
Cholera Outbreaks in India, 2011–2020: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Data Sources
- (1)
- Population: any group of individuals affected by a cholera outbreak in India;
- (2)
- Exposure: a study had to assess sources of exposure or potential risk factors for an outbreak;
- (3)
- Comparison: it was not considered obligatory to include a comparison group for the present analysis;
- (4)
- Outcomes: we focused on transmission routes as well as human practices that lead to cholera, the sources of the cholera outbreak and other human factors that may explain the seasonality of cholera;
- (5)
- Study design: prevalence and incidence studies were eligible.
2.2. Data Extraction and Analysis
3. Results
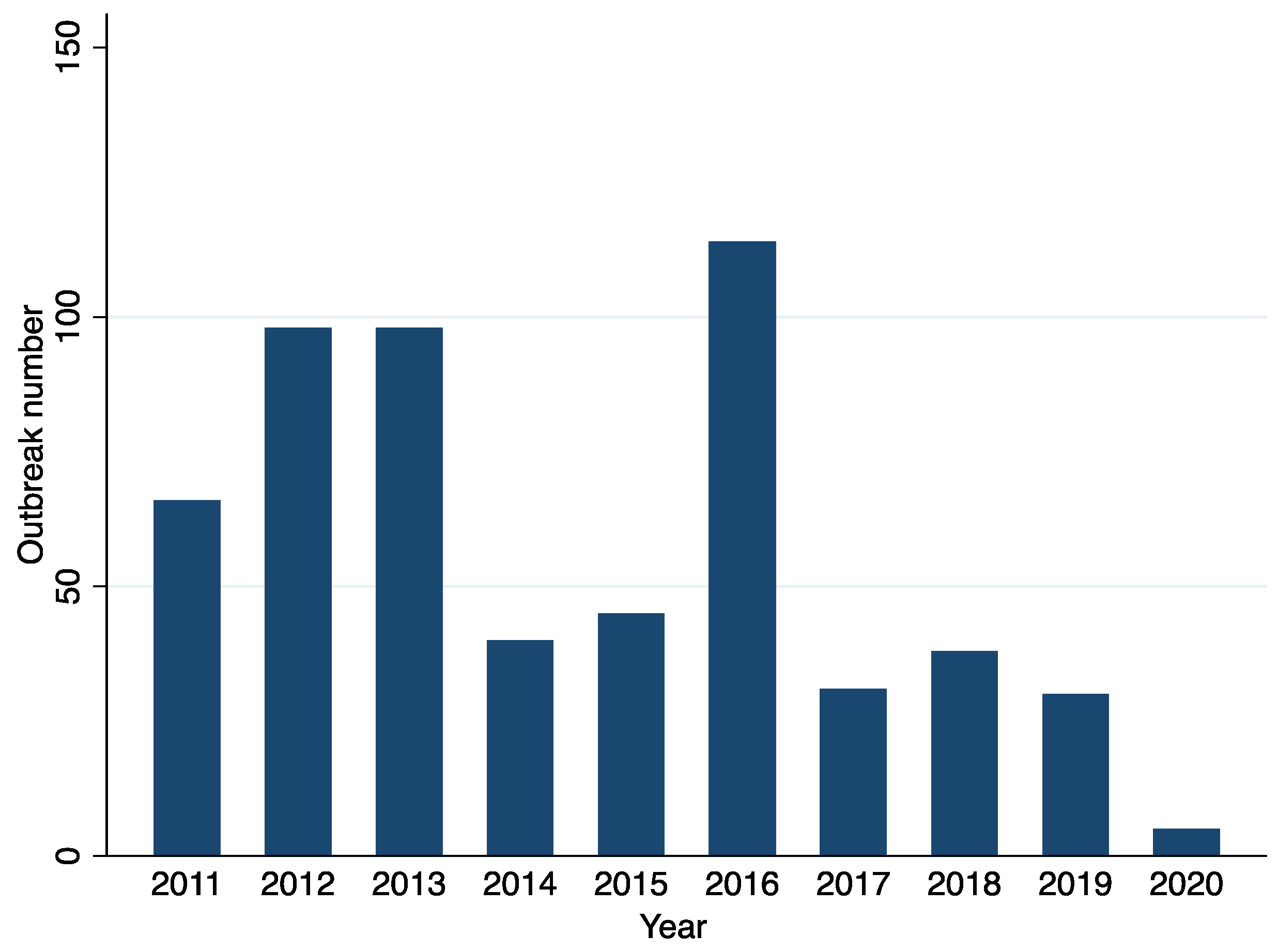
3.1. Study Characteristics
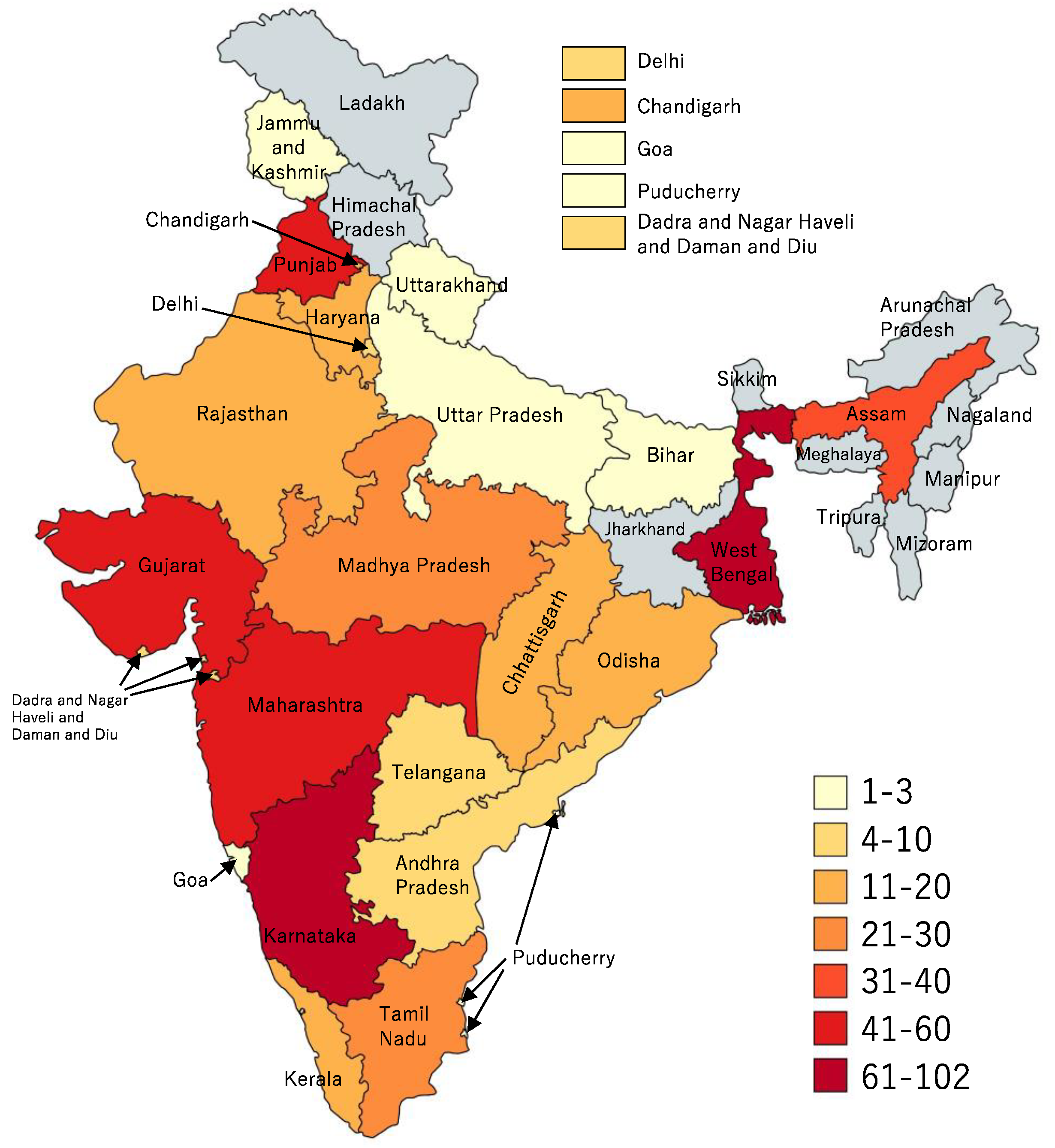
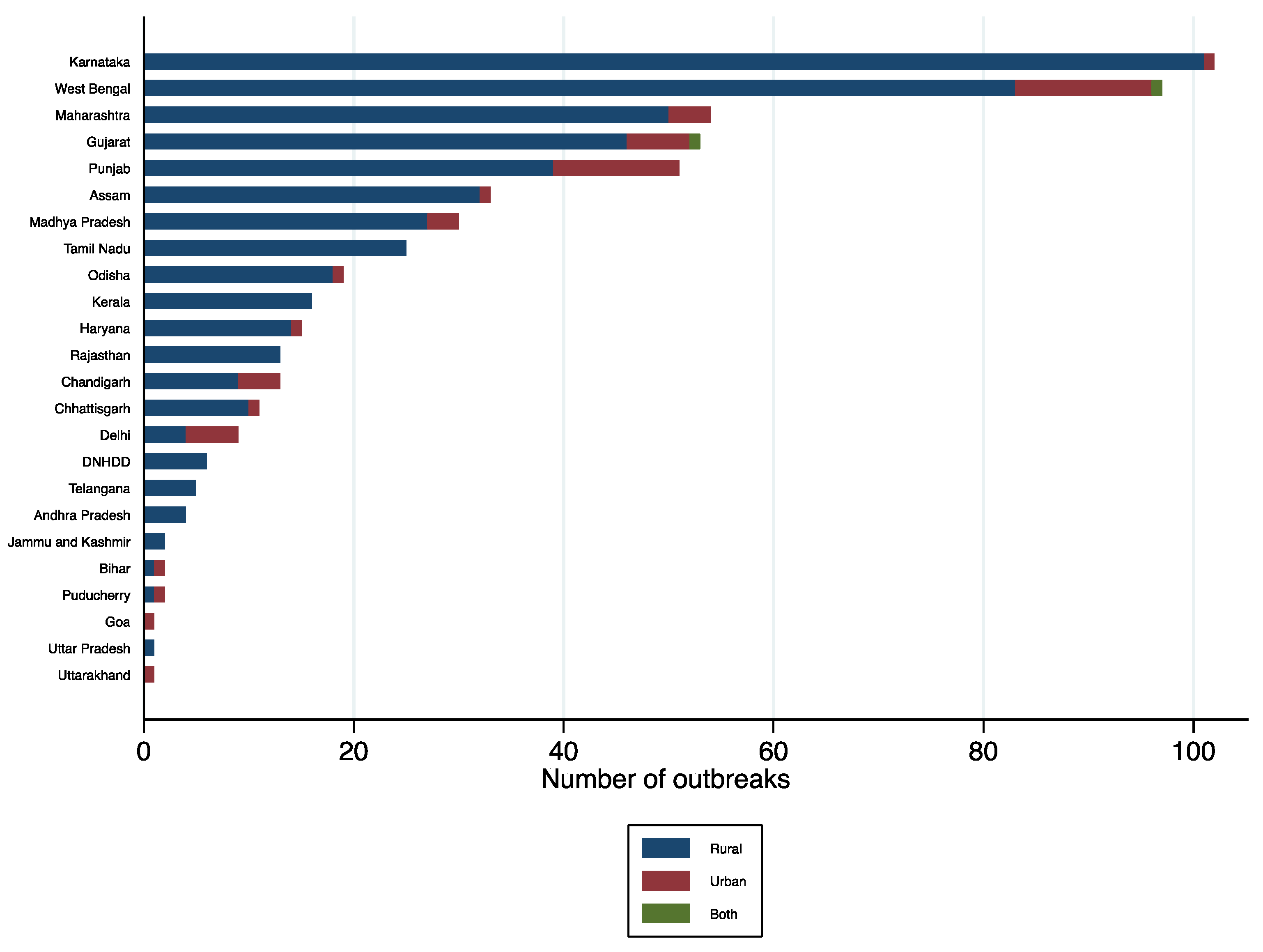
3.2. Geographical Distribution of Cholera Outbreaks
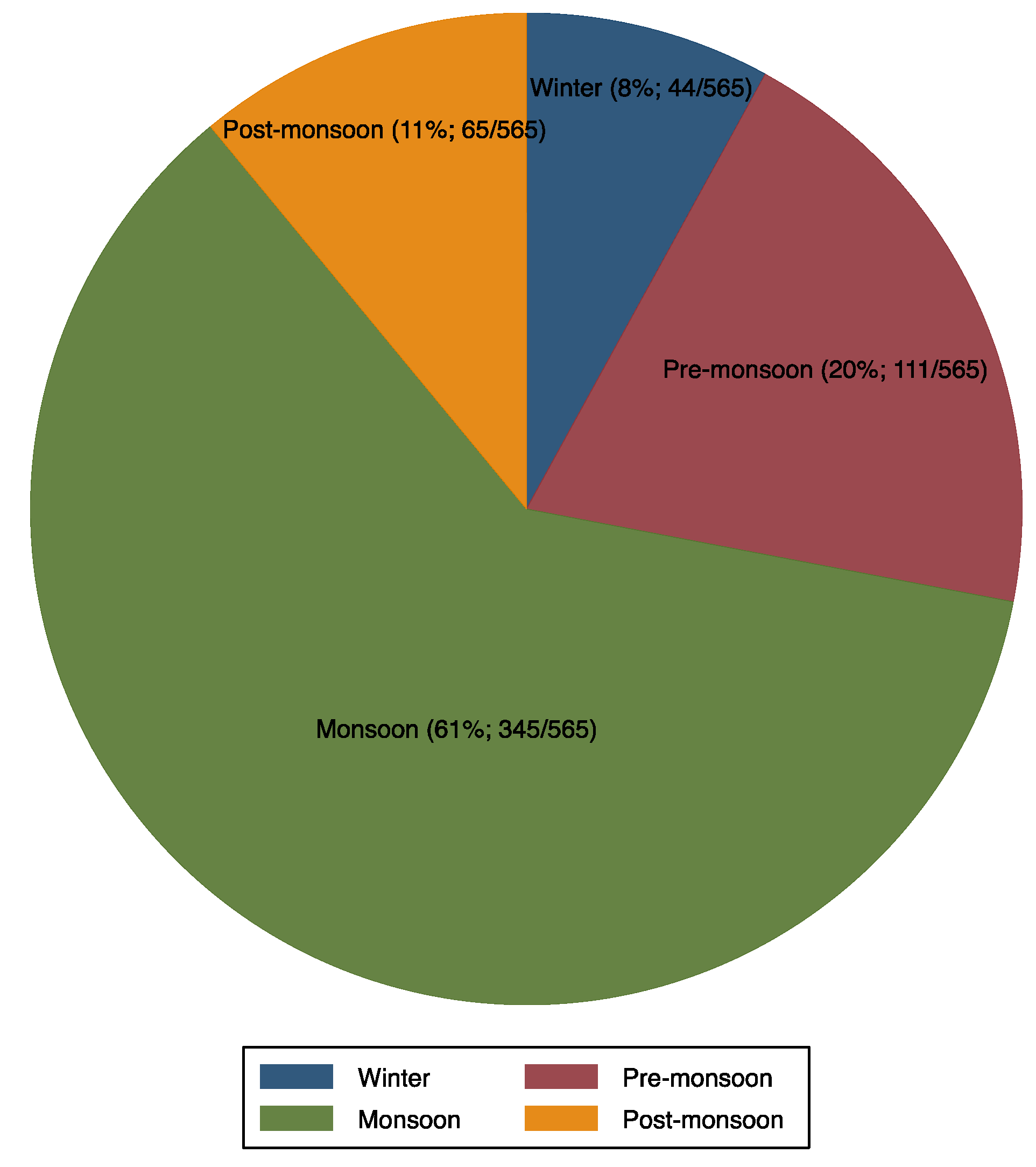
3.3. Seasonality
3.4. Transmission Routes and Source of Water Contamination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outbreak Number | References | Location | Urban/Rural Area | Study Design/Type | Study Period | Age (Year)/Descriptor | Outbreak Duration (Days) | Population at Risk | Number of Cholera Cases | Attack Rate (Case/100 Person) | Case Fatality Ratio (Number of Death) | Occurrence Month |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Dutta, 2021 [26] | Ghughri, Madhya Pradesh, Central | Rural | Cross-sectional | 2016 | 27 (1–76) | 30 | 101,115 | 628 | 0.6 | 2 (14/628) | August |
| 2 | Jain, 2021 [27] | Shahpur, Haryana, Northern | Rural | Cross-sectional | 2019 | 18 (1–65) | 29 | 2602 | 196 | 8 | 1 (2/196) | September |
| 3 | Kale, 2020 [28] | Yavatmal, Maharashtra, Western | Rural | Cross-sectional | 2018 | All | - | - | - | - | - | March–July |
| 4 and 5 | Nayak, 2020 [29] | Odisha, Eastern | Rural | Cross-sectional | 2018 | >5 | 4 | 1387 | 55 | 4.0 | 0 | August |
| 2019 | >5 | 5 | 500 | 73 | 14.6 | 1.4 | April | |||||
| 6 | Singh, 2020 [30] | Bhadola, Delhi, Northern | Urban | Case-control | 2018 | Median = 14.5 | 56–59 | 7280 | 129 | 1.8 | 0 | April-May |
| 7 | Mukhopadhyay, 2019 [31] | Kolkata and vicinity, West Bengal, Eastern | Urban | Cross-sectional | 2015 | Median = 26 | 15 | - | - | - | 1 death | August |
| 8 | Goswami, 2019 [32] | Wardha, Maharashta, Western | Urban | Cross-sectional | 2018 | 3–65 | 9 | 104 | 28 | 27 | 0 | July |
| 9 | Gopalkrishna, 2019 [33] | Aurangabad, Maharashta, Western | Urban | Cross-sectional | 2017 | >14 (90%) | 12 | 16,000 | 7447 | 47 | - | November |
| 10 | Pal, 2019 [34] | Odisha, Eastern | Rural | Cross-sectional | 2018 | All | - | - | - | - | 0 | May |
| 11 | Pal, 2017 [35] | Narla, Kalahandi, Odisha, Eastern | Urban | Cross-sectional | 2014 | >20 | 60 | 46,236 | 321 | 0.7 | 0.9 | July–September |
