1. Introduction
Obesity is a critical public health problem that affects all stages of life, yet its prevalence has increased substantially among adolescents. According to the World Health Organization (WHO), between 1975 and 2016, the prevalence of obesity increased from 11 million in 1975 to 124 million in 2016 in children and adolescents aged 5 to 19 years [
1]. Worldwide, more individuals are obese than underweight, except for sub-Saharan Africa and Asia [
2]. In the United States, between 2017 to 2020, 14.7 million children and adolescents, aged 2 to 19 years old, were diagnosed with obesity [
3]. In 2019, in Brazil, more than 620,000 adolescents aged 15 to 17 years had obesity [
4].
The complexity of the disease treatment raises the probability of persistence of obesity in adulthood and the association with the early onset of other chronic noncommunicable diseases [
5,
6]. This fact is already a reality among Brazilian adolescents, as evidenced by the Study of Cardiovascular Risks in Adolescents (ERICA), revealing the existence of comorbidities such as hypertension, dyslipidemia, insulin resistance, and metabolic syndrome in this population [
7,
8,
9,
10].
Although poor diet remains one of the main risk factors responsible for this epidemiological context [
11], social, demographic, cultural, and economic factors particularly influence the nutritional status of adolescents [
12,
13]. Thus, it is possible to make associations between contextual factors and indicators of the nutritional status of adolescents, in order to assess the contribution of risk factors for the development of obesity and implement appropriate corrective and preventive actions [
14,
15,
16].
The use of public data made available by Health Information Systems (HIS) becomes a viable, easy-to-access, and low-cost alternative for providing continuous information on the nutritional status of adolescents. Among Brazilian computerized systems, the Food and Nutritional Surveillance System (Sisvan, in Portuguese) aims to provide data over time on the nutritional profile of the population using Primary Health Care (PHC) of the Unified Health System (SUS). Sisvan data assist in the formulation of actions, programs, and policies aimed at both the promotion of adequate and healthy eating, as well as the prevention and treatment of nutritional diseases [
17].
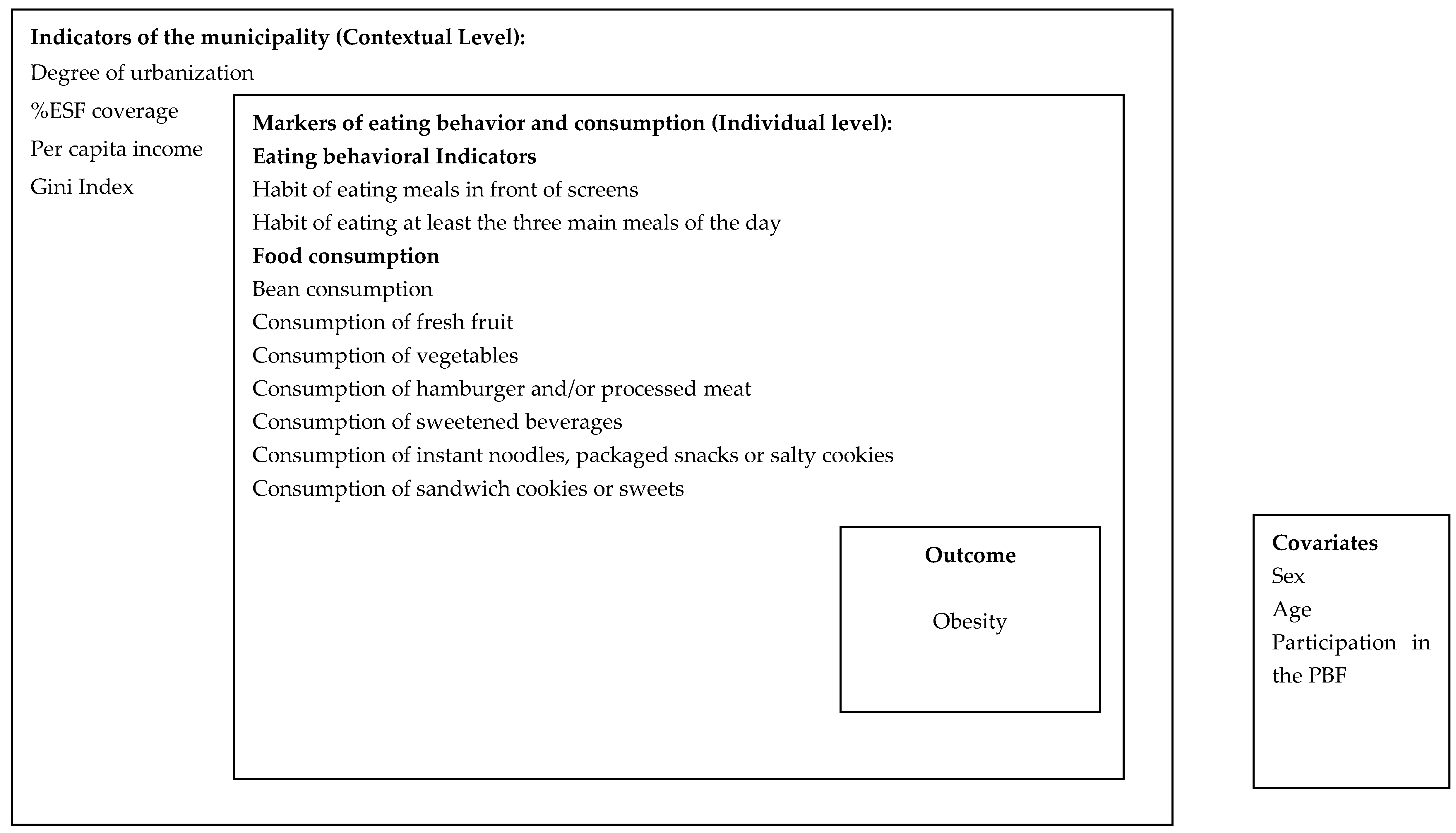
However, analysis of information on the food and nutritional status of adolescents, obtained through Sisvan, is still little explored. Thus, given the relevance of using these data in view of the current epidemiological context, as well as the absence of national data on adolescents monitored in PHC, the aim of this study was to investigate the association of socioeconomic contextual factors of the municipality of residence of adolescents, eating behavior, and food consumption with the prevalence of obesity.
4. Discussion
