
The Childbirth Fear Questionnaire and the Wijma Delivery Expectancy Questionnaire as Screening Tools for Specific Phobia, Fear of Childbirth



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants
2.3. Procedures
2.4. Measures
2.5. Data Analysis Strategy
3. Results
3.1. Participants
3.2. Prevalence of Specific Phobia, Fear of Childbirth
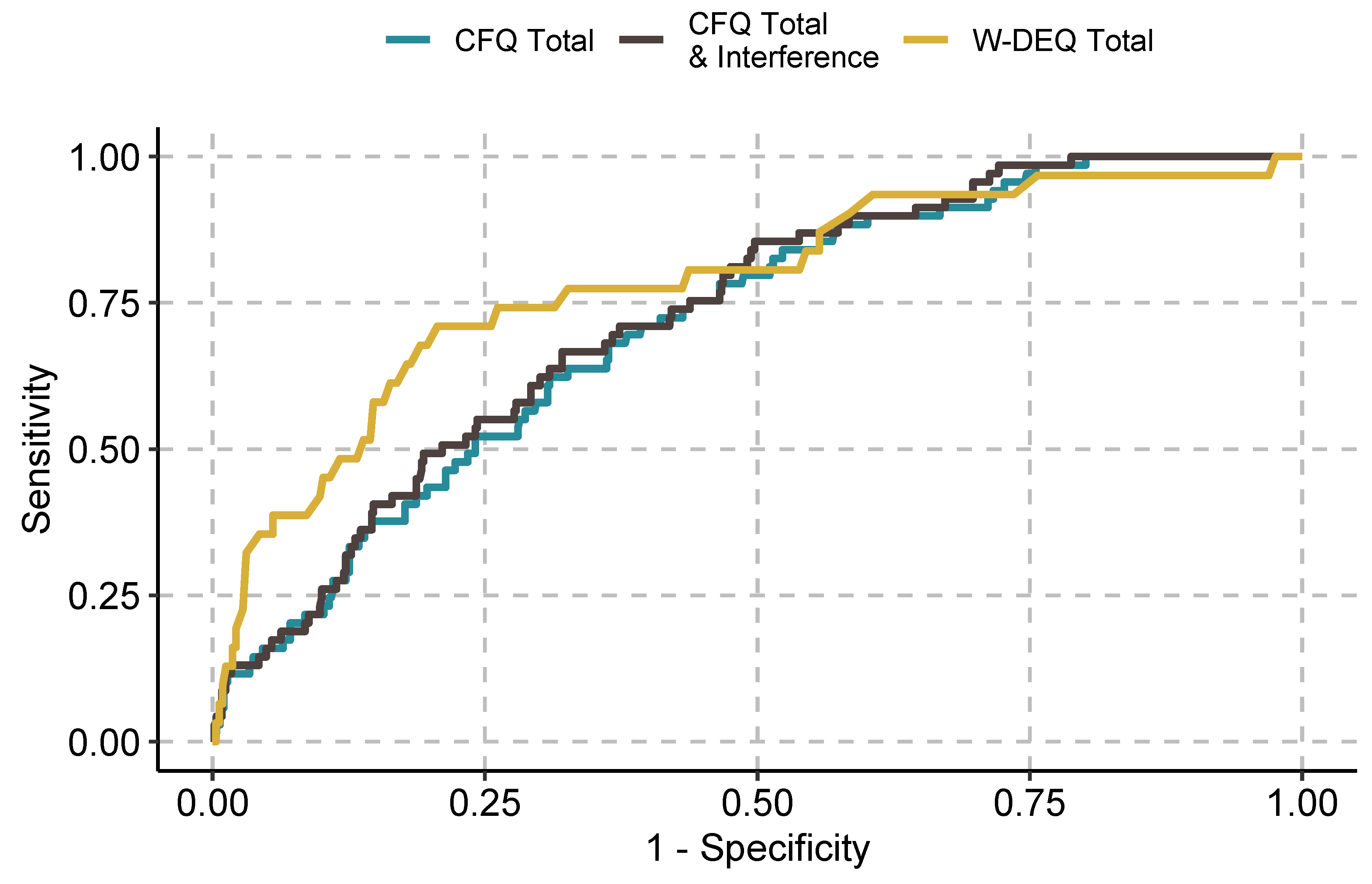
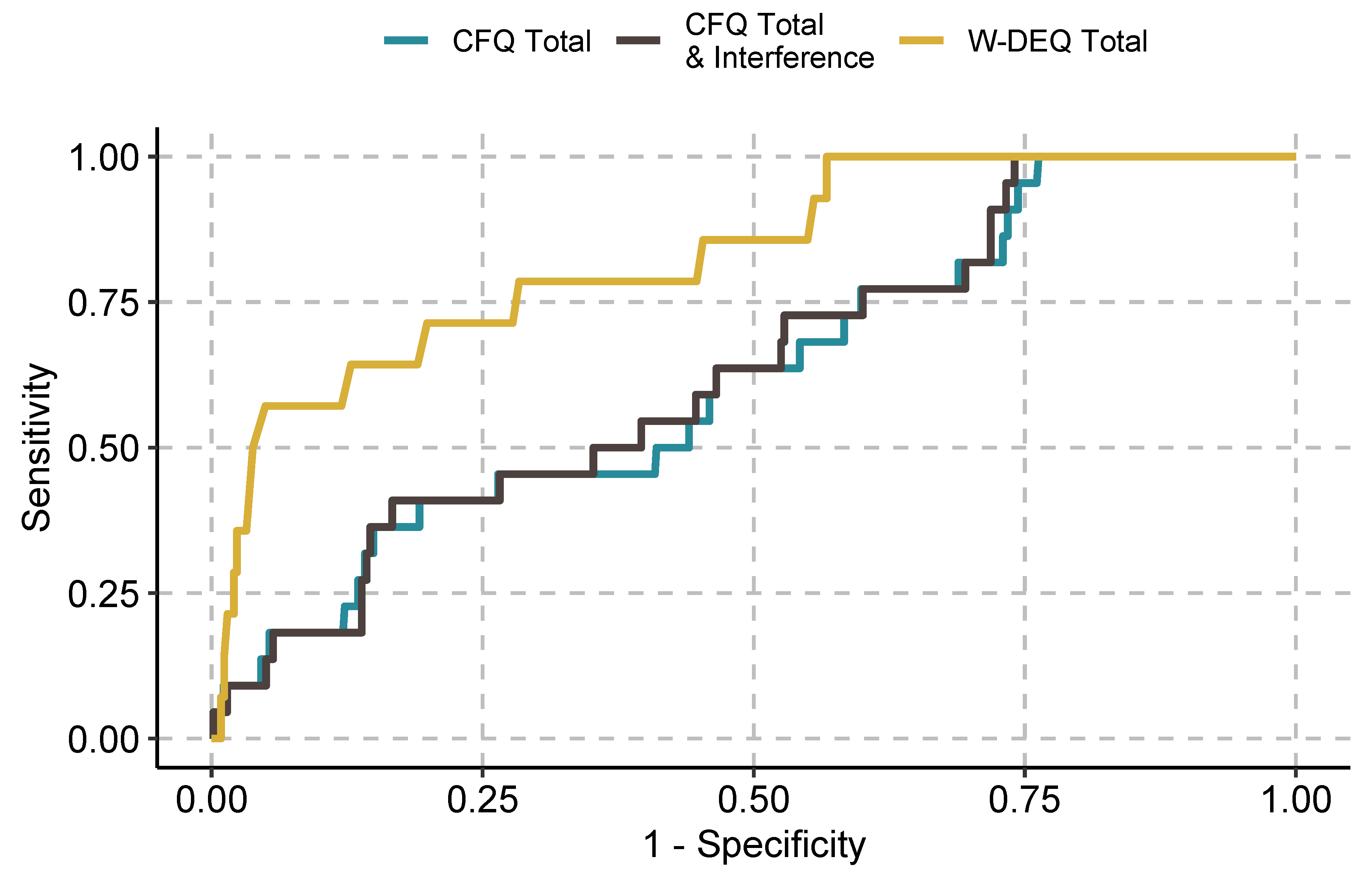
3.3. ROC Curves and Diagnostic Accuracy
4. Discussion
4.1. FoB: General Comments
4.2. Screening for FoB
4.3. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.-U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.; Fawcett, J.M. The Prevalence of Anxiety Disorders during Pregnancy and the Postpartum Period: A Multivariate Bayesian Meta-Analysis. J. Clin. Psychiatry 2019, 80, 1181. [Google Scholar] [CrossRef] [PubMed]
- Reck, C.; Struben, K.; Backenstrass, M.; Stefenelli, U.; Reinig, K.; Fuchs, T.; Sohn, C.; Mundt, C. Prevalence, onset and comorbidity of postpartum anxiety and depressive disorders. Acta Psychiatr. Scand. 2008, 118, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Fifer, S.K.; Mathias, S.D.; Patrick, D.L.; Mazonson, P.D.; Lubeck, D.P.; Buesching, D.P. Untreated Anxiety among Adult Primary Care Patients in a Health Maintenance Organization. Arch. Gen. Psychiatry 1994, 51, 740–750. [Google Scholar] [CrossRef]
- Demers, M. Frequent users of ambulatory health care in Quebec: The case of doctor-shoppers. Can. Med. Assoc. J. 1995, 153, 37–42. [Google Scholar]
- Fournier, L.; Lesage, A.D.; Toupin, J.; Cyr, M. Telephone Surveys as an Alternative for Estimating Prevalence of Mental Disorders and Service Utilization: A Montreal Catchment Area Study. Can. J. Psychiatry 1997, 42, 737–743. [Google Scholar] [CrossRef]
- Horenstein, A.; Heimberg, R.G. Anxiety disorders and healthcare utilization: A systematic review. Clin. Psychol. Rev. 2020, 81, 101894. [Google Scholar] [CrossRef]
- McCusker, J.; Boulenger, J.-P.; Boyer, R.; Bellavance, F.; Miller, J.-M. Use of health services for anxiety disorders: A multisite study in Quebec. Can. J. Psychiatry 1997, 42, 730–736. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Shapiro, C.M.; Kennedy, S. Differentiating DSM-IV Anxiety and Depressive Disorders in the General Population: Comorbidity and Treatment Consequences. Can. J. Psychiatry 2000, 45, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthey, S. Anxiety and Stress During Pregnancy and the Postpartum Period. In The Oxford Handbook of Perinatal Psychology; Oxford University Press: Oxford, UK, 2016. [Google Scholar] [CrossRef]
- Korja, R.; Nolvi, S.; Grant, K.A.; McMahon, C. The Relations Between Maternal Prenatal Anxiety or Stress and Child’s Early Negative Reactivity or Self-Regulation: A Systematic Review. Child Psychiatry Hum. Dev. 2017, 48, 851–869. [Google Scholar] [CrossRef] [PubMed]
- Erickson, N.; Gartstein, M.; Dotson, J.A.W. Review of Prenatal Maternal Mental Health and the Development of Infant Temperament. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 588–600. [Google Scholar] [CrossRef]
- Rees, S.; Channon, S.; Waters, C.S. The impact of maternal prenatal and postnatal anxiety on children’s emotional problems: A systematic review. Eur. Child Adolesc. Psychiatry 2019, 28, 257–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.-X.; Wu, Y.-L.; Xu, S.-J.; Zhu, R.-P.; Jia, X.-M.; Zhang, S.-F.; Huang, K.; Zhu, P.; Hao, J.-H.; Tao, F.-B. Maternal anxiety during pregnancy and adverse birth outcomes: A systematic review and meta-analysis of prospective cohort studies. J. Affect. Disord. 2014, 159, 103–110. [Google Scholar] [CrossRef]
- Mulder, E.J.H.; de Medina, P.G.R.; Huizink, A.C.; Bergh, B.R.H.V.D.; Buitelaar, J.K.; Visser, G.H.A. Prenatal maternal stress: Effects on pregnancy and the (unborn) child. Early Hum. Dev. 2002, 70, 3–14. [Google Scholar] [CrossRef]
- Schneider, M.L.; Moore, C.F.; Kraemer, G.W.; Roberts, A.D.; DeJesus, O.T. The impact of prenatal stress, fetal alcohol exposure, or both on development: Perspectives from a primate model. Psychoneuroendocrinology 2002, 27, 285–298. [Google Scholar] [CrossRef]
