
Exploring Blue Spaces’ Effects on Childhood Leukaemia Incidence: A Population-Based Case–Control Study in Spain

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Blue-Space Selection and Exposure Measurement
2.3. Covariates
2.3.1. Sociodemographic Covariates
2.3.2. Environmental Covariates
2.4. Statistical Analysis
2.5. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2019. [Google Scholar]
- Laybourn-Langton, L.; Quilter-Pinner, H. London Global Green City; Institute for Public Policy Research: London, UK, 2016. [Google Scholar]
- City of Vancouver. Greenest City Vancouver Action Plan 2020; City of Vancouver: Vancouver, BC, Canada, 2015. [Google Scholar]
- Solomon, S. Water: The Epic Struggle for Wealth, Power, and Civilization; Harper Perennial: New York, NY, USA, 2011. [Google Scholar]
- Pearson, A.L.; Bottomley, R.; Chambers, T.; Thornton, L.; Stanley, J.; Smith, M.; Barr, M.; Signal, L. Measuring Blue Space Visibility and ‘Blue Recreation’ in the Everyday Lives of Children in a Capital City. Int. J. Environ. Res. Public Health 2017, 14, 563. [Google Scholar] [CrossRef]
- Grellier, J.; White, M.P.; Albin, M.; Bell, S.; Elliott, L.; Gascon, M.; Gualdi, S.; Mancini, L.; Nieuwenhuijsen, M.; Sarigiannis, D.; et al. BlueHealth: A study programme protocol for mapping and quantifying the potential benefits to public health and well-being from Europe’s blue spaces. BMJ Open 2017, 7, e016188. [Google Scholar] [CrossRef] [Green Version]
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef]
- Keniger, L.E.; Gaston, K.J.; Irvine, K.N.; Fuller, R.A. What are the Benefits of Interacting with Nature? Int. J. Environ. Res. Public Health 2013, 10, 913–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Huynh, Q.; Craig, W.; Janssen, I.; Pickett, W. Exposure to public natural space as a protective factor for emotional well-being among young people in Canada. BMC Public Health 2013, 13, 407. [Google Scholar] [CrossRef] [Green Version]
- Wood, S.L.; Demougin, P.R.; Higgins, S.; Husk, K.; Wheeler, B.W.; White, M. Exploring the relationship between childhood obesity and proximity to the coast: A rural/urban perspective. Health Place 2016, 40, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental Health Benefits of Long-Term Exposure to Residential Green and Blue Spaces: A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [Green Version]
- Hopp, M.J.; Foley, J.A. Global-Scale Relationships between Climate and the Dengue Fever Vector, Aedes Aegypti. Clim. Chang. 2001, 48, 441–463. [Google Scholar] [CrossRef]
- Rosso, S.; Zanetti, R.; Martinez, C.; Tormo, M.J.; Schraub, S.; Sancho-Garnier, H.; Franceschi, S.; Gafà, L.; Perea, E.; Navarro, C.; et al. The multicentre south European study ‘Helios’. II: Different sun exposure patterns in the aetiology of basal cell and squamous cell carcinomas of the skin. Br. J. Cancer 1996, 73, 1447–1454. [Google Scholar] [CrossRef] [Green Version]
- Peris-Bonet, R.; Salmerón, D.; Martínez-Beneito, M.A.; Galceran, J.; Marcos-Gragera, R.; Felipe, S.; González, V.; Codina, J.S.D.T. Childhood cancer incidence and survival in Spain. Ann. Oncol. 2010, 21, iii103–iii110. [Google Scholar] [CrossRef] [PubMed]
