

Health Workers’ Burnout and COVID-19 Pandemic: 1-Year after—Results from a Repeated Cross-Sectional Survey

Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis of Data
2.2. Data Processing and Ethical Evaluation Survey
3. Results
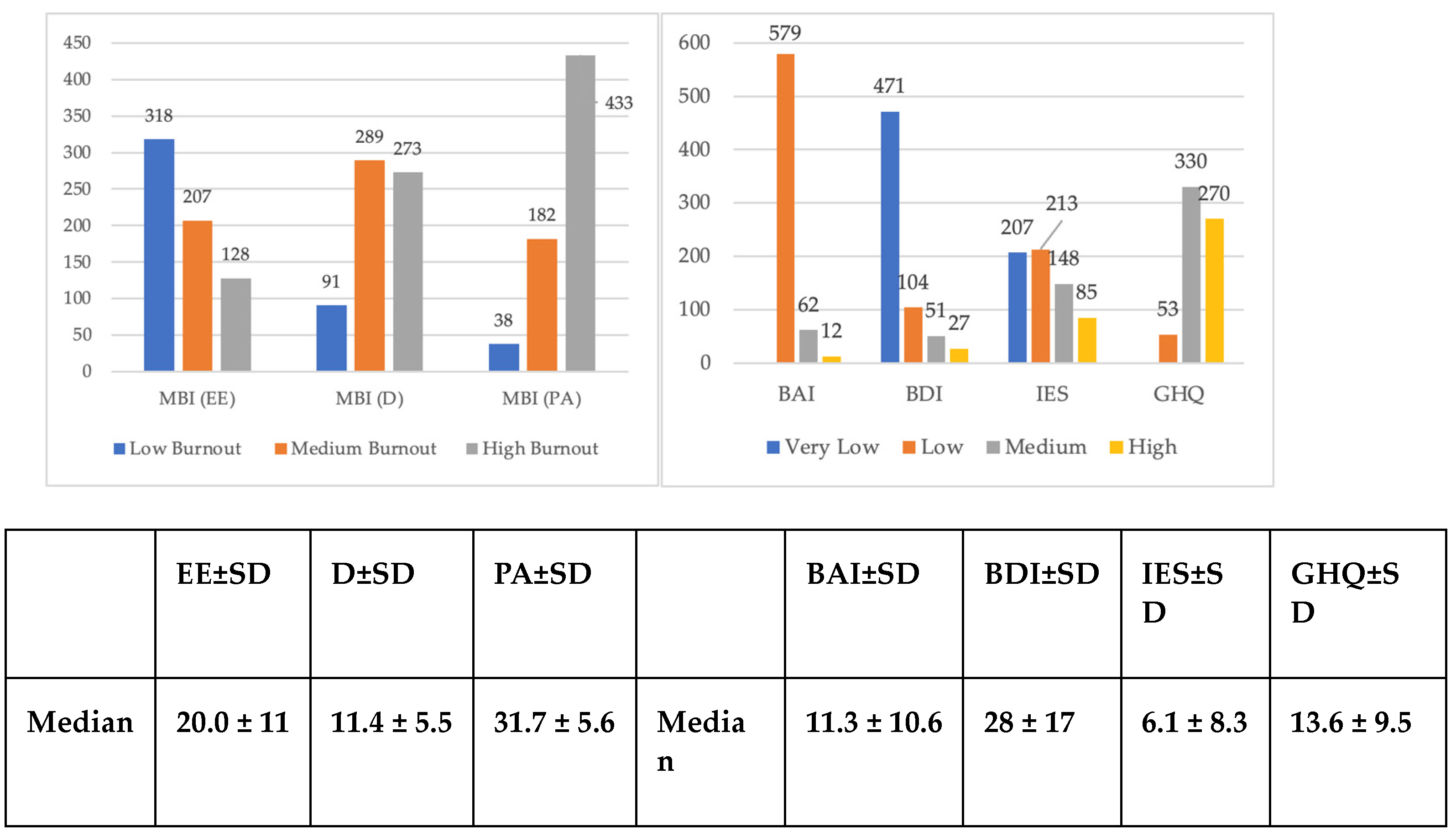
3.1. Description of the First Assessment
3.2. Description of the Second Assessment—1 Year after
3.2.1. Burnout
3.2.2. Anxiety, Depression and Post-Traumatic Stress Symptoms
3.2.3. Mental Health in HWs
3.2.4. Categorical Data Analysis based on Biographical data (n, % Column) during the Second Phase
4. Discussion
4.1. Discussion of the Results
4.1.1. Burnout
4.1.2. Anxiety, Depression, and Stress
4.1.3. Mental Health in HWs
4.2. Limitations and Strengths: Possible Future Developments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 19 November 2021).
- Hao, Q.; Wang, D.; Xie, M.; Tang, Y.; Dou, Y.; Zhu, L.; Wu, Y.; Dai, M.; Wu, H.; Wang, Q. Prevalence and Risk Factors of Mental Health Problems Among Healthcare Workers During the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 567381. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Creed, F. Stress and psychiatric disorder in healthcare professionals and hospital staff. Lancet 2000, 355, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Sonali, R. World Failing in ‘Our Duty of Care’ to Protect Mental Health and Well-Being of Health and Care Workers, Finds Report on Impact of COVID-19. Available online: https://www.who.int/news/item/05-10-2022-world-failing-i—-our-duty-of-car—-to-protect-mental-health-and-wellbeing-of-health-and-care-worker—-finds-report-on-impact-of-covid-19 (accessed on 28 May 2023).
