
Accelerometer-Measured Physical Activity, Inactivity, and Related Factors in Family Caregivers of Patients with Terminal Cancer
 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Data Collection
2.3.1. Sociodemographic Factors
2.3.2. Physical Activity and Inactivity Measured by Accelerometry
2.3.3. Assessment of Caregiver’s Quality of Life
2.3.4. Assessment of Caregiver Strain
2.3.5. Ethical Considerations
2.3.6. Data Analysis
3. Results
3.1. Characteristics of the Caregivers
3.2. Descriptive Information on the Study Variables
3.3. Bivariate Results
- -
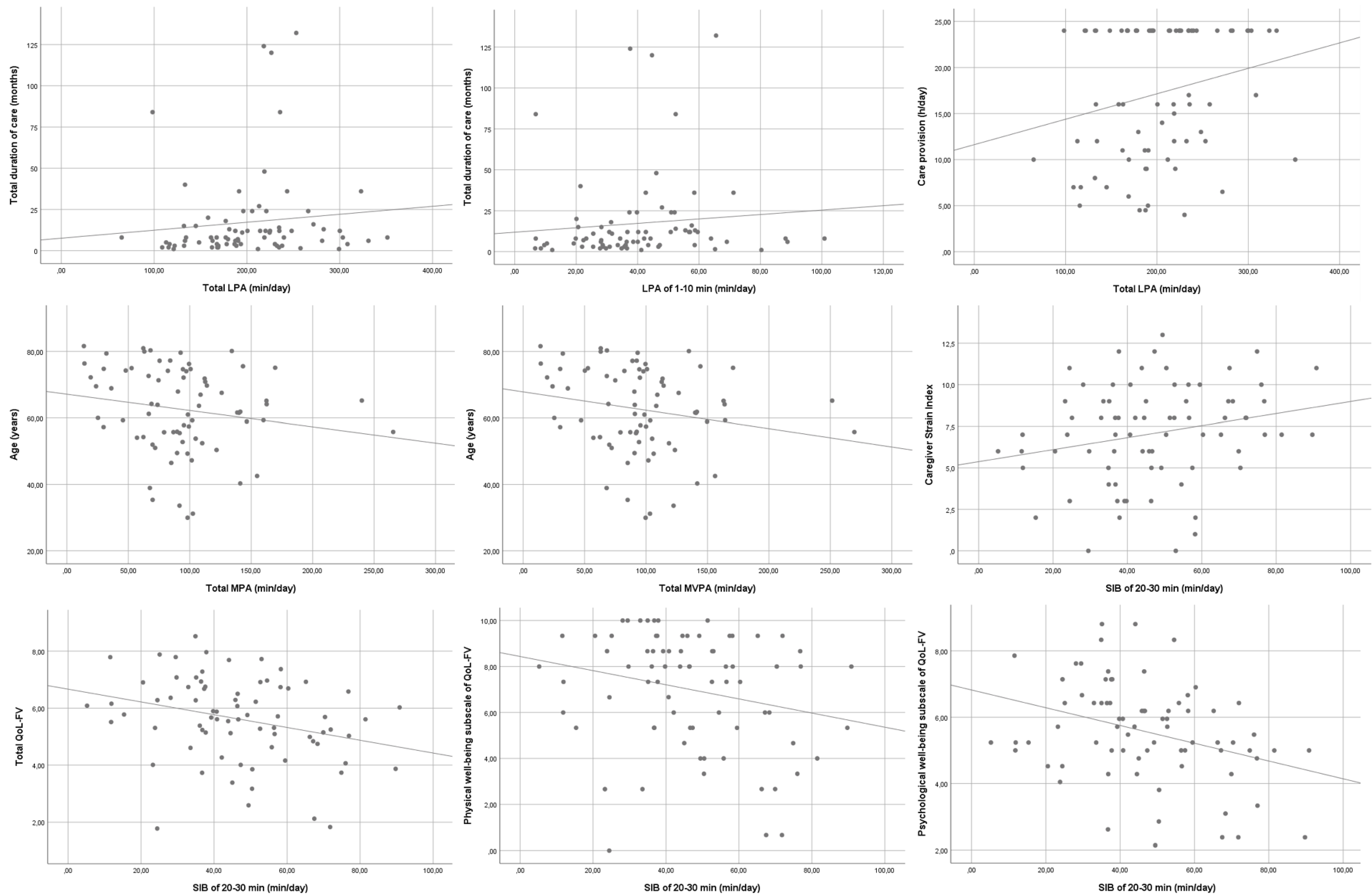
- The total duration of care is associated with a greater total LPA (r = 0.231, p = 0.046 *) and with an LPA of 1–10 min (r = 0.259, p = 0.025 *).