- Ahlbom, A.; Day, N.; Feychting, M.; Roman, E.; Skinner, J.; Dockerty, J.; Linet, M.; McBride, M.; Michaelis, J.; Olsen, J.H.; et al. A pooled analysis of magnetic fields and childhood leukaemia. Br. J. Cancer 2000, 83, 692–698. [Google Scholar] [CrossRef] [Green Version]
- Tong, J.; Qin, L.; Cao, Y.; Li, J.; Zhang, J.; Nie, J.; An, Y. Environmental Radon Exposure and Childhood Leukemia. J. Toxicol. Environ. Health Part B 2012, 15, 332–347. [Google Scholar] [CrossRef] [PubMed]
- Tamayo-Uria, I.; Boldo, E.; García-Pérez, J.; Gómez-Barroso, D.; Romaguera, E.P.; Cirach, M.; Ramis, R. Childhood leukaemia risk and residential proximity to busy roads. Environ. Int. 2018, 121, 332–339. [Google Scholar] [CrossRef]
- Filippini, T.; Heck, J.; Malagoli, C.; Del Giovane, C.; Vinceti, M. A Review and Meta-Analysis of Outdoor Air Pollution and Risk of Childhood Leukemia. J. Environ. Sci. Health Part C 2015, 33, 36–66. [Google Scholar] [CrossRef]
- García-Pérez, J.; López-Abente, G.; Gómez-Barroso, D.; Morales-Piga, A.; Romaguera, E.P.; Tamayo, I.; Fernández-Navarro, P.; Ramis, R. Childhood leukemia and residential proximity to industrial and urban sites. Environ. Res. 2015, 140, 542–553. [Google Scholar] [CrossRef]
- Sánchez, C.O.; Segú-Tell, J.; Gomez-Barroso, D.; Romaguera, E.P.; Ortega-García, J.; Ramis, R. Urban green spaces and childhood leukemia incidence: A population-based case-control study in Madrid. Environ. Res. 2021, 202, 111723. [Google Scholar] [CrossRef] [PubMed]
- Pardo Romaguera, E.; Muñoz López, A.; Valero Poveda, S.; Porta Cebolla, S.; Fernández-Delgado, R.; Barreda Reines, M.S.; Peris Bonet, R. Cáncer Infantil en España. Estadísticas 1980–2017. Registro Español de Tumores Infantiles (RETI-SEHOP) 2018. Available online: https://www.uv.es/rnti/pdfs/Informe_RETI-SEHOP_1980-2017.pdf (accessed on 6 November 2021).
- Centro Nacional de Información Geográfica (CNIG). Available online: http://centrodedescargas.cnig.es (accessed on 1 October 2021).
- Instituto Nacional de Estadística (INE). Available online: https://www.ine.es/ (accessed on 12 January 2022).
- Eurostat. Degree of Urbanisation Classification—2011 Revision 2011. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Degree_of_urbanisation_classification_-_2011_revision (accessed on 5 July 2021).
- Población Residente Por Provincias Según Tipo de Hogar y Densidad de Población. INE n.d. Available online: https://www.ine.es/jaxi/Datos.htm?path=/t20/p274/serie/def/p06/&file=05010.px (accessed on 20 January 2022).
- Interpolated Air Quality Data—European Environment Agency n.d. Available online: https://www.eea.europa.eu/data-and-maps/data/interpolated-air-quality-data-2 (accessed on 11 July 2021).
- Dzhambov, A.M.; Browning, M.H.; Markevych, I.; Hartig, T.; Lercher, P. Analytical approaches to testing pathways linking greenspace to health: A scoping review of the empirical literature. Environ. Res. 2020, 186, 109613. [Google Scholar] [CrossRef]
- Yengoh, G.T.; Dent, D.; Olsson, L.; Tengberg, A.E.; Tucker, C.J. The Use of the Normalized Difference Vegetation Index (NDVI) to Assess Land Degradation at Multiple Scales: A Review of the Current Status, Future Trends, and practical Considerations; Springer: Berlin/Heidelberg, Germany, 2014; p. 80. [Google Scholar]
- Earth Observing System Data and Information System (EOSDIS). Available online: https://earthdata.nasa.gov/learn/discipline/land/ (accessed on 4 July 2021).
