
Insights into Improving Risk and Safety Communication through Environmental Health Literacy


Abstract
:1. Introduction
- Phase 1:
- Eight focus groups
- Conducted to gain an understanding of the water use habits of Tucson residents as well as their thoughts and concerns about water contamination.
- Content analysis of the focus group transcripts using codes developed for this project
- Qualitative analysis of the focus group participants drinking water habits
- Results led to the development of a checklist for materials creation
- Phase 2:
- Pilot test materials created based on the checklist and evaluated
- A common misconception is that turbid or “cloudy” drinking water is contaminated, therefore this topic was chosen to create the pilot test materials
- Multimedia materials included a fact sheet, social media posts, a presentation, and a public service announcement
- These were then evaluated in classroom experiences with public health students
- The results of that materials evaluation lead to the identification of Nine Principles of Risk and Safety Communication
- Phase 3:
- Development of a protocol for message and materials creation
- The protocol was developed to describe the steps needed to create messages and materials that meet the nine principles, which were determined to be the following:
- ○
- Identify the audience(s)
- ○
- Understand the reason or reasons for the communication
- ○
- Use plain language to develop the needed messages–both risk and safety
- ○
- Determine the materials that best suit the audience(s)
- ○
- Evaluate the understandability of the materials
- Phase 4:
- Creation and testing of an online training module
- The purpose of the training module is to teach public health and utility professionals to use the protocol
- The training module was evaluated with a class of master’s level public health students
- The training module is available in Google Classrooms entitled Risk and Safety Classroom https://classroom.google.com/u/0/h (accessed on 18 April 2022).
1.1. Background
1.1.1. Health Literacy
“The results are based on assessment tasks designed specifically to measure the health literacy of adults living in the United States. Health literacy was reported using four performance levels: Below Basic, Basic, Intermediate, and Proficient. The majority of adults (53 percent) had Intermediate health literacy. About 22 percent had Basic and 14 percent had Below Basic health literacy. Relationships between health literacy and background variables (such as educational attainment, age, race/ethnicity, where adults get information about health issues, and health insurance coverage) were also examined and reported. For example, adults with Below Basic or Basic health literacy were less likely than adults with higher health literacy to get information about health issues from written sources (newspapers, magazines, books, brochures, or the Internet) and more likely than adults with higher health literacy to get a lot of information about health issues from radio and television.”[18]
1.1.2. Environmental Health Literacy
“an emerging and evolving concept that bridges shared theories from the fields of risk communication, environmental health science, behavioral science, evaluation, communications, public health, and the social sciences. The process of becoming environmentally health literate entails raising scientific literacy, environmental literacy, and numeracy among the general public while increasing awareness of specific exposures and their potential health effects”.[13]
- (1)
- There is a connection between the environment and health
- (2)
- How environmental agents enter the body
- (3)
- Information about harmful environmental agents
- (4)
- Ways to avoid harmful environmental agents but cannot avoid completely
- (5)
- Research takes a long time
- (6)
- Can identify reliable information about the environment
- (1)
- Find information explaining how to reduce risks in his/her life
- (2)
- Convey his/her concerns about environmental risks to others
- (3)
- Find information about regional/community environmental hazards/issues
- (4)
- Identify well-known/established hazards in his/her environment
- (5)
- Judge whether an information source is reliable
- (6)
- Find information about hazards in his/her microenvironment, home, or workplace
1.1.3. Risk Communication
2. Research Methods
2.1. Research Methods Phase 1: Focus Groups
- What is your confidence level in the safety and quality of tap water?
- On an average day, do you drink tap water, bottled water, or water after additional treatment? (Brita filters, refrigerator, and other filters)
- If only unfiltered tap water is available, will you drink it?
- Can you describe or define what a contaminant is to you?
- If there was a contaminant in your drinking water, would you feel at risk?
- What communication sources are you most likely to hear about a new contaminant?
- Would the way you hear about a new contaminant affect how severe you believe it is?
- What questions would you ask if a new contaminant were to be discovered in the water?