- Wadhwa, P.D.; Glynn, L.; Hobel, C.J.; Garite, T.J.; Porto, M.; Chicz-DeMet, A.; Wiglesworth, A.K.; Sandman, C.A. Behavioral perinatology: Biobehavioral processes in human fetal development. Regul. Pept. 2002, 108, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Adamson, B.; Letourneau, N.; Lebel, C. Prenatal maternal anxiety and children’s brain structure and function: A systematic review of neuroimaging studies. J. Affect. Disord. 2018, 241, 117–126. [Google Scholar] [CrossRef]
- O’Connor, T.G.; Heron, J.; Golding, J.; Glover, V.; the AL SPAC Study Team. Maternal antenatal anxiety and behavioural/emotional problems in children: A test of a programming hypothesis. J. Child Psychol. Psychiatry 2003, 44, 1025–1036. [Google Scholar] [CrossRef]
- O’Connor, T.G.; Heron, J.; Glover, V. Antenatal Anxiety Predicts Child Behavioral/Emotional Problems Independently of Postnatal Depression. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Grigoriadis, S.; Graves, L.; Peer, M.; Mamisashvili, L.; Tomlinson, G.; Vigod, S.N.; Dennis, C.-L.; Steiner, M.; Brown, C.; Cheung, A.; et al. A systematic review and meta-analysis of the effects of antenatal anxiety on postpartum outcomes. Arch. Women’s Ment. Health 2019, 22, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Matthey, S.; Barnett, B.; Howie, P.; Kavanagh, D. Diagnosing postpartum depression in mothers and fathers: Whatever happened to anxiety? J. Affect. Disord. 2003, 74, 139–147. [Google Scholar] [CrossRef]
- Robertson, E.; Grace, S.; Wallington, T.; Stewart, D.E. Antenatal risk factors for postpartum depression: A synthesis of recent literature. Gen. Hosp. Psychiatry 2004, 26, 289–295. [Google Scholar] [CrossRef]
- Sutter-Dallay, A.; Giaconne-Marcesche, V.; Glatigny-Dallay, E.; Verdoux, H. Women with anxiety disorders during pregnancy are at increased risk of intense postnatal depressive symptoms: A prospective survey of the MATQUID cohort. Eur. Psychiatry 2004, 19, 459–463. [Google Scholar] [CrossRef]
- Bánhidy, F.; Ács, N.; Puhó, E.; Czeizel, A.E. Association between maternal panic disorders and pregnancy complications and delivery outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 124, 47–52. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Lin, H.-C.; Lee, H.-C. Pregnancy outcomes among women with panic disorder—Do panic attacks during pregnancy matter? J. Affect. Disord. 2010, 120, 258–262. [Google Scholar] [CrossRef]
- Lilliecreutz, C.; Josefsson, A. Prevalence of blood and injection phobia among pregnant women. Acta Obstet. Gynecol. Scand. 2008, 87, 1276–1279. [Google Scholar] [CrossRef]
- Seng, J.; Oakley, D.J.; Sampselle, C.M.; Killion, C.; Graham-Bermann, S.; Liberzon, I. Posttraumatic stress disorder and pregnancy complications. Obstet. Gynecol. 2001, 97, 17–22. [Google Scholar] [CrossRef]
- Yonkers, K.A.; Blackwell, K.A.; Glover, J.; Forray, A. Antidepressant Use in Pregnant and Postpartum Women. Annu. Rev. Clin. Psychol. 2014, 10, 369–392. [Google Scholar] [CrossRef] [Green Version]
- Challacombe, F.L.; Salkovskis, P.M.; Woolgar, M.; Wilkinson, E.L.; Read, J.; Acheson, R. Parenting and mother-infant interactions in the context of maternal postpartum obsessive-compulsive disorder: Effects of obsessional symptoms and mood. Infant Behav. Dev. 2016, 44, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, R.D.; de Ávila Quevedo, L.; da Cunha Coelho, F.M.; Lopez, M.A.; da Silva, R.A.; Böhm, D.M.; Souza, L.D.D.M.; de Matos, M.B.; Pinheiro, K.A.T.; Pinheiro, R.T. Cognitive and language performance in children is associated with maternal social anxiety disorder: A study of young mothers in southern Brazil. Early Hum. Dev. 2015, 91, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Martini, J.; Knappe, S.; Beesdo-Baum, K.; Lieb, R.; Wittchen, H.-U. Anxiety disorders before birth and self-perceived distress during pregnancy: Associations with maternal depression and obstetric, neonatal and early childhood outcomes. Early Hum. Dev. 2010, 86, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Fairbrother, N.; Collardeau, F.; Albert, A.; Challacombe, F.L.; Thordarson, D.S.; Woody, S.; Janssen, P.A. High prevalence and incidence of OCD among women across pregnancy and postpartum. J. Clin. Psychiatry 2021, 82, 30368. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, K.; Berg, I.; Frankenstein, K.; Viita, L.; Larsson, K.; Persson, U.; Spånberger, L.; Wretman, A.; Silfvernagel, K.; Andersson, G.; et al. Internet-provided cognitive behaviour therapy of posttraumatic stress symptoms following childbirth—A randomized controlled trial. Cogn. Behav. Ther. 2016, 45, 287–306. [Google Scholar] [CrossRef]
