
Designing a Needs-Oriented Psychological Intervention for Chinese Women Undergoing an Abortion
 , ,
, ,
Abstract
:1. Introduction
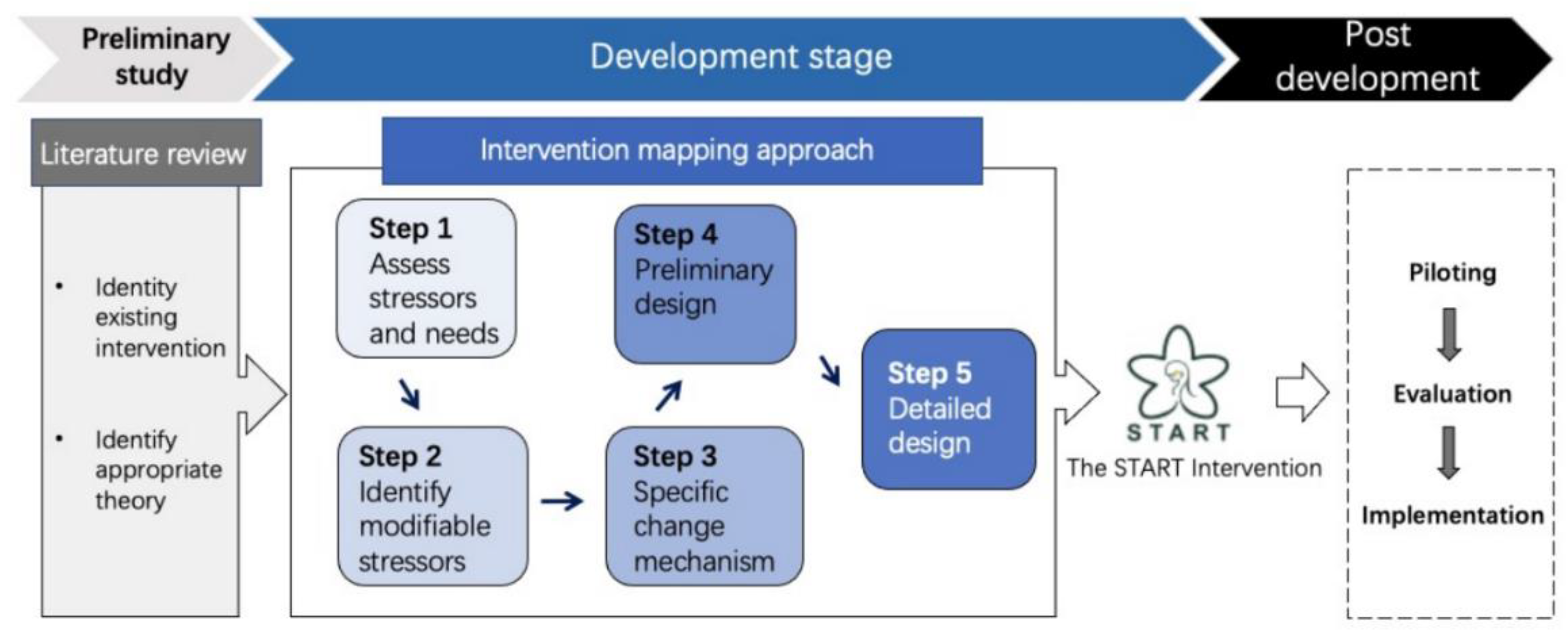
2. Methodology and Methods
2.1. Step 1: Assess Stressors and Needs
- Preparing: The dataset was reviewed by the first and fourth author for fitness for the current study based on a data-fitness assessment list for the second analysis of qualitative data (SAQD) guidelines [32] (see Supplementary File S2 for the assessment list of data fitness). After the two reviewers deemed the dataset was appropriate, an unstructured matrix informed by the aims of the study was developed by the first author (see Supplementary File S3 for the data analysis matrices);
- Organizing: The de-identified interview transcriptions were reviewed by the first and fourth authors (with detailed annotation) to gather relevant content according to the unstructured matrix. The content was grouped, and different categories were created within the matrix boundaries. Data abstraction was then undertaken. After the abstraction of each category, any discrepancies between reviewers were discussed with a third reviewer until a consensus was reached;
- Reporting: the first and the fourth author made a shared decision on how to model and report the results. To guarantee trustworthiness, details of the analysis process were recorded by all reviewers using a reflective memo. To preserve the original meaning of women’s statements, the preparing phase and organizing phase of data analysis was conducted in Chinese, and all three researchers involved were fluent Chinese speakers. The analysis matrices and reporting process were conducted bilingually to reduce potential bias and build a shared vision among the research team.