- Hunter, P.R. Climate change and waterborne and vector-borne disease. J. Appl. Microbiol. 2003, 94, 37–46. [Google Scholar] [CrossRef]
- Ali, M.; Lopez, A.L.; You, Y.A.; Kim, Y.E.; Sah, B.; Maskery, B.; Clemens, J. The global burden of cholera. Bull. World Health Organ. 2012, 90, 209–218. [Google Scholar] [CrossRef]
- Moehrle, M. Outdoor sports and skin cancer. Clin. Dermatol. 2008, 26, 12–15. [Google Scholar] [CrossRef]
- Dong, Y.; Liu, Y.; Chen, J. Will urban expansion lead to an increase in future water pollution loads?—A preliminary investigation of the Haihe River Basin in northeastern China. Environ. Sci. Pollut. Res. 2014, 21, 7024–7034. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Stegeman, J.J.; Fleming, L.E.; Allemand, D.; Anderson, D.M.; Backer, L.C.; Brucker-Davis, F.; Chevalier, N.; Corra, L.; Czerucka, D.; et al. Human Health and Ocean Pollution. Ann. Glob. Health 2020, 86, 151. [Google Scholar] [CrossRef]
- Lipiatou, E.; Tolosa, I.; Simó, R.; Bouloubassi, I.; Dachs, J.; Marti, S.; Sicre, M.-A.; Bayona, J.; Grimalt, J.; Saliott, A.; et al. Mass budget and dynamics of polycyclic aromatic hydrocarbons in the Mediterranean Sea. Deep Sea Res. Part II Top. Stud. Oceanogr. 1997, 44, 881–905. [Google Scholar] [CrossRef]
- Carratalá, A.; Moreno-González, R.; León, V. Occurrence and seasonal distribution of polycyclic aromatic hydrocarbons and legacy and current-use pesticides in air from a Mediterranean coastal lagoon (Mar Menor, SE Spain). Chemosphere 2017, 167, 382–395. [Google Scholar] [CrossRef]
- Castro-Jiménez, J.; Berrojalbiz, N.; Wollgast, J.; Dachs, J. Polycyclic aromatic hydrocarbons (PAHs) in the Mediterranean Sea: Atmospheric occurrence, deposition and decoupling with settling fluxes in the water column. Environ. Pollut. 2012, 166, 40–47. [Google Scholar] [CrossRef] [Green Version]
- White, M.P.; Alcock, I.; Wheeler, B.; Depledge, M.H. Coastal proximity, health and well-being: Results from a longitudinal panel survey. Health Place 2013, 23, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Edwards, N.J.; Giles-Corti, B.; Larson, A.; Beesley, B. The Effect of Proximity on Park and Beach Use and Physical Activity Among Rural Adolescents. J. Phys. Act. Health 2014, 11, 977–984. [Google Scholar] [CrossRef]
- de Vries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural Environments—Healthy Environments? An Exploratory Analysis of the Relationship between Greenspace and Health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef] [Green Version]
- Triguero-Mas, M.; Dadvand, P.; Cirach, M.; Martínez, D.; Medina, A.; Mompart, A.; Basagaña, X.; Gražulevičiene, R.; Nieuwenhuijsen, M.J. Natural outdoor environments and mental and physical health: Relationships and mechanisms. Environ. Int. 2015, 77, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Barroso, D.; García-Pérez, J.; López-Abente, G.; Tamayo-Uria, I.; Morales-Piga, A.; Romaguera, E.P.; Ramis, R. Agricultural crop exposure and risk of childhood cancer: New findings from a case–control study in Spain. Int. J. Health Geogr. 2016, 15, 18. [Google Scholar] [CrossRef] [Green Version]
- CLC 2018—Copernicus Land Monitoring Service n.d. Available online: https://land.copernicus.eu/pan-european/corine-land-cover/clc2018 (accessed on 12 June 2019).