- Searing, K.; Baukus, M.; Stark, M.A.; Morin, K.H.; Rudell, B. Needle Phobia during Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 592–598. [Google Scholar] [CrossRef]
- Arch, J.J. Pregnancy-specific anxiety: Which women are highest and what are the alcohol-related risks? Compr. Psychiatry 2013, 54, 217–228. [Google Scholar] [CrossRef]
- Räisänen, S.; Lehto, S.; Nielsen, H.; Gissler, M.; Kramer, M.; Heinonen, S.; Lehto, S. Fear of childbirth in nulliparous and multiparous women: A population-based analysis of all singleton births in Finland in 1997–2010. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 965–970. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, M.A.; Leahy-Warren, P.; Khashan, A.S.; Kenny, L.C.; O’Neill, S.M. Worldwide prevalence of tocophobia in pregnant women: Systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 907–920. [Google Scholar] [CrossRef] [Green Version]
- Clark, L.A.; Cuthbert, B.; Lewis-Fernández, R.; Narrow, W.E.; Reed, G.M. Three Approaches to Understanding and Classifying Mental Disorder: ICD-11, DSM-5, and the National Institute of Mental Health’s Research Domain Criteria (RDoC). Psychol. Sci. Public Interes. 2017, 18, 72–145. [Google Scholar] [CrossRef] [Green Version]
- Eaton, W.W.; Neufeld, K.; Chen, L.-S.; Cai, G. A Comparison of Self-report and Clinical Diagnostic Interviews for Depression: Diagnostic Interview Schedule and Schedules for Clinical Assessment in Neuropsychiatry in the Baltimore Epidemiologic Catchment Area Follow-Up. Arch. Gen. Psychiatry 2000, 57, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thombs, B.D.; Kwakkenbos, L.; Levis, A.W.; Benedetti, A. Addressing overestimation of the prevalence of depression based on self-report screening questionnaires. Can. Med. Assoc. J. 2018, 190, E44–E49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Challacombe, F.L.; Nath, S.; Trevillion, K.; Pawlby, S.; Howard, L.M. Fear of childbirth during pregnancy: Associations with observed mother-infant interactions and perceived bonding. Arch. Women’s Ment. Health 2020, 24, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Lukasse, M.; Schei, B.; Ryding, E.L. Prevalence and associated factors of fear of childbirth in six European countries. Sex. Reprod. Health 2014, 5, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, C.; Hessman, E.; Sjöblom, H.; Dencker, A.; Jangsten, E.; Mollberg, M.; Patel, H.; Sparud-Lundin, C.; Wigert, H.; Begley, C. Definitions, measurements and prevalence of fear of childbirth: A systematic review. BMC Pregnancy Childbirth 2018, 18, 28. [Google Scholar] [CrossRef]
- O’Connell, M.A.; Leahy-Warren, P.; Kenny, L.C.; O’Neill, S.M.; Khashan, A.S. The prevalence and risk factors of fear of childbirth among pregnant women: A cross-sectional study in Ireland. Acta Obstet. Gynecol. Scand. 2019, 98, 1014–1023. [Google Scholar] [CrossRef]
- Möller, L.; Josefsson, A.; Lilliecreutz, C.; Gunnervik, C.; Bladh, M.; Sydsjö, G. Reproduction, fear of childbirth and obstetric outcomes in women treated for fear of childbirth in their first pregnancy: A historical cohort. Acta Obstet. Gynecol. Scand. 2019, 98, 374–381. [Google Scholar] [CrossRef]
- Hofberg, K.; Ward, M.R. Fear of pregnancy and childbirth. Postgrad. Med. J. 2003, 79, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Zar, M.; Wijma, K.; Wijma, B. Pre- and Postpartum Fear of Childbirth in Nulliparous and Parous Women. Scand. J. Behav. Ther. 2001, 30, 75–84. [Google Scholar] [CrossRef]