| 12 | Uthappa, 2015 [36] | Medipally, Telangana, Southern | Rural | Case-control | 2013 | All | 9 | – | 138 | 11.5 | 0.7(1 death) | November |
| 13 | Bhattacharya, 2015 [37] | Somanakoppa, Bagalkot, Karnataka, Southern | Rural | Cross-sectional | 2013 | - | 12 | – | 49 | 3.5 | – | August |
| 14 | Allam, 2015 [38] | Medak, Andhra Pradesh, Southern | Rural | Cross-sectional | 2013 | All (0–74) | 30 | 281 | 3.3 | 1.4 (3 deaths) | August | |
| 15 | Fredrick, 2015 [39] | Pondicherry, Puducherry, Southern | Urban | Case-control | 2012 | All | 13 | 8367 | 921 | 11 | 0.1 (1 death) | January |
| 16 | Biswas, 2014 [40] | Haibatpur, West Bengal, Eastern | Rural | Cross-sectional | 2012 | 33 (5 to 80) | 14 | 780 | 41 | 5 | 0 | June |
| 17 and 18 | Dey, 2014 [41] | Talikoti, Bijapur, Karnata, Southern | Semi-rural | Cross-sectional | 2012 | All | 20 | 26,205 | 101 | 0.4 | 0 | July–August |
| Harnal, Bijapur, Karnata, Southern | Rural | Cross-sectional | 2012 | All | 7 | 960 | 200 | 21 | 0 | July–August | ||
| 19 | Kumar, 2014 * [42] | Kalamb and Yavatmal, Maharashtra, Western | Urban | Cross-sectional | 2012 | - | - | - | - | - | 4.5 | May |
| 19 | Kumar, 2014 * [43] | Kalamb and Yavatmal, Maharashtra, Western | Urban | Cross-sectional | 2012 | - | - | - | - | - | - | May |
| 20 | Puri, 2014 [44] | Vikas Nagar, Chandigarh, Northern | Urban | Cross-sectional | 2012 | All | 14 | 15,000 | 1875 | 15 | (4 deaths) | July |
| 21 | Mahanta, 2013 [45] | Bagjan, Sivasagar, Assam, North-eastern | Rural | Cross-sectional | 2012 | 41 (3–70) | - | 2503 | 120 | 4.8 | 0.83 (1 death) | May |
| Study | Risk Factors Assessed | Men (%) | Women (%) | Population | Cholera Definition | Serogroup | Serotype/Biotype | Transmission Route/Suspected Exposure | Number Examined | Number of Infected Individuals | Prevalence (95% CI) | Comment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dutta, 2021 [26] | Water | 39 | 61 | Community | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water | 34 | 11 | 32 | More women were affected. |
| Jain, 2021 [27] | Water, Environment | 46 | 54 | Community | Clinical; Culture-confirmed | - | - | Contaminated drinking water | 18 | 4 | 22 | Attack rates were highest in the 11–20 years group |
| Kale, 2020 [28] | None | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water | 711 | 109 | 15 | Males and women were equally affected |
| Nayak, 2021 [29] | Water, Hygiene | - | - | - | Clinical; Culture-confirmed | Haitian variant of VC O1 | Ogawa biotype El Tor | Pond water used to cook foods and clean utensils at a local festival and marriage ceremony | 65 | 27 | 42 (30 to 54) | Children < 5 were not affected. More women were affected |
| Singh, 2020 [30] | Water, Hygiene, Knowledge on diarrhea transmission | 48 | 52 | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Drinking untreated municipal water | 129 | 6 | 5 (2 to 10) | - |
