
Professional Competence and Its Effect on the Implementation of Healthcare 4.0 Technologies: Scoping Review and Future Research Directions

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
1.1. Background
1.1.1. Healthcare 4.0: Competence Requirement
1.1.2. The Competence Framework
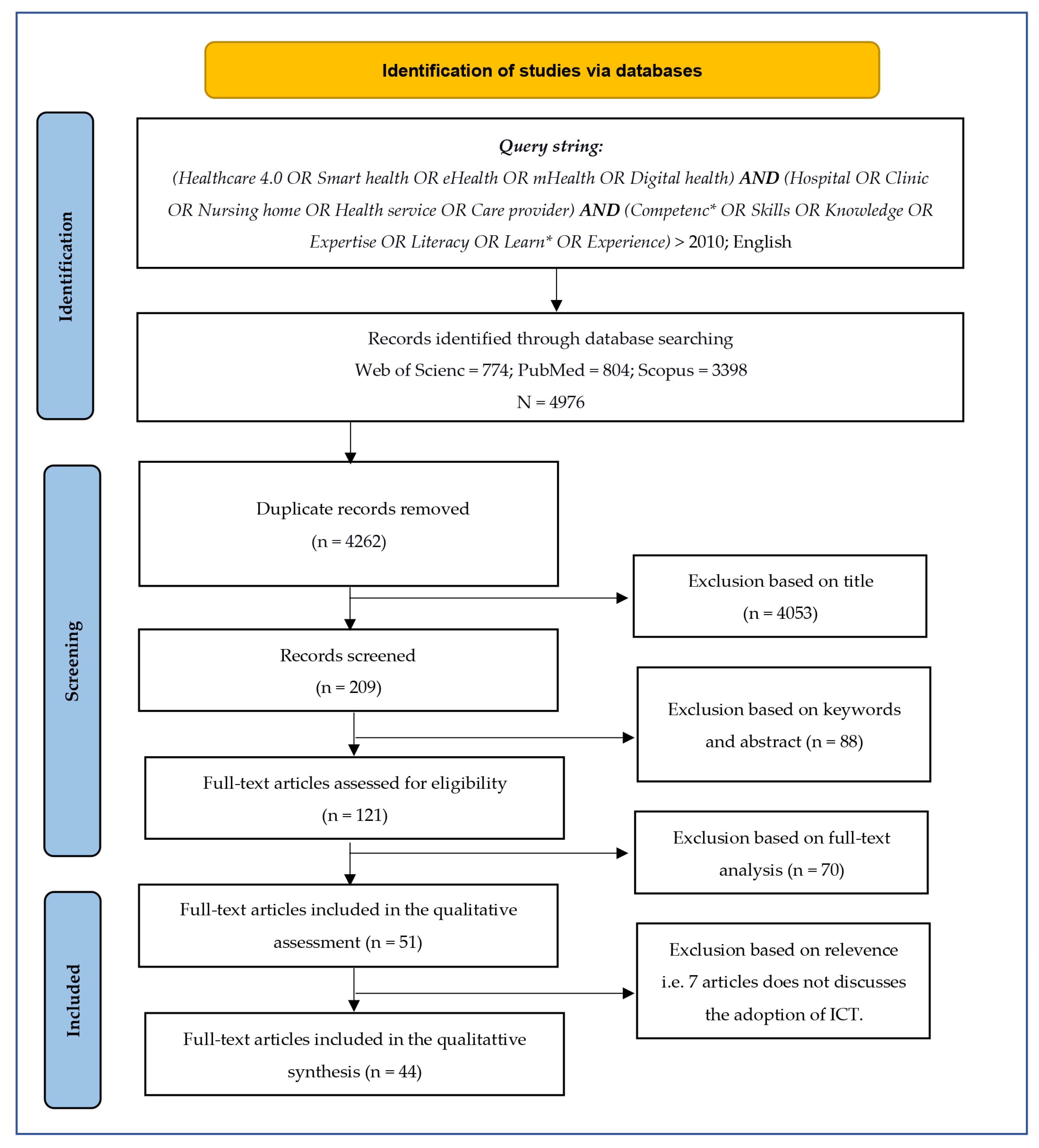
2. Materials and Methods
2.1. Identifying the Research Question
2.2. Identifying the Relevant Studies
2.3. Study Selection
2.4. Charting the Data
2.5. Collating, Summarising, and Reporting the Results
3. Results
4. Discussion
4.1. Principal Findings
4.2. Explicit Assessment of Various Competencies
4.3. Competence Development: Challenges and Solutions
5. Research Agenda
5.1. Validation of the Different Types of Competence in Adopting Healthcare 4.0
5.2. Examine the Need of Job-Specific Competence Factors
5.3. Explore the Impact of the Adoption of H4.0 on Organisational Learning Capabilities
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ajmera, P.; Jain, V. Modelling the Barriers of Health 4.0–The Fourth Healthcare Industrial Revolution in India by TISM. Oper. Manag. Res. 2019, 12, 129–145. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A. Industry 4.0 Applications in Medical Field: A Brief Review. Curr. Med. Res. Pract. 2019, 9, 102–109. [Google Scholar] [CrossRef]
- Chanchaichujit, J.; Tan, A.; Meng, F.; Eaimkhong, S. Healthcare 4.0: Next Generation Processes with the Latest Technologies, 1st ed.; Palgrave Pivot Singapore: Singapore, 2019. [Google Scholar] [CrossRef]
- Lhotska, L. Application of Industry 4.0 Concept to Health Care. Stud. Health Technol. Inform. 2020, 273, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, P.P.; Forkan, A.R.M.; Morshed, A.; Haghighi, P.D.; Kang, Y.-B. Healthcare 4.0: A Review of Frontiers in Digital Health. WIREs Data Min. Knowl. Discov. 2020, 10, e1350. [Google Scholar] [CrossRef]
- Foadi, N.; Varghese, J. Digital Competence--A Key Competence for Todays and Future Physicians. J. Eur. CME 2022, 11, 2015200. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A Scoping Review of Scoping Reviews: Advancing the Approach and Enhancing the Consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef] [Green Version]
- Hecklau, F.; Galeitzke, M.; Flachs, S.; Kohl, H. Holistic Approach for Human Resource Management in Industry 4.0. Procedia CIRP 2016, 54, 1–6. [Google Scholar] [CrossRef]
- Tortorella, G.L.; Fogliatto, F.S.; mac Cawley Vergara, A.; Vassolo, R.; Sawhney, R. Healthcare 4.0: Trends, Challenges and Research Directions. Prod. Plan. Control 2020, 31, 1245–1260. [Google Scholar] [CrossRef]
- Chukwuekwe, D.O.; Schjoelberg, P.; Roedseth, H.; Stuber, A. Reliable, Robust and Resilient Systems: Towards Development of a Predictive Maintenance Concept within the Industry 4.0 Environment. In Proceedings of the EFNMS Euro Maintenance Conference, Athens, Greece, 30 May–1 June 2016. [Google Scholar]
- Pang, Z.; Yang, G.; Khedri, R.; Zhang, Y.-T. Introduction to the Special Section: Convergence of Automation Technology, Biomedical Engineering, and Health Informatics Toward the Healthcare 4.0. IEEE Rev. Biomed. Eng. 2018, 11, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, K.A.B.; Khujamatov, H.; Akhmedov, N.; Bajuri, M.Y.; Ahmad, M.N.; Ahmadian, A. Emerging Trends and Evolutions for Smart City Healthcare Systems. Sustain. Cities Soc. 2022, 80, 103695. [Google Scholar] [CrossRef]
- Daft, R.L.; Armstrong, A. Organization Theory and Design, 3rd ed.; Nelson Education: Toronto, ON, USA, 2015. [Google Scholar]
- Buchelt, B.; Frkaczkiewicz-Wronka, A.; Dobrowolska, M. The Organizational Aspect of Human Resource Management as a Determinant of the Potential of Polish Hospitals to Manage Medical Professionals in Healthcare 4.0. Sustainability 2020, 12, 5118. [Google Scholar] [CrossRef]