- Cochrane Effective Practice and Organisation of Care Group; Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst. Rev. 2020, 11, CD013779. [Google Scholar] [PubMed]
- De Hert, S. Burnout in Healthcare Workers: Prevalence, Impact and Preventative Strategies. Local Reg. Anesth. 2020, 13, 171–183. [Google Scholar] [CrossRef]
- Kafle, B.; Bagale, Y.; Kafle, S.; Parajuli, A.; Pandey, S. Depression, Anxiety and Stress among Healthcare Workers during COVID-19 Pandemic in a Tertiary Care Centre of Nepal: A Descriptive Cross-sectional Study. JNMA J. Nepal Med. Assoc. 2021, 59, 239–242. [Google Scholar] [CrossRef]
- Sung, C.W.; Chen, C.H.; Fan, C.Y.; Chang, J.H.; Hung, C.C.; Fu, C.M.; Wong, L.P.; Huang, E.P.; Lee, T.S. Mental health crisis in healthcare providers in the COVID-19 pandemic: A cross-sectional facility-based survey. BMJ Open 2021, 11, e052184. [Google Scholar] [CrossRef]
- Sahin, T.; Aslaner, H.; Eker, O.O.; Gokcek, M.B.; Dogan, M. Effect of COVID-19 pandemic on anxiety and burnout levels in emergency healthcare workers: A questionnaire study. Res. Square 2020, 12, 987. [Google Scholar] [CrossRef]
- Kannampallil, T.G.; Goss, C.W.; Evanoff, B.A.; Strickland, J.R.; McAlister, R.P.; Duncan, J. Exposure to COVID-19 patients increases physician trainee stress and burnout. PLoS ONE 2020, 15, e0237301. [Google Scholar] [CrossRef]
- Ulbrichtova, R.; Svihrova, V.; Tatarkova, M.; Svihra, J., Jr.; Novak, M.; Hudeckova, H. Prevalence of Burnout Syndrome in COVID-19 and Non-COVID-19 Units in University Hospital: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12664. [Google Scholar] [CrossRef]
- Gramaglia, C.M.; Marangon, D.; Azzolina, D.; Guerriero, C.; Lorenzini, L.; Probo, M.; Rudoni, M.; Gambaro, E.; Zeppegno, P. The Mental Health Impact of 2019-nCOVID on Healthcare Workers From North-Eastern Piedmont, Italy. Focus on Burnout. Front. Public Health 2021, 9, 667379. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Damico, V.; Murano, L.; Demoro, G.; Russello, G.; Cataldi, G.; D’Alessandro, A. Burnout syndrome among Italian nursing staff during the COVID 19 emergency. Multicenter fact-finding survey. Prof. Inferm. 2020, 73, 250–257. [Google Scholar]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting—A Systematic Review. J. Occup. Health 2020, 62, E12175. [Google Scholar] [CrossRef]
- Jalili, M.; Niroomand, M.; Hadavand, F.; Zeinali, K.; Fotouhi, A. Burnout among healthcare professionals during COVID-19 pandemic: A cross-sectional study. Int. Arch. Occup. Environ. Health 2021, 94, 1345–1352. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef]
- de Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Buchner, D.M.; Cress, M.E.; Esselman, P.C.; Margherita, A.J.; de Lateur, B.J.; Campbell, A.J.; Wagner, E.H. Factors Associated With Changes in Gait Speed in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1996, 51, M297–M302. [Google Scholar] [CrossRef]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi Zhonghua Laodong Weisheng Zhiyebing Zazhi Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, 192–195. [Google Scholar]
- Shalev, A.; Liberzon, I.; Marmar, C. Post-Traumatic Stress Disorder. N. Engl. J. Med. 2017, 376, 2459–2469. [Google Scholar] [CrossRef]
- Benfante, A.; Di Tella, M.; Romeo, A.; Castelli, L. Traumatic Stress in Healthcare Workers During COVID-19 Pandemic: A Review of the Immediate Impact. Front. Psychol. 2020, 11, 569935. [Google Scholar] [CrossRef] [PubMed]
- Carmassi, C.; Bertelloni, C.A.; Avella, M.T.; Cremone, I.; Massimetti, E.; Corsi, M.; Dell’Osso, L. PTSD and Burnout are Related to Lifetime Mood Spectrum in Emergency Healthcare Operator. Clin. Pract. Epidemiol. Ment. Health CP EMH 2020, 16, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Couette, M.; Mouchabac, S.; Bourla, A.; Nuss, P.; Ferreri, F. Social cognition in post-traumatic stress disorder: A systematic review. Br. J. Clin. Psychology 2020, 59, 117–138. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.I.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, E15–E16. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Gambaro, E.; Gramaglia, C.; Marangon, D.; Azzolina, D.; Probo, M.; Rudoni, M.; Zeppegno, P. The Mediating Role of Gender, Age, COVID-19 Symptoms and Changing of Mansion on the Mental Health of Healthcare Workers Operating in Italy during the First Wave of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 13083. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.; Leiter, M. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of event scale: A measure of participantive stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D. Manual of the General Health Questionnaire; NFER: Windsor, ON, Canada, 1978; 32p. [Google Scholar]
