
Dietary and Physical Activity Habits as Conditioning Factors of Nutritional Status among Children of GENYAL Study

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Anthropometric Data
2.3. Dietary Data
2.4. Physical Activity Data
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nutrition—EU Science Hub—European Commission. EU Science Hub. Available online: https://ec.europa.eu/jrc/en/research-topic/nutrition (accessed on 12 July 2021).
- Townsend, N.; Rutter, H.; Foster, C. Evaluating the evidence that the prevalence of childhood overweight is plateauing. Pediatr. Obes. 2012, 7, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Childhood Obesity Surveillance Initiative (COSI) Factsheet. Highlights 2015-17 (2018). Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/activities/who-european-childhood-obesity-surveillance-initiative-cosi/cosi-publications/childhood-obesity-surveillance-initiative-cosi-factsheet.-highlights-2015-17-2018 (accessed on 12 July 2021).
- Resumen de la Cuarta Ronda COSI (2015–2017) de la Oficina Regional Para Europa de la OMS y Cmparación con los Resultados de ALADINO 2019. Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Ministerio de Sanidad, Servicios Sociales e Igualdad. 2021. Available online: https://www.aesan.gob.es/AECOSAN/docs/documentos/nutricion/observatorio/RESULTADOS_4_INFORME_COSI_2105_2017_NAOS.pdf (accessed on 7 October 2022).
- Kunwar, R.; Minhas, S.; Mangla, V. Is obesity a problem among school children? Indian J. Public Health 2018, 62, 153. [Google Scholar] [PubMed]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity—Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, J. Physical activity and obesity. Lancet 2004, 363, 182. [Google Scholar] [CrossRef]
- Verduci, E.; Di Profio, E.; Fiore, G.; Zuccotti, G. Integrated Approaches to Combatting Childhood Obesity. Ann. Nutr. Metab. 2022, 78 (Suppl. S2), 8–19. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Bo, A.P.; Castell, G.S. Hábitos Alimentarios y Estilos de Vida en Niños/as y Adolescentes. In Libro Blanco de la Nutrición Infantil en España; Prensas de la Universidad de Zaragoza: Zaragoza, España, 2015; pp. 315–324. [Google Scholar]
- Fundación para la Investigación Nutricional (FIN). Informe 2016: Actividad Física en Niños y Adolescentes en España. 2016. Available online: https://www.observatoriodelainfancia.es/oia/esp/documentos_ficha.aspx?id=5056 (accessed on 24 July 2022).
- Paduano, S.; Greco, A.; Borsari, L.; Salvia, C.; Tancredi, S.; Pinca, J.; Midili, S.; Tripodi, A.; Borella, P.; Marchesi, I. Physical and Sedentary Activities and Childhood Overweight/Obesity: A Cross-Sectional Study among First-Year Children of Primary Schools in Modena, Italy. Int. J. Environ. Res. Public Health 2021, 18, 3221. [Google Scholar] [CrossRef]
- Paduano, S.; Borsari, L.; Salvia, C.; Arletti, S.; Tripodi, A.; Pinca, J.; Borella, P. Risk Factors for Overweight and Obesity in Children Attending the First Year of Primary Schools in Modena, Italy. J. Community Health 2020, 45, 301–309. [Google Scholar] [CrossRef]
- Zhu, X.; Haegele, J.A.; Tang, Y.; Wu, X. Prevalence and Demographic Correlates of Overweight, Physical Activity, and Screen Time Among School-Aged Children in Urban China: The Shanghai Study. Asia Pac. J. Public Health 2018, 30, 118–127. [Google Scholar] [CrossRef]
- Gerber, M.; Lang, C.; Beckmann, J.; du Randt, R.; Long, K.Z.; Müller, I.; Nienaber, M.; Probst-Hensch, N.; Steinmann, P.; Pühse, U.; et al. Physical Activity, Sedentary Behaviour, Weight Status, and Body Composition among South African Primary Schoolchildren. Int. J. Environ. Res. Public Health. 2022, 19, 11836. [Google Scholar] [CrossRef]
- Gracia-Arnaiz, M.; Kraemer, F.B.; Demonte, F.C. Acting against obesity: A cross-cultural analysis of prevention models in Spain, Argentina and Brazil. Crit. Rev. Food Sci. Nutr. 2022, 62, 2192–2204. [Google Scholar] [CrossRef]
- Estudio EsNuPi 2022. Available online: https://www.estudioesnupi.org/ (accessed on 16 December 2022).