- Whelan, L. Competency Assessment of Nursing Staff. Orthop. Nurs. 2006, 25, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Locsin, R.C. Technologic Competence as Caring in Critical Care Nursing. Holist. Nurs. Pract. 1998, 12, 50–56. [Google Scholar] [CrossRef]
- Castle, N.; Garton, H.; Kenward, G. Confidence vs Competence: Basic Life Support Skills of Health Professionals. Br. J. Nurs. 2007, 16, 664–666. [Google Scholar] [CrossRef]
- Kak, N.; Burkhalter, B.; Cooper, M.-A. Measuring the Competence of Healthcare Providers. Oper. Res. Issue Pap. 2001, 2, 1–28. [Google Scholar]
- Guo, K.L. An Assessment Tool for Developing Healthcare Managerial Skills and Roles. J. Healthc. Manag. 2003, 48, 367–376; discussion 376. [Google Scholar] [CrossRef] [Green Version]
- Santric Milicevic, M.M.; Bjegovic-Mikanovic, V.M.; Terzic-Supic, Z.J.; Vasic, V. Competencies Gap of Management Teams in Primary Health Care. Eur. J. Public Health 2011, 21, 247–253. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, S.; Lanza, G.; Enna, C.; Zangrandi, A. Managerial Competences in Public Organisations: The Healthcare Professionals’ Perspective. BMC Health Serv. Res. 2020, 20, 303. [Google Scholar] [CrossRef] [Green Version]
- Köppen, J.; Maier, C.B.; Busse, R. What Are the Motivating and Hindering Factors for Health Professionals to Undertake New Roles in Hospitals? A Study among Physicians, Nurses and Managers Looking at Breast Cancer and Acute Myocardial Infarction Care in Nine Countries. Health Policy 2018, 122, 1118–1125. [Google Scholar] [CrossRef]
- Konttila, J.; Siira, H.; Kyngäs, H.; Lahtinen, M.; Elo, S.; Kääriäinen, M.; Kaakinen, P.; Oikarinen, A.; Yamakawa, M.; Fukui, S.; et al. Healthcare Professionals’ Competence in Digitalisation: A Systematic Review. J. Clin. Nurs. 2019, 28, 745–761. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tortorella, G.L.; Fogliatto, F.S.; Espôsto, K.F.; mac Cawley Vergara, A.; Vassolo, R.; Tlapa Mendoza, D.; Narayanamurthy, G. Measuring the Effect of Healthcare 4.0 Implementation on Hospitals’ Performance. Prod. Plan. Control 2022, 33, 386–401. [Google Scholar] [CrossRef]
- Borges, G.A.; Tortorella, G.; Rossini, M.; Portioli-Staudacher, A. Lean Implementation in Healthcare Supply Chain: A Scoping Review. J. Health Organ. Manag. 2019, 33, 304–322. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, G.; Fogliatto, F.S.; Gao, S.; Chan, T.-K. Contributions of Industry 4.0 to Supply Chain Resilience. Int. J. Logist. Manag. 2022, 33, 547–566. [Google Scholar] [CrossRef]
- Pagliosa, M.; Tortorella, G.; Ferreira, J.C.E. Industry 4.0 and Lean Manufacturing: A Systematic Literature Review and Future Research Directions. J. Manuf. Technol. Manag. 2021, 32, 543–569. [Google Scholar] [CrossRef]
- Landis-Lewis, Z.; Manjomo, R.; Gadabu, O.J.; Kam, M.; Simwaka, B.N.; Zickmund, S.L.; Chimbwandira, F.; Douglas, G.P.; Jacobson, R.S. Barriers to Using EHealth Data for Clinical Performance Feedback in Malawi: A Case Study. Int. J. Med. Inform. 2015, 84, 868–875. [Google Scholar] [CrossRef] [Green Version]
- Curtis, K.; Brooks, S. Digital Health Technology: Factors Affecting Implementation in Nursing Homes. Nurs. Older People 2020, 32, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Gardas, B.B. Organizational Hindrances to Healthcare 4.0 Adoption: An Multi-Criteria Decision Analysis Framework. J. Multi-Criteria Decis. Anal. 2021, 29, 185–196. [Google Scholar] [CrossRef]