| Mukhopadhyay, 2019 [31] | Habitation | 56 | 44 | Hospital-based surveillance | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor and Inaba | Living near water channel and central lake channel. Contamination of drinking water sources due to overflowing of canals and drains during heavy rains | 204 | 63 | 31 (25 to 38) | Age range: 5 months to 99 years. No difference between men and women |
| Goswami, 2019 [32] | Habitation location, Water | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Hand pump; drinking water | 28 | 2 | 7 (2 to 23) | Most cases were children (0–10); More males were affected |
| Gopalkrishna, 2019 [33] | Water | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Fecal contamination of the river water and leakage in the pipeline | 46 | 6 | 13 (6 to 26) | - |
| Pal, 2019 [34] | Water | - | - | - | Clinical; Culture-confirmed | VC O139 | - | Heavy rain contaminated muddy water supply | 20 | 15 | 75 (53 to 89) | - |
| Pal, 2017 [35] | Water | - | - | - | - | - | Ogawa biotype, ctxB7 variant of Haitian VC | Contaminated drinking water source, unhygienic conditions in the house, unsafe disposal of fecal materials, cleaning of excrement-contaminated clothes in nearby water reservoirs, visiting choleric patients | 17 | 11 | 65 (41 to 83) | Prevalence high in children < 1 year |
| Allam, 2015 [38] | Water, Hygiene | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water | 10 | 1 | - | - |
| Bhattacharya, 2015 [37] | Water, hygiene | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water | 6 | 4 | - | - |
| Uthappa, 2015 [36] | Water, household size, hygiene, socio-demographics | 53 | 47 | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water source | - | 138 | - | Prevalence high in children ≤ 5 year |
| Fredrick, 2015 [39] | Water, Hygiene | 47 | 53 | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water | 16 | 9 | - | - |
| Biswas, 2014 [40] | Water, hygiene | 69 | 31 | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water source | - | 41 | - | - |
| Dey, 2014 [41] | Water, Hygiene | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water | 7 | 5 | - | All age-groups were affected |
| Kumar, 2014 [43] | Water, Environment | - | - | Hospital | - | VC O1 | Ogawa biotype El Tor | Contaminated drinking water source | - | 20 | - | Leakage in water pipes mixing water with drainage |
| Puri, 2014 [44] | Water, Environment, Food, Mass gathering | 53 | 47 | Hospital and community | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water source | - | 8 | - | - |
| Mahanta, 2013 [45] | Demographics, Socioeconomic, Environmental | - | - | - | Clinical; Culture-confirmed | VC O1 | Ogawa biotype El Tor | Contaminated drinking water source | 13 | 3 | 23 | - |