- Qué es el Programa Thao? Programa Thao-Salud Infantil. 2016. Available online: https://programathao.com/que-es/ (accessed on 16 December 2022).
- Gómez, S.F.; Casas, R.; Palomo, V.T.; Pujol, A.M.; Fitó, M.; Schroder, H. Study protocol: Effects of the THAO-child health intervention program on the prevention of childhood obesity—The POIBC study. BMC Pediatr. 2014, 14, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, A.; Marfell-Jones, M. International Society for Advancement of Kinanthropometry. In International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E. Estudio de Crecimiento de Bilbao. Curvas y Tablas de Crecimiento. Estudio Transversal; Fundación Faustino Orbegozo Eizaguirre: Bilbao, Spain, 2011. [Google Scholar]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- WHO. Growth Reference Data for 5–19 Years 2018. Available online: http://www.who.int/growthref/en/ (accessed on 22 February 2022).
- European Food Safety Authority. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar] [CrossRef]
- FAO. Energy and Protein Requirements. Available online: http://www.fao.org/docrep/003/aa040e/aa040e00.htm (accessed on 28 August 2022).
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Ortega, R.; Requejo, A.; López-Sobaler, A. Modelos de Cuestionario de Actividad. In Nutriguía Manual de Nutrición Clínica en Atención Primaria. 2006; Editorial Médica Panamericana: Madrid, Spain, 2015; p. 468. [Google Scholar]
- WHO. Physical Status: The Use and Interpretation of Anthropometry. 2018. Available online: http://www.who.int/childgrowth/publications/physical_status/en/ (accessed on 22 February 2022).
- Institute of Medicine of the National Academies. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. 2002. Available online: https://www.nap.edu/catalog/10490/dietary-reference-intakes-for-energy-carbohydrate-fiber-fat-fatty-acids-cholesterol-protein-and-amino-acids (accessed on 22 February 2022).
- WHO. Physical Activity and Young People. 2018. Available online: http://www.who.int/dietphysicalactivity/factsheet_young_people/en/ (accessed on 16 July 2022).
- Murakami, K.; Livingstone, M.B.E.; Okubo, H.; Sasaki, S. Younger and older ages and obesity are associated with energy intake underreporting but not overreporting in Japanese boys and girls aged 1–19 years: The National Health and Nutrition Survey. Nutr. Res. 2016, 36, 1153–1161. [Google Scholar] [CrossRef]
- Schoeller, D.A.; Thomas, D.; Archer, E.; Heymsfield, S.B.; Blair, S.N.; Goran, M.I.; Hill, J.O.; Atkinson, R.L.; Corkey, B.E.; Foreyt, J.; et al. Self-report–based estimates of energy intake offer an inadequate basis for scientific conclusions. Am. J. Clin. Nutr. 2013, 97, 1413–1415. [Google Scholar] [CrossRef] [Green Version]
- Wallace, A.; Kirkpatrick, S.I.; Darlington, G.; Haines, J. Accuracy of Parental Reporting of Preschoolers’ Dietary Intake Using an Online Self-Administered 24-h Recall. Nutrients 2018, 10, 987. [Google Scholar] [CrossRef] [Green Version]
- Koning, M.; de Jong, A.; de Jong, E.; Visscher, T.L.S.; Seidell, J.C.; Renders, C.M. Agreement between parent and child report of physical activity, sedentary and dietary behaviours in 9–12-year-old children and associations with children’s weight status. BMC Psychol. 2018, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Navia Lomban, B.; Ortega Anta, R.M. Ingestas Recomendadas de Energía y Nutrientes. In NutriguíaR Manual de Nutrición Clínica. 2a; Editorial Médica Panamericana: Madrid, Spain, 2015; pp. 3–26. [Google Scholar]
- Anibes. Available online: http://www.fen.org.es/anibes/es/distribucion_de_macronutrientes (accessed on 10 September 2022).