2.1.1. Analysis Coding of Focus Group Transcripts
2.1.2. Focus Group Codes
2.2. Research Methods Phase 2: Checklist Development
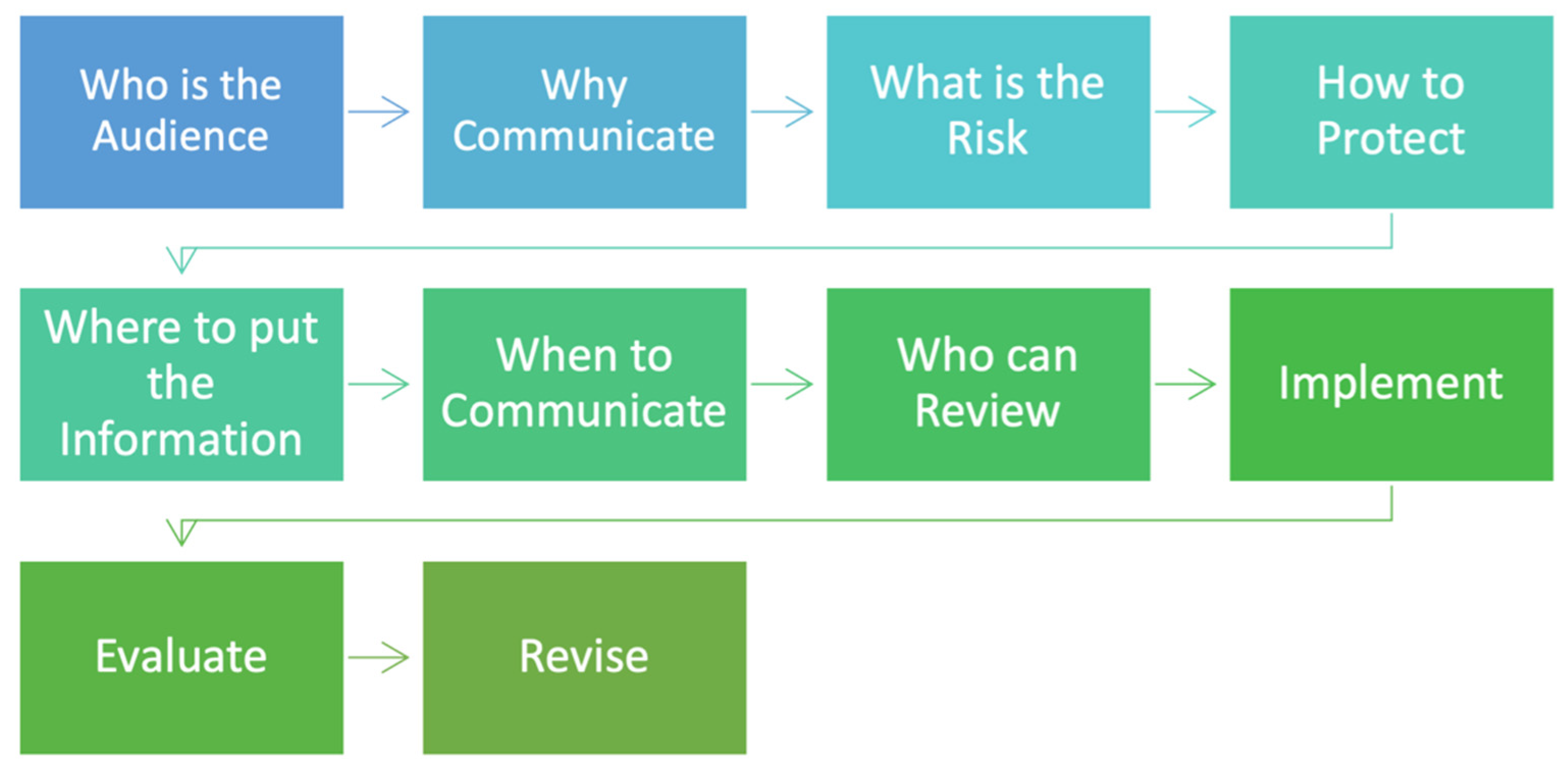
2.3. Research Methods Phase 3: Protocol Development
- Consider the audience.
- Develop the messages about the contaminant.
- ○
- Risk information
- ○
- Information about safety from the contaminant
- Develop materials specific to the audience or audiences.
- Evaluate the materials with members of the intended audience.
- Implement materials in a timely fashion.
- Recommunicate with audiences in long term contamination.
- Evaluate the process.
2.4. Research Method Phase 4: Training Module
- The basics of risk communication
- The relationship between risk perspectives and communication
- How to understand the intended audience of messages and materials
- Use of the Health Literacy Data Map [11]
- The types of materials that will be most suited to each intended audience
- The reasons for the communication, both immediate and long-term