- van Mol, M.M.C.; Kompanje, E.J.O.; Benoit, D.D.; Bakker, J.; Nijkamp, M.D. The Prevalence of Compassion Fatigue and Burnout among Healthcare Professionals in Intensive Care Units: A Systematic Review. PLoS ONE 2015, 10, e0136955. [Google Scholar] [CrossRef]
- Padula, M.S.; Ilari, G.; Baraldi, S.; Guaraldi, G.P.; Ferretti, E.; Musiani, V.; Svampa, E.; Venuta, M. Il burnout nella Medicina Generale: Personalità del medico e personalità del paziente. Riv. Della Soc. Ital. Med. Gen. 2008, 4, 42–47. [Google Scholar]
- Maslach, C.; Jackson, S. Maslach Burnout Inventory; Consulting Psychologists Press, Inc.: Palo Alto, CA, USA, 1981. [Google Scholar]
- Tang, R.; Feng, O.; Chong, J.J.; Wang, A. Evaluating the impact of coronavirus disease on burnout among healthcare workers using maslach burnout inventory tool: A systematic review. Proc. Singap. Healthc. 2022, 31, 20101058221117390. [Google Scholar] [CrossRef]
- Morse, G.; Salyers, M.P.; Rollins, A.L.; Monroe-DeVita, M.; Pfahler, C. Burnout in Mental Health Services: A Review of the Problem and Its Remediation. Adm. Policy Ment. Health Ment. Health Serv. Res. 2012, 39, 341–352. [Google Scholar] [CrossRef] [Green Version]
- Di Monte, C.; Monaco, S.; Mariani, R.; Di Trani, M. From Resilience to Burnout: Psychological Features of Italian General Practitioners During COVID-19 Emergency. Front. Psychol. 2020, 11, 2476. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, C.; Pan, W.; Zheng, J.; Gao, J.; Huang, X.; Cai, S.; Zhai, Y.; Latour, J.M.; Zhu, C. Stress, Burnout, and Coping Strategies of Frontline Nurses During the COVID-19 Epidemic in Wuhan and Shanghai, China. Front. Psychiatry 2020, 11, 1154. [Google Scholar] [CrossRef]
- Orrù, G.; Marzetti, F.; Conversano, C.; Vagheggini, G.; Miccoli, M.; Ciacchini, R.; Panait, E.; Gemignani, A. Secondary Traumatic Stress and Burnout in Healthcare Workers during COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2021, 18, 337. [Google Scholar] [CrossRef]
- Lasalvia, A.; Amaddeo, F.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Bonetto, C. Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: A cross-sectional study in a tertiary hospital of a highly burdened area of north-east Italy. BMJ Open 2021, 11, E045127. [Google Scholar] [CrossRef]
- Huo, L.; Zhou, Y.; Li, S.; Ning, Y.; Zeng, L.; Liu, Z.; Qian, W.; Yang, J.; Zhou, X.; Liu, T.; et al. Burnout and Its Relationship with Depressive Symptoms in Medical Staff During the COVID-19 Epidemic in China. Front. Psychol. 2021, 12, 616369. [Google Scholar] [CrossRef]
- Liu, X.; Chen, J.; Wang, D.; Li, X.; Wang, E.; Jin, Y.; Ma, Y.; Yu, C.; Luo, C.; Zhang, L.; et al. COVID-19 Outbreak Can Change the Job Burnout in Health Care Professionals. Front. Psychiatry 2020, 11, 1362. [Google Scholar] [CrossRef]
- Alsulimani, L.K.; Farhat, A.M.; Borah, R.A.; AlKhalifah, J.A.; Alyaseen, S.M.; Alghamdi, S.M.; Bajnaid, M.J. Health care worker burnout during the COVID-19 pandemic. Saudi Med. J. 2021, 42, 306–314. [Google Scholar] [CrossRef]
- Duarte, I.; Teixeira, A.; Castro, L.; Marina, S.; Ribeiro, C.; Jácome, C.; Martins, V.; Ribeiro-Vaz, I.; Pinheiro, H.C.; Silva, A.R.; et al. Burnout among Portuguese healthcare workers during the COVID-19 pandemic. BMC Public Health 2020, 20, 1885. [Google Scholar] [CrossRef] [PubMed]
- Khasne, R.W.; Dhakulkar, B.S.; Mahajan, H.C.; Kulkarni, A.P. Burnout among Healthcare Workers during COVID-19 Pandemic in India: Results of a Questionnaire-based Survey. Indian J. Crit. Care Med. Peer Rev. Off. Publ. Indian Soc. Crit. Care Med. 2020, 24, 664–671. [Google Scholar]
- Meynaar, I.A.; Ottens, T.; Zegers, M.; van Mol, M.M.C.; van der Horst, I.C.C. Burnout, resilience and work engagement among Dutch intensivists in the aftermath of the COVID-19 crisis: A nationwide survey. J. Crit. Care 2021, 62, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; De Waele, J.; Ferrer, R.; Staudinger, T.; Borkowska, M.; Povoa, P.; Iliopoulou, K.; Artigas, A.; Schaller, S.J.; Hari, M.S.; et al. Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann. Intensive Care 2020, 10, 110. [Google Scholar] [CrossRef] [PubMed]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Dimitriu, M.C.T.; Pantea-Stoian, A.; Smaranda, A.C.; Nica, A.A.; Carap, A.C.; Constantin, V.D.; Socea, B. Burnout syndrome in Romanian medical residents in time of the COVID-19 pandemic. Medical Hypotheses 2020, 144. [Google Scholar] [CrossRef]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Zhu, J. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. eClinicalMedicine 2020, 24, 100424. [Google Scholar] [CrossRef]