- Yusif, S.; Hafeez-Baig, A.; Soar, J. Change Management and Adoption of Health Information Technology (HIT)/EHealth in Public Hospitals in Ghana: A Qualitative Study. Appl. Comput. Inform. 2020, 18, 279–289. [Google Scholar] [CrossRef]
- Elkefi, S.; Asan, O.; Mnasouri, M. Change Management and Continuous Improvement for Smarter Care: A Systems Viewpoint. In Proceedings of the ISSE 2021—7th IEEE International Symposium on Systems Engineering, Vienna, Austria, 13 September–13 October 2021; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2021; pp. 189–195. [Google Scholar] [CrossRef]
- Saleh, S.; Khodor, R.; Alameddine, M.; Baroud, M. Readiness of Healthcare Providers for EHealth: The Case from Primary Healthcare Centers in Lebanon. BMC Health Serv. Res. 2016, 16, 644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thapa, S.; Nielsen, J.B.; Aldahmash, A.M.; Qadri, F.R.; Leppin, A. Willingness to Use Digital Health Tools in Patient Care Among Health Care Professionals and Students at a University Hospital in Saudi Arabia: Quantitative Cross-Sectional Survey. JMIR Med. Educ. 2021, 7, e18590. [Google Scholar] [CrossRef] [PubMed]
- Bravo, J.; Hervás, R.; Fontecha, J.; González, I. M-Health: Lessons Learned by m-Experiences. Sensors 2018, 18, 1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, L.; FitzPatrick, M.E.B.; Roycroft, M. The Role of the Future Physician: Building on Shifting Sands. Clin. Med. 2020, 20, 285. [Google Scholar] [CrossRef]
- Kamenjasevic, E.; Povse, D.F. A Data Protection Perspective on Training in the Mhealth Sector. EAI/Springer Innov. Commun. Comput. 2019, 2019, 71–85. [Google Scholar] [CrossRef]
- Ogoe, H.A.; Asamani, J.A.; Hochheiser, H.; Douglas, G.P. Assessing Ghana’s EHealth Workforce: Implications for Planning and Training. Hum. Resour. Health 2018, 16, 65. [Google Scholar] [CrossRef]
- Jensen, S.; Kushniruk, A. Boundary Objects in Clinical Simulation and Design of EHealth. Health Inform. J. 2016, 22, 248–264. [Google Scholar] [CrossRef]
- Anyanwu, E.C.; Ward, R.P.; Shah, A.; Arora, V.; Umscheid, C.A. A Mobile App to Facilitate Socially Distanced Hospital Communication During COVID-19: Implementation Experience. JMIR mHealth uHealth 2021, 9, e24452. [Google Scholar] [CrossRef]
- Kiberu, V.M.; Scott, R.E.; Mars, M. Assessing Core, e-Learning, Clinical and Technology Readiness to Integrate Telemedicine at Public Health Facilities in Uganda: A Health Facility--Based Survey. BMC Health Serv. Res. 2019, 19, 266. [Google Scholar] [CrossRef]
- Albarrak, A.I.; Mohammed, R.; Almarshoud, N.; Almujalli, L.; Aljaeed, R.; Altuwaijiri, S.; Albohairy, T. Assessment of Physician’s Knowledge, Perception and Willingness of Telemedicine in Riyadh Region, Saudi Arabia. J. Infect. Public Health 2021, 14, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Occelli, S.; Scelfo, B. Can We Enable Digital Transition in Healthcare Delivery?: Insights From a Survey of Telemedicine Services in the Piedmont Region. Int. J. E-Plan. Res. (IJEPR) 2020, 9, 43–65. [Google Scholar] [CrossRef]
- Loeb, A.E.; Rao, S.S.; Ficke, J.R.; Morris, C.D.; Riley III, L.H.; Levin, A.S. Departmental Experience and Lessons Learned with Accelerated Introduction of Telemedicine during the COVID-19 Crisis. J. Am. Acad. Orthop. Surg. 2020, 28, e469–e476. [Google Scholar] [CrossRef] [PubMed]
- Öberg, U.; Orre, C.J.; Isaksson, U.; Schimmer, R.; Larsson, H.; Hörnsten, Å. Swedish Primary Healthcare Nurses’ Perceptions of Using Digital EH Ealth Services in Support of Patient Self-Management. Scand. J. Caring Sci. 2018, 32, 961–970. [Google Scholar] [CrossRef]
- Stadin, M.; Nordin, M.; Fransson, E.I.; Broström, A. Healthcare Managers’ Experiences of Technostress and the Actions They Take to Handle It--A Critical Incident Analysis. BMC Med. Inform. Decis. Mak. 2020, 20, 244. [Google Scholar] [CrossRef] [PubMed]
