
Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999–2018

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Measures
2.3. Statistical Analyses
3. Results
3.1. Prevalence of Cardiometabolic Multimorbidity in the U.S., 2017–2018
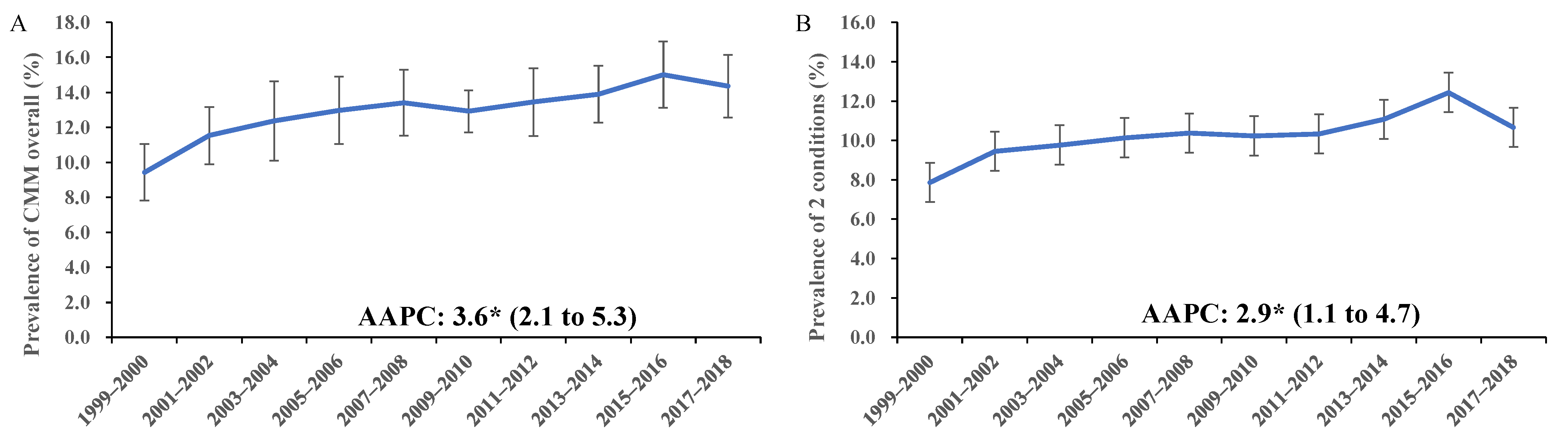
3.2. Trend in the Prevalence of Cardiometabolic Multimorbidity in the U.S., 1999–2018
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Researches
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glynn, L.G. Multimorbidity: Another key issue for cardiovascular medicine. Lancet 2009, 374, 1421–1422. [Google Scholar] [CrossRef]
- Lyall, D.M.; Celis-Morales, C.A.; Anderson, J.; Gill, J.M.; Mackay, D.F.; McIntosh, A.M.; Smith, D.J.; Deary, I.J.; Sattar, N.; Pell, J.P. Associations between single and multiple cardiometabolic diseases and cognitive abilities in 474 129 UK Biobank participants. Eur. Heart J. 2017, 38, 577–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Z.T.; Luo, Y.; Han, L.; Wang, K.; Yao, S.S.; Su, H.X.; Chen, S.; Cao, G.Y.; De Fries, C.M.; Chen, Z.S.; et al. Patterns of cardiometabolic multimorbidity and the risk of depressive symptoms in a longitudinal cohort of middle-aged and older Chinese. J. Affect. Disord. 2022, 301, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Maddaloni, E.; D’Onofrio, L.; Alessandri, F.; Mignogna, C.; Leto, G.; Pascarella, G.; Mezzaroma, I.; Lichtner, M.; Pozzilli, P.; Agro, F.E.; et al. Cardiometabolic multimorbidity is associated with a worse Covid-19 prognosis than individual cardiometabolic risk factors: A multicentre retrospective study (CoViDiab II). Cardiovasc. Diabetol. 2020, 19, 164. [Google Scholar] [CrossRef] [PubMed]
- McQueenie, R.; Foster, H.M.E.; Jani, B.D.; Katikireddi, S.V.; Sattar, N.; Pell, J.P.; Ho, F.K.; Niedzwiedz, C.L.; Hastie, C.E.; Anderson, J.; et al. Multimorbidity, polypharmacy, and COVID-19 infection within the UK Biobank cohort. PLoS ONE 2020, 15, e0238091. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration; Di Angelantonio, E.; Kaptoge, S.; Wormser, D.; Willeit, P.; Butterworth, A.S.; Bansal, N.; O’Keeffe, L.M.; Gao, P.; Wood, A.M.; et al. Association of Cardiometabolic Multimorbidity With Mortality. JAMA 2015, 314, 52–60. [Google Scholar] [CrossRef]
- Oishi, Y.; Manabe, I. Organ System Crosstalk in Cardiometabolic Disease in the Age of Multimorbidity. Front. Cardiovasc. Med. 2020, 7, 64. [Google Scholar] [CrossRef]
