
Physicians’ Experiences and Perceptions of Environmental Factors Affecting Their Practices of Continuous Deep Sedation until Death: A Secondary Qualitative Analysis of an Interview Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Context
2.3. Primary Study: Research Paradigm
2.4. Primary Study: Participants and Recruitment
2.5. Primary Study: Data Collection
2.6. Primary Study: Ethical Considerations
2.7. Secondary Study: Secondary Qualitative Analysis
3. Results
3.1. Participant Characteristics
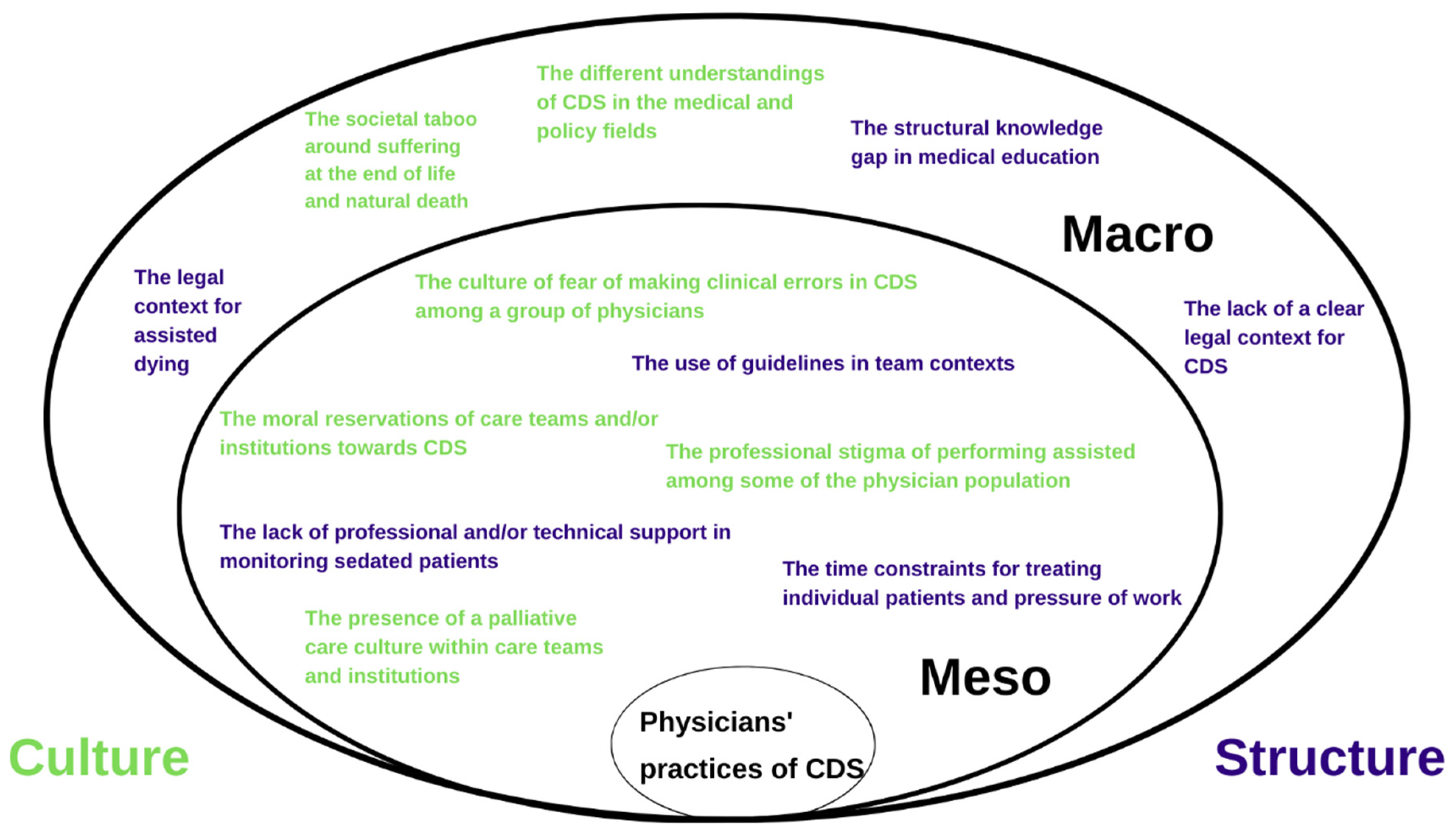
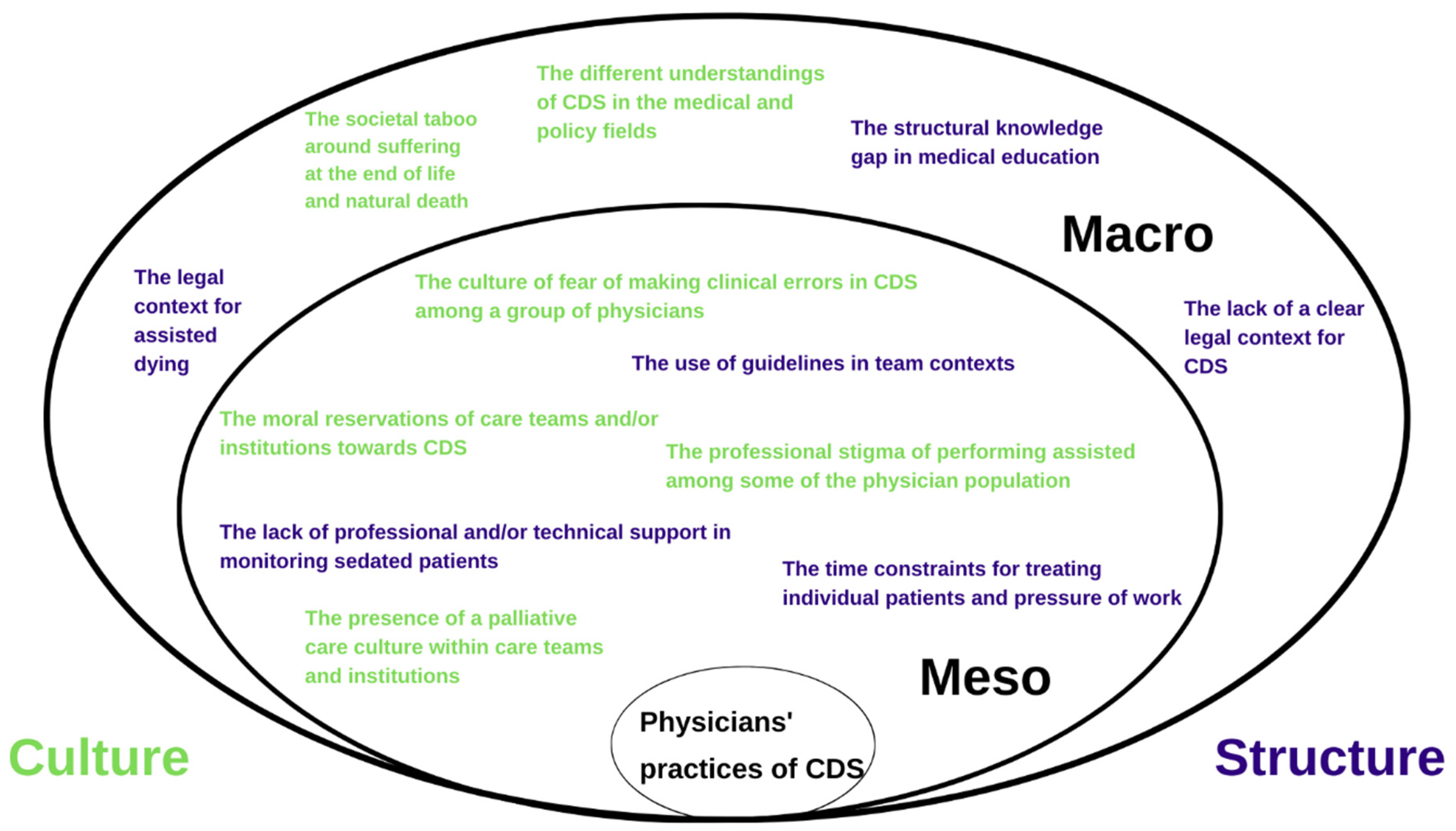
3.2. Environmental Factors
3.2.1. Structure: Meso
The Lack of Professional and/or Technical Support in Monitoring Sedated Patients
“As I am the physician, I always initiate the first step. And that works well. But it is up to the nurse to actually put their chair next to bed, so to speak, and adjust the doses so that the patient doesn’t wake up. You have to act very quickly. So that implies that you need to be with the patient all the time. In a nursing home, CDS cannot go well. Mostly there is only one nurse practitioner responsible for an entire corridor with patients. Here, too, where there is a lack of nurse practitioners, I don’t dare to initiate CDS.”(Geriatrician)
The Use of Guidelines in Team Contexts
The Time Constraints for Treating Individual Patients and Pressure of Work
“On the one hand, there is this extensive guideline. Firstly, it take some time to read it. Secondly, it devotes many pages to the conditions of CDS. This is explained in great detail. Then there is a short summary, which mainly focuses on the dosages in which starting schedule is added. The drugs have to be monitored every two hours. In practice, this is not always that easy. Monitoring CDS the way we are supposed to according to the guidelines. As a general practitioner, you lose a lot of time. You have to check the patient regularly during the CDS. That is not always possible in practical terms. Especially since they want us to treat more and more patients. So it is a matter of increasing the doses sometimes.”(General practitioner)
3.2.2. Structure: Macro
The Structural Knowledge Gap in Medical Education
“There is insufficient training for CDS and also insufficient knowledge. I have never had training on palliative sedation either. I never had anything about palliation. So a lot of doctors do not know what CDS means. Whatever their background is, they just think: “We will give them a bit of Midazolam and they will sleep. If it needs to go a bit faster? Then we should give them a bit more. After that, we add a little morphine. They think that CDS is pretty simple.”(Geriatrician)
The Legal Context for Assisted Dying