- Wheeler, B.W.; White, M.; Stahl-Timmins, W.; Depledge, M.H. Does living by the coast improve health and wellbeing? Health Place 2012, 18, 1198–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Infante-Rivard, C.; Weichenthal, S. Pesticides and Childhood Cancer: An Update of Zahm and Ward’s 1998 Review. J. Toxicol. Environ. Health Part B 2007, 10, 81–99. [Google Scholar] [CrossRef] [PubMed]
- Malagoli, C.; Malavolti, M.; Costanzini, S.; Fabbi, S.; Teggi, S.; Palazzi, G.; Arcolin, E.; Vinceti, M. Increased incidence of childhood leukemia in urban areas: A population-based case-control study. Epidemiol. Prev. 2015, 34, 102–107. [Google Scholar]
- Whitehead, T.P.; Metayer, C.; Wiemels, J.L.; Singer, A.W.; Miller, M.D. Childhood Leukemia and Primary Prevention. Curr. Probl. Pediatr. Adolesc. Health Care 2016, 46, 317–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehm, R.D.; Spector, L.G.; Poynter, J.N.; Vock, D.M.; Osypuk, T.L. Socioeconomic Status and Childhood Cancer Incidence: A Population-Based Multilevel Analysis. Am. J. Epidemiol. 2017, 187, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; de Nazelle, A.; Triguero-Mas, M.; Schembari, A.; Cirach, M.; Amoly, E.; Figueras, F.; Basagaña, X.; Ostro, B.; Nieuwenhuijsen, M. Surrounding Greenness and Exposure to Air Pollution During Pregnancy: An Analysis of Personal Monitoring Data. Environ. Health Perspect. 2012, 120, 1286–1290. [Google Scholar] [CrossRef] [PubMed]
- Demoury, C.; Thierry, B.; Richard, H.; Sigler, B.; Kestens, Y.; Parent, M.-E. Residential greenness and risk of prostate cancer: A case-control study in Montreal, Canada. Environ. Int. 2017, 98, 129–136. [Google Scholar] [CrossRef]
- James, P.; Hart, J.E.; Banay, R.F.; Laden, F. Exposure to Greenness and Mortality in a Nationwide Prospective Cohort Study of Women. Environ. Health Perspect. 2016, 124, 1344–1352. [Google Scholar] [CrossRef] [Green Version]
- Interprovincial Migration Balance by Semester, Province, Sex, Age Group and Nationality. INE. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=24450&L=1 (accessed on 21 January 2022).