- Adams, S.; Eberhard-Gran, M.; Eskild, A. Fear of childbirth and duration of labour: A study of 2206 women with intended vaginal delivery. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1238–1246. [Google Scholar] [CrossRef]
- Ryding, E.L.; Lukasse, M.; Van Parys, A.-S.; Wangel, A.-M.; Karro, H.; Kristjansdottir, H.; Schroll, A.-M.; Schei, B.; the Bidens Group. Fear of Childbirth and Risk of Cesarean Delivery: A Cohort Study in Six European Countries. Birth 2015, 42, 48–55. [Google Scholar] [CrossRef]
- Takegata, M.; Haruna, M.; Matsuzaki, M.; Shiraishi, M.; Okano, T.; Severinsson, E. Does Antenatal Fear of Childbirth Predict Postnatal Fear of Childbirth? A Study of Japanese Women. Open J. Nurs. 2015, 05, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Sydsjö, G.; Bladh, M.; Lilliecreutz, C.; Persson, A.-M.; Vyöni, H.; Josefsson, A. Obstetric outcomes for nulliparous women who received routine individualized treatment for severe fear of childbirth—A retrospective case control study. BMC Pregnancy Childbirth 2014, 14, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuglenes, D.; Aas, E.; Botten, G.; Øian, P.; Kristiansen, I.S. Why do some pregnant women prefer cesarean? The influence of parity, delivery experiences, and fear. Am. J. Obstet. Gynecol. 2011, 205, 45.e1–45.e9. [Google Scholar] [CrossRef] [PubMed]
- Haines, H.M.; Rubertsson, C.; Pallant, J.F.; Hildingsson, I. The influence of women’s fear, attitudes and beliefs of childbirth on mode and experience of birth. BMC Pregnancy Childbirth 2012, 12, 55. [Google Scholar] [CrossRef] [PubMed]
- Handelzalts, J.E.; Fisher, S.; Lurie, S.; Shalev, A.; Golan, A.; Sadan, O. Personality, fear of childbirth and cesarean delivery on demand. Acta Obstet. Gynecol. Scand. 2011, 91, 16–21. [Google Scholar] [CrossRef]
- Nieminen, K.; Stephansson, O.; Ryding, E.L. Women’s fear of childbirth and preference for cesarean section—A cross-sectional study at various stages of pregnancy in Sweden. Acta Obstet. Gynecol. Scand. 2009, 88, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, I.; Edman, G.; Andolf, E. Cesarean section on maternal request: Reasons for the request, self-estimated health, expectations, experience of birth and signs of depression among first-time mothers. Acta Obstet. Gynecol. Scand. 2007, 86, 451–456. [Google Scholar] [CrossRef]
- Saisto, T.; Salmela-Aro, K.; Nurmi, J.-E.; Halmesmäki, E. Psychosocial characteristics of women and their partners fearing vaginal childbirth. Br. J. Obstet. Gynaecol. 2001, 108, 492–498. [Google Scholar] [CrossRef]
- Salomonsson, B.; Gullberg, M.T.; Alehagen, S.; Wijma, K. Self-efficacy beliefs and fear of childbirth in nulliparous women. J. Psychosom. Obstet. Gynecol. 2013, 34, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Stoll, K.; Hauck, Y.; Downe, S.; Edmonds, J.; Gross, M.M.; Malott, A.; McNiven, P.; Swift, E.; Thomson, G.; Hall, W. Cross-cultural development and psychometric evaluation of a measure to assess fear of childbirth prior to pregnancy. Sex. Reprod. Health 2016, 8, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Otley, H. Fear of childbirth: Understanding the causes, impact and treatment. Br. J. Midwifery 2011, 19, 215–220. [Google Scholar] [CrossRef]
- Waldenström, U.; Hildingsson, I.; Ryding, E.L. Antenatal fear of childbirth and its association with subsequent caesarean section and experience of childbirth. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 638–646. [Google Scholar] [CrossRef]
- Størksen, H.T.; Garthus-Niegel, S.; Vangen, S.; Eberhard-Gran, M. The impact of previous birth experiences on maternal fear of childbirth. Acta Obstet. Gynecol. Scand. 2012, 92, 318–324. [Google Scholar] [CrossRef]
- Alipour, Z.; Lamyian, M.; Hajizadeh, E. Anxiety and fear of childbirth as predictors of postnatal depression in nulliparous women. Women Birth 2012, 25, e37–e43. [Google Scholar] [CrossRef]
- Ayers, S. Fear of childbirth, postnatal post-traumatic stress disorder and midwifery care. Midwifery 2014, 30, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Nath, S.; Busuulwa, P.; Ryan, E.G.; Challacombe, F.L.; Howard, L.M. The characteristics and prevalence of phobias in pregnancy. Midwifery 2020, 82, 102590. [Google Scholar] [CrossRef]