The present study was the first to analyze individual data from Sisvan of adolescents followed up in PHC in Brazil. The highest prevalence of obesity was associated with higher municipal per capita income and consumption of hamburgers and/or processed meats the day before. In contrast, lower prevalence of obesity was associated with having the habit of eating three main meals a day and eating fresh fruit the day before. Furthermore, the results indicate that despite the higher prevalence of consumption of healthy eating markers, there was a significant consumption of markers of unhealthy eating and a high prevalence of the habit of having meals in front of screens.
Inadequate food consumption and increased prevalence of obesity among Brazilian adolescents have been frequently observed in recent population surveys conducted in the country. The 2017−2018 Household Budget Survey (POF) pointed out that consumption of fruits and vegetables was lower among adolescents compared to older age groups. As an aggravating factor, the high consumption of markers of unhealthy eating (such as sandwich cookies, soft drinks, dairy drinks, packaged snacks, sandwiches, pizzas) by adolescents stands out [
29]. In the 2019 National School Health Survey (PeNSE), 97.3% of adolescents consumed at least one ultraprocessed food (UPF) the day before the survey [
30]. As in population surveys, there was high consumption of markers of unhealthy eating the day before by adolescents followed up in PHC in 2018.
As for the presence of obesity, our results (12.74–95% CI 12.31;13.17) are close to the data from the National Health Survey, which found a prevalence of 13.4% of adolescents aged 15–17 years with obesity [
4]. Since our data refer to PHC adolescents, who are generally more vulnerable, we can highlight the potential of using Sisvan to monitor the health of the population in this age group, as they are closer to the general population.
The prevalence of obesity demonstrates that we are facing a public health problem that has worsened over time, and that is a reflection of the food and nutrition transition process. Society has become increasingly urban and has experienced new demographic, behavioral, and consumption patterns [
31,
32]. The environment where the individual lives, and the different contextual factors that surround him/her, are recognized in the literature as risk factors for the development of diseases, especially chronic non-communicable diseases, such as obesity examined here. In a study of Chinese children and adolescents aged 6 to 17 years, higher rates of overweight and obesity were observed in urban areas and in families with higher income. In addition, the authors highlighted the higher prevalence in males [
12].
Although this study considered aggregated rather than individual contextual data, limiting comparison with the previous study, the results corroborate what was observed by Fan and Zhang (2021), with data from 137,995 adolescents aged 12 to 15 years from 21 countries based on Global School-Based Student Health Surveys from 2005 to 2017. The authors observed a trend of significant increase in the prevalence of being overweight and obesity, particularly in high-, upper-middle-, and lower-middle-income countries [
13].