“There are also a number of questions in that registration document about assisted dying that are not always easy to answer, for example, that you have to specify what exactly is unbearable suffering. That is one thing. And then there is the practical side of the registration. You have to take it to the post office. You have to send it by registered mail.. You have to register all of this in your patient file. In itself, that is quite a lot of work for something in which we have already invested a lot of time and energy. And I know that many general practitioners often think: “You know, I have really invested a lot of time, energy and effort for this, for which I have been paid little or nothing. But I also have to spend another half hour filling in the paperwork for the registration and another half hour going to the post office to get everything done, waiting in line and so on.” I also notice that colleagues ask questions about this and that this is a barrier preventing them from doing it. And then sometimes CDS is chosen.”(GP)
The Lack of a Clear Legal Context for CDS
“I think it is desirable for there to be legislation on CDS and for it to be written a bit like a guideline of how to carry things out, that you have to start at a certain dose depending on the weight of the patient, and that you then have to re-evaluate and document whether the patient is comfortable or not, and that you may then adjust the drugs proportionally. I think everyone has their own method now, because there is very little that is clear and black-and-white due to the lack of legislation.”(Intensive care physician)
3.2.3. Culture: Meso
The Moral Reservations of Care Teams and/or Institutions towards CDS
“The annoying thing is that you always get caught up in all those ethics. Some physicians say: “You cannot do that. Being so deeply sedated? And is that ethically acceptable?” So yes, in that case I try to find the middle ground based on what I know from all the fields. And searching, and gaining experience. For example, I consult the professionals from intensive care, to achieve something that is acceptable for me, but also for them. How should I put it? Intellectually acceptable. But yes, in the end, the patient is not deeply sedated.”(Palliative care physician)
The Presence of a Palliative Care Culture within Care Teams and Institutions
“The biggest difference I see is in the nursing home where I am involved. I think we have a good palliative culture there, and we have also had a palliative care coordinator for the last year who was brought in solely for palliative care. We certainly give all the information about palliative care and CDS. So if you ask, “does everybody know what CDS entails?”, then it is certainly the intention for all our nurses to know what it means. When CDS is initiated, the coordinator will take the lead and support me and the nurses who sometimes take over the monitoring, but he will also support the resident’s family. That makes you feel, of course, as a GP, that you’re working in a medically authorized way and that makes things much easier.”(GP)