| Study | Aim Clearly Stated | Setting Provided | Study Design or Sampling Method Explained | Case Definition of Diarrhea or Cholera Clearly Mentioned | Statistical or Analysis Methods Reported | Risk Factors for Outbreak (or Causes of Outbreaks) Investigated | Case Fatality Ratio Reported | Performance of Confirmatory Test (Culture or PCR) | Limitations or Potential Confounders Discussed | Score | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dutta, 2021 [26] | Yes | Yes | No | Yes | Unclear | Yes | Yes | Yes | Yes | 7 | Moderate |
| Jain, 2021 [27] | Yes | Yes | No | Yes | Unclear | Yes | Yes | Yes | Yes | 7 | Moderate |
| Kale, 2020 [28] | Yes | Yes | No | No | No | Yes | Yes | Yes | No | 5 | Moderate |
| Nayak, 2020 [29] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | 7 | Moderate |
| Singh, 2020 [30] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 9 | Low |
| Mukhopadhyay, 2019 [31] | Yes | Yes | Yes | Yes | No | Yes | Yes | Unclear | No | 6 | Moderate |
| Goswami, 2019 [32] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | 7 | Moderate |
| Gopalkrishna, 2019 [33] | Yes | Yes | No | No | No | Yes | Yes | Yes | No | 5 | Moderate |
| Pal, 2019 [34] | Yes | Yes | No | No | No | Yes | Yes | Yes | No | 5 | Moderate |
| Pal, 2017 [35] | Yes | Yes | Yes | Yes | No | Yes | Yes | Unclear | No | 6 | Moderate |
| Uthappa, 2015 [36] | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | 9 | Low |
| Bhattacharya, 2015 [37] | Yes | Yes | Yes | No | No | Yes | No | Yes | Unclear | 5 | Moderate |
| Allam, 2015 [38] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 6 | Moderate |
| Fredrick, 2015 [39] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 9 | Low |
| Biswas, 2014 [40] | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | No | 8 | Low |
| Dey, 2014 [41] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | 7 | Moderate |
| Kumar, 2014 [42] | Yes | Yes | Yes | Unclear | No | Yes | No | Yes | Unclear | 5 | Moderate |
| Kumar, 2014 [43] | Yes | Yes | Yes | No | No | No | Yes | Yes | Unclear | 5 | Moderate |
| Puri, 2014 [44] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8 | Low |
| Mahanta, 2013 [45] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | 7 | Moderate |
References
- Ali, M.; Gupta, S.S.; Arora, N.; Khasnobis, P.; Venkatesh, S.; Sur, D.; Nair, G.B.; Sack, D.A.; Ganguly, N.K. Identification of burden hotspots and risk factors for cholera in India: An observational study. PLoS ONE 2017, 12, e0183100. [Google Scholar] [CrossRef] [Green Version]
- Lipp, E.K.; Huq, A.; Colwell, R.R. Effects of Global Climate on Infectious Disease: The Cholera Model. Clin. Microbiol. Rev. 2002, 15, 757–770. [Google Scholar] [CrossRef] [Green Version]
- Glass, R.I.; Svennerholm, A.-M.; Stoll, B.J.; Khan, M.R.; Hossain, K.M.B.; Hug, M.I.; Holmgren, J. Protection against Cholera in Breast-Fed Children by Antibodies in Breast Milk. N. Engl. J. Med. 1983, 308, 1389–1392. [Google Scholar] [CrossRef]
