
Implementation Challenges and Recommendations for Employing Peer Support Workers in Emergency Departments to Support Patients Presenting after an Opioid-Related Overdose

 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of Study Subjects
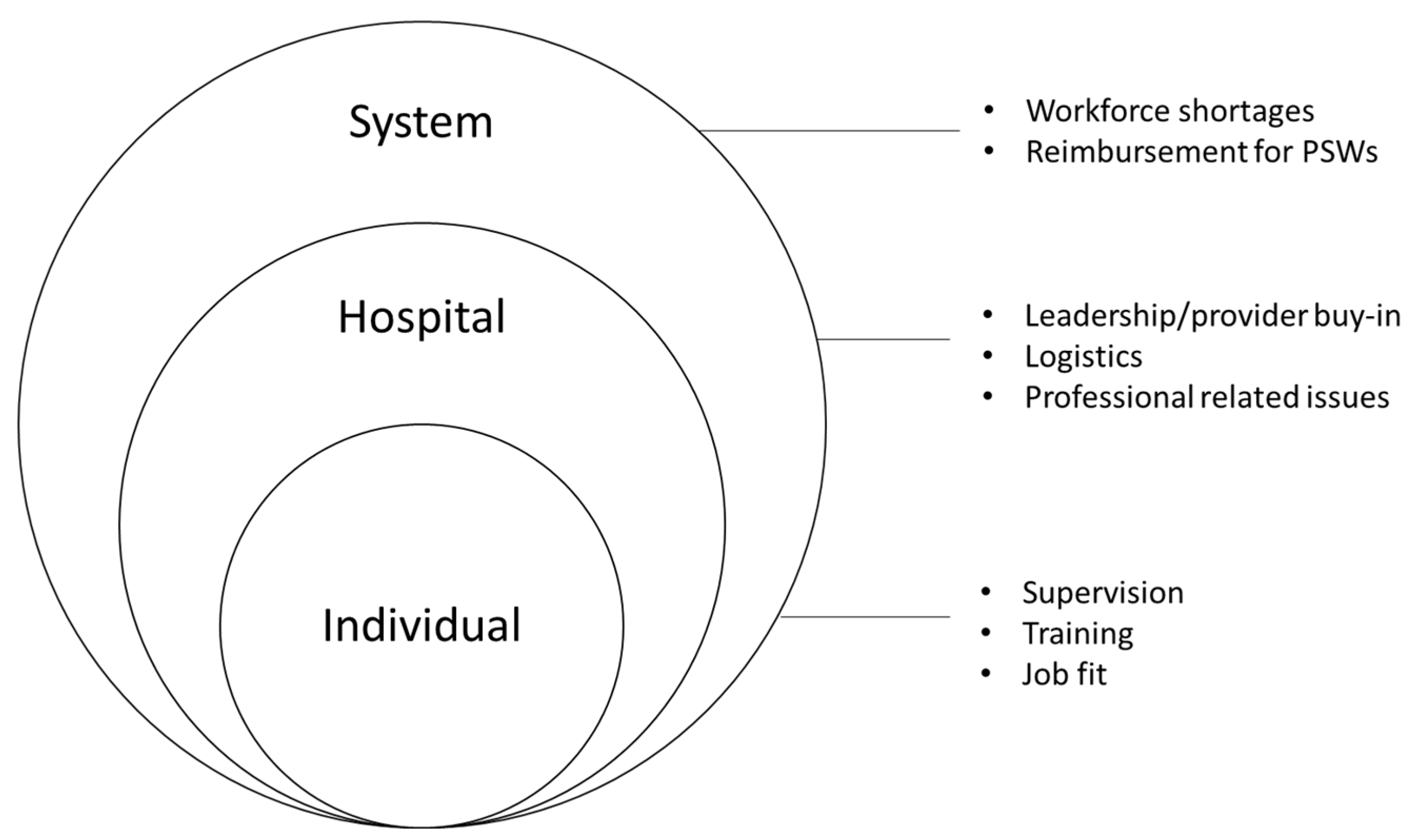
3.2. Identified Themes
4. Discussion
4.1. System Level
4.2. Hospital Level
4.3. Individual Level
5. Conclusions and Implications for Clinical Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2018 National Survey on Drug Use and Health; NSDUH Series H-54; HHS Publication No. PEP19-5068; Center for Behavioral Health Statistics and Quality: Rockville, MD, USA, 2019.