- Filippini, T.; Hatch, E.E.; Rothman, K.J.; Heck, J.; Park, A.S.; Crippa, A.; Orsini, N.; Vinceti, M. Association between Outdoor Air Pollution and Childhood Leukemia: A Systematic Review and Dose–Response Meta-Analysis. Environ. Health Perspect. 2019, 127, 046002. [Google Scholar] [CrossRef]
- Villanueva, F.; Notario, A.; Adame, J.A.; Millán, M.C.; Mabilia, R.; Albaladejo, J. A preliminary study on ambient levels of carbonyls, benzene, toluene and xylene in the south-west of the Iberian Peninsula (Huelva coast), Spain. Environ. Technol. 2013, 34, 289–299. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Controls (n = 5616) | Cases (n = 936) | Same Address (n = 515) | p Value a | Cases < 3 Years (n = 410) | p Value a |
|---|---|---|---|---|---|---|
| Sex, n (%) | ||||||
| Boy | 3126 (55.7%) | 521 (55.7%) | 283 (55%) | 224 (54.6%) | ||
| Girl | 2490 (44.3%) | 415 (44.3%) | 232 (45%) | 0.794 # | 186 (45.4%) | 0.122 # |
| Age at diagnosis, mean (SD) | x | 4.9 (0.12) | 5.0 (3.6) | 0.625 * | 2.0 (1) | x |
| Activity Rate, mean (SD) | 76.3 (4.8) | 76 (0.15) | 75.8 (4.7) | 0.535 * | 75.9 (4.5) | 0.790 * |
| SES, mean (SD) | 1.06 (0.13) | 1.05 (0.12) | 1.05 (0.12) | 0.605 * | 1.04 (0.12) | 0.7264 * |
| Histologic subtype, n (%) | ||||||
| ALL | x | 758 (81.0%) | 421 (81.8%) | 305 (74.4%) | ||
| AML | x | 144 (15.4%) | 78 (15.1%) | 84 (20.5%) | ||
| CML | x | 7 (0.7%) | 4 (0.8%) | 2 (0.5%) | ||
| Other specific leukaemia | x | 17 (1.8%) | 7 (1.4%) | 13 (3.2%) | ||
| Non-specific leukaemia | x | 10 (1.1%) | 5 (0.9%) | 0.974 # | 6 (1.4%) | 0.062 # |
| BSs within 250 m buffer, n (%) | ||||||
| Yes | 708 (12.6%) | 102 (10.9%) | 55 (10.7%) | 46 (11.2%) | ||
| No | 4908 (87.4%) | 834 (89.1%) | 460 (89.3%) | 0.898 # | 364 (87.8%) | 0.032 # |
| BSs within 500 m buffer, n (%) | ||||||
| Yes | 1630 (29%) | 240 (25.6%) | 135 (26.2%) | 99 (24.2%) | ||
| No | 3986 (71%) | 696 (74.4%) | 380 (73.8%) | 0.812 # | 311 (75.8%) | 0.340 # |
| BSs within 750 m buffer, n (%) | ||||||
| Yes | 2353 (41.9%) | 354 (37.8%) | 205 (39.8%) | 151 (36.8%) | ||