- Arnesen, E.K.; Thorisdottir, B.; Lamberg-Allardt, C.; Bärebring, L.; Nwaru, B.; Dierkes, J.; Ramel, A.; Åkesson, A. Protein intake in children and growth and risk of overweight or obesity: A systematic review and meta-analysis. Food Nutr. Res. 2022, 21, 66. [Google Scholar] [CrossRef]
- Naude, C.E.; Visser, M.E.; Nguyen, K.A.; Durao, S.; Schoonees, A. Effects of total fat intake on bodyweight in children. Cochrane Database Syst. Rev. 2018, 7, CD012960. [Google Scholar] [CrossRef]
- Wadolowska, L.; Ulewicz, N.; Sobas, K.; Wuenstel, J.W.; Slowinska, M.A.; Niedzwiedzka, E.; Czlapka-Matyasik, M. Dairy-Related Dietary Patterns, Dietary Calcium, Body Weight and Composition: A Study of Obesity in Polish Mothers and Daughters, the MODAF Project. Nutrients 2018, 10, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koca, T.; Akcam, M.; Serdaroglu, F.; Dereci, S. Breakfast habits, dairy product consumption, physical activity, and their associations with body mass index in children aged 6–18. Eur. J. Pediatr. 2017, 176, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Dougkas, A.; Barr, S.; Reddy, S.; Summerbell, C.D. A critical review of the role of milk and other dairy products in the development of obesity in children and adolescents. Nutr. Res. Rev. 2019, 32, 106–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondin, S.A.; Anzman-Frasca, S.; Djang, H.C.; Economos, C.D. Breakfast consumption and adiposity among children and adolescents: An updated review of the literature. Pediatr. Obes. 2016, 11, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Rosato, V.; Edefonti, V.; Parpinel, M.; Milani, G.P.; Mazzocchi, A.; Decarli, A.; Agostoni, C.; Ferraroni, M. Energy Contribution and Nutrient Composition of Breakfast and Their Relations to Overweight in Free-living Individuals: A Systematic Review. Adv. Nutr. 2016, 7, 455–465. [Google Scholar] [CrossRef] [Green Version]
- García Cabrera, S.; Herrera Fernández, N.; Rodríguez Hernández, C.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. KIDMED test; prevalence of low adherence to the Mediterranean Diet in children and young: A systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Commission on Ending Childhood Obesity. Report of the Commission on Ending Childhood Obesity. 2017. Available online: https://apps.who.int/iris/handle/10665/259349 (accessed on 16 December 2022).