The Culture of Fear of Making Clinical Errors Regarding CDS among a Group of Physicians
The Professional Stigma of Performing Assisted Dying among Some of the Physician Population
“And then this ‘compromise’. Yes, I think that this is often done. I have already experienced situations in which I discuss a case with medical specialists about a patient with cancer who had requested assisted dying and they say: “No, we really cannot do that. And if the suffering gets too severe, then we can always do CDS.” So then this compromise is chosen. There should be a chance to be able to talk about life-shortening actions without coming before this ‘moral court’.”(General practitioner)
3.2.4. Culture: Macro
The Different Understandings of CDS in the Medical and Policy Fields
The Societal Taboo around Suffering at the End of Life and Natural Death
“That sometimes CDS is initiated too early is also due to pressure from the families. “And look at him lying here now. That is not good, let him sleep now.” And then, as a physician, you hit a bit of a wall and sometimes the dose is increased abnormally or other things are done with the intention of speeding things up. But then that is not always what was initially intended. But it is very often under pressure from our society that these things happen. We are not always used to seeing people die. But maybe that is a reality that we have to learn to deal with as physicians? And, yes, dying, they want you to keep people alive for as long as possible. But you should not talk about it too much. You should not do too much advanced care planning. But when they lie there. You cannot do that. That is not possible. Yes, it has to be ‘done’ yesterday rather than today. And that is the current society in which we are living nowadays.”(Intensive care physician)
4. Discussion
4.1. Summary of Main Findings
4.2. Strenghts and Limitations
4.3. Interpretation of the Findings
4.4. Recommendations and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Twycross, R. Reflections on Palliative Sedation. Palliat. Care Res. Treat. 2019, 12, 1178224218823511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, T.; Tsuneto, S.; Shima, Y. Definition of Sedation for Symptom Relief: A Systematic Literature Review and a Proposal of Operational Criteria. J. Pain Symptom Manag. 2002, 24, 447–453. [Google Scholar] [CrossRef]
- Morita, T.; Maeda, I.; Mori, M.; Imai, K.; Tsuneto, S. Uniform Definition of Continuous-Deep Sedation. Lancet Oncol. 2016, 17, e222. [Google Scholar] [CrossRef] [Green Version]
