
The Effects of a 16-Week School-Based Exercise Program on Anxiety in Children with Autism Spectrum Disorder


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
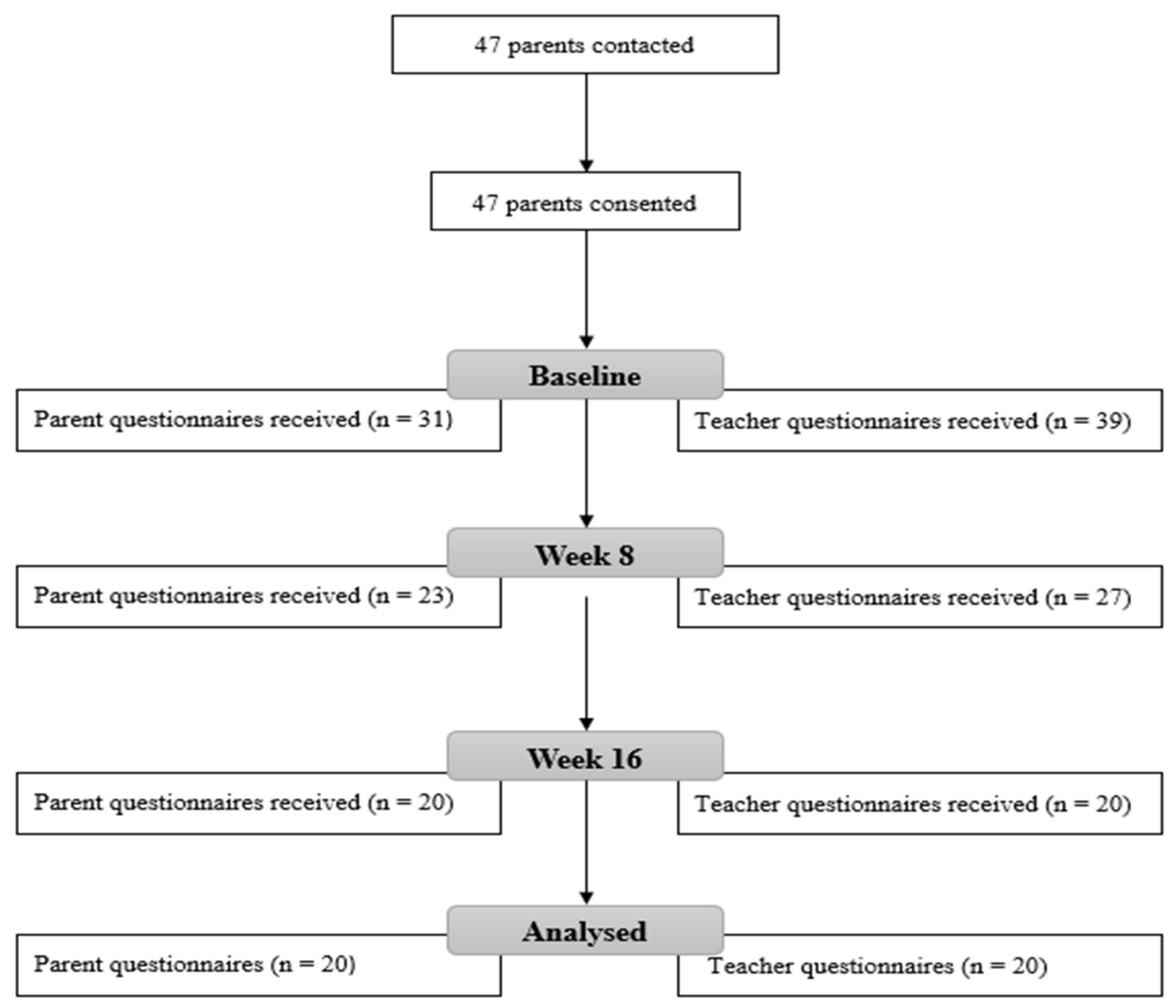
2.2. Study Design
2.3. Measures
2.4. Exercise Intervention
2.5. Statistical Analysis
3. Results
3.1. Teacher ASC-ASD
3.2. Parent ASC-ASD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leyfer, O.T.; Folstein, S.E.; Bacalman, S.; Davis, N.O.; Dinh, E.; Morgan, J.; Tager-Flusberg, H.; Lainhart, J.E. Comorbid Psyhiatric Disorders in Children with Autism: Interview Development and Rates of Disorders. J. Autism Dev. Disord. 2006, 36, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Muris, P.; Steerneman, P.; Merckelbach, H.; Holdrinet, I.; Meesters, C. Comorbid anxiety symptoms in children with pervasive developmental disorders. J. Anxiety Disord. 1998, 12, 387–393. [Google Scholar] [CrossRef]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric Disorders in Children with Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [Green Version]
- Van Steensel, F.J.A.; Bögels, S.M.; Perrin, S. Anxiety Disorders in Children and Adolescents with Autistic Spectrum Disorders: A Meta-Analysis. Clin. Child Fam. Psychol. Rev. 2001, 14, 302–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellini, S. Social Skill Deficits and Anxiety in High-Functioning Adolescents with Autism Spectrum Disorders. Focus Autism Other Dev. Disabil. 2004, 19, 78–86. [Google Scholar] [CrossRef]
- Gillott, A.; Furniss, F.; Walter, A. Anxiety in high-functioning children with autism. Autism 2001, 5, 277–286. [Google Scholar] [CrossRef]
- Kim, J.A.; Szatmari, P.; Bryson, S.E.; Streiner, D.L.; Wilson, F.J. The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism 2000, 4, 117–132. [Google Scholar] [CrossRef]
- Tantam, D. Psychological disorder in adolescents and adults with Asperger syndrome. Autism 2000, 4, 47–62. [Google Scholar] [CrossRef]
- Bastiaansen, D.; Koot, H.M.; Ferdinand, R.F.; Verhulst, F.C. Quality of Life in Children with Psychiatric Disorders: Self-, Parent, and Clinician Report. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 221–230. [Google Scholar] [CrossRef] [Green Version]
- Delli, C.K.S.; Polychronopoulou, S.A.; Kolaitis, G.A.; Antoniou, A.-S.G. Review of interventions for the management of anxiety symptoms in children with ASD. Neurosci. Biobehav. Rev. 2018, 95, 449–463. [Google Scholar] [CrossRef]
- White, S.W.; Simmons, G.L.; Gotham, K.O.; Conner, C.M.; Smith, I.C.; Beck, K.B.; Mazefsky, C.A. Psychosocial Treatments Targeting Anxiety and Depression in Adolescents and Adults on the Autism Spectrum: Review of the Latest Research and Recommended Future Directions. Curr. Psychiatry Rep. 2018, 20, 82. [Google Scholar] [CrossRef] [PubMed]