- Moss, R.J.; Süle, A.; Kohl, S. EHealth and MHealth. Eur. J. Hosp. Pharm. 2019, 26, 57–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiAngi, Y.T.; Stevens, L.A.; Halpern-Felsher, B.; Pageler, N.M.; Lee, T.C. Electronic Health Record (EHR) Training Program Identifies a New Tool to Quantify the EHR Time Burden and Improves Providers’ Perceived Control over Their Workload in the EHR. JAMIA Open 2019, 2, 222–230. [Google Scholar] [CrossRef]
- Marutha, N.S. Framework for Medical and Health Records Management Skills and Competency Development in Limpopo Public Hospitals to Support Healthcare Service Delivery in the Digital Era. Afr. J. Libr. Arch. Inf. Sci. 2019, 29, 187–199. [Google Scholar]
- Tesfa, G.A.; Kalayou, M.H.; Zemene, W. Electronic Health-Information Resource Utilization and Its Associated Factors among Health Professionals in Amhara Regional State Teaching Hospitals, Ethiopia. Adv. Med. Educ. Pract. 2021, 12, 195–202. [Google Scholar] [CrossRef]
- Gartrell, K.; Han, K.; Trinkoff, A.; Cho, H. Three-Factor Structure of the EHealth Literacy Scale and Its Relationship with Nurses’ Health-Promoting Behaviours and Performance Quality. J. Adv. Nurs. 2020, 76, 2522–2530. [Google Scholar] [CrossRef]
- Faloye, S.T.; Ndlanzi, S.L.; Ajayi, N. Factors Affecting E-Health Adoption in South African Public Hospitals: A Case of Edendale Hospital. In 2021 IST-Africa Conference, IST-Africa 2021; Cunningham, M.C.P., Ed.; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2021; pp. 902–912. [Google Scholar]
- Shiferaw, K.B.; Mengiste, S.A.; Gullslett, M.K.; Zeleke, A.A.; Tilahun, B.; Tebeje, T.; Wondimu, R.; Desalegn, S.; Mehari, E.A. Healthcare Providers’ Acceptance of Telemedicine and Preference of Modalities during COVID-19 Pandemics in a Low-Resource Setting: An Extended UTAUT Model. PLoS ONE 2021, 16, e0250220. [Google Scholar] [CrossRef] [PubMed]
- Kukhtevich, I.; Goryunova, V.; Goryunova, T. Aspects of Using Intelligent Cloud Technologies in Professional Training of General Practitioners. In Proceedings of the 2021 1st International Conference on Technology Enhanced Learning in Higher Education (TELE), Lipetsk, Russia, 24–25 June 2021; IEEE: New York, NY, USA, 2021; pp. 53–57. [Google Scholar] [CrossRef]
- van Houwelingen, T.; Ettema, R.G.A.; Bleijenberg, N.; van Os-Medendorp, H.; Kort, H.S.M.; ten Cate, O. Educational Intervention to Increase Nurses’ Knowledge, Self-Efficacy and Usage of Telehealth: A Multi-Setting Pretest-Posttest Study. Nurse Educ. Pract. 2021, 51, 102924. [Google Scholar] [CrossRef] [PubMed]
- Rubbio, I.; Bruccoleri, M.; Pietrosi, A.; Ragonese, B. Digital Health Technology Enhances Resilient Behaviour: Evidence from the Ward. Int. J. Oper. Prod. Manag. 2020, 39, 260–293. [Google Scholar] [CrossRef]
- Varsi, C.; Ekstedt, M.; Gammon, D.; Børøsund, E.; Ruland, C.M. Middle Managers’ Experiences and Role in Implementing an Interactive Tailored Patient Assessment EHealth Intervention in Clinical Practice. CIN Comput. Inform. Nurs. 2015, 33, 249–257. [Google Scholar] [CrossRef] [PubMed]
- van Houwelingen, C.T.M.; Ettema, R.G.A.; Kort, H.S.M.; ten Cate, O. Hospital Nurses’ Self-Reported Confidence in Their Telehealth Competencies. J. Contin. Educ. Nurs. 2019, 50, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjellebæk, C.; Svensson, A.; Bjørkquist, C.; Fladeby, N.; Grundén, K. Management Challenges for Future Digitalization of Healthcare Services. Futures 2020, 124, 102636. [Google Scholar] [CrossRef]
- Thi Ha, D.; Nuntaboot, K. New Competencies Required for Nurses as Compared to the National Nursing Competency Standards in Vietnam. Kontakt 2020, 22, 92–95. [Google Scholar] [CrossRef]