- Hasselaar, J. Palliative Sedation: A Medical-Ethical Exploration. In Textbook of Palliative Care; MacLeod, R.D., Van den Block, L., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Heijltjes, M.T.; van Thiel, G.J.M.W.; Rietjens, J.A.C.; van der Heide, A.; de Graeff, A.; van Delden, J.J.M. Changing Practices in the Use of Continuous Sedation at the End of Life: A Systematic Review of the Literature. J. Pain Symptom Manag. 2020, 60, 828–846. [Google Scholar] [CrossRef] [PubMed]
- Miccinesi, G.; Rietjens, J.A.C.; Deliens, L.; Paci, E.; Bosshard, G.; Nilstun, T.; Norup, M.; Van Der Wal, G. Continuous Deep Sedation: Physicians’ Experiences in Six European Countries. J. Pain Symptom Manag. 2006, 31, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Anquinet, L.; Rietjens, J.A.C.; Seale, C.; Seymour, J.; Deliens, L.; Van Der Heide, A. The Practice of Continuous Deep Sedation until Death in Flanders (Belgium), the Netherlands, and the U.K.: A Comparative Study. J. Pain Symptom Manag. 2012, 44, 33–43. [Google Scholar] [CrossRef]
- Seymour, J.; Rietjens, J.; Bruinsma, S.; Deliens, L.; Sterckx, S.; Mortier, F.; Brown, J.; Mathers, N.; Van Der Heide, A. Using Continuous Sedation until Death for Cancer Patients: A Qualitative Interview Study of Physicians’ and Nurses’ Practice in Three European Countries. Palliat. Med. 2015, 29, 48–59. [Google Scholar] [CrossRef] [Green Version]
- Raus, K.; Brown, J.; Seale, C.; Rietjens, J.A.; Janssens, R.; Bruinsma, S.; Mortier, F.; Payne, S.; Sterckx, S. Continuous Sedation until Death: The Everyday Moral Reasoning of Physicians, Nurses and Family Caregivers in the UK, the Netherlands and Belgium. BMC Med. Ethics 2014, 15, 14. [Google Scholar] [CrossRef] [Green Version]
- Robijn, L.; Seymour, J.; Deliens, L.; Korfage, I.; Brown, J.; Pype, P.; Van Der Heide, A.; Chambaere, K.; Rietjens, J. The Involvement of Cancer Patients in the Four Stages of Decision-Making Preceding Continuous Sedation until Death: A Qualitative Study. Palliat. Med. 2018, 32, 1198–1207. [Google Scholar] [CrossRef]
- Seale, C.; Raus, K.; Bruinsma, S.; van der Heide, A.; Sterckx, S.; Mortier, F.; Payne, S.; Mathers, N.; Rietjens, J. The Language of Sedation in End-of-Life Care: The Ethical Reasoning of Care Providers in Three Countries. Health 2015, 19, 339–354. [Google Scholar] [CrossRef]