- The five basic questions to answer in the messages and materials
- How a person can protect themselves, their family, and their community
- How to evaluate the materials that are developed with the intended audience
3. Results
3.1. Results Phase 1: Focus Group Results
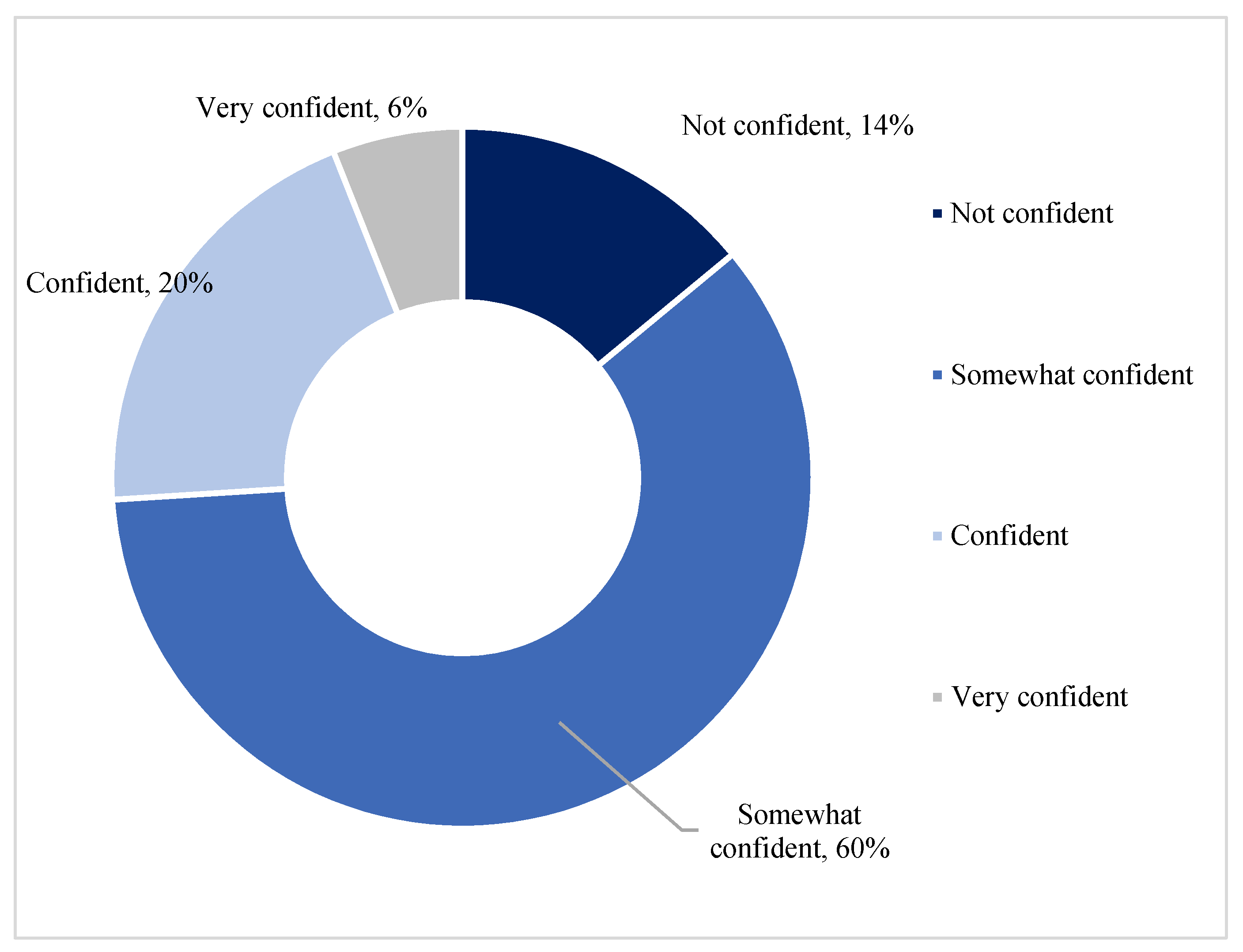
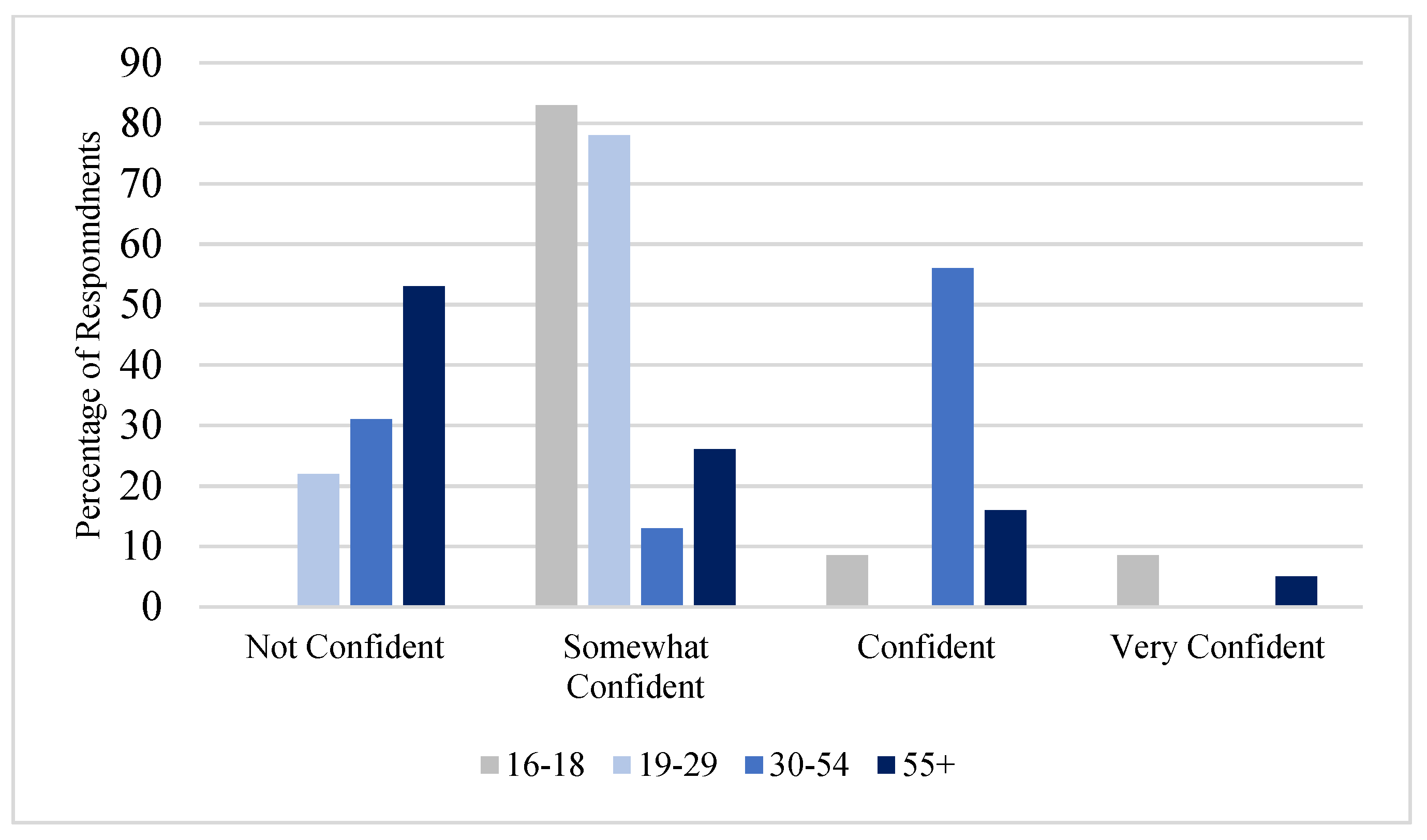
3.1.1. Summary of Participants Response to Fictitious Contaminant Exercise
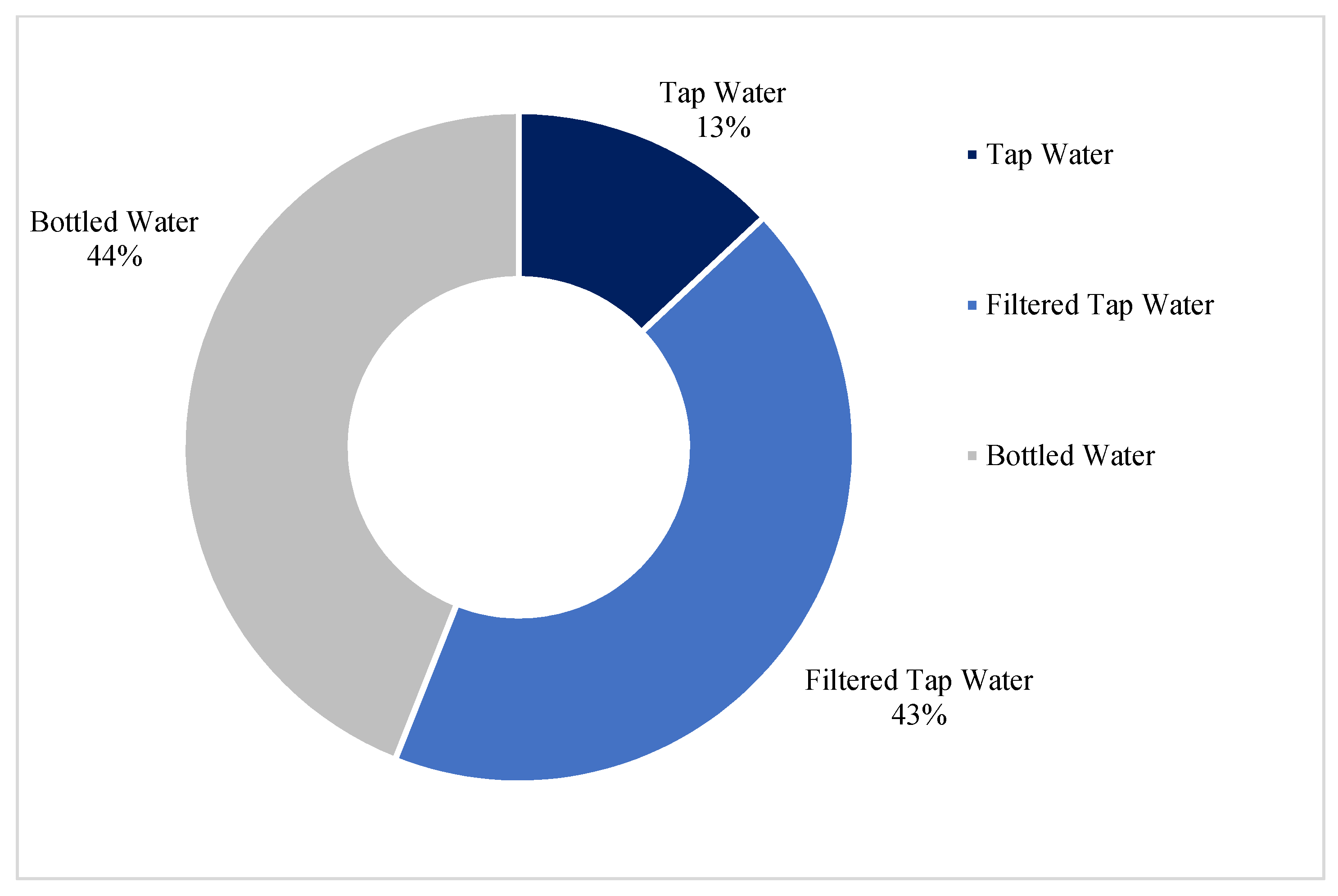
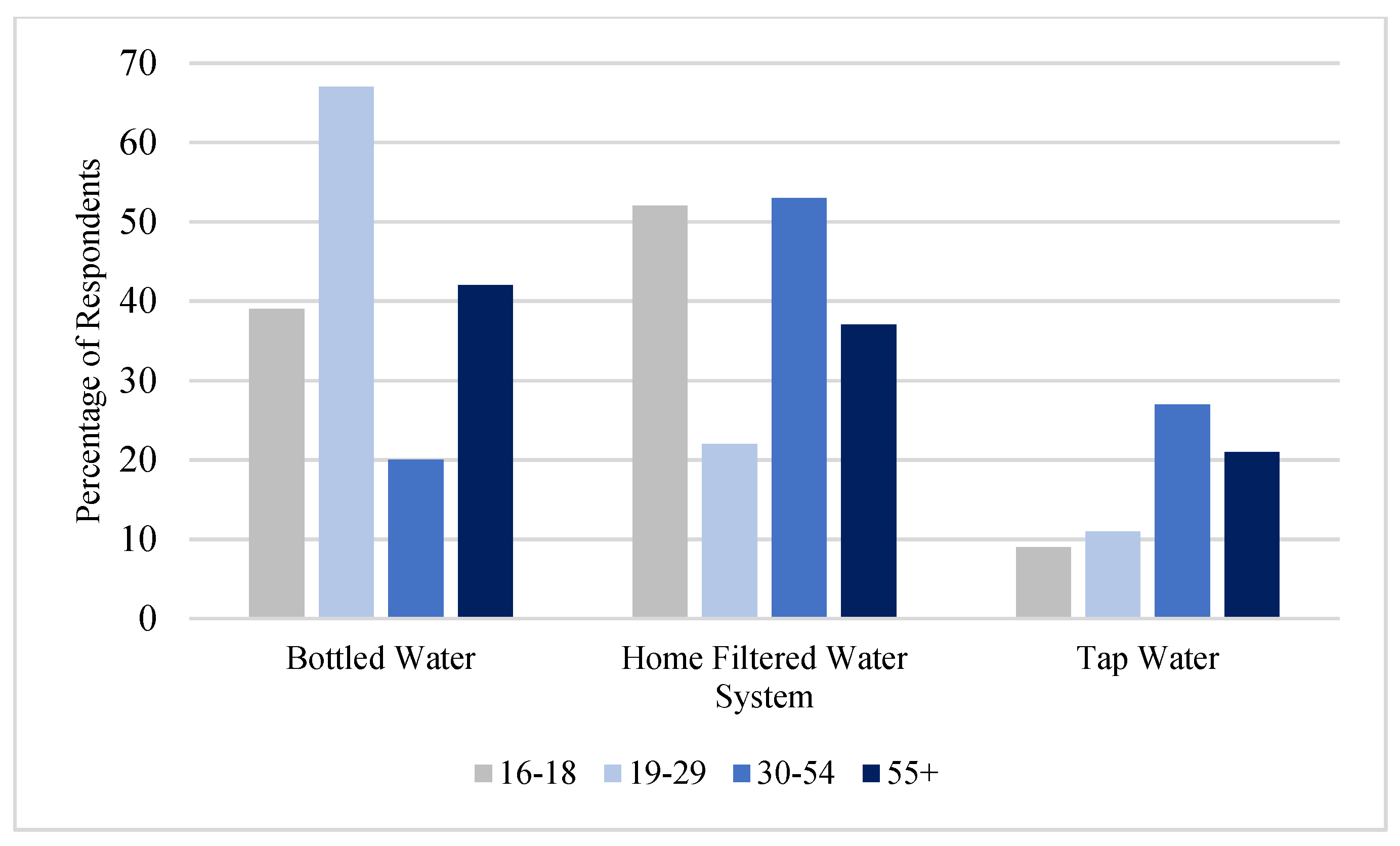
3.1.2. Summary of Participants Responses to Question about Tap Water
3.2. Results Phase 2: Checklist
- Determine the level of environmental literacy levels of the intended audience.
- Determine what the audience knows before they are exposed to the materials.
- Deliver the message as a story rather than as a lecture.
- More talking with less PowerPoint.
- Use a conversational tone.
- Communicator should have applicable knowledge as well as the personality and presentation skills to engage the audience.
- Make an emotional tie to all information to address their perceived risk.