- Wernhart, A.; Gahbauer, S.; Haluza, D. EHealth and Telemedicine: Practices and Beliefs among Healthcare Professionals and Medical Students at a Medical University. PLoS ONE 2019, 14, e0213067. [Google Scholar] [CrossRef]
- Schwarz, F.; Ward, J.; Willcock, S. E-Health Readiness in Outback Communities: An Exploratory Study. Rural Remote Health 2014, 14, 2871. [Google Scholar] [CrossRef]
- Kuek, A.; Hakkennes, S. Healthcare Staff Digital Literacy Levels and Their Attitudes towards Information Systems. Health Inform. J. 2020, 26, 592–612. [Google Scholar] [CrossRef]
- Chen, P.; Xiao, L.; Gou, Z.; Xiang, L.; Zhang, X.; Feng, P. Telehealth Attitudes and Use among Medical Professionals, Medical Students and Patients in China: A Cross-Sectional Survey. Int. J. Med. Inform. 2017, 108, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Vanagas, G. Willingness to Use EHealth Services in Lithuanian Healthcare Institutions. Countrywide Survey. Biomed. Tech. 2011, 56, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Herlambang, R.; Pertiwi, A.A.P.; Sugiarsih. Physicians and Nurses’ Readiness in Using Electronic Health Record (EHR). Enferm. Clin. 2021, 31, 489–494. [Google Scholar] [CrossRef]
- Karahanna, E.; Chen, A.; Liu, Q.B.; Serrano, C. Capitalizing on Health Information Technology to Enable Digital Advantage in US Hospitals. MIS Q. 2019, 43, 113–140. [Google Scholar] [CrossRef]
- Dyb, K.; Granja, C.; Bolle, S.R.; Hartvigsen, G. Digital Users in Pre-Digital Hospital Organisations? An Analysis on the Readiness for Electronic Communication Between a Hospital and Surgical Patients. Int. J. Adv. Life Sci. 2016, 8, 39–49. [Google Scholar]
- Chao, C.-A. The Impact of Electronic Health Records on Collaborative Work Routines: A Narrative Network Analysis. Int. J. Med. Inform. 2016, 94, 100–111. [Google Scholar] [CrossRef]
- Durrani, H.; Khoja, S.; Naseem, A.; Scott, R.E.; Gul, A.; Jan, R. Health Needs and EHealth Readiness Assessment of Health Care Organizations in Kabul and Bamyan, Afghanistan. EMHJ-East. Mediterr. Health J. 2012, 18, 663–670. [Google Scholar] [CrossRef]
- Benwell, N.; Hird, K.; Thomas, N.; Furness, E.; Fear, M.; Sweetman, G. Effectiveness and Efficiency of Training in Digital Healthcare Packages: Training Doctors to Use Digital Medical Record Keeping Software. Aust. Health Rev. 2016, 41, 479–484. [Google Scholar] [CrossRef] [Green Version]
- Purwanto, M.P.A.; Ong, F.; Kusumaningsih, S.W.; Mustikasiwi, A.; Chidir, G.; Winanti; Ardian Sopa, M.A. The Impacts of Leadership and Organizational Culture on Performance in Indonesian Public Health: The Mediating Effects of Innovative Work Behavior. Int. J. Control Autom. 2020, 13, 216–227. [Google Scholar]
- Tortorella, G.L.; Fogliatto, F.S.; Saurin, T.A.; Tonetto, L.M.; McFarlane, D. Contributions of Healthcare 4.0 Digital Applications to the Resilience of Healthcare Organizations during the COVID-19 Outbreak. Technovation 2021, 111, 102379. [Google Scholar] [CrossRef]
- Watterson, J.L.; Rodriguez, H.P.; Aguilera, A.; Shortell, S.M. Ease of Use of Electronic Health Records and Relational Coordination among Primary Care Team Members. Health Care Manag. Rev. 2020, 45, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Schallock, B.; Rybski, C.; Jochem, R.; Kohl, H. Learning Factory for Industry 4.0 to Provide Future Skills beyond Technical Training. Procedia Manuf. 2018, 23, 27–32. [Google Scholar] [CrossRef]
- Drejer, A. Organisational Learning and Competence Development. Learn. Organ. 2000, 7, 206–220. [Google Scholar] [CrossRef] [Green Version]