- Coury, D.L.; Anagnostou, E.; Manning-Courtney, P.; Reynolds, A.; Cole, L.; McCoy, R.; Whitaker, A.; Perrin, J.M. Use of Psychotropic Medication in Children and Adolescents with Autism Spectrum Disorders. Pediatrics 2012, 130, 69–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsia, Y.; Wong, A.Y.S.; Murphy, D.G.M.; Simonoff, E.; Buitelaar, J.K.; Wong, I.C.K. Psychopharmacological prescriptions for people with autism spectrum disorder (ASD): A multinational study. Psychopharmacology 2014, 231, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Vasa, R.A.; Carroll, L.M.; Nozzolillo, A.A.; Mahajan, R.; Mazurek, M.O.; Bennett, A.E.; Wink, L.K.; Bernal, M.P. A Systematic Review of Treatments for Anxiety in Youth with Autism Spectrum Disorders. J. Autism Dev. Disord. 2014, 44, 3215–3229. [Google Scholar] [CrossRef]
- Coleman, D.M.; Adams, J.B.; Anderson, A.L.; Frye, R.E. Rating of the Effectiveness of 26 Psychiatric and Seizure Medications for Autism Spectrum Disorder: Results of a National Survey. J. Child Adolesc. Psychopharmacol. 2019, 29, 107–123. [Google Scholar] [CrossRef] [Green Version]
- Hellings, J.A.; Zarcone, J.R.; Crandall, K.; Wallace, D.; Schroeder, S.R. Weight gain in a controlled study of risperidone in children, adolescents and adults with mental retardation and autism. J. Child Adolesc. Psychopharmacol. 2001, 11, 229–238. [Google Scholar] [CrossRef]
- Ung, D.; Selles, R.; Small, B.J.; Storch, E.A. A Systematic Review and Meta-Analysis of Cognitive-Behavioral Therapy for Anxiety in Youth with High-Functioning Autism Spectrum Disorders. Child Psychiatry Hum. Dev. 2015, 46, 533–547. [Google Scholar] [CrossRef]
- Kreslins, A.; Robertson, A.E.; Melville, C. The effectiveness of psychosocial interventions for anxiety in children and adolescents with autism spectrum disorder: A systematic review and meta-analysis. Child Adolesc. Psychiatry Ment. Health 2015, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Bartley, C.A.; Hay, M.; Bloch, M.H. Meta-analysis: Aerobic exercise for the treatment of anxiety disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 45, 34–39. [Google Scholar] [CrossRef]
- Jayakody, K.; Gunadasa, S.; Hosker, C. Exercise for anxiety disorders: Systematic review. Br. J. Sports Med. 2014, 48, 187–196. [Google Scholar] [CrossRef]
- Stonerock, G.L.; Hoffman, B.M.; Smith, P.J.; Blumenthal, J.A. Exercise as Treatment for Anxiety: Systematic Review and Analysis. Ann. Behav. Med. 2015, 49, 542–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strohle, A.; Hofler, M.; Pfister, H.; Muller, A.-G.; Hoyer, J.; Wittchen, H.-U.; Lieb, R. Physical activity and prevalence and incidence of mental disorders in adolescents and young adults. Psychol. Med. 2007, 37, 1657–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillier, A.; Murphy, D.; Ferrara, C. A Pilot Study: Short-Term Reduction in Salivary Cortisol Following Low Level Physical Exercise and Relaxation among Adolescents and Young Adults on the Autism Spectrum. Stress Health 2011, 27, 395–402. [Google Scholar] [CrossRef]