- Storksen, H.T.; Eberhard-Gran, M.; Garthus-Niegel, S.; Eskild, A. Fear of childbirth; the relation to anxiety and depression. Acta Obstet. Gynecol. Scand. 2012, 91, 237–242. [Google Scholar] [CrossRef]
- Rouhe, H.; Salmela-Aro, K.; Halmesmäki, E.; Saisto, T. Fear of childbirth according to parity, gestational age, and obstetric history. BJOG Int. J. Obstet. Gynaecol. 2008, 116, 67–73. [Google Scholar] [CrossRef]
- Fairbrother, N.; Thordarson, D.S.; Stoll, K. Fine tuning fear of childbirth: The relationship between Childbirth Fear Questionnaire subscales and demographic and reproductive variables. J. Reprod. Infant Psychol. 2018, 36, 15–29. [Google Scholar] [CrossRef]
- Jokić-Begić, N.; Žigić, L.; Radoš, S.N. Anxiety and anxiety sensitivity as predictors of fear of childbirth: Different patterns for nulliparous and parous women. J. Psychosom. Obstet. Gynecol. 2014, 35, 22–28. [Google Scholar] [CrossRef]
- Poikkeus, P.; Saisto, T.; Unkila-Kallio, L.; Punamaki, R.L.; Repokari, L.; Vilska, S.; Tiitinen, A.; Tulppala, M. Fear of Childbirth and Pregnancy-Related Anxiety in Women Conceiving with Assisted Reproduction. Obstet. Gynecol. 2006, 108, 70–76. [Google Scholar] [CrossRef]
- Gao, L.-L.; Liu, X.J.; Fu, B.L.; Xie, W. Predictors of childbirth fear among pregnant Chinese women: A cross-sectional questionnaire survey. Midwifery 2015, 31, 865–870. [Google Scholar] [CrossRef]
- Laursen, M.; Hedegaard, M.; Johansen, C.H. Fear of childbirth: Predictors and temporal changes among nulliparous women in the Danish National Birth Cohort. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 354–360. [Google Scholar] [CrossRef]
- Nerum, H.; Halvorsen, L.; Straume, B.; Sørlie, T.; Øian, P. Different labour outcomes in primiparous women that have been subjected to childhood sexual abuse or rape in adulthood: A case-control study in a clinical cohort. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 487–495. [Google Scholar] [CrossRef]
- Gourounti, K.; Kouklaki, E.; Lykeridou, K. Validation of the Childbirth Attitudes Questionnaire in Greek and psychosocial characteristics of pregnant women with fear of childbirth. Women Birth 2015, 28, e44–e51. [Google Scholar] [CrossRef]
- Lowe, N.K. Self-efficacy for labor and childbirth fears in nulliparous pregnant women. J. Psychosom. Obstet. Gynecol. 2000, 21, 219–224. [Google Scholar] [CrossRef]
- Heimstad, R.; Dahloe, R.; Laache, I.; Skogvoll, E.; Schei, B. Fear of childbirth and history of abuse: Implications for pregnancy and delivery. Acta Obstet. Gynecol. Scand. 2006, 85, 435–440. [Google Scholar] [CrossRef]
- Hall, W.A.; Hauck, Y.L.; Carty, E.M.; Hutton, E.K.; Fenwick, J.; Stoll, K. Childbirth Fear, Anxiety, Fatigue, and Sleep Deprivation in Pregnant Women. J. Obstet. Gynecol. Neonatal Nurs. 2009, 38, 567–576. [Google Scholar] [CrossRef]
- Qiu, L.; Sun, N.; Shi, X.; Zhao, Y.; Feng, L.; Gong, Y.; Yin, X. Fear of childbirth in nulliparous women: A cross-sectional multicentre study in China. Women Birth 2020, 33, e136–e141. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Calderani, E.; Giardinelli, L.; Scannerini, S.; Arcabasso, S.; Compagno, E.; Petraglia, F.; Ricca, V. Tocophobia in the DSM-5 era: Outcomes of a new cut-off analysis of the Wijma delivery expectancy/experience questionnaire based on clinical presentation. J. Psychosom. Res. 2019, 116, 37–43. [Google Scholar] [CrossRef]
- Hofberg, K.; Brockington, I.F. Tokophobia: An unreasoning dread of childbirth: A series of 26 cases. Br. J. Psychiatry 2000, 176, 83–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zar, M.; Wijma, K.; Wijma, B. Relations between anxiety disorders and fear of childbirth during late pregnancy. Clin. Psychol. Psychother. 2002, 9, 122–130. [Google Scholar] [CrossRef]
- World Health Organization. ICD-11. ICD-11 Classif Ment Behav Disord Clin Descr Diagn Guidel 2019. Available online: https://icd.who.int/en (accessed on 13 March 2022).