2.2. Step 2: Identify Modifiable Stressors
2.3. Step 3: Specific Change Mechanism
2.4. Step 4: Preliminary Design
2.5. Step 5: Detailed Design
3. Results
3.1. Step 1: Assess Stressors and Needs
3.2. Step 2: Identify Modifiable Stressors
3.3. Step 3: Specific Change Mechanism
3.4. Step 4: Preliminary Design
3.5. Step 5: Detailed Design
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bearak, J.; Popinchalk, A.; Ganatra, B.; Moller, A.B.; Tunçalp, Ö.; Beavin, C.; Kwok, L.; Alkema, L. Unintended pregnancy and abortion by income, region, and the legal status of abortion: Estimates from a comprehensive model for 1990–2019. Lancet Glob. Health 2020, 8, e1152–e1161. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, J.; Li, Y.; Zhou, Y.; Li, Y.; Zhao, R.; Tong, Q.; Luo, M. Changes in the prevalence of induced abortion in the floating population in major cities of China 2007–2014. Int. J. Environ. Res. Public Health 2019, 16, 3305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Wu, S.; Li, J.; Wang, K.; Xu, J.; Temmerman, M.; Zhang, W.-H. Post-abortion family planning counselling practice among abortion service providers in China: A nationwide cross-sectional study. Eur. J. Contracept. Reprod. Health Care 2017, 22, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Gao, L.; Anguzu, R.; Zhao, J. Long-acting reversible contraceptive use in the post-abortion period among women seeking abortion in mainland China: Intentions and barriers. Reprod. Health 2018, 15, 85. [Google Scholar] [CrossRef]
- WHO; Johns Hopkins Bloomberg School of Public Health. Family Planning: A Global Handbook for Providers; WHO: Geneva, Switzerland, 2018; pp. 319–324, 2018 update. [Google Scholar]
- World Health Organization. Clinical Practice Handbook for Safe Abortion; WHO Library Cataloguing: Geneva, Switzerland, 2014. [Google Scholar]
- Biggs, M.A.; Upadhyay, U.D.; McCulloch, C.E.; Foster, D.G. Women’s mental health and wellbeing 5 years after receiving or being denied an abortion: A prospective, longitudinal cohort study. JAMA Psychiatry 2017, 74, 169–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, D.G.; Biggs, M.A.; Ralph, L.; Gerdts, C.; Roberts, S.; Glymour, M.M. Socioeconomic Outcomes of Women Who Receive and Women Who Are Denied Wanted Abortions in the United States. Am. J. Public Health 2018, 108, 407–413. [Google Scholar] [PubMed]
- American Psychological Association. Report of the APA Task Force on Mental Health and Abortion; American Psychological Association: Washington, DC, USA, 2008. [Google Scholar]
- Hanschmidt, F.; Linde, K.; Hilbert, A.; Riedel-Heller, S.G.; Kersting, A. Abortion stigma: A systematic review. Perspect. Sex. Reprod. Health 2016, 48, 169–177. [Google Scholar] [CrossRef]
- Horvath, S.; Schreiber, C.A. Unintended Pregnancy, Induced Abortion, and Mental Health. Curr. Psychiatry Rep. 2017, 19, 77. [Google Scholar] [CrossRef]
- Pallitto, C.C.; O’Campo, P. Community level effects of gender inequality on intimate partner violence and unintended pregnancy in Colombia: Testing the feminist perspective. Soc. Sci. Med. 2005, 60, 2205–2216. [Google Scholar] [CrossRef]
- Dietz, P.M.; Spitz, A.M.; Anda, R.F.; Williamson, D.F.; McMahon, P.M.; Santelli, J.S.; Nordenberg, D.F.; Felitti, V.J.; Kendrick, J.S. Unintended pregnancy among adult women exposed to abuse or household dysfunction during their childhood. JAMA 1999, 282, 1359–1364. [Google Scholar] [CrossRef]
- Miller, E.; Decker, M.R.; McCauley, H.L.; Tancredi, D.J.; Levenson, R.R.; Waldman, J.; Schoenwald, P.; Silverman, J.G. Pregnancy coercion, intimate partner violence and unintended pregnancy. Contraception 2010, 81, 316–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Collaborating Centre for Mental Health. Induced Abortion and Mental Health: A Systematic Review of the Mental Health Outcomes of Induced Abortion, Including Their Prevalence and Associated Factors; Academy of Medical Royal Colleges: London, UK, 2011. [Google Scholar]