There is evidence that low socioeconomic status is associated with higher BMI in high-income countries, and low BMI in middle-income countries [
32]. It is noteworthy that 14.97% of adolescents assessed in this study were beneficiaries of the former PBF.
In Brazil, there is great sociocultural, economic and urbanization inequality between geographic regions. The country has many developed cities and regions, in terms of urban infrastructure, basic sanitation, work, housing, access to health and education; on the other hand, it is possible to find others with much lower development rates, which impacts the lifestyle of young people, especially in relation to behavior and healthy food consumption [
33,
34,
35].
This scenario demonstrates the importance of systematic and constant monitoring of the nutritional status and dietary profile of adolescents, since in this age group there is the consolidation of eating behavior, with a great diversity and complexity of food choices, which, associated with body changes inherent to growth and sexual maturation, can lead to excessive weight gain [
6,
36]. Excess weight gain in the transition from adolescence to adulthood increases the risk of obesity in young adults. According to Kartiosuo et al. (2019), obese adolescents are 89.0% more likely to become obese adults [
37]. Similar data was found in the meta-analysis study carried out with 15 prospective cohort studies, where it was shown that about 80.0% of obese adolescents will still have obesity in adulthood and about 70.0% will have obesity after 30 years [
38].
The eating behavior of adolescents has been highlighted in different studies. Data from ERICA showed that more than half of adolescents had meals almost always or always in front of the TV, and consumed snacks in front of screens with this same frequency [
34]. Eating in front of screens, as well as spending more time in front of screens, is associated with higher caloric contribution of UPF in adolescents’ diet and sedentary lifestyle [
36,
39].
According to national and international studies, it is difficult for young people to adopt and maintain healthy eating patterns during adolescence. In the Longitudinal Study of Nutritional Assessment (ELANA), carried out with 1,035 adolescents from six schools in the metropolitan region of Rio de Janeiro, adolescents who consumed UPF tended to have a lower daily intake of fruits, raw and cooked vegetables and a higher intake of sugar [
40]. Doggui et al., (2021) evaluated 744 Canadian adolescents (age 11 to 18 years), followed from 2013 to 2019, and observed a decline in daily breakfast consumption, low consumption of fruits and vegetables, and increased consumption of fast food [
6].
A previous study with data from ERICA highlighted that the UPF most consumed by adolescents were instant pasta, packaged cookies, soft drinks and processed meat, and that higher consumption of these foods was associated with not having breakfast regularly [
36]. In our final model, presented in this work, having the three main meals a day (breakfast, lunch and dinner) and the consumption of fruits the day before were associated with a lower prevalence of obesity.
Our findings are in agreement with the recommendation of the Food Guide for the Brazilian Population, to have at least three main meals, since these represent about 90% of the total calories consumed throughout the day [
41]. This result is believed to be unprecedented in the literature, since it differs from most analyses carried out by other studies with adolescents.
The contribution of having meals instead of snacks to reduce the prevalence of obesity has already been observed in studies that evaluated adherence to school meals by adolescents [
42,
43]. Adolescents with high adherence to school meals (5 times/week) had 11.00% less prevalence of overweight (PR = 0.89–95% CI 0.80;0.99) and 24.00% less prevalence of obesity (PR = 0.76−95% CI 0.62;0.93) than those with lower adherence (<5 times/week) [
43].
In general, it can be considered that the fact that the traditional Brazilian food pattern (consumption of rice, beans, among other foods) is present in the daily life of the population contributes to the prevention of obesity, since it is characterized as a more nutritious diet compared to UPF [
44,
45]. In a study with seven cohorts of Swedish adolescents, high fruit intake was associated with higher vegetable intake (OR=25.7–95% CI 20.0;33.1), and a higher frequency of vegetable consumption was associated the lowest chance of being overweight and obesity among them (OR=0.77–95% CI 0.62–0.95) [
46]. In Norway, researchers did not find any beneficial effect on the BMI of children and adolescents who consumed fruits and vegetables in schools for up to four years [
47].