- Fairbrother, N.; Collardeau, F.; Albert, A.; Thordarson, D.S.; Stoll, K. Screening for Perinatal Anxiety Using the Childbirth Fear Questionnaire: A New Measure of Fear of Childbirth. Int. J. Environ. Res. Public Health 2022, 19, 2223. [Google Scholar] [CrossRef] [PubMed]
- Areskog, B.; Kjessler, B.; Uddenberg, N. Identification of Women with Significant Fear of Childbirth during Late Pregnancy. Gynecol. Obstet. Investig. 1982, 13, 98–107. [Google Scholar] [CrossRef]
- Elvander, C.; Cnattingius, S.; Kjerulff, K.H. Birth Experience in Women with Low, Intermediate or High Levels of Fear: Findings from the First Baby Study. Birth 2013, 40, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, C.; Westman, G.; Hamberg, K. Experiential factors associated with childbirth-related fear in Swedish women and men: A population based study. J. Psychosom. Obstet. Gynecol. 2005, 26, 63–72. [Google Scholar] [CrossRef]
- Hildingsson, I.; Nilsson, C.; Karlström, A.; Lundgren, I. A Longitudinal Survey of Childbirth-Related Fear and Associated Factors. J. Obstet. Gynecol. Neonatal Nurs. 2011, 40, 532–543. [Google Scholar] [CrossRef]
- Melender, H.-L. Experiences of Fears Associated with Pregnancy and Childbirth: A Study of 329 Pregnant Women. Birth 2002, 29, 101–111. [Google Scholar] [CrossRef]
- Prelog, P.R.; Makovec, M.R.; Šimic, M.V.; Premru-Srsen, T.; Perat, M. Individual and contextual factors of nulliparas’ levels of depression, anxiety and fear of childbirth in the last trimester of pregnancy: Intimate partner attachment a key factor? Slov. J. Public Health 2019, 58, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Wijma, K.; Wijma, B.; Zar, M. Psychometric aspects of the W-DEQ; a new questionnaire for the measurement of fear of childbirth. J. Psychosom. Obstet. Gynecol. 1998, 19, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Wootton, B.M.; Davis, E.; Moses, K.; Moody, A.; Maguire, P. The development and initial validation of the Tokophobia Severity Scale. Clin. Psychol. 2020, 24, 267–275. [Google Scholar] [CrossRef]
- Saxbe, D.; Horton, K.T.; Tsai, A.B. The Birth Experiences Questionnaire: A brief measure assessing psychosocial dimensions of childbirth. J. Fam. Psychol. 2018, 32, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Slade, P.; Pais, T.; Fairlie, F.; Simpson, A.; Sheen, K. The development of the Slade-Pais Expectations of Childbirth Scale (SPECS)*. J. Reprod. Infant Psychol. 2016, 34, 495–510. [Google Scholar] [CrossRef] [Green Version]
- Redshaw, M.; Martin, C.; Rowe, R.; Hockley, C. The Oxford Worries about Labour Scale: Women’s experience and measurement characteristics of a measure of maternal concern about labour and birth. Psychol. Health Med. 2009, 14, 354–366. [Google Scholar] [CrossRef]
- Austin, M.P.; Highet, N. ; Expert Working Group. Mental Health Care in the Perinatal Period: Australian Clinical Practice Guideline 2017; Centre of Perinatal Excellence: Melbourne, Australia, 2017. [Google Scholar]
- Hart, K.; Flynn, H.A. Screening, Assessment, and Diagnosis of Mood and Anxiety Disorders During Pregnancy and the Postpartum Period. In The Oxford Handbook of Perinatal Psychology; Oxford University Press: New York, NY, USA, 2016; pp. 319–340. [Google Scholar] [CrossRef]
- Stoll, K.; Fairbrother, N.; Thordarson, D.S. Childbirth Fear: Relation to Birth and Care Provider Preferences. J. Midwifery Women’s Health 2018, 63, 58–67. [Google Scholar] [CrossRef]
- Johnson, R.; Slade, P. Does fear of childbirth during pregnancy predict emergency caesarean section? BJOG Int. J. Obstet. Gynaecol. 2002, 109, 1213–1221. [Google Scholar] [CrossRef]
- Garthus-Niegel, S.; Størksen, H.T.; Torgersen, L.; Von Soest, T.; Eberhard-Gran, M. The Wijma Delivery Expectancy/Experience Questionnaire—A factor analytic study. J. Psychosom. Obstet. Gynecol. 2011, 32, 160–163. [Google Scholar] [CrossRef]
- McCabe, R.E.; Milosevic, I.; Rowa, K.; Shnaider, P.; Pawluk, E.J.; Antony, M.M. Diagnostic Assessment Research Tool (DART) 2017. Available online: https://healthsci.mcmaster.ca/docs/librariesprovider122/pdf/dart-instructions-current.pdf?sfvrsn=b95b406e_2 (accessed on 13 March 2022).