- Golsefidi, R.N.; Hashemi, E.S. Effect of Selected Spark Motor Program on Anxiety of Children with Asperger. Phys. Treat. Specif. Phys. Ther. 2015, 5, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.; Shivakumar, G. Effects of exercise and physical activity on anxiety. Front. Psychiatry 2013, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.-W.; Kuo, Y.-M.; Lin, T.-W.; Kuo, Y.-M. Exercise Benefits Brain Function: The Monoamine Connection. Brain Sci. 2013, 3, 39–53. [Google Scholar] [CrossRef]
- Ströhle, A.; Feller, C.; Onken, M.; Godemann, F.; Heinz, A.; Dimeo, F. The Acute Antipanic Activity of Aerobic Exercise. Am. J. Psychiatry 2005, 162, 2376–2378. [Google Scholar] [CrossRef]
- Thoren, P.; Floras, J.S.; Hoffmann, P.; Seals, D.R. Endorphins and exercise: Physiological mechanisms and clinical implications. Med. Sci. Sports Exerc. 1990, 22, 417–428. [Google Scholar]
- Goddard, A.W.; Ball, S.G.; Martinez, J.; Robinson, M.J.; Yang, C.R.; Russell, J.M.; Shekhar, A. Current perspectives of the roles of the central norepinephrine system in anxiety and depression. Depression Anxiety 2010, 27, 339–350. [Google Scholar] [CrossRef]
- Hang, A.; Wang, Y.; He, L.; Liu, J. The role of the dynorphin/κ opioid receptor system in anxiety. Acta Pharmacol. Sin. 2015, 36, 783–790. [Google Scholar] [CrossRef]
- Kant, G.J.; Leu, J.R.; Anderson, S.M.; Mougey, E.H. Effects of chronic stress on plasma corticosterone, ACTH and prolactin. Physiol. Behav. 1987, 40, 775–779. [Google Scholar] [CrossRef]
- Bodin, T.; Martinsen, E.W. Mood and Self-Efficacy during Acute Exercise in Clinical Depression. A Randomized, Controlled Study. J. Sport Exerc. Psychol. 2004, 26, 623–633. [Google Scholar] [CrossRef]
- Broman-Fulks, J.J.; Berman, M.E.; Rabian, B.A.; Webster, M.J. Effects of aerobic exercise on anxiety sensitivity. Behav. Res. Ther. 2004, 42, 125–136. [Google Scholar] [CrossRef] [Green Version]
- Petruzzello, S.J.; Landers, D.M.; Hatfield, B.D.; Kubitz, K.A.; Salazar, W. A Meta-Analysis on the Anxiety-Reducing Effects of Acute and Chronic Exercise. Sports Med. 1991, 11, 143–182. [Google Scholar] [CrossRef] [PubMed]
- Mayes, S.D.; Calhoun, S.L.; Murray, M.J.; Zahid, J. Variables Associated with Anxiety and Depression in Children with Autism. J. Dev. Phys. Disabil. 2011, 23, 325–337. [Google Scholar] [CrossRef]
- Adams, D.; Young, K.; Keen, D. Anxiety in Children with Autism at School: A Systematic Review. Rev. J. Autism Dev. Disord. 2019, 6, 274–288. [Google Scholar] [CrossRef]
- South, M.; Williams, B.J.; McMahon, W.M.; Owley, T.; Filipek, P.A.; Shernoff, E.; Corsello, C.; Lainhart, J.E.; Lainhart, J.E.; Ozonoff, S. Utility of the Gilliam Autism Rating Scale in Research and Clinical Populations. J. Autism Dev. Disord. 2002, 32, 593–599. [Google Scholar] [CrossRef]