It is not possible to infer that the consumption of fruits and vegetables, by itself, has a protective effect against the disease; however, it should be encouraged and guaranteed by public policies for children and adolescents, especially those with lower family income, in order to guarantee the daily consumption of fiber, vitamins, minerals and antioxidant compounds. In this regard, Brazil is a protagonist in the formulation of public policies that aim to reduce the impact of the burden of chronic diseases on the population and improve the quality of life, through food and nutrition actions [
5,
48].
On the other hand, the adherence to eating patterns consisting of snacks and fast food by Brazilian adolescents showed a high correlation with the consumption of ham, bologna, turkey breast and salami, among other UPF groups [
45]. In the same study, young people who adhered to these standards were more likely to be overweight (OR = 1.50–95% CI 1.13–1.99 for the fifth quintile of the snacks pattern; OR = 1.55–95% CI 1.12–2.12 for the fifth quintile of the fast-food standard) [
45].
Kelly et al. (2022) in their study addressing the role of the gut-brain axis and its interaction with reward systems from UPF consumption, point out that understanding the different food choices is a critical problem in health research [
49]. However, the main points of discussion about the choice and consumption of UPF are related to its formulation, which deconstructs whole foods into chemical constituents, altering and recombining them with additives in products composed of low diversity of nutrients and highly palatable [
41]. Another property of UPFs is the supply of usable calories quickly becoming a potential factor driving their overconsumption [
49]. The mechanisms of action of this consumption, which lead to adverse health implications, may be the result of nutrient content, or ultra-processing [
49,
50].
The fact is that the amount of scientific evidence proving the association of UPF consumption with chronic non-communicable diseases and negative health outcomes has grown. In a systematic review and meta-analysis, five prospective cohort studies showed that higher UPF consumption was associated with an increased risk of all-cause mortality (RR = 1.25–95% CI, 1.14, 1.37;
p < 0.00001), three studies showed an increased risk of cardiovascular disease (RR = 1.29−95% CI, 1.12;1.48;
p = 0.0003), two studies showed a risk for cerebrovascular disease (RR = 1.34−95% CI, 1.07;1.68;
p = 0.01) and two studies for depression (RR = 1.20–95% CI, 1.03;1.40;
p = 0.02) [
51]. Another review with prospective cohort studies showed that higher UPF intake increases the risk of obesity, cardiovascular disease, cancer and type 2 diabetes [
52]. Therefore, actions are needed to help reduce the consumption of UPF by the population and promote an adequate and healthy diet.
The consumption of hamburgers and processed meats was associated with the highest prevalence of obesity in our study. In the systematic review and meta-analysis conducted by Rouhani et al., (2014), it was shown that red and processed meat intake was directly associated with risk of obesity, higher BMI and waist circumference. In addition, consumption of processed meat has been also proved as a cause of colorectal cancer [
53].
The markers of eating behavior and food consumption of Sisvan are not routinely recorded by professionals, who prioritize recording anthropometric measurements. This questionnaire of food consumption markers was included in Primary Health Care routine in 2015, but many professionals are still reluctant to incorporate this practice as a habit, generating less data on the population’s diet. Furthermore, food consumption data are based only on the day before the consultation and the anthropometric assessment based only on BMI does not reflect body composition. However, despite these possible variations, these instructions are reinforced in the national guideline for data collection and measurements of Sisvan in Primary Health Care in Brazil [
20].
Other limitations must be taken into account, such as the fact that a secondary database is used, where information may be underreported, errors may occur in the collection, typing and storage of data, reflecting the representativeness of the sample. Similar to all studies with secondary data from health services, our sample does not have representativeness and it is not an intentional study. Despite these limitations, a comparison was made between the analyzed sample and the projection of the Brazilian population according to the IBGE, in the year 2018, observing a similar distribution between the macroregions. For the adolescents’ data of Sisvan, the Southeast and Northeast regions were the ones that most contributed to the total sample, as well as the contingent estimated by the IBGE, whose largest projected populations for the same age group would be in these regions. Sisvan data cover all Brazilian regions, and the system is available to all Brazilian municipalities, which makes its capillarity of great relevance for public health actions in Brazil.
The cross-sectional design of the study prevents the inference of causality in the associations found. However, the way in which the data were obtained, and the consistency analysis performed, with the removal of duplicate follow-ups, missing data or inconsistent data on age, BMI calculations and nutritional status classification, were taken care of to minimize possible biases, thus, it may be considered a strength of our study. In addition, the cross-sectional design is a starting point for future investigations that will be able to carry out more robust analyses based on the results found.




{kind=link}