| No | 3363 (58.1%) | 582 (62.2%) | 310 (60.2%) | 0.457 # | 259 (63.2%) | 0.119 # |
| BSs within 1000 m buffer, n (%) | ||||||
| Yes | 2934 (52.2%) | 455 (48.6%) | 264 (51.3%) | 196 (52.2%) | ||
| No | 2682 (47.8%) | 481 (51.4%) | 251 (48.7%) | 0.334 # | 214 (47.8%) | 0.074 # |
| DGUR, n (%) | ||||||
| Densely populated area | 5042 (89.8%) | 867 (92.6%) | 476 (92.4%) | 378 (92.2%) | ||
| Non-densely populated areas | 574 (10.2%) | 69 (7.4%) | 39 (7.6%) | 0.889 # | 32 (7.8%) | 0.781 # |
| PM10 levels at residence, mean (SD) | 26.02 (0.07) | 26.2 (5.41) | 25.9 (5.32) | 0.314 * | 25.0 (5.29) | <0.01 * |
| Surrounding greenness (NDVI), median (IQR) | ||||||
| in 250 m buffer | −0.06 (0.10) | −0.07 (0.11) | −0.06 (0.11) | 0.904 ¥ | −0.05 (0.15) | 0.012 ¥ |
| in 500 m buffer | −0.04 (0.11) | −0.05 (0.13) | −0.05 (0.13) | 0.948 ¥ | −0.03 (0.16) | 0.014 ¥ |
| in 750 m buffer | −0.03 (0.12) | −0.03 (0.14) | −0.03 (0.14) | 0.898 ¥ | −0.02 (0.16) | 0.013 ¥ |
| in 1000 m buffer | −0.02 (0.13) | −0.03 (0.14) | −0.03 (0.15) | 0.851 ¥ | −0.01 (0.17) | 0.016 ¥ |
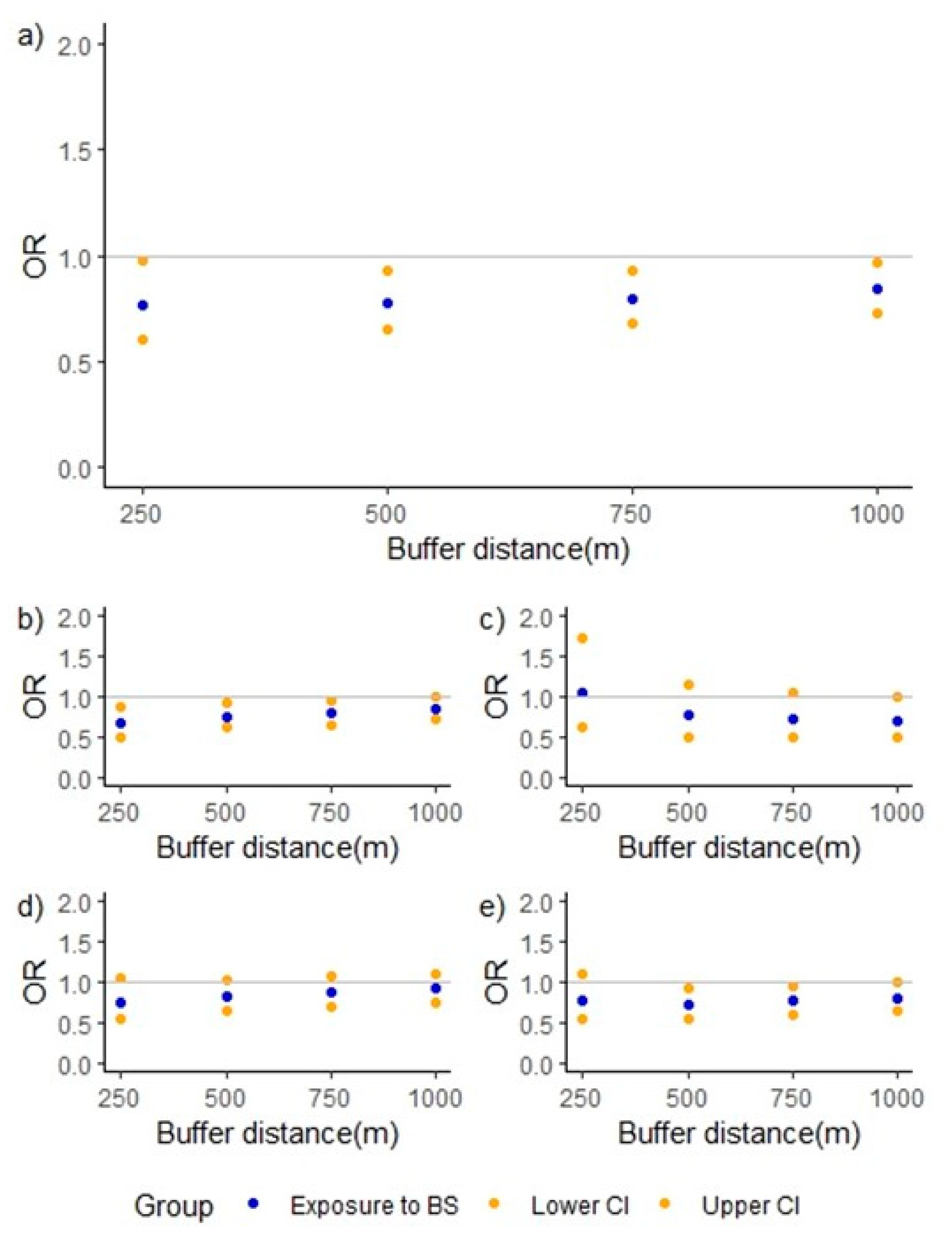
| Analysis Group | Exposure Category | Controls (n) | Cases (n) | Adjusted OR (95%CI) a | p Value |
|---|---|---|---|---|---|
| Childhood Leukaemia | |||||
| Reference | 2682 | 481 | - | ||
| 250 m | 708 | 102 | 0.77 (0.60–0.97) | 0.031 | |
| 500 m | 1630 | 240 | 0.78 (0.65–0.93) | 0.006 | |
| 750 m | 2353 | 354 | 0.80 (0.68–0.93) | 0.005 | |
| 1000 m | 2934 | 455 | 0.84 (0.72–0.97) | 0.019 | |
| ALL subtype | |||||
| Reference | 2682 | 388 | - | ||
| 250 m | 708 | 73 | 0.68 (0.51–0.89) | 0.006 | |
| 500 m | 1630 | 188 | 0.75 (0.62–0.91) | 0.004 | |
| 750 m | 2353 | 283 | 0.79 (0.67–0.94) | 0.008 | |
| 1000 m | 2934 | 370 | 0.85 (0.72–1.00) | 0.049 | |
| AML subtype | |||||
| Reference | 2682 | 78 | - | ||
| 250 m | 708 | 23 | 1.06 (0.63–1.71) | 0.818 | |
| 500 m | 1630 | 39 | 0.77 (0.50–1.15) | 0.210 | |
| 750 m | 2353 | 55 | 0.72 (0.50–1.04) | 0.084 | |
| 1000 m | 2934 | 66 | 0.70 (0.49–0.99) | 0.045 | |
| Same address | |||||
| Reference | 2682 | 251 | - | ||