- Schröder, H.; Mendez, M.A.; Ribas-Barba, L.; Covas, M.-I.; Serra-Majem, L. Mediterranean diet and waist circumference in a representative national sample of young Spaniards. Int. J. Pediatr. Obes. 2010, 5, 516–519. [Google Scholar] [CrossRef]
- Pérez-Farinós, N.; Villar-Villalba, C.; Sobaler, A.M.L.; Dal Re Saavedra, M.Á.; Aparicio, A.; Santos Sanz, S.; Robledo de Dios, T.; Castrodeza-Sanz, J.J.; Ortega Anta, R.M. The relationship between hours of sleep, screen time and frequency of food and drink consumption in Spain in the 2011 and 2013 ALADINO: A cross-sectional study. BMC Public Health 2017, 17, 33. [Google Scholar] [CrossRef] [Green Version]
- Domingues-Montanari, S. Clinical and psychological effects of excessive screen time on children. J. Paediatr. Child Health 2017, 53, 333–338. [Google Scholar] [CrossRef]
- Felső, R.; Lohner, S.; Hollódy, K.; Erhardt, É.; Molnár, D. Relationship between sleep duration and childhood obesity: Systematic review including the potential underlying mechanisms. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 751–761. [Google Scholar] [CrossRef]


{kind=link}
| Total | Girls | Boys | |||||
|---|---|---|---|---|---|---|---|
| N | x ± SD | N | x ± SD | N | x ± SD | p | |
| Height (cm) | 221 | 124.74 ± 6.41 | 105 | 123.75 ± 6.63 | 116 | 125.63 ± 6.10 | 0.029 |
| Weight (kg) | 221 | 26.60 ± 6.03 | 105 | 26.37 ± 6.07 | 116 | 26.81 ± 6.00 | 0.555 |
| Fat mass (%) | 218 | 20.59 ± 7.17 | 103 | 20.50 ± 7.60 | 115 | 20.67 ± 6.80 | 0.635 |
| BMI (kg/m2) | 221 | 16.92 ± 2.63 | 105 | 17.04 ± 2.73 | 116 | 16.82 ± 2.55 | 0.448 |
| IPAC | 198 | 1.58 ± 0.11 | 92 | 1.57 ± 0.09 | 106 | 1.60 ± 0.12 | 0.054 |
| Sleeping hours | 198 | 9.92 ± 1.09 | 92 | 9.92 ± 1.19 | 106 | 9.92 ± 1.00 | 0.938 |
| TAWH (h) | 221 | 3.74 ± 1.81 | 105 | 3.46 ± 1.62 | 116 | 4.03 ± 1.94 | 0.025 |
| TEE (kJ/day) | 198 | 7256.02 ± 1000.69 | 92 | 7103.49 ± 975.32 | 106 | 7388.40 ± 1008.10 | 0.029 |