- -
- Care provision per day is associated with greater total LPA (r = 0.230, p = 0.047 *).
- -
- Caregiver age is associated with lower total VPA (r = −0.236, p = 0.041 *) and total MVPA (r = −0.237, p = 0.042 *).
- -
- CSI is positively associated with an SIB of 20–30 min (r= 0.232, p = 0.046 *).
- -
- Total QoL-FV is associated with an SIB of 20–30 min (r = −0.322, p = 0.005 *).
- -
- A physical well-being subscale of QoL-FV is associated with an SIB of 20–30 min (r= −0.261, p = 0.024 *).
- -
- A psychological well-being subscale of QoL-FV is associated with an SIB of 20–30 min (r= −0.327, p = 0.04 *).
- -
- Compliance with the WHO recommendation of MVPA ≥150 min/week is associated with total QoL-FV (r = −0.269, p = 0.020 *).
- -
- Moreover, mean nocturnal sleep is 359.11 min (SD, 46.60) for men and 400.18 (SD, 67.11) minutes for women (p = 0.042 *).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valero-Cantero, I.; Wärnberg, J.; Carrión-Velasco, Y.; Martínez-Valero, F.J.; Casals, C.; Vázquez-Sánchez, M.Á. Predictors of sleep disturbances in caregivers of patients with advanced cancer receiving home palliative care: A descriptive cross-sectional study. Eur. J. Oncol. Nurs. 2021, 51, 101907. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.C.; Hsieh, Y.L.; Lin, P.C.; Lin, Y.P. Sleep Pattern and Predictors of Sleep Disturbance Among Family Caregivers of Terminal Ill Patients with Cancer in Taiwan: A Longitudinal Study. Am. J. Hosp. Palliat. Care 2018, 35, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Sonza, A.; da Cunha de Sá-Caputo, D.; Sartorio, A.; Tamini, S.; Seixas, A.; Sanudo, B.; Süßenbach, J.; Provenza, M.M.; Xavier, V.L.; Taiar, R.; et al. COVID-19 Lockdown and the Behavior Change on Physical Exercise, Pain and Psychological Well-Being: An International Multicentric Study. Int. J. Environ. Res. Public Health 2021, 18, 3810. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 10 February 2022).