- Graells, A.; Castell Ariño, N.; Insa, E. Learning Based on Challenges in the Context of Multidisciplinary Teamwork in Ehealth: An Evaluation of the Students’ Experience. In Proceedings of the ICERI 2019: 12th International Conference of Education, Research and Innovation, Seville, Spain, 11–13 November 2019; pp. 7798–7803. [Google Scholar] [CrossRef]
- Risling, T.L.; Risling, D.E. Advancing Nursing Participation in User-Centred Design. J. Res. Nurs. 2020, 25, 226–238. [Google Scholar] [CrossRef]
- Gagnon, M.P.; Légaré, F.; Labrecque, M.; Frémont, P.; Pluye, P.; Gagnon, J.; Car, J.; Pagliari, C.; Desmartis, M.; Turcot, L.; et al. Interventions for Promoting Information and Communication Technologies Adoption in Healthcare Professionals. Cochrane Database Syst. Rev. 2009, 1, CD006093. [Google Scholar] [CrossRef]
- Strecher, V. Internet Methods for Delivering Behavioral and Health-Related Interventions (EHealth). Annu. Rev. Clin. Psychol. 2007, 3, 53–76. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Competency Type | Technical Competency | Methodological Competency | Social Competency | Personal Competency |
|---|---|---|---|---|
| Definition | Individual’s abilities to handle different ICTs, large amounts of data, and work virtually with associated sub-skills. | Individual’s abilities to be innovative, involved in strategic tasks, resolve potential issues in the tasks efficiently, and learn continuously with associated sub-skills. | Individual’s ability to work with people from diverse backgrounds, utilise knowledge networks, transfer work and knowledge, and take on more responsibilities. | Individual’s abilities to be flexible with job profiles, accept changes, be ready to learn new things and support sustainable initiatives, manage pressure, and understand regulatory requirements. |
| Associated sub-skills |
|
|
|
|
| Keywords | Database | Initial Screening |
|---|---|---|
| (Healthcare 4.0 OR Smart health OR eHealth OR mHealth OR Digital health) AND (Hospital) AND (Competenc* OR Skills OR Knowledge) | Web of Science | 234 |
| PubMed | 233 | |
| Scopus | 264 | |
| Total | 731 |
| Keywords | Database | Initial Screening | Articles Filtering Steps | |||
|---|---|---|---|---|---|---|
| Removal of Duplicate Articles | Article’s Titles Aligned with the Research Topic | Abstracts Aligned with the Research Topic | Article’s Full Text Aligned with the Research Topic | |||
| (Healthcare 4.0 OR Smart health OR eHealth OR mHealth OR Digital health) AND (Hospital OR Clinic OR Nursing home OR Health service OR Care provider) AND (Competenc* OR Skills OR Knowledge OR Expertise OR Literacy OR Learn* OR Experience) | Web of Science | 774 | 4262 | 209 | 121 | 51 |
| PubMed | 804 | |||||
| Scopus | 3398 | |||||
| Total | 4976 | |||||
| Year | Count |
|---|---|
| 2011 | 1 |
| 2012 | 1 |
| 2014 | 1 |
| 2015 | 2 |
| 2016 | 4 |
| 2017 | 2 |
| 2018 | 3 |
| 2019 | 10 |
| 2020 | 15 |
| 2021 | 12 |
| Journal Name | Count |
|---|---|
| BMC Health Services Research | 3 |
| International Journal of Medical Informatics | 3 |
| Health Informatics Journal | 2 |
| PLoS ONE | 2 |
| Others | 41 |
| H4.0 ICTs Sr. No. | Name of ICTs/Role | Non-Clinical Applications | Clinical Application |
|---|---|---|---|
| t1 | Biomedical/digital wireless sensors/(S–C) | - | |
| t2 | Internet of things (IoT)/(S–C) | Monitoring of patients [55,56] | |
| t3 | Big data/(S–C) | - | A large amount of health data, big data analytics for healthcare [33,38] |
| t4 | Cloud/fog computing/(S–C) | Healthcare data stored in cloud [33] | |
| t5 | Remote control/monitoring/(S–C) | Remote consultations [58]/remote medical reporting [46] | Remote assistance [46], remote patient rounding/remote monitoring of patients [56] |