- Arevalo, J.J.; Rietjens, J.A.; Swart, S.J.; Perez, R.S.G.M.; van der Heide, A. Day-to-Day Care in Palliative Sedation: Survey of Nurses’ Experiences with Decision-Making and Performance. Int. J. Nurs. Stud. 2013, 50, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Van Deijck, R.H.P.D.; Hasselaar, J.G.J.; Verhagen, S.C.A.H.H.V.M.; Vissers, K.C.P.; Koopmans, R.T.C.M. Determinants of the Administration of Continuous Palliative Sedation: A Systematic Review. J. Palliat. Med. 2013, 16, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- McBee, E.; Ratcliffe, T.; Picho, K.; Schuwirth, L.; Artino, A.R.; Yepes-Rios, A.M.; Masel, J.; Van Der Vleuten, C.; Durning, S.J. Contextual Factors and Clinical Reasoning: Differences in Diagnostic and Therapeutic Reasoning in Board Certified versus Resident Physicians. BMC Med. Educ. 2017, 17, 211. [Google Scholar] [CrossRef] [Green Version]
- Swart, S.J.; Rietjens, J.A.C.; Van Zuylen, L.; Zuurmond, W.W.A.; Perez, R.S.G.M.; Van Der Maas, P.J.; Van Delden, J.J.M.; Van Der Heide, A. Continuous Palliative Sedation for Cancer and Noncancer Patients. J. Pain Symptom Manag. 2012, 43, 172–181. [Google Scholar] [CrossRef]
- Maessen, M.; Veldink, J.; Onwuteaka-Philipsen, B.; de Vries, J.; Wokke, J.; Van Der Wal, G.; van den Berg, L. Trends and Determinants of End-of-Life Practices in ALS in the Netherland. Neurology 2009, 73, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Hasselaar, J.; Reuzel, R.; van den Muijsenbergh, M.; Koopmans, R.; Leget, C.; Crul, B.; Vissers, K. Dealing with Delicate Issues in Continuous Deep Sedation: Varying Practices among Dutch Medical Specialists, General Practitioners, and Nursing Home Physicians. Arch. Intern. Med. 2008, 168, 537–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, S.; Schmid, M.; Bopp, M.; Bosshard, G.; Puhan, M.A. Continuous Deep Sedation Until Death—a Swiss Death Certificate Study. J. Gen. Intern. Med. 2018, 33, 1052–1059. [Google Scholar] [CrossRef] [Green Version]
- van Tol, D.G.; Kouwenhoven, P.; Van Der Vegt, B.; Weyers, H. Dutch Physicians on the Role of the Family in Continuous Sedation. J. Med. Ethics 2015, 41, 240–244. [Google Scholar] [CrossRef]
- Reuzel, R.P.B.; Hasselaar, G.J.; Vissers, K.C.P.; van der Wilt, G.J.; Groenewoud, J.M.M.; Crui, B.J.P. Inappropriateness of Using Opioids for End-Stage Palliative Sedation: A Dutch Study. Palliat. Med. 2008, 22, 641–646. [Google Scholar] [CrossRef]
- Swart, S.J.; Brinkkemper, T.; Rietjens, J.A.C.; Blanker, M.H.; van Zuylen, L.; Ribbe, M.; Zuurmond, W.W.A.; van der Heide, A.; Perez, R.S.G.M. Physicians’ and Nurses’ Experiences With Continuous Palliative Sedation in the Netherlands Ontinuous. Arch. Intern. Med. 2010, 170, 1271–1274. [Google Scholar] [CrossRef] [Green Version]
- Robijn, L.; Deliens, L.; Scherrens, A.L.; Pauwels, N.S.; Pype, P.; Rietjens, J.; Chambaere, K. A Systematic Review of Quality Improvement Initiatives for Continuous Sedation until Death. Palliat. Med. 2021, 35, 670–682. [Google Scholar] [CrossRef] [PubMed]
- Vissers, S.; Robijn, L.; Dierickx, S.; Mortier, F.; Cohen, J.; Deliens, L.; Chambaere, K. Control Measures for Continuous Deep Sedation Until Death: A Framing Analysis of the Views of Physicians. Qual. Health Res. 2021, 31, 2390–2402. [Google Scholar] [CrossRef] [PubMed]