- Macapagal, K.; Janssen, E.; Matson, M.; Finn, P.R.; Heiman, J.R. The Impact of Gain- and Loss-Framed Messages on Young Adults’ Sexual Decision Making: An Experimental Study. Arch. Sex. Behav. 2017, 46, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Karasek, D. Reproductive Decision-Making under Uncertainty Exploring the Relationship of Economic Preferences and Reproductive Health; University of California: Berkeley, CA, USA, 2017. [Google Scholar]
- Ashton, L.; Giridhar, N.; Holcombe, S.J.; Madon, T.; Turner, E. A Review of Behavioral Economics in Reproductive Health; Global Action, Center for Effective: Berkeley, CA, USA, 2015. [Google Scholar]
- Wang, N.; Allen, J.; Gamble, J.; Creedy, D.K. Nonpharmacological interventions to improve the psychological well-being of women accessing abortion services and their satisfaction with care: A systematic review. Nurs. Health Sci. 2020, 22, 854–867. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Wei, W.; Gong, L. Rebuilding psychosocial competence for unmarried adolescent pregnancies using an integrated intervention. Int. J. Adolesc. Med. Health 2010, 22, 491–502. [Google Scholar] [CrossRef]
- Gurevitch, J.; Koricheva, J.; Nakagawa, S.; Stewart, G. Meta-analysis and the science of research synthesis. Nature 2018, 555, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Duncan, E.; O’Cathain, A.; Rousseau, N.; Croot, L.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance for reporting intervention development studies in health research (GUIDED): An evidence-based consensus study. BMJ Open 2020, 10, e033516. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Folkman, S. Stress: Appraisal and Coping; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Wethington, E.; Glanz, K.; Schwartz, M.D. Stress, Coping, and Health Behavior, in Health behavior: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 223–242. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G. Intervention mapping: A process for developing theory- and evidence-based health education programs. Health Educ. Behav. 1998, 25, 545–563. [Google Scholar] [CrossRef]
- Eldredge, L.K.; Markham, C.M.; Ruiter, R.A.; Fernández, M.E.; Kok, G.; Parcel, G.S. Planning Health Promotion Programs: An Intervention Mapping Approach; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Moon, Z.; Moss-Morris, R.; Hunter, M.S.; Hughes, L.D. Development of a self-management intervention to improve tamoxifen adherence in breast cancer survivors using an Intervention Mapping framework. Support. Care Cancer 2021, 29, 3329–3338. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. J. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- UK Data Service. Reusing Qualitative Data, Secondary Analysis; University of Essex: Colchester, UK, 2016; Available online: https://www.ukdataservice.ac.uk/use-data/secondary-analysis/reusing-qualitative-data (accessed on 7 October 2020).
- Flick, U. (Ed.) Data Collection in Secondary Analysis. In The SAGE Handbook of Qualitative Data Collection; SAGE Publications Ltd.: London, UK, 2018; pp. 164–181. [Google Scholar]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassam-Adams, N.; Marsac, M.L.; Kohser, K.L.; Kenardy, J.A.; March, S.; Winston, F.K. A new method for assessing content validity in model-based creation and iteration of eHealth interventions. J. Med. Internet Res. 2015, 17, e95. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Chen, N.-S.; Chen, G. Effects of teacher role on student engagement in WeChat-Based online discussion learning. Comput. Educ. 2020, 157, 103956. [Google Scholar] [CrossRef]
- Montag, C.; Becker, B.; Gan, C. The multipurpose application WeChat: A review on recent research. Front. Psychol. 2018, 9, 2247. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.L.; Börjesson, E.; Huber, A.; Mulligan, C. Abortion Care for Young Women a Training Toolkit; Ipas: Chapel Hill, NC, USA, 2011. [Google Scholar]
- Barak, A.; Grohol, J.M. Current and future trends in internet-supported mental health interventions. J. Technol. Hum. Serv. 2011, 29, 155–196. [Google Scholar] [CrossRef]