- CDC/NCHS, National Vital Statistics System, Mortality. CDC Wonder; US Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019. Available online: https://wonder.cdc.gov (accessed on 24 February 2022).
- CDC. Centers for Disease Control and Prevention, Drug Overdose Deaths. Drug Overdose Deaths Remain High. 2021. Available online: https://www.cdc.gov/drugoverdose/deaths/index.html (accessed on 4 April 2022).
- CDC. Centers for Disease Control and Prevention, Overdose Deaths Accelerating during COVID-19, Expanded Prevention Efforts Needed. Press Release 17 December 2020. 2020. Available online: https://www.cdc.gov/media/releases/2020/p1218-overdose-deaths-covid-19.html (accessed on 4 April 2022).
- CDC. Centers for Disease Control and Prevention, Emergency Preparedness and Response, Increase in Fatal Drug Overdoses Across the United States Driven by Synthetic Opioids before and during the COVID-19 Pandemic. Distributed via the CDC Health Alert Network December 17, 2020, 8:00 AM ET CDCHAN-0043. 2021. Available online: https://emergency.cdc.gov/han/2020/han00438.asp (accessed on 4 April 2022).
- Vivolo-Kantor, A.M.; Seth, P.; Gladden, M.; Mattson, C.L.; Baldwin, G.T.; Kite-Powell, A.; Coletta, M.A. Vital Signs: Trends in Emergency Department Visits for Suspected Opioid Overdoses—United States, July 2016–September 2017. US Department of Health and Human Services, Centers for Disease Control and Prevention. Morb. Mortal. Wkly. Rep. 2018, 67, 279–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, E.; Gordon, M.; Friedmann, P.D.; Fishman, M.J.; Lee, J.; Chen, D.T.; Hu, M.C.; Boney, T.Y.; Wilson, D.; O’Brien, C.P. Relapse to opioid use disorder after inpatient treatment: Protective effect of injection naltrexone. J. Subst. Abus. Treat. 2017, 85, 49–55. [Google Scholar] [CrossRef] [PubMed]
- New Mexico Department of Health. New Mexico Substance Use Epidemiology Profile; New Mexico Department of Health: Santa Fe, NM, USA, 2020.
- Houry, D.E.; Haegerich, T.M.; Vivolo-Kantor, A. Opportunities for Prevention and Intervention of Opioid Overdose in the Emergency Department. Ann. Emerg. Med. 2018, 71, 688–690. [Google Scholar] [CrossRef] [Green Version]
- Frank, J.W.; Levy, C.; Calcaterra, S.L.; Hoppe, J.A.; Binswanger, I.A. Naloxone Administration in US Emergency Departments, 2000–2011. J. Med Toxicol. 2015, 12, 148–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lister, J.J.; Weaver, A.; Ellis, J.D.; Himle, J.A.; Ledgerwood, D.M. A systematic review of rural-specific barriers to medication treat-ment for opioid use disorder in the United States. Am. J. Drug Alcohol Abus. 2020, 46, 273–288. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; O’Connor, P.G.; Pantalon, M.V.; Chawarski, M.C.; Busch, S.H.; Owens, P.H.; Bernstein, S.L.; Fiellin, D. Emergency Department–Initiated Buprenorphine/Naloxone Treatment for Opioid Dependence. JAMA 2015, 313, 1636–1644. [Google Scholar] [CrossRef]
- Bassuk, E.L.; Hanson, J.; Greene, R.N.; Richard, M.; Laudet, A. Peer-Delivered Recovery Support Services for Addictions in the United States: A Systematic Review. J. Subst. Abus. Treat. 2016, 63, 1–9. [Google Scholar] [CrossRef]
- Reif, S.; Braude, L.; Lyman, D.R.; Dougherty, R.H.; Daniels, A.S.; Ghose, S.S.; Salim, O.; Delphin-Rittmon, M.E. Peer Recovery Support for Individuals with Substance Use Disorders: Assessing the Evidence. Psychiatr. Serv. 2014, 65, 853–861. [Google Scholar] [CrossRef] [Green Version]
- Eddie, D.; Hoffman, L.; Vilsaint, C.; Abry, A.; Bergman, B.; Hoeppner, B.; Weinstein, C.; Kelly, J.F. Lived Experience in New Models of Care for Substance Use Disorder: A Systematic Review of Peer Recovery Support Services and Recovery Coaching. Front. Psychol. 2019, 10, 1052. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.; Rosenberg, L. Peer Support Workers in Emergency Departments: Engaging Individuals Surviving Opioid Overdoses—A Qualitative Assessment; National Council for Behavioral Health: Washington, DC, USA, 2019.
