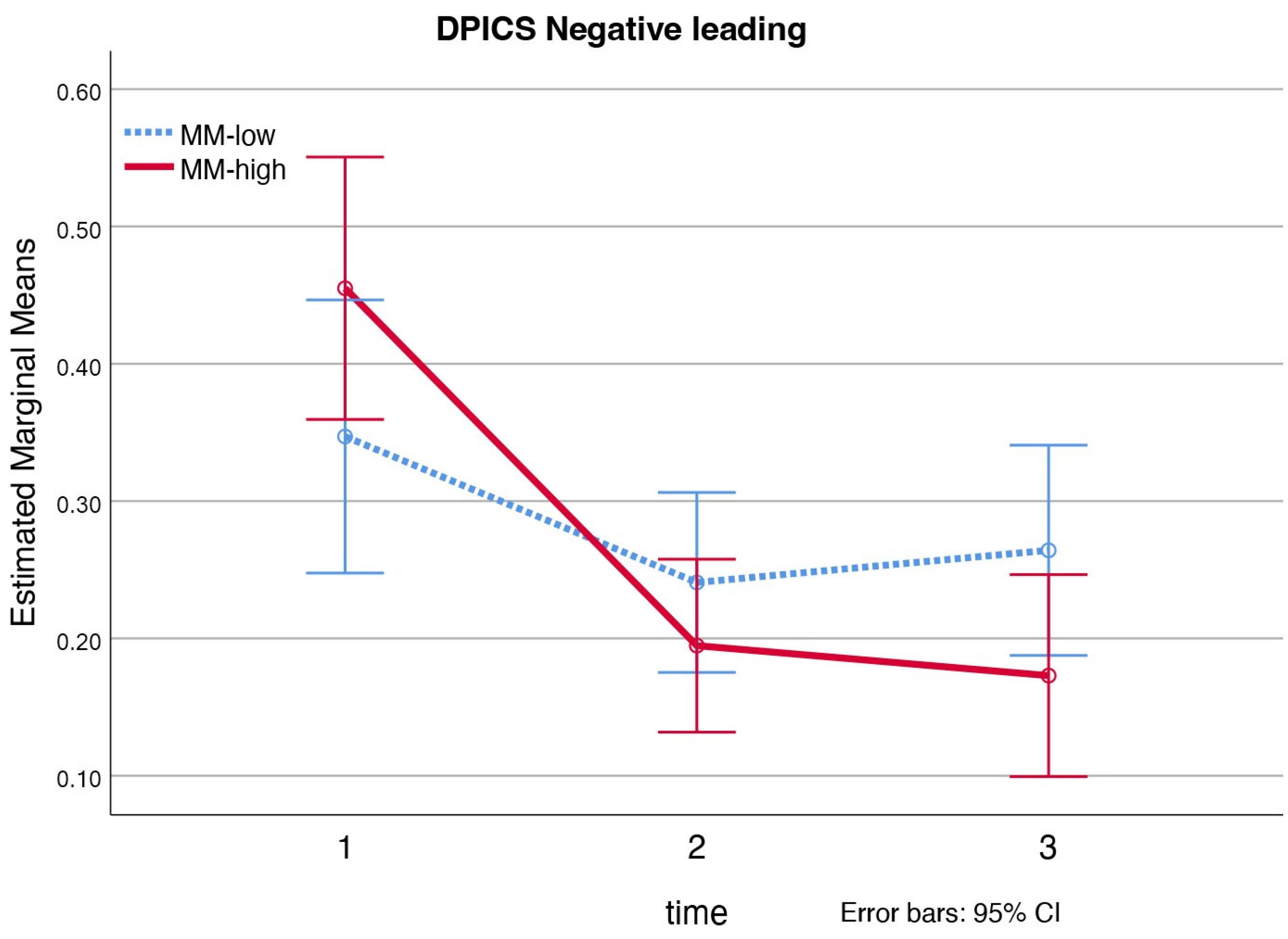
Looking at the quality of the parent−child interaction measured with the Dyadic Parent–Child Interaction Coding System (DPICS), a significant interaction effect of mind-mindedness was found for the parental subcategory ‘negative leading’,
F = 5.40,
ηp2 = 0.19,
p = 0.008 (see
Figure 2). Adjusted SIDAK comparisons show that mothers with a medium-high level of mind-mindedness, displayed significant more ‘negative leading’ before the intervention than at post-measurement (
Mpre = 0.46,
SE = 0.05,
Mpost = 0.19,
SE = 0.03),
p < 0.001, and at follow-up measurement (
Mfollow-up = 0.17,
SE = 0.04),
p < 0.001. No significant interaction effects of mind-mindedness were found for the child’s behavioral problems (ECBI Intensity, ECBI Problem), parenting stress (PSI-SF) and mother’s anxious and depressive symptoms (ASR).
Furthermore, no significant group effects of mind-mindedness were found (see
Table 3 for
F,
ηp2,
p values).
5.3. Premature Attrition and Total Sessions
In the PCIT-Clinic sample, treatment continues until the mastery criteria for successful treatment are met, resulting in a varying number of sessions between families that complete treatment. In the PCIT-Home sample, all families completing treatment received eight sessions in total according to treatment procedure. Accordingly, we performed analyses on associations between level of mind-mindedness and total number of sessions for the PCIT-Clinic sample only. Analyses on associations between level of mind-mindedness and premature attrition were performed for both samples.
5.3.1. PCIT-Home Sample
The PCIT-Home sample (n = 19) contained only three dropouts, which were all of mothers with a medium-high level of mind-mindedness (MM). Among the completers (n = 16), 37.5% were MM-high and 62.5% MM-low. A chi-square test of independence, showed mind-mindedness was significantly associated with dropouts, X2 (1, n = 19) = 4.0, φ = 0.46, p = 0.047.
5.3.2. PCIT-Clinic Sample
We investigated if the level of mind-mindedness (MM) was correlated with treatment dropouts, using the PCIT-Clinic sample which included both treatment completers and dropouts (n = 37). Mind-mindedness was distributed differently between treatment completers (n = 25; MM-high = 40.0%, MM-low = 60.0%;) and dropouts (n = 12; MM-high = 66.7%, MM-low = 33.3%). However, a chi-square test of independence showed that there was no significant association between mind-mindedness and dropouts, X2 (1, n = 37) = 2.3, φ = 0.25, p = 0.129.
To examine whether level of mind-mindedness had an effect on the total number of sessions for a successful treatment, we performed analyses with completers only (n = 25). The number of total sessions did not differ significantly between the two mind-mindedness groups (MM-high M = 19.39, MM-low M = 19.27), F(24) = 0.57, p = 0.974.
5.4. Sensitivity Analyses
For the PCIT-Home sample we performed sensitivity analyses with the educational level of the mother and the relationship of the mother to the child (biological/foster) as covariates to examine the robustness of our finding (see
Appendix A,
Table A3). We did not add family income as a covariate because it was already significantly correlated with educational level of the mother,
r(17) = 0.63,
p = 0.005. Due to missing data of the educational level of the mothers, the total sample for the sensitivity analyses was 18. Results of the sensitivity analyses were largely similar compared to the initial analyses, only the group effect for ECBI Problem and OBVL became non-significant. We did not include sensitivity analyses for the PCIT-Clinic sample, because for this sample mind-mindedness was not significantly correlated with the mothers’ or child’s characteristics or with any of the outcome measures.



{kind=link}
{kind=link}