- Sterckx, S.; Raus, K.; Mortier, F. Continuous Sedation at the End of Life: Ethical, Clinical and Legal Perspectives; Cambridge University Press: Cambridge, UK, 2012; pp. 1–285. [Google Scholar] [CrossRef]
- Heaton, J. Reworking Qualitative Data; SAGE Publications: London, UK, 2004. [Google Scholar]
- Heaton, J. Secondary Analysis of Qualitative Data. In The Sage Handbook of Social Research Methods; SAGE: Newcastle upon Tyne, UK, 2008; pp. 1–631. [Google Scholar]
- Ruggiano, N.; Perry, T.E. Conducting Secondary Analysis of Qualitative Data: Should We, Can We, and How? Qual. Soc. Work 2019, 18, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Brownlie, J.; Howson, A. “Between the Demands of Truth and Government”: Health Practitioners, Trust and Immunisation Work. Soc. Sci. Med. 2006, 62, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Kia, H.; Salway, T.; Lacombe-Duncan, A.; Ferlatte, O.; Ross, L.E. “You Could Tell I Said the Wrong Things”: Constructions of Sexual Identity Among Older Gay Men in Healthcare Settings. Qual. Health Res. 2022, 32, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Dufour, I.F.; Richard, M.C. Theorizing from Secondary Qualitative Data: A Comparison of Two Data Analysis Methods. Cogent Educ. 2019, 6, 1690265. [Google Scholar] [CrossRef]
- Whiteside, M.; Mills, J.; McCalman, J. Using Secondary Data for Grounded Theory Analysis. Aust. Soc. Work 2012, 65, 504–516. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Robijn, L.; Cohen, J.; Rietjens, J.; Deliens, L.; Chambaere, K. Trends in Continuous Deep Sedation until Death between 2007 and 2013: A Repeated Nationwide Survey. PLoS ONE 2016, 11, e0158188. [Google Scholar] [CrossRef] [Green Version]
- Van Den Block, L.; Deschepper, R.; Bilsen, J.; Bossuyt, N.; Van Casteren, V.; Deliens, L. Euthanasia and Other End-of-Life Decisions: A Mortality Follow-Back Study in Belgium. BMC Public Health 2009, 9, 79. [Google Scholar] [CrossRef] [Green Version]
- Raus, K. Continuous Sedation at the End of Life: Practice, Perspectives and Ethical Analyses. Ph.D. Thesis, Ghent University, Ghent, Belgium, 2013. [Google Scholar]
- Federal Control and Evaluation Committee for Euthanasia. Ninth Report to the Belgian Parliament 2018–2019. Available online: https://www.endoflifecare.be/sites/default/files/atoms/files/KasperRaus_tekst_aangepast.pdf (accessed on 22 March 2022).
- Broeckaert, B.; Mullie, A.; Gielen, J.; Desmet, M.; Declerck, P.; Vanden Bergje, P. Palliatieve Sedatie Richtlijn Versie 2.0. 2012. Available online: https://palliatievezorgvlaanderen.be/wp-content/uploads/2021/07/richtlijn_palliatieve_sedatie.pdf (accessed on 22 March 2022).
