
The Impact of COVID-19 Pandemic on Outpatient Visits for All-Cause and Chronic Diseases in Korea: A Nationwide Population-Based Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design
2.3. Outbreak of COVID-19 in Korea
2.4. Statistical Analysis
3. Results
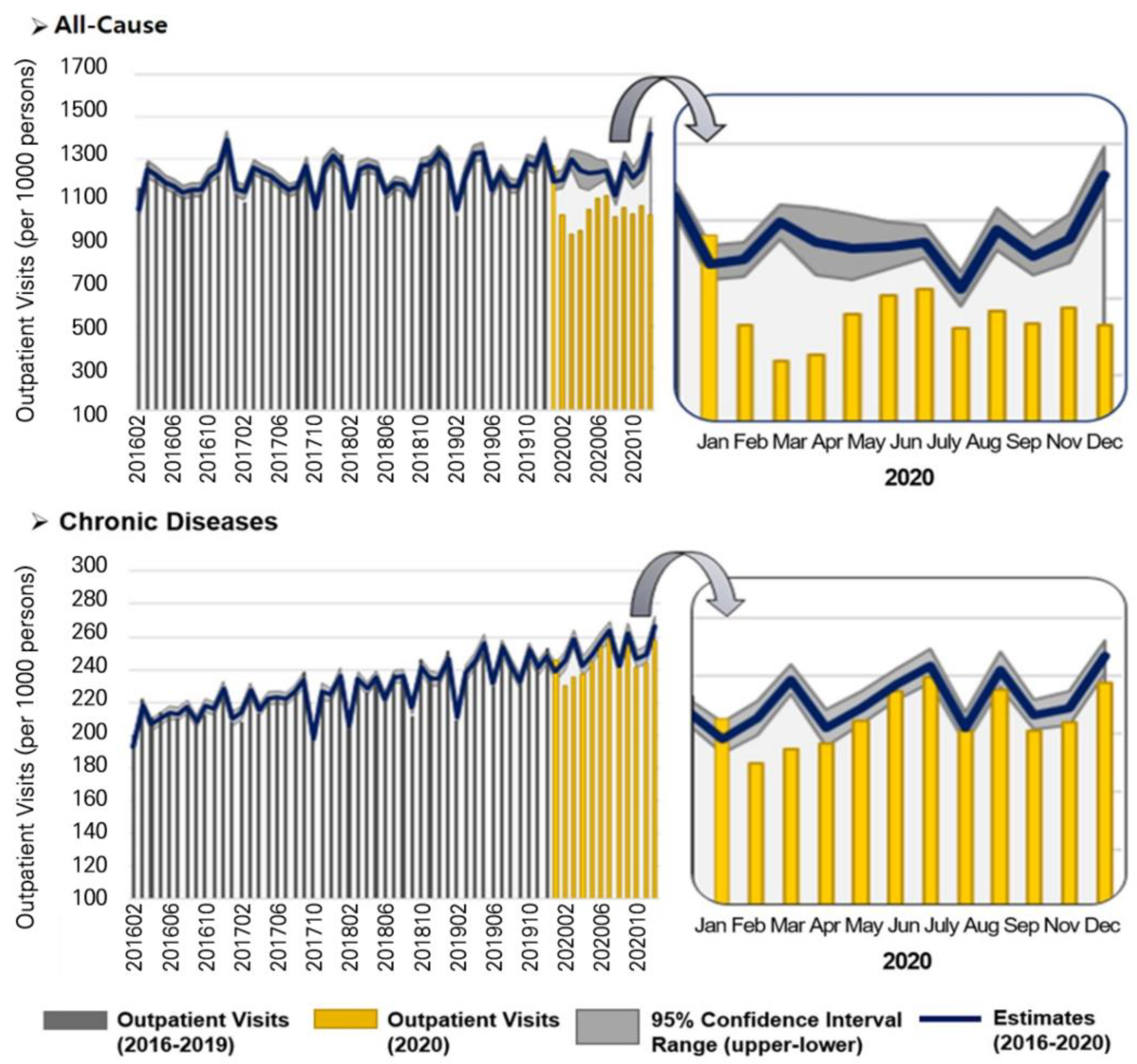
3.1. Trends in OP Visits from 2016 to 2020
3.2. Changes in OP Visits for All-Cause and Chronic Diseases in 2020
3.3. Changes in OP Visits among Chronic Disease Groups in 2020
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 26 December 2021).