- Darragh, A.R.; Sommerich, C.M.; Lavender, S.A.; Tanner, K.J.; Vogel, K.; Campo, M. Musculoskeletal Discomfort, Physical Demand, and Caregiving Activities in Informal Caregivers. J. Appl. Gerontol. 2015, 34, 734–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, N.P.; Pedreira, L.C.; Nunes, S.F.L.; Alvarez, A.M.; Siewert, J.S.; Oliveira, L.M.S. Musculoskeletal disorders of older adults: An integrative literature review. Rev. Bras. Enferm. 2021, 74, e20200626. [Google Scholar] [CrossRef]
- Fagerström, C.; Elmståhl, S.; Wranker, L.S. Analyzing the situation of older family caregivers with a focus on health-related quality of life and pain: A cross-sectional cohort study. Health Qual. Life Outcomes 2020, 18, 79. [Google Scholar] [CrossRef] [Green Version]
- Beesley, V.L.; Price, M.A.; Webb, P.M.; Australian Ovarian Cancer Study Group, Australian Ovarian Cancer Study—Quality of Life Study Investigators. Loss of lifestyle: Health behaviour and weight changes after becoming a caregiver of a family member diagnosed with ovarian cancer. Support Care Cancer 2011, 19, 1949–1956. [Google Scholar] [CrossRef]
- Govina, O.; Vlachou, E.; Kalemikerakis, I.; Papageorgiou, D.; Kavga, A.; Konstantinidis, T. Factors Associated with Anxiety and Depression among Family Caregivers of Patients Undergoing Palliative Radiotherapy. Asia Pac. J. Oncol. Nurs. 2019, 6, 283–291. [Google Scholar] [CrossRef]
- Cai, Y.; Simons, A.; Toland, S.; Zhang, J.; Zheng, K. Informal caregivers’ quality of life and management strategies following the transformation of their cancer caregiving role: A qualitative systematic review. Int. J. Nurs. Sci. 2021, 8, 227–236. [Google Scholar] [CrossRef]
- Perpiñá-Galvañ, J.; Orts-Beneito, N.; Fernández-Alcántara, M.; García-Sanjuán, S.; García-Caro, M.P.; Cabañero-Martínez, M.J. Level of Burden and Health-Related Quality of Life in Caregivers of Palliative Care Patients. Int. J. Env. Res. Public Health 2019, 16, 4806. [Google Scholar] [CrossRef]
- Valero-Cantero, I.; Casals, C.; Carrión-Velasco, Y.; Barón-López, F.J.; Martínez-Valero, F.J.; Vázquez-Sánchez, M.Á. The influence of symptom severity of palliative care patients on their family caregivers. BMC Palliat. Care 2022, 21, 27. [Google Scholar] [CrossRef]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Bennie, J.A.; De Cocker, K.; Biddle, S.J.H.; Teychenne, M.J. Joint and dose-dependent associations between aerobic and muscle-strengthening activity with depression: A cross-sectional study of 1.48 million adults between 2011 and 2017. Depress. Anxiety 2020, 37, 166–178. [Google Scholar] [CrossRef]
- Repple, J.; Opel, N. Sport und körperliche Bewegung bei unipolarer Depression: Prävention, Therapie und neurobiologische Wirkmechanismen [Sport and physical exercise in unipolar depression: Prevention, therapy, and neurobiological mechanisms of action]. Nervenarzt 2021, 92, 507–514. [Google Scholar] [CrossRef]
- Kandola, A.; Vancampfort, D.; Herring, M.; Rebar, A.; Hallgren, M.; Firth, J.; Stubbs, B. Moving to Beat Anxiety: Epidemiology and Therapeutic Issues with Physical Activity for Anxiety. Curr. Psychiatry Rep. 2018, 20, 63. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- López-Ortiz, S.; Pinto-Fraga, J.; Valenzuela, P.L.; Martín-Hernández, J.; Seisdedos, M.M.; García-López, O.; Toschi, N.; Di Giuliano, F.; Garaci, F.; Mercuri, N.B.; et al. Physical Exercise and Alzheimer’s Disease: Effects on Pathophysiological Molecular Pathways of the Disease. Int. J. Mol. Sci. 2021, 22, 2897. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [Green Version]