- Arora, M.; Asha, S.; Chinnappa, J.; Diwan, A.D. Review article: Burnout in emergency medicine physicians. Emerg. Med. Australas. 2013, 25, 491–495. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, J.; Luo, C.; Hu, S.; Lin, X.; Anderson, A.E.; Qian, Y. A Comparison of Burnout Frequency among Oncology Physicians and Nurses Working on the Frontline and Usual Wards During the COVID-19 Epidemic in Wuhan, China. J. Pain Symptom Manag. 2020, 60, e60–e65. [Google Scholar] [CrossRef]
- Torrente, M.; Sousa, P.A.; Sánchez-Ramos, A.; Pimentao, J.; Royuela, A.; Franco, F.; Collazo-Lorduy, A.; Menasalvas, E.; Provencio, M. To burn-out or not to burn-out: A cross-sectional study in healthcare professionals in Spain during COVID-19 pandemic. BMJ Open 2021, 11, E044945. [Google Scholar] [CrossRef]
- Chen, R.; Sun, C.; Chen, J.J.; Jen, H.J.; Kang, X.L.; Kao, C.C.; Chou, K.R. A Large-Scale Survey on Trauma, Burnout, and Posttraumatic Growth among Nurses during the COVID-19 Pandemic. Int. J. Ment. Health Nurs. 2021, 30, 102–116. [Google Scholar] [CrossRef]
- Abdelhafiz, A.S.; Ali, A.; Ziady, H.H.; Maaly, A.M.; Alorabi, M.; Sultan, E.A. Prevalence, Associated Factors, and Consequences of Burnout Among Egyptian Physicians During COVID-19 Pandemic. Front. Public Health 2020, 8, 590190. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Burnout Syndrome Among Hospital Healthcare Workers During the COVID-19 Pandemic and Civil War: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 579563. [Google Scholar] [CrossRef]
- Dillon, E.C.; Stults, C.D.; Deng, S.; Martinez, M.; Szwerinski, N.; Koenig, P.T.; Gregg, L.; Cobb, J.K.; Mahler, E.; Frosch, D.L.; et al. Women, Younger Clinician’’, and Caregiver’’ Experiences of Burnout and Well-being During COVID-19 in a US Healthcare System. J. Gen. Intern. Med. 2002, 37, 145–153. [Google Scholar] [CrossRef]
- Leo, C.G.; Sabina, S.; Tumolo, M.R.; Bodini, A.; Ponzini, G.; Sabato, E.L.; Mincarone, P. Burnout among Healthcare Workers in the COVID 19 Era: A Review of the Existing Literature. Front. Public Health 2021, 9, 750529. [Google Scholar] [CrossRef]
- Çelmeçe, N.; Menekay, M. The Effect of Stress, Anxiety and Burnout Levels of Healthcare Professionals Caring for COVID-19 Patients on Their Quality of Life. Front. Psychol. 2020, 11, 597624. [Google Scholar] [CrossRef]
- Pniak, B.; Leszczak, J.; Adamczyk, M.; Rusek, W.; Matłosz, P.; Guzik, A. Occupational burnout among active physiotherapists working in clinical hospitals during the COVID-19 pandemic in south-eastern Poland. Work 2021, 68, 285–295. [Google Scholar] [CrossRef]
- Grigorescu, S.; Cazan, A.M.; Rogozea, L.; Grigorescu, D.O. Predictive Factors of the Burnout Syndrome Occurrence in the Healthcare Workers During the COVID-19 Pandemic. Front. Med. 2022, 9, 842457. [Google Scholar] [CrossRef]
- Asai, M.; Morita, T.; Akechi, T.; Sugawara, Y.; Fujimori, M.; Akizuki, N.; Nakano, T.; Uchitomi, Y. Burnout and psychiatric morbility among physicians engaged in end-to-life care for cancer patients: A cross-sectional nationwide survey in Japan. Psychooncology 2007, 16, 421–428. [Google Scholar] [CrossRef]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Sauta, M.D.; Lochner, P.; Tondo, G.; Bragazzi, N.L.; et al. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of North-West Italy. BJPsych Open 2021, 7, e27. [Google Scholar] [CrossRef]
- Cyr, S.; Marcil, M.J.; Houchi, C.; Marin, M.F.; Rosa, C.; Tardif, J.C.; Guay, S.; Guertin, M.C.; Genest, C.; Forest, J.; et al. Evolution of burnout and psychological distress in healthcare workers during the COVID-19 pandemic: A 1-year observational study. BMC Psychiatry 2022, 22, 809. [Google Scholar] [CrossRef] [PubMed]
- Biber, J.; Ranes, B.; Lawrence, S.; Malpani, V.; Trinh, T.T.; Cyders, A.; English, S.; Staub, C.L.; McCausland, K.L.; Kosinski, M.; et al. Mental health impact on healthcare workers due to the COVID-19 pandemic: A U.S. cross-sectional survey study. J. Patient-Rep. Outcomes 2022, 6, 63. [Google Scholar] [CrossRef] [PubMed]