- Use anecdotes, stories, narratives, or examples to make data come alive.
- Use risk comparisons; they must consider the distinctions the public considers important.
3.2.1. Nine Principles of Risk and Safety Communication
3.2.2. Results Phase 3: Protocol Development
3.3. Results Phase 4: Training Module
- Introduction to the broad strokes of Risk and Safety communication, its importance, and how it is implemented to a larger community audience.
- Discussion of the importance of an understanding of risk perception and plain language for effective communication
- Description of the Risk and Safety Model for developing messages and materials as well as the various media for different audiences
- Using the evaluation checklist to ensure all components of the protocol are included in the creation of messages and materials.
- An assignment to describe the community audience and any hazards that are present to create a fact sheet, presentation, or social media regarding the hazard and how the community can protect themselves, their family members, or their community. A list of other materials to include should be created but not developed.
- To access the site, potential students are asked to contact Ben Richmond at richmond@pharmacy.arizona.edu.
4. Discussion
4.1. Lessons Learned
4.2. Limitations and Future Research Directions
“the strength of focus groups lies not in quantitative analysis or in making statistically probable generalizations but in the fact that focus groups can show some evaluations, approaches, and mechanisms that exist in the target population, and they can provide characterization of the phenomena studied. Focus groups can help in building theories”.[37]
4.3. Novelty of This Project
5. Summary and Conclusions
5.1. Recommendations
5.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lindsey, M. Implications of Literacy Related to Comprehension of Environmental Health Materials. 2010. Available online: https://repository.arizona.edu/handle/10150/193851 (accessed on 30 August 2021).