- Narici, M.; Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport. Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Silva, L.R.B.; Seguro, C.S.; de Oliveira, C.G.A.; Santos, P.O.S.; de Oliveira, J.C.M.; de Souza Filho, L.F.M.; de Paula Júnior, C.A.; Gentil, P.; Rebelo, A.C.S. Physical Inactivity Is Associated with Increased Levels of Anxiety, Depression, and Stress in Brazilians During the COVID-19 Pandemic: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 565291. [Google Scholar] [CrossRef]
- Epps, F.; To, H.; Liu, T.T.; Karanjit, A.; Warren, G. Effect of Exercise Training on the Mental and Physical Well-Being of Caregivers for Persons Living with Chronic Illnesses: A Systematic Review and Meta-Analysis. J. Appl. Gerontol. 2021, 40, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Connell, C.M.; Janevic, M.R. Effects of a Telephone-Based Exercise Intervention for Dementia Caregiving Wives: A Randomized Controlled Trial. J. Appl. Gerontol. 2009, 28, 171–194. [Google Scholar] [CrossRef] [PubMed]
- van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hees, V.T.; Gorzelniak, L.; Dean León, E.C.; Eder, M.; Pias, M.; Taherian, S.; Ekelund, U.; Renström, F.; Franks, P.W.; Horsch, A.; et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE 2013, 8, e61691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hees, V.T.; Sabia, S.; Jones, S.E.; Wood, A.R.; Anderson, K.N.; Kivimäki, M.; Frayling, T.M.; Pack, A.I.; Bucan, M.; Trenell, M.I.; et al. Estimating sleep parameters using an accelerometer without sleep diary. Sci. Rep. 2018, 8, 12975. [Google Scholar] [CrossRef]
- van Hees, V.T.; Sabia, S.; Anderson, K.N.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.G.; Kivimäki, M.; Trenell, M.I.; Singh-Manoux, A. A Novel, Open Access Method to Assess Sleep Duration Using a Wrist-Worn Accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef] [Green Version]
- Rowlands, A.V.; Edwardson, C.L.; Davies, M.J.; Khunti, K.; Harrington, D.M.; Yates, T. Beyond Cut Points: Accelerometer Metrics that Capture the Physical Activity Profile. Med. Sci. Sport. Exerc. 2018, 50, 1323–1332. [Google Scholar] [CrossRef]
- Hildebrand, M.; Hansen, B.H.; van Hees, V.T.; Ekelund, U. Evaluation of raw acceleration sedentary thresholds in children and adults. Scand. J. Med. Sci. Sport. 2017, 27, 1814–1823. [Google Scholar] [CrossRef]
- Hildebrand, M.; VAN Hees, V.T.; Hansen, B.H.; Ekelund, U. Age group comparability of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sport. Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef]
- Menai, M.; van Hees, V.T.; Elbaz, A.; Kivimaki, M.; Singh-Manoux, A.; Sabia, S. Accelerometer assessed moderate-to-vigorous physical activity and successful ageing: Results from the Whitehall II study. Sci. Rep. 2017, 8, 45772. [Google Scholar] [CrossRef]
- Ferrell, B.; Grant, M.; Padilla, G.; Vemuri, S.; Rhiner, M. The experience of pain and perceptions of quality of life: Validation of a conceptual model. Hosp. J. 1991, 7, 9–24. [Google Scholar] [CrossRef]
- Ortiz, L.B. Construct validity and reliability of quality of life instrument family version in Spanish. Enferm. Global 2015, 14, 239–249. [Google Scholar]
- Robinson, C.A.; Pesut, B.; Bottorff, J.L. Supporting rural family palliative caregivers. J. Fam. Nurs. 2012, 18, 467–490. [Google Scholar] [CrossRef]
- López, S.R.; Morqal, M.S. Validation of the caregiver strain index in Spanish population. Enferm. Comunitaria. 2005, 1, 12–17. [Google Scholar]