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.G.; Kucharski, A.J.; Eggo, R.M.; Gimma, A.; Edmunds, W.J.; Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group. Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: A modelling study. Lancet Public Health 2020, 5, e375–e385. [Google Scholar] [CrossRef]
- Clerk, A.M. Beware of Neglect of Non-COVID Patients in COVID Era. Indian J. Crit. Care Med. 2021, 25, 837–838. [Google Scholar] [CrossRef]
- Hübner, M.; Zingg, T.; Martin, D.; Eckert, P.; Demartines, N. Surgery for non-COVID-19 patients during the pandemic. PLoS ONE 2020, 15, e0241331. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.T.U.; Villarroel, D.; de Luca, P.V.; Harnik, S.B.; Lima, B.L.S.; Wieselberg, R.J.P.; Giampaoli, V. COVID-19 impact on people with diabetes in South and Central America (SACA region). Diabetes Res. Clin. Pract. 2020, 166, 108301. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19-Related Concerns—United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- NPR, the Robert Wood Johnson Foundation, and the Harvard T.H. Chan School of Public Health. The impact of coronavirus on households across America. September 2020. Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/21/2020/09/NPR-RWJF-Harvard-National-Report_092220_Final1-4.pdf (accessed on 19 March 2022).
- Mian, B.M.; Siddiqui, S.; Ahmad, A.E. Management of urologic cancers during the pandemic and potential impact of treatment deferrals on outcomes. Urol. Oncol. 2021, 39, 258–267. [Google Scholar] [CrossRef]
- Mobula, L.M.; Heller, D.J.; Commodore-Mensah, Y.; Harris, V.W.; Cooper, L.A. Protecting the vulnerable during COVID-19: Treating and preventing chronic disease disparities. Gates Open Res. 2020, 4, 125. [Google Scholar] [CrossRef]
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; Felix, S.E.B.; Tie, Y.; Fullerton, K.E. Coronavirus Disease 2019 Case Surveillance—United States, 22 January–30 May 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control & Prevention. The Updates of COVID-19 in Republic of Korea (As of 17 February 2020). Available online: https://www.kdca.go.kr/board/board.es?mid=a30402000000&bid=0030 (accessed on 14 January 2022).
- Korea Central Disaster Management Headquarters. Extending Intensive “Social Distancing” for Another 2 Weeks. Available online: http://www.mohw.go.kr/eng/nw/nw0101vw.jsp?PAR_MENU_ID=1007&MENU_ID=100701&page=6&CONT_SEQ=353953 (accessed on 14 January 2022).
- Cho, K. Current status of non-communicable diseases in the Republic of Korea. Public Health Wkly. Rep. PHWR 2020, 14, 174–177. [Google Scholar]
- Seo, J.H.; Kim, S.J.; Lee, M.; Kang, J.I. Impact of the COVID-19 pandemic on mental health service use among psychiatric outpatients in a tertiary hospital. J. Affect. Disord. 2021, 290, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lim, A.-R.; Kim, M.J.; Choi, Y.J.; Kim, J.W.; Park, K.H.; Shine, S.W.; Kim, Y.H. Innovative countermeasures can maintain cancer care continuity during the coronavirus disease-2019 pandemic in Korea. Eur. J. Cancer. 2020, 136, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Coronavirus Pandemic (COVID-19). Published Online at OurWorldInData.org. Available online: https://ourworldindata.org/coronavirus (accessed on 14 January 2022).
- Lee, M.; You, M. Avoidance of Healthcare Utilization in South Korea during the Coronavirus Disease 2019 (COVID-19) Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4363. [Google Scholar] [CrossRef] [PubMed]
- Mantica, G.; Riccardi, N.; Terrone, C.; Gratarola, A. Non-COVID-19 visits to emergency departments during the pandemic: The impact of fear. Public Health 2020, 183, 40–41. [Google Scholar] [CrossRef]
- Mailnews. “72.5% of the People Responded Positively to the Policy of “Participation in COVID-19 Testing and Treatment of Local Hospitals”. Available online: http://www.bosa.co.kr/news/articleView.html?idxno=2169759 (accessed on 1 May 2022).
- Osawa, I.; Goto, T.; Asami, Y.; Itoh, N.; Kaga, Y.; Yamamoto, Y.; Tsugawa, Y. Physician visits and medication prescriptions for major chronic diseases during the COVID-19 pandemic in Japan: Retrospective cohort study. BMJ Open 2021, 11, e050938. [Google Scholar] [CrossRef]
- Lee, D.E.; Ro, Y.S.; Ryoo, H.W.; Moon, S. Impact of temporary closures of emergency departments during the COVID-19 outbreak on clinical outcomes for emergency patients in a metropolitan area. Am. J. Emerg. Med. 2021, 47, 35–41. [Google Scholar] [CrossRef]
- Ahn, S.; Kim, S.; Koh, K. Changes in healthcare utilization, spending, and perceived health during COVID–19: A longitudinal study from Singapore. Soc. Sci. Res. Netw. 2020. [Google Scholar] [CrossRef]
- Mehrotra, A.; Chernew, M.; Linetsky, D.; Hatch, H.; Cutler, D. The Impact of the COVID-19 Pandemic on Outpatient Visits: Practices Are Adapting to the New Normal. The Commonwealth Fund 2020. Available online: https://www.commonwealthfund.org/publications/2020/jun/impact-covid-19-pandemic-outpatient-visits-practices-adapting-new-normal (accessed on 14 January 2022).