- Richterman, A.; Sainvilien, D.R.; Eberly, L.; Ivers, L.C. Individual and Household Risk Factors for Symptomatic Cholera Infection: A Systematic Review and Meta-analysis. J. Infect. Dis. 2018, 218, S154–S164. [Google Scholar] [CrossRef]
- Harris, J.B.; Khan, A.I.; LaRocque, R.C.; Dorer, D.J.; Chowdhury, F.; Faruque, A.S.G.; Sack, D.A.; Ryan, E.T.; Qadri, F.; Calderwood, S.B. Blood Group, Immunity, and Risk of Infection with Vibrio cholerae in an Area of Endemicity. Infect. Immun. 2005, 73, 7422–7427. [Google Scholar] [CrossRef] [Green Version]
- Glass, R.I.; Holmgren, J.; Haley, C.E.; Khan, M.R.; Svennerholm, A.; Stoll, B.J.; Hossain, K.M.B.; Black, R.E.; Yunus, M.; Barua, D. Predisposition for cholera of individuals with o blood group possible evolutionary significance. Am. J. Epidemiol. 1985, 121, 791–796. [Google Scholar] [CrossRef]
- Legros, D. Partners of the Global Task Force on Cholera Control Global Cholera Epidemiology: Opportunities to Reduce the Burden of Cholera by 2030. J. Infect. Dis. 2018, 218, S137–S140. [Google Scholar] [CrossRef]
- Kanungo, S.; Sah, B.K.; Lopez, A.L.; Sung, J.S.; Paisley, A.M.; Sur, D.; Clemens, J.D.; Nair, G.B. Cholera in India: An analysis of reports, 1997–2006. Bull. World Health Organ. 2010, 88, 185–191. [Google Scholar] [CrossRef]
- Chatterjee, P.; Kanungo, S.; Bhattacharya, S.K.; Dutta, S. Mapping cholera outbreaks and antibiotic resistant Vibrio cholerae in India: An assessment of existing data and a scoping review of the literature. Vaccine 2020, 38 (Suppl. S1), A93–A104. [Google Scholar] [CrossRef]
- Gupta, S.S.; Gupta, S.K. Social mobilization for cholera prevention & control in India: Building on the existing framework. Vaccine 2020, 38 (Suppl. S1), A181–A183. [Google Scholar] [CrossRef]
- Nayyar, A.; Privor-Dumm, L. Cholera control and prevention: Role of evidence-based advocacy and communications. Vaccine 2020, 38, A178–A180. [Google Scholar] [CrossRef]
- Taneja, N.; Mishra, A.; Batra, N.; Gupta, P.; Mahindroo, J.; Mohan, B. Inland cholera in freshwater environs of north India. Vaccine 2020, 38 (Suppl. S1), A63–A72. [Google Scholar] [CrossRef]
- Koelle, K.; Rodo, X.; Pascual, M.; Yunus, M.; Mostafa, G. Refractory periods and climate forcing in cholera dynamics. Nature 2005, 436, 696–700. [Google Scholar] [CrossRef]
- Pal, B.B.; Nayak, S.R.; Khuntia, H.K. Epidemiology and Antibiogram Profile of Vibrio cholerae Isolates between 2004–2013 from Odisha, India. Jpn. J. Infect. Dis. 2018, 71, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, A.; Kang, G. Pathways to a policy for cholera control in India. Vaccine 2020, 38 (Suppl. S1), A157–A159. [Google Scholar] [CrossRef]
- World Health Organization (WHO) and Unicef. Progress on Sanitation and Drinking Water: 2015 Update and MDG Assessment; World Health Organization: Geneva, Switzerland, 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/177752/9789241509145_eng.pdf?sequence=1&isAllowed=y (accessed on 23 June 2021).