- Pala, A.N.; Chuang, J.C.; Chien, A.; Krauth, D.M.; Leitner, S.A.; Okoye, N.M.; Costello, S.C.; Rodriguez, R.M.; Sheira, L.A.; Solomon, G.; et al. Depression, anxiety, and burnout among hospital workers during the COVID-19 pandemic: A cross-sectional study. PLoS ONE 2022, 17, e0276861. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.; Zielinski, M.J.; Thompson, R.G., Jr.; Willis, D.E.; Purvis, R.S.; McElfish, P.A. “This Pandemic Is Making Me More Anxious about My Welfare and the Welfare of Others:” COVID-19 Stressors and Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 5680. [Google Scholar] [CrossRef]
- Adams, J.G.; Walls, R.M. Supporting the Health Care Workforce During the COVID-19 Global Epidemic. JAMA 2020, 323, 1439–1440. [Google Scholar] [CrossRef] [Green Version]
- Hwang, S.; Kwon, K.T.; Lee, S.H.; Kim, S.W.; Chang, H.H.; Kim, Y.; Bae, S.; Cheong, H.S.; Park, S.Y.; Kim, B.; et al. Correlates of burnout among healthcare workers during the COVID-19 pandemic in South Korea. Sci. Rep. 2023, 13, 3360. [Google Scholar] [CrossRef]
- Kalin, N.H. The Critical Relationship Between Anxiety and Depression. Am. J. Psychiatry 2020, 177, 365–367. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| N = 653 | Categories | N |
|---|---|---|
| Age (mean age = 44.28 years) | >50 years | 227 (35%) |
| 30–49 years | 334 (51%) | |
| 18–29 years | 92 (14%) | |
| Gender | Female | 443 (68%) |
| Marital status | Married/cohabiting | 413 (63%) |
| Lives alone | 240 (37%) | |
| Sons | Yes | 358 (55%) |
| Job category | Doctor | 286 (44%) |
| Nurse | 137 (21%) | |
| Other | 131 (20%) | |
| Resident doctor | 99 (15%) | |
| Change in job? | Yes | 331 (51%) |
| Changing family habits? | Yes | 564 (86%) |
| Have you tested positive for COVID-19? | No | 564 (86%) |
| Did you have any symptoms related to COVID-19? | No | 528 (81%) |
| Have you had any health problems that are unrelated to COVID-19? | No | 556 (85%) |
| Has anyone dear to you tested positive for the virus? | No | 454 (70%) |
| N = 688 | Categories | N |
|---|---|---|
| Age (mean age = 43.99 years) | >50 years | 165 (35%) |
| 30–49 years | 245 (53%) | |
| 18–29 years | 55 (12%) | |
| Gender | Female | 316 (68%) |
| Marital status | Married/cohabiting | 354 (76%) |
| Lives alone | 111 (24%) | |
| Sons | Yes | 257 (55%) |
| Have you tested positive for COVID-19? | No | 343 (74%) |
| Have you had symptoms related to COVID-19? | No | 338 (73%) |
| Have you had health problems unrelated to COVID-19? | No | 368 (80%) |
| Has anyone dear to you tested positive for COVID-19? | Yes | 253 (54%) |
| Changing family habits? | Yes | 399 (86%) |
| Change in job during emergency? | No | 249 (54%) |
| Did you participate in the previous edition of the survey? | Yes | 287 (62%) |
| Job category | Doctor | 143 (31%) |
| Nurse | 130 (28%) | |
| Resident in training | 63 (13%) | |
| Freelance doctor | 38 (8%) | |
| Other | 91 (20%) | |
| Do you carry out urgent or emergent activities? | Yes | 187 (40%) |
| Area | Clinic | 196 (42%) |
| Surgical | 66 (14%) | |
| Services | 102 (22%) | |
| Emergency/Urgency | 101 (22%) | |
| Have you ever been followed by a specialist psychiatrist? | Yes | 56 (12%) |
| Have you taken psychopharmacological therapy in the past? | Yes | 72 (16%) |
| Are you currently followed by a mental health specialist? | Yes | 29 (6%) |
| Do you currently take psychopharmacological therapy? | Yes | 36 (7%) |
| Did you feel protected in the workplace during the pandemic? | Yes | 108 (23%) |
| No | 98 (21%) | |
| Not always | 259 (56%) | |
| Do you think you have had the correct number of PPE available during your work? | Yes | 174 (37%) |
| No | 77 (17%) | |
| Not always | 214 (46%) | |
| Do you think you have had a correct number of works shifts in the context of COVID-19-related work? | Yes | 258 (55%) |
| No | 97 (21%) | |
| Not always | 110 (24%) | |
| How has the COVID-19 emergency influenced the number of working hours? | Stable | 169 (59%) |
| Decreased | 22 (5%) | |
| Increased | 274 (36%) | |
| Have you had the COVID-19 vaccine? | Yes | 451 (97%) |
| N = 688 | OVER CUT OFF—EE | OVER CUT OFF—D | OVER CUT OFF—PA | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off Subscale, N Participants | ≤17 N = 393 | 18–29 N = 139 | ≥30 N = 156 | p | ≤05 N = 238 | 06–11 N = 196 | ≥12 N = 254 | p | ≤34 N = 538 | 35–39 N = 114 | ≥40 N = 36 | p | |
| Burnout Level | Low | Middle | High | Low | Middle | High | High | Middle | Low | ||||
| Marital status (I) | Unmarried | 15% (39) | 22% (30) | 22% (34) | 0.049 | 17% (18) | 16% (31) | 21% (54) | 0.026 | ||||
| Married | 55% (144) | 46% (64) | 47% (73) | 56% (61) | 57% (111) | 43% (109) | |||||||
| Divorced | 7% (18) | 6% (8) | 1% (2) | 6% (7) | 7% (13) | 3% (8) | |||||||
| Cohabiting | 13% (34) | 18% (25) | 22% (35) | 11% (12) | 13% (26) | 22% (56) | |||||||