- Lindsey, M.; Chen, S.; Richmond, B.; Valdez, M.; Velez, M.; Spradlin, J. Knowledge and skills associated with Environmental Health Literacy. Int. J. Environ. Res. Public Health 2021, 18, 11626. [Google Scholar] [CrossRef] [PubMed]
- Tucson Water. Site History—City of Tucson. Available online: https://www.tucsonaz.gov/files/water/docs/AOP_TARP_educational_signs.pdf (accessed on 3 April 2022).
- Arizona Departments of Environmental Quality. Protecting Tucson’s Drinking Water Supply|PFAS Resources. Available online: https://www.azdeq.gov/protecting-tucsons-drinking-water-supply-pfas-resources (accessed on 3 April 2022).
- US Environmental Protection Agency. EPA Superfund Site Cleanup Activities. Available online: https://cumulis.epa.gov/supercpad/SiteProfiles/index.cfm?fuseaction=second.Cleanup&id=0900684#bkground (accessed on 3 April 2022).
- Unified Community Advisory Board 1,4-Dioxane|Official website of the City of Tucson (tucsonaz.gov). Available online: https://www.tucsonaz.gov/water/1-4-dioxane (accessed on 18 April 2022).
- EPA. Trichloroethylene—US Environmental Protection Agency. 2000. Available online: https://www.epa.gov/assessing-and-managing-chemicals-under-tsca/risk-management-trichloroethylene-tce (accessed on 18 April 2022).
- Sneed, A. Forever Chemicals Are Widespread in U.S. Drinking Water. 2021. Available online: https://www.scientificamerican.com/article/forever-chemicals-are-widespread-in-u-s-drinking-water/#:~:text=The%20scientists%20estimated%20that%20more,trillion%20(ppt)%20or%20higher (accessed on 3 April 2022).
- Water Resources; US Geological Service. Groundwater Quality in Principal Aquifers of the Nation, 1991–2010. 2019. Available online: https://www.usgs.gov/mission-areas/water-resources/science/groundwater-quality-principal-aquifers-nation-1991-2010 (accessed on 3 April 2022).
- World Population Review. Tucson, Arizona Population 2022. Available online: https://worldpopulationreview.com/us-cities/tucson-az-population (accessed on 30 August 2021).
- National Health Literacy Mapping to Inform Health Care Policy. Health Literacy Data Map. University of North Carolina at Chapel Hill. 2014. Retrieved 30 August 2021. Available online: http://healthliteracymap.unc.edu/ (accessed on 3 April 2011).
- PlainLanguage.gov. Plain Language. Available online: https://www.plainlanguage.gov/about/definitions/ (accessed on 3 April 2022).
- National Institute of Environmental Health Sciences. Environmental Health Literacy: The Evolution of a New Field. 2014. Available online: https://www.niehs.nih.gov/research/supported/translational/peph/webinars/health_literacy/index.cfm (accessed on 30 August 2021).
- London, J.K.; Haapanen, K.A.; Backus, A.; Mack, S.M.; Lindsey, M.; Andrade, K. Aligning community-engaged research to context. Int. J. Environ. Res. Public Health 2020, 17, 1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, S.; Fewtrell, L.; Brtram, J. Risk Communication. In Water Quality: Guidelines, Standards and Health; WHO: Geneva, Switzerland, 2001; pp. 317–332. [Google Scholar]
- Guillaume, J.H.; Helgeson, C.; Elsawah, S.; Jakeman, A.J.; Kummu, M. Toward best practice framing of uncertainty in scientific publications: A review of Water Resources Research abstracts. Water Resour. Res. 2017, 53, 6744–6762. [Google Scholar] [CrossRef] [Green Version]
- Hyman, A.; Arlikatti, S.; Huang, S.K.; Lindell, M.K.; Mumpower, J.; Prater, C.S.; Wu, H.C. How do Perceptions of Risk Communicator Attributes Affect Emergency Response? An Examination of a Water Contamination Emergency in Boston, USA. Water Resour. Res. 2022, 58, e2021WR030669. [Google Scholar] [CrossRef]
- Kutner, M.; Greenberg, E.; Jin, Y.; Paulsen, C. The Health Literacy of America’s Adults. 2006. Available online: https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2006483 (accessed on 30 August 2021).
- Finn, S.; O’Fallon, L. The emergence of environmental health literacy—From its roots to its future potential. Environ. Health Perspect. 2017, 125, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covello, V.T.; McCallum, D.B.; Pavlova, M. Principles and guidelines for improving risk communication. In Effective Risk Communication; Springer: Boston, MA, USA, 1989; pp. 3–16. [Google Scholar]
- Chen, S.R.; Lindsey, M. Workshop Abstracts. Partners in Environmental Public Health Conference, Communication Research in Environmental Health Sciences: Environmental Health Literacy. 2014. Available online: https://www.niehs.nih.gov/news/events/pastmtg/2014/peph/index.cfm. (accessed on 30 August 2021).
- Covello, V.T. Development of Risk Communication Theory and Practice. 2022. Available online: https://ieeexplore.ieee.org/abstract/document/9649003 (accessed on 3 April 2022).