| TEI (kJ/day) | 201 | 7755.46 ± 1407.94 | 93 | 7582.32 ± 1286.16 | 108 | 7894.91 ± 1494.10 | 0.125 |
| CHD (% TEI) | 201 | 44.48 ± 5.30 | 93 | 44.43 ± 5.73 | 108 | 44.53 ± 4.93 | 0.900 |
| Simple sugars (% TEI) | 201 | 20.15 ± 4.08 | 93 | 20.17 ± 3.63 | 108 | 20.13 ± 4.45 | 0.539 |
| Vegetable fibre (g) | 201 | 18.17 ± 5.82 | 93 | 17.76 ± 5.73 | 108 | 18.52 ± 5.91 | 0.185 |
| Proteins (% TEI) | 201 | 16.55 ± 2.17 | 93 | 16.60 ± 2.16 | 108 | 16.51 ± 2.18 | 0.778 |
| Fats (% TEI) | 201 | 38.96 ± 5.02 | 93 | 38.96 ± 5.44 | 108 | 38.95 ± 4.65 | 0.987 |
| SFA (% TEI) | 201 | 13.29 ± 2.27 | 93 | 13.25 ± 2.35 | 108 | 13.33 ± 2.20 | 0.806 |
| MFA (% TEI) | 201 | 17.23 ± 3.25 | 93 | 17.20 ± 3.49 | 108 | 17.25 ± 3.04 | 0.927 |
| PFA (% TEI) | 201 | 4.84 ± 1.50 | 93 | 4.83 ± 1.57 | 108 | 4.85 ± 1.44 | 0.826 |
| Cereals and grains (s/d) | 201 | 4.05 ± 1.45 | 93 | 3.95 ± 1.59 | 108 | 4.15±1.32 | 0.069 |
| Vegetables (s/d) | 201 | 2.48 ± 1.05 | 93 | 2.51 ± 1.13 | 108 | 2.46 ± 0.98 | 0.722 |
| Fruits (s/d) | 201 | 1.42 ± 0.93 | 93 | 1.46 ± 0.95 | 108 | 1.39 ± 0.91 | 0.689 |
| Milk and dairy products (s/d) | 201 | 2.61 ± 0.80 | 93 | 2.59 ± 0.76 | 108 | 2.63 ± 0.84 | 0.850 |
| Meats, fish and eggs (s/d) | 201 | 2.45 ± 0.90 | 93 | 2.46 ± 0.91 | 108 | 2.44 ± 0.91 | 0.881 |
| KIDMED index | 200 | 6.50 ± 1.91 | 93 | 6.51 ± 1.93 | 107 | 6.50 ± 1.90 | 0.863 |
| Normal Weight (n = 154) | Overweight (n = 36) | Obesity (n = 20) | p | |
|---|---|---|---|---|
| TEI (kJ/day) | 7783.26 ± 1394.20 | 7816.76 ± 1339.78 | 7268.28 ± 1632.85 | 0.308 |
| CHD (%TEI) | 44.42 ± 5.41 | 44.63 ± 5.01 | 44.58 ± 4.92 | 0.997 |
| Simple sugar (%TEI) | 19.91 ± 3.97 | 20.63 ± 4.69 | 21.39 ± 3.89 | 0.310 |
| Fiber (%TEI) | 18.14 ± 5.59 | 18.74 ± 7.35 | 16.96 ± 4.67 | 0.731 |
| Fats (%TEI) | 38.90 ± 5.06 | 39.44 ± 4.94 | 38.55 ± 4.86 | 0.815 |
| PFA (%TEI) | 4.75 ± 1.43 | 5.20 ± 1.67 | 5.02 ± 1.75 | 0.286 |
| MFA (%TEI) | 17.18 ± 3.27 | 17.42 ± 3.14 | 17.26 ± 3.29 | 0.928 |
| SFA (%TEI) | 13.37 ± 2.22 | 13.20 ± 2.56 | 12.77 ± 2.20 | 0.598 |
| Proteins (%TEI) | 16.67 ± 2.20 | 15.92 ± 2.08 | 16.86 ± 2.08 | 0.193 |