- Janjusevic, M.; Fluca, A.L.; Gagno, G.; Pierri, A.; Padoan, L.; Sorrentino, A.; Beltrami, A.P.; Sinagra, G.; Aleksova, A. Old and Novel Therapeutic Approaches in the Management of Hyperglycemia, an Important Risk Factor for Atherosclerosis. Int. J. Mol. Sci. 2022, 23, 2336. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieslar, G.; Stanek, A. Pathogenesis and Clinical Significance of In-Stent Restenosis in Patients with Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Ferrannini, E.; Cushman, W.C. Diabetes and hypertension: The bad companions. Lancet 2012, 380, 601–610. [Google Scholar] [CrossRef]
- Sakakibara, B.M.; Obembe, A.O.; Eng, J.J. The prevalence of cardiometabolic multimorbidity and its association with physical activity, diet, and stress in Canada: Evidence from a population-based cross-sectional study. BMC Public Health 2019, 19, 1361. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Jehan, I.; de Silva, H.A.; Naheed, A.; Farazdaq, H.; Hirani, S.; Kasturiratne, A.; Ranasinha, C.D.; Islam, M.T.; Siddiquee, A.T.; et al. Prevalence and correlates of cardiometabolic multimorbidity among hypertensive individuals: A cross-sectional study in rural South Asia-Bangladesh, Pakistan and Sri Lanka. BMJ Open 2019, 9, e030584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Tang, X.; Shen, P.; Si, Y.; Liu, X.; Xu, Z.; Wu, J.; Zhang, J.; Lu, P.; Lin, H.; et al. Multimorbidity of cardiometabolic diseases: Prevalence and risk for mortality from one million Chinese adults in a longitudinal cohort study. BMJ Open 2019, 9, e024476. [Google Scholar] [CrossRef] [Green Version]
- About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 28 March 2022).
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. National Health and Nutrition Examination Survey: Plan and Operations, 1999–2010; CDC: Atlanta, GA, USA, 2013; pp. 1–37. [Google Scholar]
- Perloff, D.; Grim, C.; Flack, J.; Frohlich, E.D.; Hill, M.; McDonald, M.; Morgenstern, B.Z. Human blood pressure determination by sphygmomanometry. Circulation 1993, 88, 2460–2470. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.L.; Carroll, M.D.; Kruszon-Moran, D.; Dohrmann, S.M.; Curtin, L.R. National Health and Nutrition Examination Survey: Analytic Guidelines, 1999–2010; CDC: Atlanta, GA, USA, 2013; pp. 1–24. [Google Scholar]
- Ingram, D.D.; Malec, D.J.; Makuc, D.M.; Kruszon-Moran, D.; Gindi, R.M.; Albert, M.; Beresovsky, V.; Hamilton, B.E.; Holmes, J.; Schiller, J.; et al. National Center for Health Statistics Guidelines for Analysis of Trends; CDC: Atlanta, GA, USA, 2018; pp. 1–71. [Google Scholar]
- National Health and Nutrition Examination Survey, Specific Considerations for Analyzing NHANES Data. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/Module6.aspx (accessed on 1 January 2022).
- Underlying Cause of Death 1999–2020. Available online: https://wonder.cdc.gov/wonder/help/ucd.html#Unreliable (accessed on 1 January 2022).