- Ahn, S.; Romo, R.D.; Campbell, C.L. A systematic review of interventions for family caregivers who care for patients with advanced cancer at home. Patient. Educ. Couns. 2020, 103, 1518–1530. [Google Scholar] [CrossRef]
- Longacre, M.L.; Weber-Raley, L.; Kent, E.E. Cancer Caregiving While Employed: Caregiving Roles, Employment Adjustments, Employer Assistance, and Preferences for Support. J. Cancer Educ. 2021, 36, 920–932. [Google Scholar] [CrossRef]
- Unsar, S.; Erol, O.; Ozdemir, O. Caregiving burden, depression, and anxiety in family caregivers of patients with cancer. Eur. J. Oncol. Nurs. 2021, 50, 101882. [Google Scholar] [CrossRef]
- Jadalla, A.; Ginex, P.; Coleman, M.; Vrabel, M.; Bevans, M. Family Caregiver Strain and Burden: A Systematic Review of Evidence-Based Interventions When Caring for Patients with Cancer. Clin. J. Oncol. Nurs. 2020, 24, 31–50. [Google Scholar] [CrossRef]
- Kilic, S.T.; Oz, F. Family Caregivers’ Involvement in Caring with Cancer and their Quality of Life. Asian Pac. J. Cancer Prev. 2019, 20, 1735–1741. [Google Scholar] [CrossRef] [Green Version]
- Ito, E.; Tadaka, E. Quality of life among the family caregivers of patients with terminal cancer at home in Japan. Jpn. J. Nurs. Sci. 2017, 14, 341–352. [Google Scholar] [CrossRef] [Green Version]
- Rezende, V.L.; Derchain, S.F.M.; Botega, N.J.; Sarian, L.O.; Vial, D.L.; Morais, S.S. Depression and anxiety in caregivers of terminally-ill breast and gynecological cancer patients. Rev. Bras. Ginecol. Obs. 2005, 27, 737–743. [Google Scholar] [CrossRef]
- Cuthbert, C.A.; King-Shier, K.; Tapp, D.; Ruether, D.; Culos-Reed, S.N. Exploring Gender Differences in Self-Reported Physical Activity and Health Among Older Caregivers. Oncol. Nurs. Forum 2017, 44, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Skender, S.; Ose, J.; Chang-Claude, J.; Paskow, M.; Brühmann, B.; Siegel, E.M.; Steindorf, K.; Ulrich, C.M. Accelerometry and physical activity questionnaires—A systematic review. BMC Public Health 2016, 16, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Drenowatz, C.; Prasad, V.K.; Hand, G.A.; Shook, R.P.; Blair, S.N. Effects of moderate and vigorous physical activity on fitness and body composition. J. Behav. Med. 2016, 39, 624–632. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Durães, A.R.; Reis, H.F.C.D.; Neves, V.R.; Martinez, B.P.; Carvalho, V.O. High-intensity interval training versus moderate-intensity continuous training on exercise capacity and quality of life in patients with coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1696–1707. [Google Scholar] [CrossRef]
- Costa, E.C.; Hay, J.L.; Kehler, D.S.; Boreskie, K.F.; Arora, R.C.; Umpierre, D.; Szwajcer, A.; Duhamel, T.A. Effects of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training on Blood Pressure in Adults with Pre- to Established Hypertension: A Systematic Review and Meta-Analysis of Randomized Trials. Sport. Med. 2018, 48, 2127–2142. [Google Scholar] [CrossRef]
- De Strijcker, D.; Lapauw, B.; Ouwens, D.M.; Van de Velde, D.; Hansen, D.; Petrovic, M.; Cuvelier, C.; Tonoli, C.; Calders, P. High intensity interval training is associated with greater impact on physical fitness, insulin sensitivity and muscle mitochondrial content in males with overweight/obesity, as opposed to continuous endurance training: A randomized controlled trial. J. Musculoskelet Neuronal Interact. 2018, 18, 215–226. [Google Scholar]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef]


{kind=link}
| Mean | SD | |
|---|---|---|
| Age (years) | 62.71 | 12.80 |
| N | % | |
| Gender | ||
| Female | 66 | 88.0 |