- Schneider, L.H.; Pawluk, E.J.; Milosevic, I.; Shnaider, P.; Rowa, K.; Antony, M.M.; Musielak, N.; McCabe, R.E. The Diagnostic Assessment Research Tool in action: A preliminary evaluation of a semistructured diagnostic interview for DSM-5 disorders. Psychol. Assess. 2022, 34, 21–29. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 24.0; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Bujang, M.A.; Adnan, T.H. Requirements for Minimum Sample Size for Sensitivity and Specificity Analysis. J. Clin. Diagn. Res. 2016, 10, YE01–YE06. [Google Scholar] [CrossRef]
- Holtman, G.A.; Berger, M.Y.; Burger, H.; Deeks, J.; Donner-Banzhoff, N.; Fanshawe, T.R.; Koshiaris, C.; Leeflang, M.M.; Oke, J.L.; Perera, R.; et al. Development of practical recommendations for diagnostic accuracy studies in low-prevalence situations. J. Clin. Epidemiol. 2019, 114, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Thiele, C. Cutpointr: Determine and Evaluate Optimal cutpoints in Binary Classification Tasks. R Package Version 1.0.32 2020:158. Available online: https://cran.r-project.org/web/packages/cutpointr/cutpointr.pdf (accessed on 13 March 2022).
- Fairbrother, N.; Corbyn, B.; Thordarson, D.S.; Ma, A.; Surm, D. Screening for perinatal anxiety disorders: Room to grow. J. Affect. Disord. 2019, 250, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.L.; Rosenberg, W.; Gray, J.A.M.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Räisänen, S.; Lehto, S.M.; Nielsen, H.S.; Gissler, M.; Kramer, M.R.; Heinonen, S. Risk factors for and perinatal outcomes of major depression during pregnancy: A population-based analysis during 2002–2010 in Finland. BMJ Open 2014, 4, e004883. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | ||
|---|---|---|
| Percentage | n | |
| Married or cohabitating | 93.3% | 613 |
| Cis-gender female | 99.1% | 652 |
| Some postsecondary education | 94.4% | 623 |
| European heritage | 76.3% | 502 |
| English spoken at home | 95.4% | 629 |
| Current Pregnancy | ||
| Singleton pregnancy | 97.7% | 642 |
| Weeks pregnant: M (SD) | 34.6 (2.1) | 497 |
| Pregnancy complications | 30.8% | 202 |
| Reproductive History | ||
| Prior births | 52.3% | 296 |
| Prior vaginal birth | 51.2% | 198 |
| Prior cesarean birth | 17.7% | 66 |
| Prior pregnancy loss < 20 weeks | 40.6% | 157 |
| Prior pregnancy loss > 20 weeks | 1.3% | 5 |
| Full Sample M (SD) | Nullips Only M (SD) | Multips Only M (SD) | |
|---|---|---|---|
| CFQ Total | 1.11 (0.59) | 1.23 (0.61) | 1.02 (0.56) |
| CFQ Interference | 0.42 (0.47) | 0.44 (0.47) | 0.39 (0.45) |
| W-DEQ | 55.44 (23.76) | 59.07 (22.77) | 52.8 (24.09) |
| Prevalence | AUC | J | Cutpoint | Sensitivity | Specificity | NPV | LR+ | ||
|---|---|---|---|---|---|---|---|---|---|
| CFQ Total Scores | Full sample | 3.3% | 0.63 | 0.11 | 1.17 | 0.56 | 0.55 | 0.97 | 1.24 |
| Nulliparous only | 1.9% | 0.45 | 0.45 | 1.34 | 0.60 | 0.45 | 0.98 | 1.09 | |
| Multiparous only | 5.0% | 0.67 | 0.17 | 1.05 | 0.60 | 0.57 | 0.96 | 1.40 | |
| CFQ Total & Interference Subscale Scores | Full sample | 3.3% | 0.62 | 0.10 | 1.13 | 0.53 | 0.57 | 0.97 | 1.23 |
| Nulliparous only | 1.9% | 0.56 | 0.23 | 0.69 | 1.00 | 0.23 | 1.0 | 1.30 | |
| Multiparous only | 5.0% | 0.69 | 0.35 | 1.63 | 0.47 | 0.89 | 0.97 | 4.27 | |
| W-DEQ | Full sample | 3.9% | 0.82 | 0.43 | 78.87 | 0.62 | 0.81 | 0.98 | 3.26 |
| Nulliparous only | 2.5% | 0.88 | 0.69 | 95.37 | 0.75 | 0.94 | 0.99 | 12.50 | |
| Multiparous only | 5.9% | 0.83 | 0.53 | 76.56 | 0.70 | 0.83 | 0.98 | 4.12 |
| Prevalence | AUC | J | Cutpoint | Sensitivity | Specificity | NPV | LR+ | ||
|---|---|---|---|---|---|---|---|---|---|
| CFQ Total Scores | Full sample | 10.0% | 0.72 | 0.29 | 1.18 | 0.29 | 0.69 | 0.90 | 0.94 |
| Nulliparous only | 8.0% | 0.75 | 0.30 | 1.46 | 0.66 | 0.64 | 0.96 | 1.83 | |
| Multiparous only | 12.0% | 0.71 | 0.26 | 1.13 | 0.63 | 0.63 | 0.93 | 1.70 | |
| CFQ Total & Interference Subscale Scores | Full sample | 10.0% | 0.73 | 0.30 | 1.13 | 0.69 | 0.61 | 0.95 | 1.77 |
| Nulliparous only | 8.0% | 0.77 | 0.37 | 1.38 | 0.71 | 0.66 | 0.96 | 2.09 | |
| Multiparous only | 12.0% | 0.73 | 0.30 | 1.05 | 0.67 | 0.63 | 0.93 | 1.81 | |
| W-DEQ Total Scores | Full sample | 9.0% | 0.79 | 0.47 | 73.59 | 0.68 | 0.79 | 0.96 | 3.24 |