- Watson, D.P.; Weathers, T.; McGuire, A.; Cohen, A.; Huynh, P.; Bowes, C.; O’Donnell, D.; Brucker, K.; Gupta, S. Evaluation of an emergency department-based opioid overdose survivor intervention: Difference-in-difference analysis of electronic health record data to assess key outcomes. Drug Alcohol Depend. 2021, 221, 108595. [Google Scholar] [CrossRef]
- Wagner, K.D.; Oman, R.F.; Smith, K.P.; Harding, R.W.; Dawkins, A.D.; Lu, M.; Woodard, S.; Berry, M.N.; Roget, N.A. “Another tool for the tool box? I’ll take it!”: Feasibility and acceptability of mobile recovery outreach teams (MROT) for opioid overdose patients in the emergency room. J. Subst. Abus. Treat. 2019, 108, 95–103. [Google Scholar] [CrossRef] [Green Version]
- McGuire, A.B.; Powell, K.G.; Treitler, P.C.; Wagner, K.D.; Smith, K.P.; Cooperman, N.; Robinson, L.; Carter, J.; Ray, B.; Watson, D.P. Emer-gency department-based peer support for opioid use disorder: Emergent functions and forms. J. Subst. Abus. Treat. 2020, 108, 82–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, C.; Jones, R.; Yarborough, H.; Kahler, Z.; Moschella, P.; Lommel, K. 366 Peer-to-Peer Addiction Counseling Initiated in the Emergency Department Leads to High Initial Opioid Recovery Rates. Ann. Emerg. Med. 2018, 72, S143–S144. [Google Scholar] [CrossRef]
- Samuels, E.A.; Bernstein, S.L.; Marshall, B.D.; Krieger, M.; Baird, J.; Mello, M.J. Peer navigation and take-home naloxone for opioid overdose emergency department patients: Preliminary patient outcomes. J. Subst. Abus. Treat. 2018, 94, 29–34. [Google Scholar] [CrossRef]
- Waye, K.M.; Goyer, J.; Dettor, D.; Mahoney, L.; Samuels, E.A.; Yedinak, J.; Marshall, B.D. Implementing peer recovery services for overdose prevention in Rhode Island: An examination of two outreach-based approaches. Addict. Behav. 2018, 89, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Samuels, E.A.; Baird, J.; Yang, E.S.; Mello, M.J. Adoption and Utilization of an Emergency Department Naloxone Distribution and Peer Recovery Coach Consultation Program. Acad. Emerg. Med. 2018, 26, 160–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, K.D.; Mittal, M.L.; Harding, R.W.; Smith, K.P.; Dawkins, A.D.; Wei, X.; Woodard, S.; Roget, N.A.; Oman, R.F. “It’s Gonna be a Lifeline”: Findings from Focus Group Research to Investigate What People Who Use Opioids Want from Peer-Based Postoverdose Interventions in the Emergency Department. Ann. Emerg. Med. 2020, 76, 717–727. [Google Scholar] [CrossRef]
- Schneider, A.; Weigl, M. Associations between psychosocial work factors and provider mental well-being in emergency departments: A systematic review. PLoS ONE 2018, 13, e0197375. [Google Scholar] [CrossRef]
- Dir, A.L.; Watson, D.P.; Zhiss, M.; Taylor, L.; Bray, B.C.; McGuire, A. Barriers impacting the POINT pragmatic trial: The unavoidable overlap between research and intervention procedures in “real-world” research. Trials 2021, 22, 1–11. [Google Scholar] [CrossRef]
- Johnston, A.; Abraham, L.; Greenslade, J.; Thom, O.; Carlstrom, E.; Wallis, M.; Crilly, J. Review article: Staff perception of the emergency department working environment: Integrative review of the literature. Emerg. Med. Australas. 2016, 28, 7–26. [Google Scholar] [CrossRef]
- Bragard, I.; Dupuis, G.; Fleet, R. Quality of work life, burnout, and stress in emergency department physicians. Eur. J. Emerg. Med. 2015, 22, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Hunsaker, S.; Chen, H.-C.; Maughan, D.; Heaston, S. Factors That Influence the Development of Compassion Fatigue, Burnout, and Compassion Satisfaction in Emergency Department Nurses. J. Nurs. Scholarsh. 2015, 47, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Public Health Crisis Notice of Funding Opportunity. Available online: https://www.cdc.gov/cpr/readiness/funding-crisis.htm (accessed on 25 October 2019).