| Widower | 0% (1) | 1% (1) | 1% (1) | 0% (0) | 1% (1) | 1% (2) | |||||||
| In relation | 10% (26) | 8% (11) | 7% (11) | 9% (10) | 7% (13) | 10% (25) | |||||||
| Living situation (II) | Lives alone | 22% (88) | 33% (37) | 25% (9) | 0.048 | ||||||||
| Cohabit | 78% (320) | 67% (76) | 75% (27) | ||||||||||
| Have children | Yes | 59% (155) | 50% (70) | 47% (74) | 0.044 | 58% (63) | 63% (122) | 45% (114) | <0.001 | ||||
| No | 41% (107) | 50% (69) | 53% (82) | 42% (45) | 37% (73) | 55% (140) | |||||||
| Non-COVID 19 related health issues | Yes | 18% (46) | 17% (24) | 33% (51) | <0.001 | ||||||||
| No | 82% (215) | 83% (115) | 67% (105) | ||||||||||
| Change habits due to the pandemic | Yes | 78% (205) | 89% (124) | 92% (144) | <0.001 | 79% (85) | 82% (159) | 90% (229) | 0.005 | ||||
| No | 22% (57) | 11% (15) | 8% (12) | 21% (23) | 18% (36) | 10% (25) | |||||||
| Change habits due to the fear of infecting loved ones | Yes | 87% (74) | 89% (141) | 95% (218) | 0.02 | ||||||||
| No | 13% (11) | 11% (18) | 5% (11) | ||||||||||
| Change in job | Yes | 33% (87) | 53% (73) | 58% (90) | <0.001 | 24% (26) | 42% (81) | 56% (143) | <0.001 | ||||
| No | 67% (175) | 47% (66) | 42% (66) | 76% (82) | 58% (114) | 44% (111) | |||||||
| Participation in the first survey | Yes | 54% (140) | 70% (96) | 67% (103) | 0.004 | ||||||||
| No | 46% (117) | 30% (42) | 33% (51) | ||||||||||
| Type HW | General practitioners | 25% (66) | 35% (48) | 30% (47) | 0.027 | 22% (24) | 27% (52) | 33% (85) | 0.004 | 28% (116) | 32% (36) | 25% (9) | 0.046 |
| Nurse | 32% (83) | 22% (30) | 22% (35) | 31% (33) | 35% (69) | 18% (46) | 28% (114) | 24% (27) | 19% (7) | ||||
| Residents in Training | 15% (38) | 19% (26) | 10% (15) | 12% (13) | 11% (22) | 17% (44) | 15% (60) | 14% (16) | 8% (3) | ||||
| Freelance doctors | 9% (24) | 6% (9) | 10% (15) | 8% (9) | 8% (16) | 9% (23) | 7% (28) | 10% (11) | 25% (9) | ||||
| Other | 19% (51) | 19% (26) | 28% (44) | 27% (29) | 18% (36) | 22% (56) | 22% (90) | 20% (23) | 22% (8) | ||||
| Medical area | Clinic | 37% (95) | 47% (65) | 51% (78) | 0.001 | 34% (35) | 40% (76) | 50% (127) | 0.005 | 40% (160) | 58% (64) | 39% (14) | 0.033 |
| Surgical | 11% (28) | 20% (27) | 12% (19) | 9% (9) | 15% (29) | 14% (36) | 14% (57) | 9% (10) | 19% (7) | ||||
| Services | 27% (69) | 17% (23) | 22% (34) | 31% (32) | 27% (51) | 17% (43) | 25% (102) | 15% (17) | 19% (7) | ||||
| Emergency/Urgency | 26% (66) | 16% (22) | 14% (22) | 27% (28) | 19% (36) | 18% (46) | 20% (82) | 18% (20) | 22% (8) | ||||
| Never been followed by psychiatrist | Yes | 11% (28) | 7% (10) | 17% (27) | 0.02 | ||||||||
| No | 89% (232) | 93% (129) | 83% (128) | ||||||||||
| Past psychopharmacologic treatments | Yes | 12% (30) | 12% (17) | 23% (35) | 0.005 | ||||||||
| No | 88% (228) | 88% (122) | 77% (119) | ||||||||||
| Noncurrent psychopharmacological treatment | Yes | 4% (10) | 9% (12) | 12% (19) | 0.005 | ||||||||
| No | 96% (250) | 91% (125) | 88% (136) | ||||||||||
| Feeling protected at work | Yes | 36% (94) | 17% (23) | 8% (12) | <0.001 | 37% (40) | 27% (53) | 14% (36) | <0.001 | ||||
| No | 11% (28) | 20% (27) | 38% (60) | 7% (8) | 12% (24) | 33% (83) | |||||||
| Not always | 53% (139) | 64% (87) | 54% (84) | 55% (59) | 60% (117) | 53% (134) | |||||||
| Enough PPE available | Yes | 44% (114) | 37% (50) | 24% (37) | <0.001 | 43% (46) | 40% (78) | 31% (77) | <0.001 | ||||
| No | 11% (28) | 12% (17) | 31% (48) | 9% (10) | 11% (22) | 24% (61) | |||||||
| Not always | 45% (118) | 51% (69) | 46% (71) | 47% (50) | 48% (94) | 45% (114) | |||||||
| Sufficient work shifts | Yes | 44% (114) | 37% (50) | 24% (37) | <0.001 | 75% (80) | 64% (124) | 41% (102) | <0.001 | ||||
| No | 11% (28) | 12% (17) | 31% (48) | 2% (2) | 12% (24) | 34% (86) | |||||||
| Not always | 45% (118) | 51% (69) | 46% (71) | 23% (24) | 23% (45) | 25% (63) | |||||||
| Working hours | Stable | 47% (122) | 32% (44) | 27% (42) | <0.001 | 51% (55) | 42% (82) | 28% (71) | <0.001 | ||||
| Decreased | 5% (12) | 6% (8) | 3% (4) | 3% (3) | 5% (10) | 4% (11) | |||||||
| Increased | 49% (127) | 62% (86) | 70% (109) | 46% (49) | 53% (102) | 68% (171) | |||||||
| Vaccine for COVID-19 | Yes | 98% (398) | 98% (110) | 89% (32) | 0.009 | ||||||||
| No | 2% (10) | 2% (2) | 11% (4) | ||||||||||
| N = 688 | MBI—EE | MBI—D | MBI—PA | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off Subscale, N Participants | ≤17 N = 393 | 18–29 N = 139 | ≥30 N = 156 | p | ≤05 N = 238 | 06–11 N = 196 | ≥12 N = 254 | p | ≤34 N = 538 | 35–39 N = 114 | ≥40 N = 36 | p | |