- Sandman, P.M. Risk communication: Facing public outrage. EPA J. 1987, 13, 21. [Google Scholar] [CrossRef] [Green Version]
- Slovic, P. Public perception of risk. J. Environ. Health 1997, 59, 22–25. [Google Scholar]
- Löfstedt, R.E.; Perri. What environmental and technological risk communication research and health risk research can learn from each other. J. Risk Res. 2008, 11, 141–167. Available online: https://www.tandfonline.com/doi/abs/10.1080/13669870701797137 (accessed on 30 August 2021). [CrossRef]
- Sinisi, L. Public Concerns and Risk Communication; National Environmental Protection Agency: Roma, Italy, 2004.
- McComas, K.A. Citizen satisfaction with public meetings used for risk communication. J. Appl. Commun. Res. 2003, 31, 164–184. [Google Scholar] [CrossRef]
- Fortun, K. From Bhopal to the informating of environmentalism: Risk communication in historical perspective. Osiris 2004, 19, 283–296. [Google Scholar] [CrossRef]
- Klein, W.M.; Boutté, A.K.; Brake, H.; Beal, M.; Lyon-Daniel, K.; Eisenhauer, E.; Grasso, M.; Hubbell, B.; Jenni, K.E.; Lauer, C.J.; et al. Leveraging risk communication science across US federal agencies. Nat. Hum. Behav. 2021, 5, 411–413. Available online: https://pubmed.ncbi.nlm.nih.gov/33737732/. (accessed on 18 April 2022). [CrossRef] [PubMed]
- Gibbs, A. Social Research Update 19: Focus Groups; Department of Sociology, University of Surrey: Guildford, UK, 1997; Available online: https://sru.soc.surrey.ac.uk/SRU19.html#:~:text=Why%20use%20focus%20groups%20and,one%20interviewing%2C%20or%20questionnaire%20surveys (accessed on 3 April 2022).
- Wilkinson, S. Focus group methodology: A review. Int. J. Soc. Res. Methodol. 1998, 1, 181–203. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; Pine Forge Press: Newbury Park, CA, USA, 2006. [Google Scholar]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Farmer, T.; Robinson, K.; Elliott, S.J.; Eyles, J. Developing and implementing a triangulation protocol for qualitative health research. Qual. Health Res. 2006, 16, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Davidson, D.J. Evaluating the effects of living with contamination from the lens of trauma: A case study of fracking development in Alberta, Canada. Environ. Sociol. 2018, 4, 196–209. [Google Scholar] [CrossRef] [Green Version]
- Turner, M.M.; Skubisz, C.; Rimal, R.N. Theory and practice in risk communication: A review of the literature and visions for the future. In The Routledge Handbook of Health Communication; Routledge: London, UK, 2011; pp. 174–192. [Google Scholar]
- Barbour, R.S. Making sense of focus groups. Med. Educ. 2005, 39, 742–750. [Google Scholar] [CrossRef]
- Smithson, J. Using and analysing focus groups: Limitations and possibilities. Int. J. Soc. Res. Methodol. 2000, 3, 103–119. [Google Scholar] [CrossRef]
- Rohlman, D.; Kile, M.L.; Irvin, V.L. Developing a Short Assessment of Environmental Health Literacy (SA-EHL). Int. J. Environ. Res. Public Health 2022, 19, 2062. [Google Scholar] [CrossRef]
- Hoover, A.G.; Heiger-Bernays, W.; Ojha, S.; Pennell, K.G. Balancing incomplete COVID-19 evidence and local priorities: Risk communication and stakeholder engagement strategies for school re-opening. Rev. Environ. Health 2021, 36, 27–37. [Google Scholar] [CrossRef]
- Binder, A.R.; May, K.; Murphy, J.; Gross, A.; Carlsten, E. Environmental Health Literacy as Knowing, Feeling, and Believing: Analyzing Linkages between Race, Ethnicity, and Socioeconomic Status and Willingness to Engage in Protective Behaviors against Health Threats. Int. J. Environ. Res. Public Health 2022, 19, 2701. [Google Scholar] [CrossRef]
- Pleasant, A.; Kuruvilla, S. A tale of two health literacies: Public health and clinical approaches to health literacy. Health Promot. Int. 2008, 23, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Adebisi, Y.A.; Rabe, A.; Lucero-Prisno, D.E., III. Risk communication and community engagement strategies for COVID-19 in 13 African countries. Health Promot. Perspect. 2021, 11, 137. [Google Scholar] [CrossRef] [PubMed]
- Hancock, H.E.; Bowles, T.C.; Rogers, W.A.; Fisk, A.D. Comprehension and retention of warning information. In Handbook of Warnings; Wogalter, M.S., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2006; pp. 267–278. [Google Scholar]
- Faour-Klingbeil, D.; Osaili, T.M.; Al-Nabulsi, A.A.; Jemni, M.; Todd, E.C. The public perception of food and non-food related risks of infection and trust in the risk communication during COVID-19 crisis: A study on selected countries from the Arab region. Food Control 2021, 121, 107617. [Google Scholar] [CrossRef] [PubMed]
- Koester, B.D.; Sloane, S.; Fujimoto, E.M.; Fiese, B.H.; Su, L.Y.F. What Do Childcare Providers Know about Environmental Influences on Children’s Health? Implications for Environmental Health Literacy Efforts. Int. J. Environ. Res. Public Health 2021, 18, 5489. [Google Scholar] [CrossRef] [PubMed]
- Junker, M.; Carpenter, A.T. Improving Public Perceptions of Tap Water. J. Am. Water Work. Assoc. 2021, 113, 66–72. [Google Scholar] [CrossRef]
- Odimayomi, T.O.; Proctor, C.R.; Wang, Q.E.; Sabbaghi, A.; Peterson, K.S.; Yu, D.J.; Lee, J.; Shah, A.D.; Ley, C.J.; Noh, Y.; et al. Water safety attitudes, risk perception, experiences, and education for households impacted by the 2018 Camp Fire, California. Nat. Hazards 2021, 108, 947–975. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Code Name | Sub-Code Name | 2nd Level Sub-Code | Description |