- Baral, S.; Logie, C.H.; Grosso, A.; Wirtz, A.L.; Beyrer, C. Modified social ecological model: A tool to guide the assessment of the risks and risk contexts of HIV epidemics. BMC Public Health 2013, 13, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biernacki, P.; Waldorf, D. Snowball Sampling: Problems and Techniques of Chain Referral Sampling. Sociol. Methods Res. 1981, 10, 141–163. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef] [PubMed]
- Jobe, J.B.; Mingay, D.J. Cognitive research improves questionnaires. Am. J. Public Health 1989, 79, 1053–1055. [Google Scholar] [CrossRef] [Green Version]
- Alaimo, K.; Olson, C.M.; Frongillo, E.A. Importance of cognitive testing for survey items: An example from food security ques-tionnaires. J. Nutr. Educ. 1999, 31, 269–275. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Bengtsson, M. How to plan and perform a qualitative study using content analysis. NursingPlus Open 2016, 2, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Staton, M.D.; Watson, D.P.; Thorpe, D. Implementation of peer recovery coach services for opioid overdose patients in emergency departments in Indiana: Findings from an informal learning collaborative of stakeholders. Transl. Behav. Med. 2021, 11, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.O.; Hunter, K.M.; Mabe, A.P.; Tucker, S.J.; Buckley, P.F. The Professional Experiences of Peer Specialists in the Georgia Mental Health Consumer Network. Community Ment. Health J. 2015, 51, 424–436. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, A.; Horton, T.; Ewen, E.; Becher, J.; Wright, P.A.; Silverman, B.; McGraw, P.; Woody, G.E. Early data from project engage: A program to identify and transition medically hospitalized patients into addictions treatment. Addict. Sci. Clin. Pract. 2012, 7, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruhl, K.L.R.; LaCarte, S.; Calixte, S. Authentic peer support work: Challenges and opportunities for an evolving occupation. J. Ment. Health 2015, 25, 78–86. [Google Scholar] [CrossRef]
- Gates, L.B.; Akabas, S.H. Developing Strategies to Integrate Peer Providers into the Staff of Mental Health Agencies. Adm. Ment. Health 2007, 34, 293–306. [Google Scholar] [CrossRef]
- Chinman, M.; Hamilton, A.; Butler, B.; Knight, E.; Murray, S.; Young, A. Mental Health Consumer Providers: A Guide for Clinical Staff; RAND Corporation: Santa Monica, CA, USA, 2008. [Google Scholar]
- Morris, C.W.; Banning, L.B.; Mumby, S.J.; Morris, C.D. Dimensions: Peer Support Program Toolkit; University of Colorado Anschultz Medical Campus, School of Medicine, Behavioral Health and Wellness Program: Aurora, CO, USA, 2015; pp. 1–51. Available online: https://www.bhwellness.org/toolkits/Peer-Support-Program-Toolkit.pdf (accessed on 15 March 2022).
- Daniels, A.S.; Tunner, T.P.; Powell, I.; Fricks, L.; Ashenden, P. Pillars of Peer Support Services Summit Six: Peer Specialist Supervision; Annual Summit: Atlanta, GA, USA, 2014. [Google Scholar]
- Crisanti, A.; Murray-Krezan, C.; Karlin, L.; Sutherland-Bruaw, K.; Najavits, L. Evaluation of an evidence-based practice training for peer support workers in behavioral health care. Cogent Psychol. 2016, 3, 1212453. [Google Scholar] [CrossRef]
- Jacobson, N.; Trojanowski, L.; Dewa, C.S. What do peer support workers do? A job description. BMC Health Serv. Res. 2012, 12, 205. [Google Scholar] [CrossRef] [Green Version]
- Heathfield, S. Assess Job Fit When You Select Your Employees. The Balance Careers. Published July 27, 2019. Available online: https://www.thebalancecareers.com/assess-job-fit-when-you-select-employees-1918165 (accessed on 25 November 2019).