- Rodgers, J.; Wigham, S.; McConachie, H.; Freeston, M.; Honey, E.; Parr, J.R. Development of the anxiety scale for children with autism spectrum disorder (ASC-ASD). Autism Res. 2016, 9, 1205–1215. [Google Scholar] [CrossRef] [Green Version]
- Den Houting, J.; Adams, D.; Roberts, J.; Keen, D. An exploration of autism-specific and non-autism-specific measures of anxiety symptomatology in school-aged autistic children. Clin. Psychol. 2018, 23, 237–248. [Google Scholar] [CrossRef]
- Coffey, C.; Carey, M.; Kinsella, S.; Byrne, P.J.; Sheehan, D.; Lloyd, R.S. Exercise Programming for Children with Autism Spectrum Disorder. Strength Cond. J. 2020, 43, 64–74. [Google Scholar] [CrossRef]
- Yanardağ, M.; Yılmaz, İ.; Aras, Ö. Approaches to the Teaching Exercise and Sports for the Children with Autism. Int. J. Early Child. Spec. Educ. (INT-JECSE) 2010, 2, 214–230. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Mangiafico, S.S. Summary and Analysis of Extension Program Evaluation in R.; Rutgers Cooperative Extension: Mays Landing, NJ, USA, 2016. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE Publications: London, UK, 2013. [Google Scholar]
- Ambler, P.G.; Eidels, A.; Gregory, C. Anxiety and aggression in adolescents with autism spectrum disorders attending mainstream schools. Res. Autism Spectr. Disord. 2015, 18, 97–109. [Google Scholar] [CrossRef]
- Ashburner, J.; Ziviani, J.; Rodger, S. Surviving in the mainstream: Capacity of children with autism spectrum disorders to perform academically and regulate their emotions and behavior at school. Res. Autism Spectr. Disord. 2010, 4, 18–27. [Google Scholar] [CrossRef]
- Tobias, A. Supporting students with autistic spectrum disorder (ASD) at secondary school: A parent and student perspective. Int. J. Phytoremediation 2009, 25, 151–165. [Google Scholar] [CrossRef]

{kind=link}
| Activity | Aim | Description |
|---|---|---|
| Traffic lights | Increase heart rate and warming up the muscles | Different-colored cones will be assigned an action: green = run, yellow = walk, red = stop. Progression: Introduce more actions such as blue = jump, orange = skipping, purple = high knees |
| Throwing and catching | Develop throwing and catching skills, coordination | Throwing and catching a small light ball between two children. Progression: Change ball and distance. Different throwing techniques such as overhead, underhand. Aim for different targets such as hoops, baskets. Games such as basketball. |
| Jumping | Jumping and landing skills, lower limb strength, balance | Double leg jumping through hula hoops in a straight line. Progression: Increasing distance between hoops and number of hoops. Different jumping techniques: single leg, sideways. Introduce ladders and hurdles. |
| Kicking | Kicking skills, coordination, balance | Kicking a small light ball between two children. Progression: Increase the distance. Dribbling around cones. Taking shots at goals. |