| Burnout Level | Low | Middle | High | Low | Middle | High | High | Middle | Low | ||||
| BAI | Minimum (0–21) | 95% (215) | 86% (115) | 64% (96) | <0.001 | 95% (69) | 89% (170) | 77% (187) | <0.001 | ||||
| Medium (22–35) | 4% (9) | 11% (15) | 22% (33) | 5% (4) | 8% (16) | 15% (37) | |||||||
| High (>36) | 1% (2) | 2% (3) | 13% (20) | 0% (0) | 3% (5) | 8% (20) | |||||||
| BDI | Minimal (0–13) | ||||||||||||
| Low (14–19) | |||||||||||||
| Moderate (20–28) | |||||||||||||
| High (29–63) | |||||||||||||
| IES | Subclinical (0–8) | 85% (336) | 59% (82) | 47% (73) | <0.001 | 93% (222) | 68% (133) | 54% (136) | <0.001 | ||||
| Mild (9–25) | 13% (50) | 37% (52) | 40% (63) | 6% (15) | 27% (52) | 39% (98) | |||||||
| Moderate (26–43) | 2% (6) | 3% (4) | 10% (16) | 0% (1) | 4% (8) | 7% (17) | |||||||
| Severe (>44) | 0% (1) | 1% (1) | 3% (4) | 0% (0) | 2% (3) | 1% (3) | |||||||
| GHQ | No problem (0–14) | 55% (217) | 17% (24) | 13% (20) | <0.001 | 76% (182) | 20% (39) | 16% (40) | <0.001 | 42% (227) | 21% (24) | 28% (10) | <0.001 |
| Some problems (15–19) | 36% (141) | 40% (55) | 19% (29) | 22% (52) | 46% (90) | 33% (83) | 29% (158) | 43% (49) | 50% (18) | ||||
| Several problems (20–36) | 9% (35) | 43% (60) | 69% (107) | 2% (4) | 34% (67) | 52% (131) | 28% (153) | 36% (41) | 22% (8) | ||||
| N = 688 | BAI | BDI | IES | GHQ | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off Subscale N Participants | Minimum ≤21 N = 426 | Medium 22–35 N = 57 | High ≥36 N = 25 | p | Minimal 0–13 N = 186 | Medium 14–19 N = 20 | High ≥ 20 N = 482 | p | Subclinical 0–8 N = 491 | Mild 9–25 N = 165 | Moderate 26–43 N = 26 | Severe ≥43 N = 6 | p | No Problem 0–14 N = 261 | Some Problems 15–19 N = 225 | Several Problems 20–36 N = 202 | p | |
| Gender | Male | 34% (144) | 19% (11) | 20% (5) | 0.037 | |||||||||||||
| Female | 66% (281) | 81% (46) | 80% (20) | |||||||||||||||
| Living situation (II) | Lives alone | 24% (86) | 21% (35) | 35% (9) | 67% (4) | 0.04 | ||||||||||||
| Cohabits | 76% (274) | 79% (130) | 65% (17) | 33% (2) | ||||||||||||||
| Marital status (I) | Unmarried | 19% (68) | 15% (25) | 23% (6) | 67% (4) | 0.039 | ||||||||||||
| Married | 51% (183) | 51% (84) | 46% (12) | 33% (2) | ||||||||||||||
| Divorced | 5% (17) | 5% (9) | 8% (2) | 0% (0) | ||||||||||||||
| Cohabiting | 15%(53) | 22 (36) | 19% (5) | 0% (0) | ||||||||||||||
| Widower | 0% (1) | 1% (1) | 4% (1) | 0% (0) | ||||||||||||||
| In relation | 11%(38) | 6% (10) | 0% (0) | 0% (0) | ||||||||||||||
| Have children | Yes | 54% (231) | 63% (36) | 32% (8) | 0.033 | 43% (56) | 61% (137) | 52% (106) | 0.005 | |||||||||
| No | 46% (194) | 37% (21) | 68% (17) | 57% (74) | 39% (88) | 48% (96) | ||||||||||||
| Non-COVID 19 related health issues | Yes | 17% (74) | 37% (21) | 40% (10) | <0.001 | 37% (20) | 45% (9) | 19% (92) | <0.001 | 21% (27) | 14% (32) | 31% (62) | <0.001 | |||||
| No | 83% (351) | 63% (36) | 60% (15) | 63% (34) | 55% (11) | 81% (390) | 79% (102) | 86% (193) | 69% (140) | |||||||||
| Changed habits due to the pandemic | Yes | 81% (293) | 91% (150) | 92% (24) | 100% (6) | 0.016 | 78% (101) | 84% (188) | 91% (184) | 0.003 | ||||||||
| No | 19% (67) | 9% (15) | 8% (2) | 0% (0) | 22% (29) | 16% (37) | 9% (18) | |||||||||||
| Change in job | Yes | 38% (49) | 40% (90) | 55% (111) | 0.001 | |||||||||||||
| No | 62% (81) | 60% (135) | 45% (91) | |||||||||||||||
| HW Job Categories | Doctor | 32% (137) | 19% (11) | 16% (4) | 0.013 | 18% (10) | 25% (5) | 30% (146) | 0.011 | 19% (25) | 29% (65) | 35% (71) | 0.045 | |||||
| Nurse | 27% (114) | 30% (17) | 28% (7) | 20% (11) | 15% (3) | 28% (134) | 25% (32) | 30% (67) | 24% (49) | |||||||||
| Resident in training | 15% (64) | 11% (6) | 8% (2) | 15% (8) | 5% (1) | 15% (70) | 18% (24) | 14% (32) | 11% (23) | |||||||||
| Freelance doctor | 9% (37) | 9% (5) | 4% (1) | 9% (5) | 10% (2) | 9% (41) | 9% (12) | 7% (16) | 10% (20) | |||||||||
| Other | 17% (73) | 32% (18) | 44% (11) | 38% (21) | 45% (9) | 19% (91) | 28% (37) | 20% (45) | 19% (39) | |||||||||
| Emergency professions | No | 41% (175) | 35% (20) | 16% (4) | 0.032 | 20% (11) | 20% (4) | 40% (194) | 0.004 | |||||||||
| Yes | 59% (248) | 65% (37) | 84% (21) | 80% (43) | 80% (16) | 60% (286) | ||||||||||||
| Medical area | Clinic | 44% (23) | 58% (11) | 43% (204) | 0.025 | 41% (52) | 39% (87) | 50% (99) | 0.049 | |||||||||
| Surgical | 10% (5) | 5% (1) | 14% (68) | 13% (16) | 12% (28) | 15% (30) | ||||||||||||
| Services | 38% (20) | 26% (5) | 21% (101) | 29% (37) | 25% (57) | 16% (32) | ||||||||||||