| t6 | Collaborative robots/robotics/(P–A) | - | Machine-assisted procedures [39] |
| t7 | Machine/deep learning/(P–A) | - | Informed decisions [55] |
| State-of-the-Art Knowledge | Technical Skills | Process Understanding | Handling Smart Devices, Apps, Smart Media | Data/Information Processing Skills | Understanding IT Security | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Professional Knowledge of Individual | Knowledge to Handle Various Technologies | Knowledge of System-Specific Tasks | Knowledge Acquired from Experience | Knowledge Acquired from Interactions and Meetings | Knowledge to Prioritise the Needs | Knowledge of the Pre-Operative Planning Process | Knowledge of Data Protection | Technical Skills in the Workplace | Handling of Healthcare 4.0 and Other eHealth Technologies | Operation of Computer Systems and Computer Literacy | Device Testing and Troubleshooting | Evaluation Abilities | Understanding of Related Processes and Procedures | Feedbacks Processed with Data | Hardware and Software Processing | |||
| Kukhtevich [57] Elkefi [35] Rubbio [59] Curtis and Brooks [32] Varsi [60] Houwelingen [61] Gjellebæk [62] Ha and Nuntaboot [63] Buchel t [15] Fernandes [39] Gartrell [54] Marutha [52] | Kiberu [44] Wernhart [64] Schwarwz [65] Kuek and Hakkennes, [66] Saleh [36] Öberg [48] Chen [67] Vanagas [68] Albarrak [45] Herlambang [69] | Jensen and Kushniruk [42] Moss [50] Varsi [60] | Yusif [34] Marutha, [52] Bravo [38] Chen [67] | Yusif [34] | Karahanna [70] | Dyb [71] | Houwelingen [58] | Kukhtevich [57] Rubbio [59] Moss [50] Schwarz [65] Ha and Nuntaboot, [63] Buchelt [15] Fernan des [39] | Kiberu [44] Ogoe [41] Albarrak [45] Curtis and Brooks, [32] Houwelingen [58] Faloye [55] Marutha [52] Kuek and Hakkennes [66] Houwelingen [61] Gardas [33] Chao [72] Durrani [73] | Landis-Lewis [31] Benwell [74] Tesfa [53] Stadin [49] Shiferaw [56] Saleh [36] Öberg [48] Herlamb ang [69] | Jensen and Kushniruk, [42] Loeb [47] Karahanna [70] | Gartrell [54] | Albarrak [45] Loeb [47] Marutha [52] Varsi [60] Ha and Nuntaboot [63] Fernandes [39] | Landis-Lewis [31] | Karahanna [70] | Albarrak [45] Landis-Lewis [31] Jensen and Kushniruk [42] Loeb [47] Curtis and Brooks [32] Houwelingen [58] Tesfa [53] Shiferaw [56] Kuek and Hakkennes [66] Saleh [36] Öberg [48] Moss [50] | Landis-Lewis [31] Marutha [52] Shiferaw [56] | Kamenjasevic and Povese [40] Anyanwu [43] Curtis and Brooks [32] Houwelingen [61] Houw elingen [58] Vanagas [68] |
| Creativity | Entrepreneurial Thinking | Problem Solving | Conflict Solving | Decision Making | Analytical Skills | Research Skills | Efficiency Orientation | Creativity |
|---|---|---|---|---|---|---|---|---|
| Anyanwu [43] Karahanna [70] Prameswari [75] Buchelt [15] | Buchelt [15] | Jensen and Kushniru [42] Loeb [47] Rubbio [59] Houwelingen [58] Scharwz [65] Marutha [52] Shiferaw [56] Buchtel [15] Gartrell [54] Houwelingen [58] | Buchelt [15] Gartrell [54] | Jensen and Kushniruk [42] Rubbio [59] Houwelingen [58] Scharwz [65] Houwelingen [61] Buchtel [15] Karahanna [70] Elkefi [35] Yusif [34] Fernandes [39] Gartrell [54] Buchtel [15] | Shiferaw [56] Kuck and Hakkennes [66] Fernandes [39] Gartrell [54] Buchelt [15] Jensen and Kushniruk [42] | Fernandes [39] | Buchelt [15] | Anyanwu [43] Karahanna [70] Prameswari [75] Buchelt [15] |
| Intercultural Skills | Language Skills | Communication Skills | Networking Skills | Ability to Work in a Team | Ability to Be Compromising | Ability to Transfer Knowledge | Leadership Skills |
|---|---|---|---|---|---|---|---|