- Coffey, D.; Spears, D.; Vyas, S. Switching to sanitation: Understanding latrine adoption in a representative panel of rural Indian households. Soc. Sci. Med. 2017, 188, 41–50. [Google Scholar] [CrossRef]
- Ramamurthy, T.; Sharma, N.C. Cholera Outbreaks in India. Tuberculosis 2014, 379, 49–85. [Google Scholar] [CrossRef]
- Panda, S.; Chatterjee, P.; Deb, A.; Kanungo, S.; Dutta, S. Preventing cholera in India: Synthesizing evidences through a systematic review for policy discussion on the use of oral cholera vaccine. Vaccine 2020, 38 (Suppl. S1), A148–A156. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Global Task Force on Cholera Control (GTFCC) Working Group on Surveillance. Surveillance & Global Monitoring Sub-Group and Outbreak Sub-Group. Available online: https://www.gtfcc.org/wp-content/uploads/2021/04/5th-meeting-of-the-gtfcc-working-group-on-surveillance-webinars-2021-report.pdf (accessed on 3 June 2021).
- National Centre for Disease Control. Integrated Disease Surveillance Programme. Dir Gen Heal Serv Minist Heal Fam Welfare, Gov India. Available online: https://www.idsp.nic.in (accessed on 20 March 2021).
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- MapChart. Available online: https://mapchart.net (accessed on 31 May 2021).
- Central Bureau of Health Intelligence (CBHI). Government of India, National Health Profile. 2019. Available online: http://www.cbhidghs.nic.in/showfile.php?lid=1147 (accessed on 25 March 2021).
- Dutta, B.P.; Kumar, N.; Meshram, K.; Yadav, R.; Sodha, S.V.; Gupta, S. Cholera outbreak associated with contaminated water sources in paddy fields, Mandla District, Madhya Pradesh, India. Indian J. Public Health 2021, 65, 46–50. [Google Scholar] [CrossRef]
- Jain, A.; Choudhary, S.; Saroha, E.; Bhatnagar, P.; Harvey, P. Cholera outbreak in an informal settlement at Shahpur huts, Panchkula District, Haryana State, India, 2019. Indian J. Public Health 2021, 65, S51–S54. [Google Scholar] [CrossRef]
- Kale, S.S.; Bulle, P.A.; Deshmukh, D.G.; Tankhiwale, S.S.; Gujar, V.M. An outbreak of diarrhoeal disease of El Tor Vibrio cholerae O1 Ogawa in and around Yavatmal district, Maharashtra, India in 2018. Int. J. Community Med. Public Health 2020, 7, 1297. [Google Scholar] [CrossRef]
- Nayak, S.R.; Nayak, A.K.; Biswal, B.L.; Pati, S.; Pal, B.B. Spread of Haitian Variant Vibrio cholerae O1 Causing Cholera Outbreaks in Odisha, India. Jpn. J. Infect. Dis. 2021, 74, 137–143. [Google Scholar] [CrossRef]
- Singh, A.; Gupta, R.; Dikid, T.; Saroha, E.; Sharma, N.C.; Sagar, S.; Gupta, S.; Bindra, S.; Khasnobis, P.; Jain, S.K.; et al. Cholera outbreak investigation, Bhadola, Delhi, India, April–May 2018. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 762–769. [Google Scholar] [CrossRef]
- Mukhopadhyay, A.K.; Deb, A.K.; Chowdhury, G.; Debnath, F.; Samanta, P.; Saha, R.N.; Manna, B.; Bhattacharya, M.K.; Datta, D.; Okamoto, K.; et al. Post-monsoon waterlogging-associated upsurge of cholera cases in and around Kolkata metropolis, 2015. Epidemiol. Infect. 2019, 147, e167. [Google Scholar] [CrossRef] [Green Version]
- Goswami, S.; Jha, A.; Sivan, S.P.; Dambhare, D.; Gupta, S.S. Outbreak investigation of cholera outbreak in a slum area of urban Wardha, India: An interventional epidemiological study. J. Fam. Med. Prim. Care 2019, 8, 1112–1116. [Google Scholar] [CrossRef]
- Gopalkrishna, V.; Joshi, M.; Viswanathan, R.; Malu, G.; Ganorkar, N.; Chavan, N.; Shinde, M.; Kumar, A.; Dhurandhare, S. Cholera outbreak in Aurangabad, Maharashtra, western India. Indian J. Med. Res. 2019, 150, 640–643. [Google Scholar] [CrossRef]
- Pal, B.B.; Mohanty, A.; Biswal, B.; Nayak, S.R. New Variant of Vibrio cholerae O139 in Odisha, India. J. Clin. Microbiol. 2019, 57, e01877-18. [Google Scholar] [CrossRef] [Green Version]
- Pal, B.B.; Khuntia, H.K.; Nayak, S.R.; Mohanty, A.; Biswal, B. Vibrio cholerae O1 Ogawa Strains Carrying the ctxB7 Allele Caused a Large Cholera Outbreak during 2014 in the Tribal Areas of Odisha, India. Jpn. J. Infect. Dis. 2017, 70, 549–553. [Google Scholar] [CrossRef] [Green Version]
- Uthappa, C.K.; Allam, R.R.; Nalini, C.; Gunti, D.; Udaragudi, P.R.; Tadi, G.P.; Murhekar, M.V. An outbreak of cholera in Medipally village, Andhra Pradesh, India, 2013. J. Health Popul. Nutr. 2015, 33, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharya, D.; Dey, S.; Roy, S.; Parande, M.V.; Telsang, M.; Seema, M.H.; Parande, A.V.; Mantur, B.G. Multidrug-Resistant Vibrio cholerae O1 was Responsible for a Cholera Outbreak in 2013 in Bagalkot, North Karnataka. Jpn. J. Infect. Dis 2015, 68, 347–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allam, R.R.; Uthappa, C.K.; Nalini, C.; Udaragudi, P.R.; Tadi, G.P.; Murhekar, M.V. An Outbreak of Cholera due to Contaminated Water, Medak District, Andhra Pradesh, India, 2013. Indian J. Community Med. 2015, 40, 283–285. [Google Scholar] [CrossRef]