- Zorgnet-Icuro. Ethisch Advies: Palliatieve Sedatie. Available online: https://www.zorgneticuro.be/publicaties/ethisch-advies-16-palliatieve-sedatie (accessed on 15 March 2022). [CrossRef]
- Life End Information Forum, L. Life End Application—LEA. Available online: https://www.levenseindeapp.be (accessed on 15 March 2022).
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Burr, V. Social Constructionism, 3rd ed.; Routledge: London, UK, 2003. [Google Scholar] [CrossRef]
- Palinkas, L.; Horwitz, S.; Green, C.; Wisdom, J.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, P. Toward an Ecology of Social Action: Merging the Ecological and Constructivist Traditions. Hum. Ecol. Rev. 2001, 8, 12–28. [Google Scholar]
- Besthorn, F.H. Ecological Social Work: Shifting Paradigms in Environmental Practice. Int. Encycl. Soc. Behav. Sci. Second Ed. 2015, 871–877. [Google Scholar] [CrossRef]
- Catton, W.R.; Dunlap, R.E. A New Ecological Paradigm for Post-Exuberant Sociology. Am. Behav. Sci. 1980, 24, 15–47. [Google Scholar] [CrossRef]
- Reckwitz, A. Toward a Theory of Social Practices: A Development in Culturalist Theorizing. Eur. J. Soc. Theory 2002, 5, 243–263. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Thomas, D. A General Inductive Approach for Qualitative Data Analysis. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, CA, USA, 1979. [Google Scholar] [CrossRef]
- Corden, A.; Sainsbury, R. Using Verbatim Quotations in Reporting Qualitative Social Research: The Views of Research Users; The Publications Office of the University of York: Heslington, UK, 2006. [Google Scholar]
- Williams, D.D.; Kimmons, R. Qualitative Rigor: How Do I Conduct Qualitative Research in a Rigorous Manner? Educ. Res. 2019, 1–20. [Google Scholar]
- Corti, L.; Thompson, P. The Secondary Analysis of Archived Qualitative Data; Qualitative Research Practice; Sage: London, UK, 2012; pp. 327–343. [Google Scholar]
- Higgs, J.; Jensen, G.M.; Stephen, L.; Christensen, N. Clinical Reasoning in the Health Professions, 4th ed.; Elsevier: Edinburgh, UK; London, UK; New York, NY, USA; Oxford, UK; Philadelphia, PA, USA; St. Louis, MO, USA; Sydney, Australia, 2019. [Google Scholar]
- McBee, E.; Ratcliffe, T.; Schuwirth, L.; O’Neill, D.; Meyer, H.; Madden, S.J.; Durning, S.J. Context and Clinical Reasoning: Understanding the Medical Student Perspective. Perspect. Med. Educ. 2018, 7, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Vivat, B.; Twycross, R. CSD Continuous Sedation Until Death; A Response to Changing Practices in the Use of Continuous Sedation at the End of Life: A Systematic Review of the Literature (Heijltjes et al., 2020). J. Pain Symptom Manag. 2022, 63, e139–e141. [Google Scholar] [CrossRef] [PubMed]
- Robijn, L.; Chambaere, K.; Raus, K.; Rietjens, J.; Deliens, L. Reasons for Continuous Sedation until Death in Cancer Patients: A Qualitative Interview Study. Eur. J. Cancer Care 2017, 26, e12405. [Google Scholar] [CrossRef] [PubMed]
- Sercu, M.; Pype, P.; Christiaens, T.; Derese, A.; Deveugele, M. Belgian General Practitioners’ Perspectives on the Use of Palliative Sedation in End-of-Life Home Care: A Qualitative Study. J. Pain Symptom Manag. 