| Jensen and Kushniruk [42] Tortorella [76] Durrani [73] Ha and Nuntaboot [63] | - | Jensen and Kushniruk [42] Yusif [34] Elkefi [35] Loeb [47] Curtis and Brooks [32] Marutha [52] Shiferaw [56] Houwelingen [61] Gjellebæk [62] Varsi [60] Chao [72] Buchtel [15] | Occelli and Scelfo [46] Karahanna [70] Yusif [34] Scharwz [65] Durrani [73] Gjellebæk [62] Varsi [60] Buchelt [15] Fernandes [39] Vanagas [68] | Jensen and Kushniruk [42] Rubbio [59] Dyb [71] Scharwz [65] Marutha [52] Shiferaw [56] Gjellebæk [62] Bravo [38] Varsi [60] Gardas [33] Chao [72] Watterson [77] | Stadin [49] Gardas [33] Watterson [77] | Jensen and Kushniruk [42] Karahanna [70] Tortorella [76] Houwelingen [58] Benwell [74] Scharwz [65] Houwelingen [61] | Scharwz [65] Marutha [52] Gjellebæk [62] Varsi [60] Gardas [33] Prameswari [75] Buchelt [15] Fernandes [39] |
| Flexibility | Ambiguity Tolerance | Motivation to Learn | Ability to Work under Pressure | Sustainable Mindset | Compliance |
|---|---|---|---|---|---|
| Anyanwu [43] Rubbio [59] Stadin [49] Buchtel [15] Fernandes [39] | Rubbio [59] Scharwz [65] Marutha [52] Varsi [60] Saleh [36] Öberg [48] | Kiberu [44] Elkefi [35] Rubbio [59] Scharwz [65] Varsi [60] Öberg [48] Buchtel [15] Fernandes [39] | Varsi [60] Öberg [48] | Anyanwu [43] | Kamenjasevic and Povse [40] Kiberu [44] Albarrak [45] Jensen and Kushniruk [42] Occelli and Scelfo [46] Tortorella [76] Loeb [47] Houwelingen [61] Ha and Nuntaboot [63] Vanagas [68] |
| Competence Type | S–C | P–A | |||||
|---|---|---|---|---|---|---|---|
| t1 | t2 | t3 | t4 | t5 | t6 | t7 | |
| Technical | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Methodological | 1 | 1 | 0 | 0 | 1 | 1 | 0 |
| Social | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Personal | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Competence Type | S–C | P–A | |||||
|---|---|---|---|---|---|---|---|
| t1 | t2 | t3 | t4 | t5 | t6 | t7 | |
| Technical | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Methodological | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Social | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Personal | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Competence Type | S–C | P–A | |||||
|---|---|---|---|---|---|---|---|
| t1 | t2 | t3 | t4 | t5 | t6 | t7 | |
| Technical | 2 | 4 | 1 | 1 | 2 | 1 | 1 |
| Methodological | 1 | 4 | 0 | 0 | 1 | 1 | 0 |
| Social | 1 | 4 | 1 | 1 | 2 | 1 | 1 |
| Personal | 1 | 4 | 1 | 1 | 1 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jose, A.; Tortorella, G.L.; Vassolo, R.; Kumar, M.; Mac Cawley, A.F. Professional Competence and Its Effect on the Implementation of Healthcare 4.0 Technologies: Scoping Review and Future Research Directions. Int. J. Environ. Res. Public Health 2023, 20, 478. https://doi.org/10.3390/ijerph20010478
Jose A, Tortorella GL, Vassolo R, Kumar M, Mac Cawley AF. Professional Competence and Its Effect on the Implementation of Healthcare 4.0 Technologies: Scoping Review and Future Research Directions. International Journal of Environmental Research and Public Health. 2023; 20(1):478. https://doi.org/10.3390/ijerph20010478
Chicago/Turabian StyleJose, Abey, Guilherme L. Tortorella, Roberto Vassolo, Maneesh Kumar, and Alejandro F. Mac Cawley. 2023. "Professional Competence and Its Effect on the Implementation of Healthcare 4.0 Technologies: Scoping Review and Future Research Directions" International Journal of Environmental Research and Public Health 20, no. 1: 478. https://doi.org/10.3390/ijerph20010478
APA StyleJose, A., Tortorella, G. L., Vassolo, R., Kumar, M., & Mac Cawley, A. F. (2023). Professional Competence and Its Effect on the Implementation of Healthcare 4.0 Technologies: Scoping Review and Future Research Directions. International Journal of Environmental Research and Public Health, 20(1), 478. https://doi.org/10.3390/ijerph20010478