- Zhang, Y.N.; Chen, Y.; Wang, Y.; Li, F.; Pender, M.; Wang, N.; Yan, F.; Ying, X.H.; Tang, S.L.; Fu, C.W. Reduction in healthcare services during the COVID-19 pandemic in China. BMJ Glob. Health 2020, 5, e003421. [Google Scholar] [CrossRef]
- Choi, H.; Cho, W.; Kim, M.H.; Hur, J.Y. Public health emergency and crisis management: Case study of SARS-CoV-2 outbreak. Int. J. Environ. Res. Public Health 2020, 17, 3984. [Google Scholar] [CrossRef]
- Gonzalez, D.; Zuckerman, S.; Kenney, G.M.; Karpman, M. Almost Half of Adults in Families Losing Work during the Pandemic Avoided Health Care Because of Costs or COVID-19 Concerns; Urban Institute: Washington, DC, USA, 2020. [Google Scholar]
- Chen, H.; Zhang, K. Insight into the impact of the COVID-19 epidemic on tuberculosis burden in China. Eur. Respir. J. 2020, 56, 2002710. [Google Scholar] [CrossRef]
- Kwak, N.; Hwang, S.S.; Yim, J.J. Effect of COVID-19 on tuberculosis notification, South Korea. Emerg. Infect. Dis. 2020, 26, 2506–2508. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersen, E.S.; Faiz, K.W.; Sandset, E.C.; Storstein, A.M.; Stefansen, S.; Winsvold, B.; Hansen, J.M. Hospital-based headache care during the COVID-19 pandemic in Denmark and Norway. J. Headache Pain 2020, 21, 128. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.G.; Li, Y.; Shen, J.; Shao, M.M.; Lin, X.D.; Zhu, J.J.; Huang, X.Y.; Cheng, Z.C.; Yan, J.Y.; Chen, K.Y. Clinical activity changes in the neurology department of Wenzhou during the COVID-19 pandemic: An observational analysis. Neurol. Sci. 2021, 42, 1653–1659. [Google Scholar] [CrossRef]
- Yoo, B.S.; Lee, M.A.; Jang, B.S. A Study of Service Development for Long-Term Care Facility in the Post-COVID Era; Gyeonggi Welfare Foundation: Suwon-si, Korea, 2020. [Google Scholar]
- Huang, Y.; Zhao, N. Chinese mental health burden during the COVID-19 pandemic. Asian J. Psychiatry 2020, 54, 102052. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Health Insurance Review and Assessment Service (HIRA); National Health Insurance Service (NHIS). 2020 National Health Insurance Statistical Yearbook; HIRA & NHIS: Wonju, Korea, 2021. [Google Scholar]
- Lee, S.Y.; Khang, Y.H.; Lim, H.K. Impact of the 2015 Middle East respiratory syndrome outbreak on emergency care utilization and mortality in South Korea. Yonsei Med. J. 2019, 60, 796–803. [Google Scholar] [CrossRef]
- Lu, T.H.; Chou, Y.J.; Liou, C.S. Impact of SARS on healthcare utilization by disease categories: Implications for delivery of healthcare services. Health Policy 2007, 83, 375–381. [Google Scholar] [CrossRef]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilization of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef]
- Sorenson, C.; Japinga, M.; Crook, H.; McClellan, M. Building a better health care system post-COVID-19: Steps for reducing low-value and Wasteful care. NEJM Catal. Innov. Care Deliv. 2020, 1. [Google Scholar] [CrossRef]

{kind=link}
| Diseases | Actual Visits (Cases) | Expected Visits † (Cases) | Impact of the Pandemic in 2020 | ||
|---|---|---|---|---|---|
| Exp (B) | 95% Confidence Interval (Upper–Lower) | p-Value | |||
| All-cause | 658,504,435 | 773,530,267 | 0.88 | 0.83–0.93 | <0.0001 *** |
| Chronic diseases | 152,720,186 | 156,625,911 | 0.98 | 0.96–0.99 | 0.0074 ** |
| Months | All-Cause | Chronic Diseases | ||||||
|---|---|---|---|---|---|---|---|---|
| Actual Visits (per 1000 People) | Expected Visits (per 1000 People) | 95% CI * | Change † | Actual Visits (per 1000 People) | Expected Visits (per 1000 People) | 95% CI * | Change † | |
| January | 1263 | 1190 | 1235–1147 | △ | 245 | 238 | 244–233 | △ |
| February | 1028 | 1199 | 1244–1155 | ▼ | 230 | 245 | 251–240 | ▼ |