- Fredrick, T.; Ponnaiah, M.; Murhekar, M.V.; Jayaraman, Y.; David, J.K.; Vadivoo, S.; Joshua, V. Cholera outbreak linked with lack of safe water supply following a tropical cyclone in Pondicherry, India, 2012. J. Health Popul. Nutr. 2015, 33, 31–38. [Google Scholar] [PubMed]
- Biswas, D.K.; Bhunia, R.; Maji, D.; Das, P. Contaminated pond water favors cholera outbreak at haibatpur village, purba medinipur district, west bengal, India. J. Trop. Med. 2014, 2014, 764530. [Google Scholar] [CrossRef]
- Dey, S.; Parande, M.V.; Parande, A.M.; Lakkannavar, S.L.; Rathore, P.K.; Mantur, B.G.; Kholkute, S.D.; Roy, S. Twin outbreak of cholera in rural North Karnataka, India. Indian J. Med. Res. 2014, 140, 420–426. [Google Scholar] [PubMed]
- Kumar, P.; Mishra, D.K.; Deshmukh, D.G.; Jain, M.; Zade, A.M.; Ingole, K.V.; Yadava, P.K. Haitian variant ctxB producing Vibrio cholerae O1 with reduced susceptibility to ciprofloxacin is persistent in Yavatmal, Maharashtra, India, after causing a cholera outbreak. Clin. Microbiol. Infect. 2014, 20, O292–O293. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P.; Mishra, D.K.; Deshmukh, D.G.; Jain, M.; Zade, A.M.; Ingole, K.V.; Goel, A.K.; Yadava, P.K. Vibrio cholerae O1 Ogawa El Tor strains with the ctxB7 allele driving cholera outbreaks in south-western India in 2012. Infect. Genet. Evol. 2014, 25, 93–96. [Google Scholar] [CrossRef]
- Puri, S.; Sarpal, S.; Kumar, A.; Goel, N. An outbreak of Vibrio cholerae in Vikas Nagar, Chandigarh, India. Med. J. DY Patil. Univ. 2014, 7, 147–151. [Google Scholar]
- Mahanta, B.N.; Mahanta, T.G.; Sinha, R.; Dutta, A.; Payeng, D.; Jawed, Q. Investigation of a cholera outbreak in a tea garden of sivasagar district of assam. Indian J. Community Med. 2013, 38, 240–243. [Google Scholar] [CrossRef]
- Haque, F.; Hossain, M.J.; Kundu, S.K.; Naser, A.M.; Rahman, M.; Luby, S.P. Cholera Outbreaks in Urban Bangladesh in 2011. Epidemiology 2013, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Dongdem, A.Z.; Opare, D.; Cottavoz, P.; Fookes, M.; Sadji, A.Y.; Dzotsi, E.; Dogbe, M.; Jeddi, F.; Bidjada, B.; et al. Dynamics of cholera epidemics from Benin to Mauritania. PLoS Negl. Trop. Dis. 2018, 12, e0006379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francois, J. Cholera remains a public health threat in Haiti. Lancet Glob. Health 2020, 8, e984. [Google Scholar] [CrossRef]
- Sack, D.A.; Debes, A.K.; Ateudjieu, J.; Bwire, G.; Ali, M.; Ngwa, M.C.; Mwaba, J.; Chilengi, R.; Orach, C.C.; Boru, W.; et al. Contrasting Epidemiology of Cholera in Bangladesh and Africa. J. Infect. Dis 2021, 224, S701–S709. [Google Scholar] [CrossRef] [PubMed]
- Chowdary, J.S.; Srinivas, G.; Du, Y.; Gopinath, K.; Gnanaseelan, C.; Parekh, A.; Singh, P. Month-to-month variability of Indian summer monsoon rainfall in 2016: Role of the Indo-Pacific climatic conditions. Clim. Dyn. 2019, 52, 1157–1171. [Google Scholar] [CrossRef]
- Palit, A.; Batabyal, P.; Kanungo, S.; Sur, D. In-house contamination of potable water in urban slum of Kolkata, India: A possible transmission route of diarrhea. Water Sci. Technol. 2012, 66, 299–303. [Google Scholar] [CrossRef]
- Ziegelbauer, K.; Speich, B.; Mausezahl, D.; Bos, R.; Keiser, J.; Utzinger, J. Effect of sanitation on soil-transmitted helminth infection: Systematic review and meta-analysis. PLoS Med. 2012, 9, e1001162. [Google Scholar] [CrossRef] [Green Version]
- Oguttu, D.W.; Okullo, A.; Bwire, G.; Nsubuga, P.; Ario, A.R. Cholera outbreak caused by drinking lake water contaminated with human faeces in Kaiso Village, Hoima District, Western Uganda, October 2015. Infect. Dis. Poverty 2017, 6, 146. [Google Scholar] [CrossRef] [Green Version]
- Eurien, D.; Mirembe, B.B.; Musewa, A.; Kisaakye, E.; Kwesiga, B.; Ogole, F.; Ayen, D.O.; Kadobera, D.; Bulage, L.; Ario, A.R.; et al. Cholera outbreak caused by drinking unprotected well water contaminated with faeces from an open storm water drainage: Kampala City, Uganda, January 2019. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Sur, D.; Deen, J.L.; Manna, B.; Niyogi, S.K.; Deb, A.K.; Kanungo, S.; Sarkar, B.L.; Kim, D.R.; Danovaro-Holliday, M.C.; Holliday, K.; et al. The burden of cholera in the slums of Kolkata, India: Data from a prospective, community based study. Arch. Dis. Child 2005, 90, 1175–1181. [Google Scholar] [CrossRef]