- Merckaert, I.; Lewis, F.; Delevallez, F.; Herman, S.; Caillier, M.; Delvaux, N.; Libert, Y.; Liénard, A.; Nogaret, J.-M.; Ogez, D.; et al. Improving anxiety regulation in patients with breast cancer at the beginning of the survivorship period: A randomized clinical trial comparing the benefits of single component and multiple component group interventions. Psycho-Oncol. 2017, 26, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Biggs, M.A.; Rowland, B.; E McCulloch, C.; Foster, D.G. Does abortion increase women’s risk for post-traumatic stress? Findings from a prospective longitudinal cohort study. BMJ Open 2016, 6, e009698. [Google Scholar] [CrossRef] [Green Version]
- van Ditzhuijzen, J.; Ten Have, M.; de Graaf, R.; Lugtig, P.; van Nijnatten, C.H.; Vollebergh, W.A. Long-term incidence and recurrence of common mental disorders after abortion. A Dutch prospective cohort study. J. Psychiatr. Res. 2018, 102, 132–135. [Google Scholar] [CrossRef] [PubMed]
- McSmith, D.; Börjesson, E.; Villa, L.; Turner, K.L. Exploring Abortion-A Collection of Self-Reflection and Sensitization Activities for Global Audiences; Ipas: Chapel Hill, NC, USA, 2011. [Google Scholar]
- Feng, L.; Zhang, T.; Wang, Q.; Xie, Y.; Peng, Z.; Zheng, J.; Qin, Y.; Zhang, M.; Lai, S.; Wang, D.; et al. Impact of COVID-19 outbreaks and interventions on influenza in China and the United States. Nat. Commun. 2021, 12, 3249. [Google Scholar] [CrossRef] [PubMed]
- Pietromonaco, P.R.; Overall, N.C. Applying relationship science to evaluate how the COVID-19 pandemic may impact couples’ relationships. Am. Psychol. 2021, 76, 438. [Google Scholar] [CrossRef]
- Agüero, J.M. COVID-19 and the rise of intimate partner violence. World Dev. 2021, 137, 105217. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ID | Age | Gestation (Week+Day) | Number of Abortions | Interview Timepoint | Interview Length (min) |
|---|---|---|---|---|---|
| 1 | 19 | 9+3 | 1 | 2 weeks post-abortion | 46 |
| 2 | 21 | 11+4 | 1 | 2 weeks post-abortion | 49 |
| 3 | 20 | 9+6 | 1 | 2 weeks post-abortion | 55 |
| 4 | 25 | 9+2 | 2 | 6 weeks post-abortion | 72 |
| 5 | 20 | 13+1 | 1 | 2 weeks post-abortion | 33 |
| 6 | 24 | 10 | 1 | 2 weeks post-abortion | 47 |
| 7 | 20 | 9+4 | 3 | 6 weeks post-abortion | 52 |
| 8 | 18 | 10+6 | 1 | 2 weeks post-abortion | 59 |
| 9 | 21 | 10+2 | 1 | 2 weeks post-abortion | 40 |
| 10 | 24 | 12 | 2 | 6 weeks post-abortion | 59 |
| 11 | 20 | 9+4 | 1 | 6 weeks post-abortion | 48 |
| 12 | 18 | 10+1 | 1 | 2 weeks post-abortion | 46 |
| 13 | 18 | 12+4 | 1 | 2 weeks post-abortion | 35 |
| 14 | 29 | 11+6 | 2 | 6 weeks post-abortion | 49 |
| Time Frame | Stressors | Needs | Support Preferences |
|---|---|---|---|
| First appointment |
|
|
|
| During abortion |
|
|
|
| Post-abortion |
|
|
|
| Whole process |
|
|
|
| Modifiable Stressors | General Determinants | Change Strategies/Mechanisms |
|---|---|---|
| Pressure deciding about an abortion |
|
|
| Concerns about the abortion procedures (pain and bleeding symptoms) |
| |
| Possibility of being discharged before feeling ready |
| |
| Desire to be “back to normal” in the context of having an abortion |
| |
| Possibility of a repeat unintended pregnancy or abortion |
| |
| Keep the abortion a secret |
|
| Components | Who | How | Where | When and How Much |
|---|---|---|---|---|
| Instructional Support | The first author |
|
|
|
| Informational Support | The first author |
|
|
|
| Communication Channel | A registered nurse |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, N.; Creedy, D.K.; Zhang, M.; Lu, H.; Elder, E.; Allen, J.; Guo, L.; Xiao, Q.; Gamble, J. Designing a Needs-Oriented Psychological Intervention for Chinese Women Undergoing an Abortion. Int. J. Environ. Res. Public Health 2023, 20, 782. https://doi.org/10.3390/ijerph20010782
Wang N, Creedy DK, Zhang M, Lu H, Elder E, Allen J, Guo L, Xiao Q, Gamble J. Designing a Needs-Oriented Psychological Intervention for Chinese Women Undergoing an Abortion. International Journal of Environmental Research and Public Health. 2023; 20(1):782. https://doi.org/10.3390/ijerph20010782
Chicago/Turabian StyleWang, Na, Debra K. Creedy, Mingna Zhang, Hong Lu, Elizabeth Elder, Jyai Allen, Li Guo, Qian Xiao, and Jenny Gamble. 2023. "Designing a Needs-Oriented Psychological Intervention for Chinese Women Undergoing an Abortion" International Journal of Environmental Research and Public Health 20, no. 1: 782. https://doi.org/10.3390/ijerph20010782