| Nulliparous only | 7.0% | 0.68 | 0.26 | 81.51 | 0.44 | 0.82 | 0.95 | 2.44 | |
| Multiparous only | 11.0% | 0.88 | 0.53 | 70.62 | 0.74 | 0.79 | 0.96 | 3.52 |
| CFQ Total & Interference Subscale Scores | |||||||||
| Prevalence | AUC | J | Cutpoint | Sensitivity | Specificity | NPV | LR+ | ||
| Fear of Vaginal Birth | Full sample | 3.2% | 0.81 | 0.43 | 1.38 | 0.71 | 0.72 | 0.99 | 2.54 |
| Nulliparous only | 1.5% | 0.88 | 0.67 | 1.42 | 1.00 | 0.67 | 1.00 | 3.03 | |
| Multiparous only | 4.1% | 0.80 | 0.44 | 1.38 | 0.67 | 0.77 | 0.98 | 2.91 | |
| Fear of cesarean birth | Full sample | 6.9% | 0.71 | 0.27 | 1.04 | 0.73 | 0.54 | 0.96 | 1.59 |
| Nulliparous only | 4.9% | 0.78 | 0.49 | 1.51 | 0.77 | 0.72 | 0.98 | 2.75 | |
| Multiparous only | 8.6% | 0.73 | 0.39 | 0.94 | 0.84 | 0.55 | 0.97 | 1.87 | |
| W-DEQ | |||||||||
| Prevalence | AUC | J | Cutpoint | Sensitivity | Specificity | NPV | LR+ | ||
| Fear of Vaginal Birth | Full sample | 4.2% | 0.86 | 0.56 | 78.87 | 0.74 | 0.83 | 0.99 | 4.35 |
| Nulliparous only | 2.5% | 0.73 | 0.70 | 96.36 | 0.75 | 0.95 | 0.99 | 15.0 | |
| Multiparous only | 5.3% | 0.92 | 0.70 | 75.24 | 0.89 | 0.81 | 0.99 | 4.68 | |
|
SP Diagnostic Status Dichotomized (FULL&SUB versus NOT)–Reduced Model |
Fear of CS Birth Dichotomized (FULL&SUB versus NOT)–Reduced Model | |||||
|---|---|---|---|---|---|---|
| Predictors | Log-Odds | CI | p | Log-Odds | CI | p |
| (Intercept) | −6.23 | −8.18–−4.69 | <0.001 | −8.96 | −13.09–−6.18 | <0.001 |
| INT | 1.31 | 0.48–2.22 | 0.003 | 1.31 | 0.32–2.43 | 0.01 |
| CS | 0.62 | 0.09–1.19 | 0.03 | 1.57 | 0.68–2.71 | 0.002 |
| INTERFERENCE | 1.01 | 0.08–1.97 | 0.03 | |||
| Observations | 267 | 267 | ||||
| R2 Tjur | 0.25 | 0.27 | ||||
| AUC | 0.87 | Cases correctly classified:
| 0.94 | Cases correctly classified:
| ||
| Optimal cutpoint | 0.10 | 0.12 | ||||
| Youden’s index | 0.51 | 0.65 | ||||
| Sensitivity | 0.69 | 0.80 | ||||
| Specificity | 0.82 | 0.85 | ||||
| SP Diagnostic Status Dichotomized (FULL&SUB versus NOT)–Reduced Model | Fear of Vaginal Birth Dichotomized (FULL&SUB versus NOT)–Reduced Model | Fear of Cesarean Birth Dichotomized (FULL&SUB versus NOT)–Reduced Model | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Predictors | Log-Odds | CI | p | Log-Odds | CI | p | Log-Odds | CI | p |
| (Intercept) | −3.83 | −4.86–−2.96 | <0.001 | −5.89 | −8.38–−4.02 | <0.001 | −3.25 | −4.07–−2.54 | <0.001 |
| SEX | −1.1 | −1.96–−0.36 | 0.007 | −0.72 | −1.59–0.01 | 0.074 | |||
| PAIN | 0.76 | 0.33–1.21 | 0.001 | 1.03 | 0.39–1.75 | 0.003 | |||
| HARM | 1.29 | 0.08–2.61 | 0.044 | ||||||
| CS | −0.79 | −1.65–−0.05 | 0.049 | ||||||
| DEATH | −1.02 | −2.18–−0.01 | 0.063 | ||||||
| INTERFERENCE | 2.48 | 1.66–3.39 | <0.001 | 2.43 | 1.09–4.00 | 0.001 | 2.31 | 1.48–3.21 | <0.001 |
| Observations | 291 | 291 | 291 | ||||||
| R2 Tjur | 0.24 | 0.239 | 0.16 | ||||||
| AUC | 0.84 | Cases correctly classified:
| 0.92 | Cases correctly classified:
| 0.79 | Cases correctly classified:
| |||
| Optimal cutpoint | 0.15 | 0.07 | 0.10 | ||||||
| Youden’s index | 0.42 | 0.67 | 0.41 | ||||||
| Sensitivity | 0.62 | 0.77 | 0.61 | ||||||
| Specificity | 0.82 | 0.90 | 0.80 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fairbrother, N.; Albert, A.; Collardeau, F.; Keeney, C. The Childbirth Fear Questionnaire and the Wijma Delivery Expectancy Questionnaire as Screening Tools for Specific Phobia, Fear of Childbirth. Int. J. Environ. Res. Public Health 2022, 19, 4647. https://doi.org/10.3390/ijerph19084647
Fairbrother N, Albert A, Collardeau F, Keeney C. The Childbirth Fear Questionnaire and the Wijma Delivery Expectancy Questionnaire as Screening Tools for Specific Phobia, Fear of Childbirth. International Journal of Environmental Research and Public Health. 2022; 19(8):4647. https://doi.org/10.3390/ijerph19084647
Chicago/Turabian StyleFairbrother, Nichole, Arianne Albert, Fanie Collardeau, and Cora Keeney. 2022. "The Childbirth Fear Questionnaire and the Wijma Delivery Expectancy Questionnaire as Screening Tools for Specific Phobia, Fear of Childbirth" International Journal of Environmental Research and Public Health 19, no. 8: 4647. https://doi.org/10.3390/ijerph19084647