| Volleyball | Striking with a hand, coordination, upper limb strength | Passing a beach ball between two children (volleyball set and bump technique). Progression: Using a volleyball. Hitting over a net. |
| Badminton | Striking with an implement, coordination, upper limb strength | Hitting a beach ball with a badminton racket between two children. Progression: Using a shuttle instead of beach ball. Hitting over a net. Using tennis rackets. |
| Stretches | Lower heart rate, flexibility | Butterfly stretch, toe touches, knee hugs, quadricep stretch, shoulder stretch. |
| Variables | Overall Sample (n = 24) | Teacher-Reported Sample (n = 20) | Parent-Reported Sample (n = 20) | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Age (years) | 10.79 | 3.87 | 11.20 | 4.05 | 10.2 | 3.74 |
| Moderate ASD (n, %) | 6 (25%) | 5 | 6 | |||
| Severe ASD (n, %) | 18 (75%) | 15 | 14 | |||
| Variables | Baseline | Week 8 | Week 16 | p | % Change | |||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | Baseline–Week 16 | ||
| Total ASC-ASD | 19.05 | 12.08 | 14.55 | 12.48 | 6.8 | 5.77 | <0.001 | ↓ 64.3% |
| Performance Anxiety | 4.25 | 4.24 | 3 | 4.07 | 1.1 | 2.02 | <0.001 | ↓ 74.12% |
| Anxious Arousal | 3 | 2.43 | 1.75 | 2.22 | 0.55 | 0.95 | <0.001 | ↓ 81.67% |
| Separation Anxiety | 2.3 | 3.06 | 1.9 | 2.81 | 0.8 | 1.58 | 0.165 | ↓ 65.22% |
| Uncertainty | 9.5 | 5.69 | 7.9 | 5.65 | 4.35 | 3.03 | <0.001 | ↓ 54.21% |
| Variable | Baseline | Week 8 | Week 16 | p | % Change | |||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | Baseline–Week 16 | ||
| Total ASC-ASD | 14 | 9.41 | 13.1 | 7.46 | 12.75 | 8.64 | 0.911 | ↓ 8.93% |
| Performance Anxiety | 1.2 | 1.85 | 1.3 | 2.34 | 1.15 | 2.08 | 0.879 | ↓ 4.17% |
| Anxious Arousal | 2 | 2 | 1.35 | 1.39 | 1.35 | 1.81 | 0.41 | ↓ 32.5% |
| Separation Anxiety | 1.65 | 1.79 | 2.05 | 1.71 | 1.9 | 2.1 | 0.172 | ↑ 3.03% |
| Uncertainty | 9.15 | 6.01 | 8.4 | 4.8 | 8.35 | 5.6 | 0.647 | ↓ 8.74% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carey, M.; Sheehan, D.; Healy, S.; Knott, F.; Kinsella, S. The Effects of a 16-Week School-Based Exercise Program on Anxiety in Children with Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2022, 19, 5471. https://doi.org/10.3390/ijerph19095471
Carey M, Sheehan D, Healy S, Knott F, Kinsella S. The Effects of a 16-Week School-Based Exercise Program on Anxiety in Children with Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2022; 19(9):5471. https://doi.org/10.3390/ijerph19095471
Chicago/Turabian StyleCarey, Marie, Damien Sheehan, Sean Healy, Fiona Knott, and Sharon Kinsella. 2022. "The Effects of a 16-Week School-Based Exercise Program on Anxiety in Children with Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 19, no. 9: 5471. https://doi.org/10.3390/ijerph19095471