2014, 47, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Anquinet, L.; Raus, K.; Sterckx, S.; Smets, T.; Deliens, L.; Rietjens, J.A.C. Similarities and Differences between Continuous Sedation until Death and Euthanasia—Professional Caregivers’ Attitudes and Experiences: A Focus Group Study. Palliat. Med. 2013, 27, 553–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rietjens, J.A.C.; Buiting, H.M.; Pasman, H.R.W.; van der Maas, P.J.; van Delden, J.J.M.; van der Heide, A. Deciding about Continuous Deep Sedation: Physicians’ Perspectives: A Focus Group Study. Palliat. Med. 2009, 23, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Rys, S.; Deschepper, R.; Mortier, F.; Deliens, L.; Bilsen, J. Bridging the Gap Between Continuous Sedation Until Death and Physician-Assisted Death: A Focus Group Study in Nursing Homes in Flanders, Belgium. Am. J. Hosp. Palliat. Med. 2015, 32, 407–416. [Google Scholar] [CrossRef]
- Tomczyk, M.; Dieudonné-Rahm, N.; Jox, R.J. A Qualitative Study on Continuous Deep Sedation until Death as an Alternative to Assisted Suicide in Switzerland. BMC Palliat. Care 2021, 20, 67. [Google Scholar] [CrossRef]
- Cohen-Almagor, R.; Wesley Ely, E. Euthanasia and Palliative Sedation in Belgium. BMJ Support. Palliat. Care 2018, 8, 307–313. [Google Scholar] [CrossRef]
- Onwuteaka-Philipsen, B.D.; Legemaate, J.; van der Heide, A.; van Delden, H.; Evenblij, K.; El Hammoud, I.; Pasman, H.R.W.; Ploem, C.; Pronk, R.; van de Vathorst, S.; et al. Derde Evaluatie—Wet Toetsing Levensbeëindiging Op Verzoek En Hulp Bij Zelfdoding. Available online: https://publicaties.zonmw.nl/derde-evaluatie-wet-toetsing-levensbeeindiging-op-verzoek-en-hulp-bij-zelfdoding/ (accessed on 22 March 2022).

{kind=link}
| Medical Specialty | N (%) |
|---|---|
| Oncology | 13 (28) |
| General practice | 13 (28) |
| Intensive care medicine | 12 (26) |
| Geriatrics | 8 (17) |
| Anesthetics | 1 (2) |
| Additional medical training in palliative medicine * | 25 (53) |
| Professional care setting | |
| Hospital | 29 (62) |
| Home | 18 (38) |
| Age | |
| <35 years | 7 (15) |
| 35–44 years | 8 (17) |
| 45–54 years | 15 (32) |
| 55–64 years | 12 (26) |
| >64 years | 5 (11) |
| Sex | |
| Male | 26 (55) |
| Female | 21 (45) |
| Number of patients treated who had died in the 12 months prior to the interview | |
| none | 0 (0) |
| 1–5 patients | 2 (4) |
| 6–10 patients | 7 (15) |
| >10 patients | 38 (81) |
| Number of continuous deep sedations performed in the 12 months prior to the interview | |
| none | 0 (0) |
| 1–5 patients | 14 (30) |
| 6–10 patients | 5 (11) |
| >10 patients | 28 (59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vissers, S.; Dierickx, S.; Robijn, L.; Cohen, J.; Deliens, L.; Mortier, F.; Chambaere, K. Physicians’ Experiences and Perceptions of Environmental Factors Affecting Their Practices of Continuous Deep Sedation until Death: A Secondary Qualitative Analysis of an Interview Study. Int. J. Environ. Res. Public Health 2022, 19, 5472. https://doi.org/10.3390/ijerph19095472
Vissers S, Dierickx S, Robijn L, Cohen J, Deliens L, Mortier F, Chambaere K. Physicians’ Experiences and Perceptions of Environmental Factors Affecting Their Practices of Continuous Deep Sedation until Death: A Secondary Qualitative Analysis of an Interview Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5472. https://doi.org/10.3390/ijerph19095472
Chicago/Turabian StyleVissers, Stijn, Sigrid Dierickx, Lenzo Robijn, Joachim Cohen, Luc Deliens, Freddy Mortier, and Kenneth Chambaere. 2022. "Physicians’ Experiences and Perceptions of Environmental Factors Affecting Their Practices of Continuous Deep Sedation until Death: A Secondary Qualitative Analysis of an Interview Study" International Journal of Environmental Research and Public Health 19, no. 9: 5472. https://doi.org/10.3390/ijerph19095472