| Male | 9 | 12.0 |
| Relationship with patient | ||
| Spouse | 41 | 54.7 |
| Daughter | 25 | 33.3 |
| Sister | 4 | 5.3 |
| Mother | 2 | 2.7 |
| Daughter-in-law | 1 | 1.3 |
| Sister-in-law | 1 | 1.3 |
| Mother-in-law | 1 | 1.3 |
| Caregiver’s marital status | ||
| Married | 52 | 69.3 |
| Single | 12 | 16.0 |
| Divorced | 9 | 12.0 |
| Widowed | 2 | 2.7 |
| Caregiver’s children (n) | ||
| None | 15 | 20.0 |
| One | 10 | 13.3 |
| Two | 29 | 38.7 |
| Three | 17 | 22.7 |
| Four or more | 4 | 5.3 |
| Caregiver’s education | ||
| Primary studies | 39 | 52.0 |
| Secondary studies | 20 | 26.7 |
| No formal studies | 8 | 10.7 |
| University studies | 8 | 10.7 |
| Employment status | ||
| No paid employment | 36 | 48.00 |
| In paid employment | 26 | 34.67 |
| Retired | 13 | 17.33 |
| Mean | SD | |
|---|---|---|
| SIB total (min/day) | 665.78 | 94.92 |
| SIB 1–10 min (min/day) | 69.40 | 25.93 |
| SIB 10–20 min (min/day) | 57.11 | 21.88 |
| SIB 20–30 min (min/day) | 46.84 | 18.91 |
| SIB >30 min (min/day) | 500.43 | 155.20 |
| Total LPA (min/day) | 201.64 | 59.06 |
| LPA 1–10 min (min/day) | 40.34 | 19.73 |
| LPA >10 min (min/day) | 4.24 | 10.59 |
| Total MPA (min/day) | 93.92 | 45.63 |
| Total VPA (min/day) | 2.47 | 5.46 |
| Total MVPA (min/day) | 96.40 | 46.93 |
| MVPA 1–10 min (min/day) | 26.14 | 19.00 |
| MVPA >10 min (min/day) | 9.48 | 15.95 |
| Napping (min/day) | 70.15 | 64.11 |
| Nocturnal sleep (min/day) | 395.25 | 66.12 |
| Sleep efficiency | 0.84 | 0.09 |
| N | % | |
| Compliance with WHO recommendation (MVPA ≥150 min/week) in episodes of at least 1 min/day | ||
| Yes | 68 | 90.7 |
| No | 7 | 9.3 |
| MVPA (≥150 min/week) in episodes of at least 10 min/day | ||
| Yes | 6 | 8.0 |
| No | 69 | 92.0 |
| MVPA (≥300 min/week) in episodes of at least 1 min/day | ||
| Yes | 66 | 88.0 |
| No | 9 | 12.0 |
| Mean | SD | |
|---|---|---|
| Quality of Life Family Version | ||
| Physical domain | 6.99 | 2.52 |
| Social domain | 5.92 | 1.97 |
| Psychological domain | 5.57 | 1.5 |
| Spiritual domain | 3.98 | 1.85 |
| Total quality of life | 5.62 | 1.46 |
| Care provision (hours/day) | 17.19 | 7.18 |
| Duration of care (months) | 17.33 | 27.04 |
| Duration of palliative care (months) | 3.93 | 4.82 |
| N | % | |
| Assistance received for care provision | ||
| No | 48 | 64.0 |
| Yes | 27 | 36.0 |
| Caregiver Strain Index | ||
| ≥7 points: 46 61.3 | 46 | 61.3 |
| <7 points: 29 38.7 | 29 | 38.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valero-Cantero, I.; Casals, C.; Corral-Pérez, J.; Barón-López, F.J.; Wärnberg, J.; Vázquez-Sánchez, M.Á. Accelerometer-Measured Physical Activity, Inactivity, and Related Factors in Family Caregivers of Patients with Terminal Cancer. Int. J. Environ. Res. Public Health 2023, 20, 179. https://doi.org/10.3390/ijerph20010179
Valero-Cantero I, Casals C, Corral-Pérez J, Barón-López FJ, Wärnberg J, Vázquez-Sánchez MÁ. Accelerometer-Measured Physical Activity, Inactivity, and Related Factors in Family Caregivers of Patients with Terminal Cancer. International Journal of Environmental Research and Public Health. 2023; 20(1):179. https://doi.org/10.3390/ijerph20010179
Chicago/Turabian StyleValero-Cantero, Inmaculada, Cristina Casals, Juan Corral-Pérez, Francisco Javier Barón-López, Julia Wärnberg, and María Ángeles Vázquez-Sánchez. 2023. "Accelerometer-Measured Physical Activity, Inactivity, and Related Factors in Family Caregivers of Patients with Terminal Cancer" International Journal of Environmental Research and Public Health 20, no. 1: 179. https://doi.org/10.3390/ijerph20010179