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Yang, L.; Sun, J.; Zhao, M.; Magnussen, C.G.; Xi, B. Trends in Cardiometabolic and Cancer Multimorbidity Prevalence and Its Risk with All-Cause and Cause-Specific Mortality in U.S. Adults: Prospective Cohort Study. Front. Cardiovasc. Med. 2021, 8, 731240. [Google Scholar] [CrossRef]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Larsen, F.B.; Pedersen, M.H.; Friis, K.; Glumer, C.; Lasgaard, M. A Latent Class Analysis of Multimorbidity and the Relationship to Socio-Demographic Factors and Health-Related Quality of Life. A National Population-Based Study of 162,283 Danish Adults. PLoS ONE 2017, 12, e0169426. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Fayosse, A.; Sabia, S.; Tabak, A.; Shipley, M.; Dugravot, A.; Kivimaki, M. Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: A cohort study. PLoS Med. 2018, 15, e1002571. [Google Scholar] [CrossRef]
- Chudasama, Y.V.; Khunti, K.; Gillies, C.L.; Dhalwani, N.N.; Davies, M.J.; Yates, T.; Zaccardi, F. Healthy lifestyle and life expectancy in people with multimorbidity in the UK Biobank: A longitudinal cohort study. PLoS Med. 2020, 17, e1003332. [Google Scholar] [CrossRef] [PubMed]
- Chudasama, Y.V.; Zaccardi, F.; Gillies, C.L.; Dhalwani, N.N.; Yates, T.; Rowlands, A.V.; Davies, M.J.; Khunti, K. Leisure-time physical activity and life expectancy in people with cardiometabolic multimorbidity and depression. J. Intern. Med. 2020, 287, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Whitty, C.J.M.; MacEwen, C.; Goddard, A.; Alderson, D.; Marshall, M.; Calderwood, C.; Atherton, F.; McBride, M.; Atherton, J.; Stokes-Lampard, H.; et al. Rising to the challenge of multimorbidity. BMJ 2020, 368, l6964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Back, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Wang, L.; Li, X.; Wang, Z.; Bancks, M.P.; Carnethon, M.R.; Greenland, P.; Feng, Y.Q.; Wang, H.; Zhong, V.W. Trends in Prevalence of Diabetes and Control of Risk Factors in Diabetes Among US Adults, 1999–2018. JAMA 2021, 326, 1–13. [Google Scholar] [CrossRef]
- Zhang, Y.; Moran, A.E. Trends in the Prevalence, Awareness, Treatment, and Control of Hypertension Among Young Adults in the United States, 1999 to 2014. Hypertension 2017, 70, 736–742. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall | Two Diseases | ≥Three Diseases | |||
|---|---|---|---|---|---|---|
| n = 523 | n = 385 | n = 138 | ||||
| Prevalence, % (95% CI) 1 | Estimated Counts, Million | Prevalence, % (95% CI) 1 | Estimated Counts, Million | Prevalence, % (95% CI) 1 | Estimated Counts, Million | |
| Total | 14.4 (12.6 to 16.1) | 34.27 | 10.7 (9.5 to 11.9) | 25.47 | 3.7 (2.8 to 4.6) | 8.80 |
| Age, year | ||||||
| 20–39 2 | 2.3 (1.0 to 3.6) | 5.49 | 1.6 (1.0 to 2.2) | 3.81 | \ | \ |
| 40–59 | 13.5 (9.9 to 17.1) | 32.16 | 10.6 (8.2 to 12.9) | 25.19 | 2.9 (1.1 to 4.7) | 6.97 |
| 60–79 | 34.8 (29.0 to 40.6) | 83.14 | 25.5 (20.2 to 30.8) | 60.94 | 9.3 (6.5 to 12.1) | 22.20 |
| ≥80 | 42.9 (34.5 to 51.2) | 102.33 | 29.8 (23.9 to 35.6) | 71.10 | 13.1 (8.1 to 18.1) | 31.23 |
| Gender | ||||||
| Male | 15.6 (13.3 to 17.8) | 37.23 | 11.1 (9.4 to 12.9) | 26.56 | 4.5 (3.1 to 5.8) | 10.68 |
| Female | 13.4 (11.0 to 15.7) | 31.91 | 10.3 (8.3 to 12.3) | 24.64 | 3.0 (2.0 to 4.1) | 7.27 |
| Race/ethnicity | ||||||
| White | 13.4 (11.1 to 15.6) | 31.90 | 9.9 (8.2 to 11.6) | 23.60 | 3.5 (2.6 to 4.4) | 8.31 |
| Black | 21.0 (17.4 to 24.5) | 50.04 | 16.1 (13.6 to 18.7) | 38.51 | 4.8 (3.6 to 6.1) | 11.54 |
| Hispanic | 13.4 (9.5 to 17.4) | 32.01 | 9.3 (7.2 to 11.5) | 22.32 | 4.1 (1.3 to 6.8) | 9.69 |
| Other 3 | 15.5 (12.5 to 18.6) | 37.02 | 11.7 (9.2 to 14.2) | 27.90 | 3.8 (2.0 to 5.7) | 9.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, X.; Ma, T.; Ouyang, F.; Zhang, G.; Bai, Y. Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999–2018. Int. J. Environ. Res. Public Health 2022, 19, 4726. https://doi.org/10.3390/ijerph19084726
Cheng X, Ma T, Ouyang F, Zhang G, Bai Y. Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999–2018. International Journal of Environmental Research and Public Health. 2022; 19(8):4726. https://doi.org/10.3390/ijerph19084726
Chicago/Turabian StyleCheng, Xunjie, Tianqi Ma, Feiyun Ouyang, Guogang Zhang, and Yongping Bai. 2022. "Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999–2018" International Journal of Environmental Research and Public Health 19, no. 8: 4726. https://doi.org/10.3390/ijerph19084726
APA StyleCheng, X., Ma, T., Ouyang, F., Zhang, G., & Bai, Y. (2022). Trends in the Prevalence of Cardiometabolic Multimorbidity in the United States, 1999–2018. International Journal of Environmental Research and Public Health, 19(8), 4726. https://doi.org/10.3390/ijerph19084726