| Cereals and grains (s/d) | 4.12 ± 1.47 | 4.02 ± 1.50 | 3.45 ± 0.98 | 0.249 |
| Vegetables (s/d) | 2.45 ± 1.05 | 2.46 ± 1.22 | 2.65 ± 0.92 | 0.768 |
| Fruits (s/d) | 1.38 ± 0.92 | 1.49 ± 0.90 | 1.74 ± 1.01 | 0.331 |
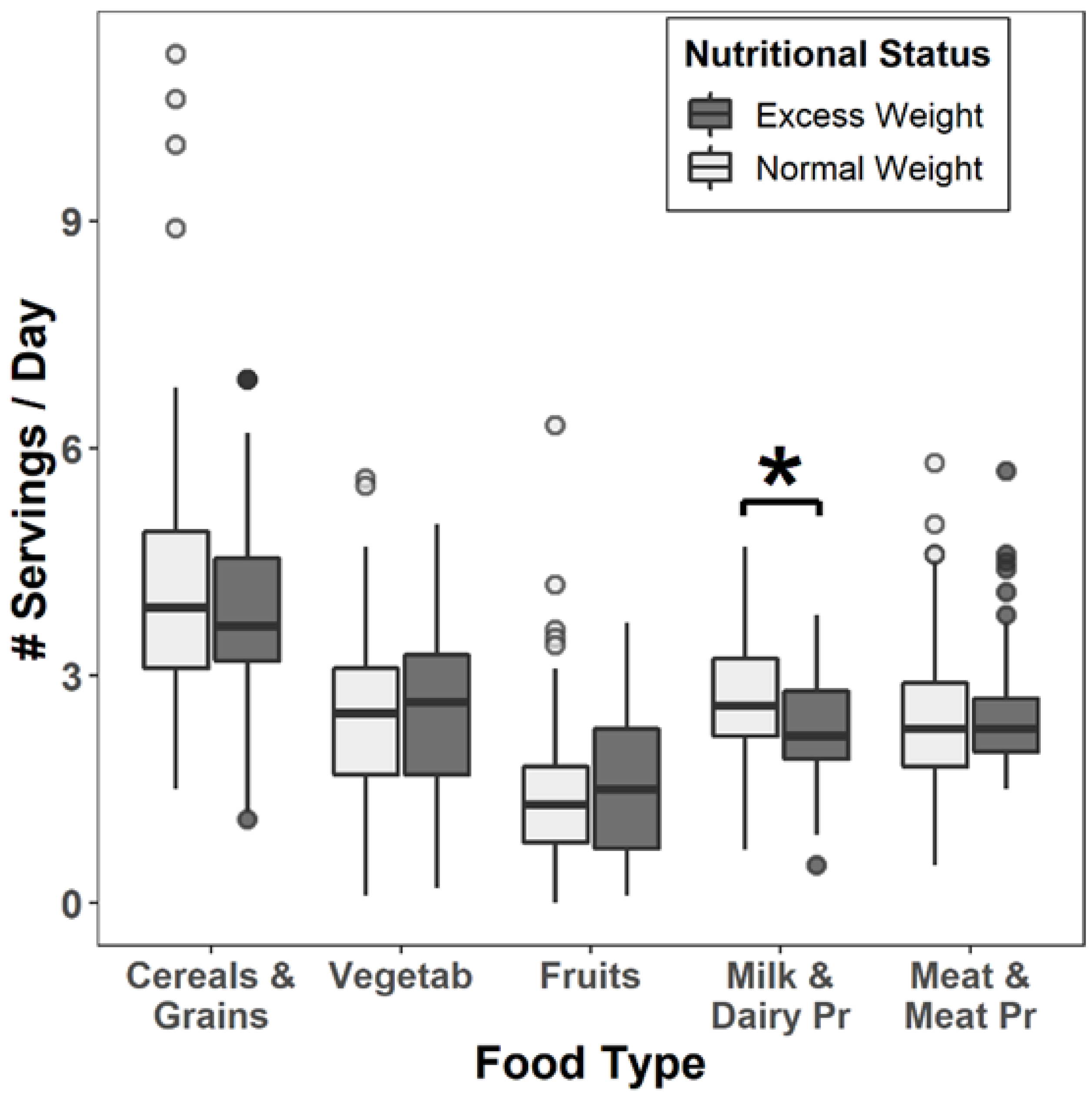
| Milk and dairy products (s/d) | 2.70 ± 0.80 | 2.30 ± 0.76 | 2.29 ± 0.67 | 0.011 † |
| Meat and meat products (s/d) | 2.42 ± 0.89 | 2.47 ± 0.83 | 2.75 ± 1.11 | 0.697 |
| Normal Weight (n = 156) | Overweight (n = 31) | Obesity (n = 15) | p | |
|---|---|---|---|---|
| IPAC | 1.58 ± 0.11 | 1.57 ± 0.08 | 1.62 ± 0.15 | 0.489 |
| Sleep length (hours) | 9.88 ± 1.06 | 10.29 ± 1.20 | 9.61 ± 1.00 | 0.050 |
| TAWH (hours) | 3.75 ± 1. 73 | 3.64 ± 2.06 | 4.05 ± 2.07 | 0.601 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcos-Pasero, H.; Aguilar-Aguilar, E.; Colmenarejo, G.; Ramírez de Molina, A.; Reglero, G.; Loria-Kohen, V. Dietary and Physical Activity Habits as Conditioning Factors of Nutritional Status among Children of GENYAL Study. Int. J. Environ. Res. Public Health 2023, 20, 866. https://doi.org/10.3390/ijerph20010866
Marcos-Pasero H, Aguilar-Aguilar E, Colmenarejo G, Ramírez de Molina A, Reglero G, Loria-Kohen V. Dietary and Physical Activity Habits as Conditioning Factors of Nutritional Status among Children of GENYAL Study. International Journal of Environmental Research and Public Health. 2023; 20(1):866. https://doi.org/10.3390/ijerph20010866
Chicago/Turabian StyleMarcos-Pasero, Helena, Elena Aguilar-Aguilar, Gonzalo Colmenarejo, Ana Ramírez de Molina, Guillermo Reglero, and Viviana Loria-Kohen. 2023. "Dietary and Physical Activity Habits as Conditioning Factors of Nutritional Status among Children of GENYAL Study" International Journal of Environmental Research and Public Health 20, no. 1: 866. https://doi.org/10.3390/ijerph20010866
APA StyleMarcos-Pasero, H., Aguilar-Aguilar, E., Colmenarejo, G., Ramírez de Molina, A., Reglero, G., & Loria-Kohen, V. (2023). Dietary and Physical Activity Habits as Conditioning Factors of Nutritional Status among Children of GENYAL Study. International Journal of Environmental Research and Public Health, 20(1), 866. https://doi.org/10.3390/ijerph20010866