| 250 m | 708 | 55 | 0.77 (0.56–1.04) | 0.100 | |
| 500 m | 1630 | 135 | 0.82 (0.65–1.03) | 0.097 | |
| 750 m | 2353 | 205 | 0.87 (0.71–1.07) | 0.198 | |
| 1000 m | 2934 | 264 | 0.92 (0.76–1.12) | 0.407 | |
| Cases < 3 years | |||||
| Reference | 2682 | 214 | - | ||
| 250 m | 708 | 46 | 0.79 (0.55–1.10) | 0.172 | |
| 500 m | 1630 | 99 | 0.73 (0.56–0.94) | 0.017 | |
| 750 m | 2353 | 151 | 0.77 (0.61–0.97) | 0.025 | |
| 1000 m | 2934 | 196 | 0.81 (0.66–1.01) | 0.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojeda Sánchez, C.; García-Pérez, J.; Gómez-Barroso, D.; Domínguez-Castillo, A.; Pardo Romaguera, E.; Cañete, A.; Ortega-García, J.A.; Ramis, R. Exploring Blue Spaces’ Effects on Childhood Leukaemia Incidence: A Population-Based Case–Control Study in Spain. Int. J. Environ. Res. Public Health 2022, 19, 5232. https://doi.org/10.3390/ijerph19095232
Ojeda Sánchez C, García-Pérez J, Gómez-Barroso D, Domínguez-Castillo A, Pardo Romaguera E, Cañete A, Ortega-García JA, Ramis R. Exploring Blue Spaces’ Effects on Childhood Leukaemia Incidence: A Population-Based Case–Control Study in Spain. International Journal of Environmental Research and Public Health. 2022; 19(9):5232. https://doi.org/10.3390/ijerph19095232
Chicago/Turabian StyleOjeda Sánchez, Carlos, Javier García-Pérez, Diana Gómez-Barroso, Alejandro Domínguez-Castillo, Elena Pardo Romaguera, Adela Cañete, Juan A. Ortega-García, and Rebeca Ramis. 2022. "Exploring Blue Spaces’ Effects on Childhood Leukaemia Incidence: A Population-Based Case–Control Study in Spain" International Journal of Environmental Research and Public Health 19, no. 9: 5232. https://doi.org/10.3390/ijerph19095232
APA StyleOjeda Sánchez, C., García-Pérez, J., Gómez-Barroso, D., Domínguez-Castillo, A., Pardo Romaguera, E., Cañete, A., Ortega-García, J. A., & Ramis, R. (2022). Exploring Blue Spaces’ Effects on Childhood Leukaemia Incidence: A Population-Based Case–Control Study in Spain. International Journal of Environmental Research and Public Health, 19(9), 5232. https://doi.org/10.3390/ijerph19095232