|---|---|---|---|
| Reasoning | Reasoning-Safe | Reasoning-safe-explanation: clear, boiling water, informer, have not become sick | A participant’s stance and explanation about the safety of their water. |
| Reasoning-Avoided | Reasoning-avoided-explanation: taste, feels funny, not clear | A participant’s stance and explanation about the concerns they identify in their water. | |
| Reasoning-Bottled Water | Reasoning-Bottled Water: taste, convenient, available | A participant’s choice to drink bottled water, and factors leading to that decision. | |
| Reasoning-Tap Water | Reasoning-Tap Water: bottles, expensive | A participant’s choice to drink tap water due to prohibitive cost of other forms. | |
| Reasoning-Tap Water: environmentally better | A participant’s choice to drink tap water due to environmental factors. | ||
| Reasoning-Tap Water: convenient, mixes to make other drinks | A participant’s choice to drink tap water due to convenience and easy use with other products. | ||
| Reasoning-Tap Water: forced | Participants are only willing to drink tap water when there are no other options. | ||
| Reasoning-Filtered Water | None | A participant’s choice to drink filtered water. | |
| Reasoning-Confidence level | Reasoning-Confidence Level: Level of confidence specified | A participant’s confidence or lack of confidence in their drinking water. | |
| Reasoning-Last Resort | None | A participant’s choice to only drink a form of water in a dire situation. | |
| Reasoning-Feeling of risk | Reasoning-Feeling of risk: Level of risk specified | A participant’s feelings of risks around drinking water. | |
| Treatment | Treatment-specific (ex: Brita) | Brita, fridge, filter | A participant’s actions to treat their water before consumption. |
| Consumption Pattern | Consumption Pattern-Regularly | Consumption Pattern-Regularly: Type of Water | How often and/or what type of water they consume. |
| Consumption Pattern-After Treatment | None | Alternative consumption pattern based on a treatment in the water. | |
| Consumption Pattern-Changing | None | A change in behavior around drinking water. | |
| Demographics | Demographics-Birthplace/origin | None | A participant’s birthplace/place of origin. |
| Demographics-Residence | Demographics-Residence: Time in Tucson | A participant’s area of residence, and how long they have resided in an area. | |
| Demographics-Education | None | The educational background of participants. | |
| Definition | Definitions-Contaminated Water | Definitions-Contaminated Water-Example | A participant’s definition or example of contaminated water. |
| Information Source | Information Source-Influence | None | A participant’s beliefs surrounding the influence of an information source. |
| Information Source-Trusted | Information Source-Trusted-Specific Media: news, social media, Twitter, water company/utility | A participant’s trust in an information source. | |
| Information Source-Trusted-Level of Trust/Credibility | A participant’s belief in the credibility and/or level of trust in a source. | ||
| Information Source-Type of Source Specified | None | A specific type of source that is sought out for information. | |
| Information Source-Severity | None | A participant’s belief that a type of information source means the information is more severe. | |
| Information Seeking | Information Seeking-Questions | None | A participant is asking questions about information that is wanted. |
| Information Seeking-Concerns | None | A participant has concerns about some information and would more information to address them. | |
| Information Seeking-Answers | None | Provide answers to participant questions or concerns. | |
| Preexisting Knowledge | Preexisting Knowledge-Contaminants | None | Prior knowledge about contaminants that participants brought in. |
| Preexisting Knowledge-Example of World Events | None | Knowledge about current world events that serve as examples of information in the focus group. |
| Information needed for effective message and materials development: |
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindsey, M.; Richmond, B.; Quintanar, D.R.; Spradlin, J.; Halili, L. Insights into Improving Risk and Safety Communication through Environmental Health Literacy. Int. J. Environ. Res. Public Health 2022, 19, 5330. https://doi.org/10.3390/ijerph19095330
Lindsey M, Richmond B, Quintanar DR, Spradlin J, Halili L. Insights into Improving Risk and Safety Communication through Environmental Health Literacy. International Journal of Environmental Research and Public Health. 2022; 19(9):5330. https://doi.org/10.3390/ijerph19095330
Chicago/Turabian StyleLindsey, Marti, Ben Richmond, Daniel R. Quintanar, Jordan Spradlin, and Loren Halili. 2022. "Insights into Improving Risk and Safety Communication through Environmental Health Literacy" International Journal of Environmental Research and Public Health 19, no. 9: 5330. https://doi.org/10.3390/ijerph19095330
APA StyleLindsey, M., Richmond, B., Quintanar, D. R., Spradlin, J., & Halili, L. (2022). Insights into Improving Risk and Safety Communication through Environmental Health Literacy. International Journal of Environmental Research and Public Health, 19(9), 5330. https://doi.org/10.3390/ijerph19095330