- Das, A.; Manickam, P.; Hutin, Y.; Pattanaik, B.; Pal, B.B.; Chhotray, G.P.; Kar, S.K.; Gupte, M.D. Two sequential outbreaks in two villages illustrate the various modes of transmission of cholera. Epidemiol. Infect. 2009, 137, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Khuntia, H.K.; Pal, B.B.; Meher, P.K.; Chhotray, G.P. Environmental Vibrio cholerae O139 may be the progenitor of outbreak of cholera in coastal area of Orissa, eastern India, 2000: Molecular evidence. Am. J. Trop Med. Hyg. 2008, 78, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Pati, K.K.; Bhattacharya, M.K.; Koley, H.; Pahari, S.; Nair, G.B. Rapid situation & response assessment of diarrhoea outbreak in a coastal district following tropical cyclone AILA in India. Indian J. Med. Res. 2011, 133, 395–400. [Google Scholar] [PubMed]
- Gallandat, K.; Huang, A.; Rayner, J.; String, G.; Lantagne, D.S. Household spraying in cholera outbreaks: Insights from three exploratory, mixed-methods field effectiveness evaluations. PLoS Negl. Trop. Dis. 2020, 14, e0008661. [Google Scholar] [CrossRef] [PubMed]
- Swaddiwudhipong, W.; Hannarong, S.; Peanumlom, P.; Pittayawonganon, C.; Sitthi, W. Two consecutive outbreaks of food-borne cholera associated with consumption of chicken rice in northwestern Thailand. Southeast Asian J. Trop. Med. Public Health 2012, 43, 927–932. [Google Scholar] [PubMed]
- Wong, C.S.; Ang, L.W.; James, L.; Goh, K.T. Epidemiological Characteristics of Cholera in Singapore, 1992–2007. Ann. Acad. Med. Singap. 2010, 39, 507–512. [Google Scholar]
- Shroff, B.D.; Mazumdar, V. Investigation of a cholera outbreak in Kanpur village of Panchmahal, Gujarat. Natl. J. Commun. Med. 2011, 2, 371–373. [Google Scholar]







| Study | Number of Stool Samples Examined | Number of Positive Samples | Detection Rate, % (95% CI) | Weight (%) |
|---|---|---|---|---|
| Dutta, 2021 [26] | 34 | 11 | 32 (19 to 50) | 7.7 |
| Jain, 2021 [27] | 18 | 4 | 22 (9 to 47) | 6.4 |
| Kale, 2020 [28] | 711 | 109 | 15 (13 to 18) | 8.9 |
| Nayak, 2020 [29] | 65 | 27 | 42 (30 to 54) | 8.4 |
| Singh, 2020 [30] | 129 | 6 | 5 (2 to 10) | 7.4 |
| Mukhopadhyay, 2019 [31] | 204 | 63 | 31 (25 to 38) | 8.8 |
| Goswami, 2019 [32] | 28 | 2 | 7 (2 to 25) | 5.4 |
| Gopalkrishna, 2019 [33] | 46 | 6 | 13 (6 to 26) | 7.3 |
| Pal, 2019 [34] | 20 | 15 | 75 (53 to 89) | 6.8 |
| Pal, 2017 [35] | 17 | 11 | 65 (40 to 83) | 6.8 |
| Allam, 2015 [38] | 10 | 1 | 10 (1 to 47) | 3.8 |
| Bhattacharya, 2015 [37] | 6 | 4 | 67 (3 to 92) | 4.7 |
| Fredrick, 2015 [39] | 16 | 9 | 56 (32 to 78) | 6.9 |
| Dey, 2014 [41] | 7 | 5 | 71 (33 to 93) | 4.8 |
| Mahanta, 2013 [45] | 13 | 3 | 23 (8 to 52) | 5.9 |
| Total (random effects) | 1324 | 276 | 32 (23 to 44) | 100.0 |
| Transmission Routes | Number of Outbreaks during 2011–2015, n (%) | Number of Outbreaks during 2016–2020, n (%) | Median (Min-Max) Annual Outbreaks Number during 2011–2015 versus 2016–2020 | p Value * |
|---|---|---|---|---|
| Unimproved water sources/Non-potable water/Contaminated drinking water | 127 (36.6) | 114 (52.3) | 21 (14–43) vs. 12 (3–75) | 0.058 |
| Water pipeline leaks | 67 (19.3) | 11 (5.0) | 8 (6–26) vs. 4 (2–5) | 0.028 ** |
| Open defecation | 14 (4.0) | 1 (0.5) | 4 (1–6) vs. 1 (1–1) | 0.361 |
| Poor sanitation | 6 (1.7) | 1 (0.5) | 1 (1–4) vs. 1 (1–1) | 0.505 |
| Waterborne combined with inadequate sanitation and poor hygiene | 2 (0.6) | 2 (0.9) | 1 (1–1) vs. 1 (1–1) | - |
| Foodborne/gathering/close contact | 5 (1.4) | 1 (0.5) | 2 (1–2) vs. 1 (1–1) | 0.248 |
| Not reported or unknown | 126 (36.3) | 88 (40.4) | 16 (11–45) vs. 16 (2–37) | 1.000 |
| Total | 347 (100.0) | 218 (100) | 66 (40–98) vs. 31 (5–114) | 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muzembo, B.A.; Kitahara, K.; Debnath, A.; Ohno, A.; Okamoto, K.; Miyoshi, S.-I. Cholera Outbreaks in India, 2011–2020: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5738. https://doi.org/10.3390/ijerph19095738
Muzembo BA, Kitahara K, Debnath A, Ohno A, Okamoto K, Miyoshi S-I. Cholera Outbreaks in India, 2011–2020: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(9):5738. https://doi.org/10.3390/ijerph19095738
Chicago/Turabian StyleMuzembo, Basilua Andre, Kei Kitahara, Anusuya Debnath, Ayumu Ohno, Keinosuke Okamoto, and Shin-Ichi Miyoshi. 2022. "Cholera Outbreaks in India, 2011–2020: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 9: 5738. https://doi.org/10.3390/ijerph19095738