| March | 938 | 1296 | 1342–1252 | ▼ | 235 | 259 | 264–254 | ▼ |
| April | 955 | 1245 | 1334–1161 | ▼ | 237 | 242 | 248–236 | - |
| May | 1057 | 1230 | 1318–1147 | ▼ | 245 | 249 | 255–243 | - |
| June | 1109 | 1235 | 1296–1176 | ▼ | 255 | 257 | 263–252 | - |
| July | 1124 | 1245 | 1289–1203 | ▼ | 260 | 264 | 269–258 | - |
| August | 1023 | 1123 | 1169–1078 | ▼ | 241 | 242 | 247–237 | - |
| September | 1067 | 1279 | 1335–1225 | ▼ | 255 | 262 | 268–256 | ▼ |
| October | 1033 | 1208 | 1259–1158 | ▼ | 241 | 247 | 252–242 | ▼ |
| November | 1074 | 1253 | 1318–1191 | ▼ | 244 | 249 | 255–243 | - |
| December | 1032 | 1420 | 1491–1353 | ▼ | 258 | 267 | 273–261 | ▼ |
| Chronic Disease Groups | Actual Visits (Cases) | Expected Visits (Cases) | Impact of the Pandemic in 2020 | ||
|---|---|---|---|---|---|
| Exp (B) | 95% Confidence Interval (Upper–Lower) | p-Value | |||
| Hypertension | 47,155,146 | 46,907,780 | 1.01 | 0.99–1.02 | 0.4789 |
| Diabetes | 24,639,134 | 25,344,665 | 0.97 | 0.96–0.99 | 0.0014 ** |
| Mental and behavioral disorders | 26,958,894 | 28,071,403 | 0.96 | 0.94–0.98 | 0.0002 ** |
| Respiratory tuberculosis | 237,652 | 270,496 | 0.89 | 0.86–0.91 | <0.0001 *** |
| Heart disease | 6,436,864 | 6,752,433 | 0.96 | 0.93–0.98 | <0.0001 *** |
| Cerebral cardiovascular disease | 4,563,098 | 4,770,861 | 0.96 | 0.93–0.99 | 0.0050 |
| Neurological disease | 11,561,938 | 12,494,176 | 0.93 | 0.90–0.96 | <0.0001 *** |
| Malignant neoplasm | 12,179,249 | 12,474,396 | 0.98 | 0.96–1.00 | 0.0482 * |
| Thyroid disease | 5,160,853 | 5,381,911 | 0.96 | 0.93–0.99 | 0.0103 * |
| Liver disease | 5,182,999 | 5,513,492 | 0.94 | 0.90–0.97 | 0.0006 ** |
| Chronic renal failure | 8,644,359 | 8,575,289 | 1.01 | 0.99–1.02 | 0.2734 |
| Months | Changes † in Chronic Disease Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hypertension | Diabetes | Mental and Behavioral Disorders | Respiratory Tuberculosis | Heart Disease | Cerebral Cardiovascular Disease | Neurological Disease | Malignant Neoplasm | Thyroid Disease | Liver Disease | Chronic Renal Failure | |
| January | △ | △ | - | - | - | △ | △ | △ | - | - | △ |
| February | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | - |
| March | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ |
| April | - | ▼ | ▼ | ▼ | ▼ | - | ▼ | - | ▼ | - | - |
| May | - | - | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | - | - | - |
| June | - | - | ▼ | ▼ | - | - | ▼ | - | - | - | - |
| July | - | - | ▼ | ▼ | - | - | ▼ | - | - | ▼ | △ |
| August | △ | - | - | ▼ | - | - | ▼ | - | - | ▼ | - |
| September | - | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | - |
| October | - | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | - | - | ▼ | △ |
| November | - | ▼ | - | ▼ | ▼ | - | ▼ | - | - | - | - |
| December | - | ▼ | ▼ | ▼ | ▼ | ▼ | ▼ | - | ▼ | ▼ | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, B.; Nam, E.W. The Impact of COVID-19 Pandemic on Outpatient Visits for All-Cause and Chronic Diseases in Korea: A Nationwide Population-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 5674. https://doi.org/10.3390/ijerph19095674
Sim B, Nam EW. The Impact of COVID-19 Pandemic on Outpatient Visits for All-Cause and Chronic Diseases in Korea: A Nationwide Population-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5674. https://doi.org/10.3390/ijerph19095674
Chicago/Turabian StyleSim, Boram, and Eun Woo Nam. 2022. "The Impact of COVID-19 Pandemic on Outpatient Visits for All-Cause and Chronic Diseases in Korea: A Nationwide Population-Based Study" International Journal of Environmental Research and Public Health 19, no. 9: 5674. https://doi.org/10.3390/ijerph19095674