- Tinsley, H.E. The Congruence Myth: An Analysis of the Efficacy of the Person–Environment Fit Model. J. Vocat. Behav. 2000, 56, 147–179. [Google Scholar] [CrossRef]
- Rutakumwa, R.; Mugisha, J.O.; Bernays, S.; Kabunga, E.; Tumwekwase, G.; Mbonye, M.; Seeley, J. Conducting in-depth interviews with and without voice recorders: A comparative analysis. Qual. Res. 2019, 20, 565–581. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Respondent Role | Hospital Had PSW? | Data Collection | Format | Mode |
|---|---|---|---|---|
| Yes | 1–1 interview | Phone | Recorded |
| Yes | Paired interview | Phone | Recorded |
| Yes | |||
| No | Focus group | In-person | Recorded |
| No | |||
| No | |||
| No | |||
| No | |||
| Yes | 1–1 Interview | Phone | Recorded |
| Yes | 1–1 Interview | Phone | Recorded |
| No (rural) * | 1–1 Interview | Phone | Recorded |
| No | 1–1 Interview | Phone | Recorded |
| Yes | 1–1 Interview | Phone | Recorded |
| N/A + | 1–1 Interview | Phone | Recorded |
| N/A + | 1–1 Interview | Phone | Notes |
| N/A + | 1–1 Interview | Phone | Notes |
| N/A + | Paired interview | Phone | Recorded |
| N/A + | Recorded | ||
| Yes | 1–1 Interview | In-person | Recorded |
| Summary of Data Collection Details | ||||
| Manager/directors (8) | Hospitals w/PSW (7) | 1 Focus group (N = 5) | Phone (N = 13) | Recorded (N = 15) |
| Nurses (2) | Hospitals no PSW (7) | 2 paired interviews (N = 4) | In-person (N = 6) | Notes (N = 4) |
| PSWs (3) | Participant not from | 10 1–1 interviews (N = 10) | ||
| Content experts (6) | hospital setting (5) | |||
| System-Level Themes | Respondent Statements |
|---|---|
| PSW workforce shortages |
|
| Reimbursement for peer services |
|
| Hospital-Level Themes | |
| Buy-in from hospital leadership, providers, and staff |
|
| Logistics related to integrating PSWs |
|
| Concerns related to professionalism |
|
| Individual-Level Themes | |
| Need for appropriate supervision |
|
| Need for additional training |
|
| Choosing a peer that is a good fit |
|
| System Level | |
| Workforce |
|
| Reimbursement |
|
| Hospital Level | |
| Buy-in |
|
| Logistics |
|
| Professionalism concerns |
|
| Individual Level | |
| Supervision |
|
| Training |
|
| Good fit |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crisanti, A.S.; Earheart, J.; Deissinger, M.; Lowerre, K.; Salvador, J.G. Implementation Challenges and Recommendations for Employing Peer Support Workers in Emergency Departments to Support Patients Presenting after an Opioid-Related Overdose. Int. J. Environ. Res. Public Health 2022, 19, 5276. https://doi.org/10.3390/ijerph19095276
Crisanti AS, Earheart J, Deissinger M, Lowerre K, Salvador JG. Implementation Challenges and Recommendations for Employing Peer Support Workers in Emergency Departments to Support Patients Presenting after an Opioid-Related Overdose. International Journal of Environmental Research and Public Health. 2022; 19(9):5276. https://doi.org/10.3390/ijerph19095276
Chicago/Turabian StyleCrisanti, Annette S., Jennifer Earheart, Megan Deissinger, Kathryn Lowerre, and Julie G. Salvador. 2022. "Implementation Challenges and Recommendations for Employing Peer Support Workers in Emergency Departments to Support Patients Presenting after an Opioid-Related Overdose" International Journal of Environmental Research and Public Health 19, no. 9: 5276. https://doi.org/10.3390/ijerph19095276
APA StyleCrisanti, A. S., Earheart, J., Deissinger, M., Lowerre, K., & Salvador, J. G. (2022). Implementation Challenges and Recommendations for Employing Peer Support Workers in Emergency Departments to Support Patients Presenting after an Opioid-Related Overdose. International Journal of Environmental Research and Public Health, 19(9), 5276. https://doi.org/10.3390/ijerph19095276