| Emergency/ xcvbUrgency | 8% (4) | 11% (2) | 22% (104) | 17% (21) | 23% (52) | 19% (37) | ||||||||||||
| Past psychopharmacological treatment | Yes | 12% (49) | 32% (18) | 25% (6) | <0.001 | 11% (40) | 20% (33) | 27% (7) | 33% (2) | 0.007 | ||||||||
| No | 88% (374) | 68% (39) | 75% (18) | 89% (316) | 80% (130) | 73% (19) | 67% (4) | |||||||||||
| Followed by psychiatrist in the present | Yes | 11% (6) | 20% (4) | 5% (24) | 0.007 | |||||||||||||
| No | 89% (49) | 80% (16) | 95% (455) | |||||||||||||||
| Current psychopharmacological treatment | Yes | 5% (23) | 16% (9) | 12% (3) | 0.01 | 13% (7) | 25% (5) | 6% (29) | 0.002 | |||||||||
| No | 95% (397) | 84% (48) | 88% (22) | 87% (48) | 75% (15) | 94% (448) | ||||||||||||
| Feeling protected at work | Yes | 25% (105) | 12% (7) | 8% (2) | <0.001 | 28% (102) | 14% (23) | 12% (3) | 17% (1) | <0.001 | 32% (41) | 28% (62) | 13% (26) | <0.001 | ||||
| No | 17% (74) | 32% (18) | 44% (11) | 16% (57) | 30% (49) | 31% (8) | 17% (1) | 15% (19) | 17% (37) | 29% (59) | ||||||||
| Not always | 58% (245) | 55% (31) | 48% (12) | 56% (199) | 56% (92) | 58% (15) | 67% (4) | 53% (69) | 56% (125) | 58% (116) | ||||||||
| Sufficient availability of PPE | Yes | 39% (164) | 27% (15) | 24% (6) | <0.001 | 41% (147) | 27% (45) | 23% (6) | 50% (3) | 0.008 | 40% (51) | 43% (97) | 26% (53) | 0.003 | ||||
| No | 13% (57) | 32% (18) | 36% (9) | 13% (47) | 23% (37) | 31% (8) | 17% (1) | 14% (18) | 13% (30) | 22% (45) | ||||||||
| Not always | 48% (202) | 41% (23) | 40% (10) | 46% (162) | 50% (82) | 46% (12) | 33% (2) | 46% (59) | 43% (96) | 51% (103) | ||||||||
| Sufficient work shifts | Yes | 58% (246) | 44% (24) | 32% (8) | 0.033 | 61% (215) | 47% (76) | 42% (11) | 67% (4) | 0.036 | 60% (75) | 69% (154) | 38% (77) | <0.001 | ||||
| No | 19% (82) | 29% (16) | 36% (9) | 17% (61) | 27% (44) | 27% (7) | 0% (0) | 15% (19) | 13% (30) | 32% (63) | ||||||||
| Not always | 23% (96) | 27% (15) | 32% (8) | 22% (79) | 26% (43) | 31% (8) | 33% (2) | 25% (32) | 18% (40) | 30% (60) | ||||||||
| Working hours | Stable | 46% (59) | 42% (93) | 28% (56) | 0.006 | |||||||||||||
| Decreased | 2% (3) | 5% (11) | 5% (10) | |||||||||||||||
| Increased | 52% (67) | 54% (120) | 67% (135) | |||||||||||||||
| OR | CI (95%) | x-Square | Df | p | |||
|---|---|---|---|---|---|---|---|
| GHQ | Non-COVID 19 related health issues | Yes vs. No | 17.678 | 11.946–26.159 | 8.12 | 1 | <0.001 |
| Changed habits due to the pandemic | No vs. Yes | 0.476 | 0.310–0.732 | 11.45 | 1 | <0.001 | |
| BDI | Non-COVID 19 related health issues | Yes vs. No | 0.428 | 0.236–0.775 | 7.84 | 1 | 0.01 |
| IES | Gender | Male vs. Female | 0.475 | 0.266–0.849 | 6.3 | 1 | 0.01 |
| Non-COVID 19 related health issues | Yes vs. No | 28.677 | 17.261–47.644 | 16.64 | 1 | <0.001 | |
| BAI | Changed habits due to the pandemic | No vs. Yes | 0.411 | 0.234–0.720 | 9.65 | 1 | <0.001 |
| OVER CUTOFF-D | Age | <33 vs. >54 | 0.520 | 0.392–0.688 | 20.82 | 1 | <0.001 |
| Have children | No vs. Yes | 17.061 | 12.428–23.421 | 10.92 | 1 | <0.001 | |
| Changed habits due to the pandemic | No vs. Yes | 0.505 | 0.330–0.773 | 9.89 | 1 | <0.001 | |
| Changed habits due to the fear of infecting loved ones | No vs. Yes | 0.447 | 0.248–0.804 | 7.23 | 1 | 0.01 | |
| OVER CUT OFF-PA | Civil status | Cohabiting vs. Lives alone | 15.586 | 10.311–2.356 | 4.43 | 1 | 0.04 |
| OVER CUT OFF-EE | Age | <33 vs. >54 | 0.680 | 0.515–0.899 | 7.36 | 1 | 0.01 |
| Have children | No vs. Yes | 14.793 | 10.826–20.213 | 6.04 | 1 | 0.01 | |
| Non-COVID 19 related health issues | Yes vs. No | 18.969 | 12.945–27.797 | 10.78 | 1 | <0.001 | |
| Changed habits due to the pandemic | No vs. Yes | 0.366 | 0.226–0. 592 | 16. 73 | 1 | <0. 001 | |
| N = 688 | BAI | BDI | IES | GHQ | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off Subscale, N Participants | Minimum ≤21 N = 426 | Medium 22–35 N = 57 | High ≥36 N = 25 | Minimal 0–13 N = 186 | Medium 14–19 N = 20 | High ≥20 N = 482 | Subclinical 0–8 N = 491 | Mild 9–25 N = 165 | Moderate 26–43 N = 26 | Severe ≥43 N = 6 | No Problem 0–14 N = 261 | Some Problems 15–19 N = 225 | Several Problems 20–36 N = 202 | |
| BAI | Minimum (0–21) | 50% (3) | 50% (10) | 86% (413) | 90% (281) | 79% (131) | 46% (12) | 33% (2) | 89% (72) | 93% (210) | 71% (144) | |||
| Medium (22–35) | 33% (2) | 25% (5) | 10% (50) | 7% (22) | 13% (22) | 38% (10) | 50% (3) | 9% (7) | 4% (10) | 20% (40) | ||||
| High (>36) | 17% (1) | 25% (5) | 4% (19) | 3% (8) | 7% (12) | 15% (4) | 17% (1) | 2% (2) | 2% (5) | 9% (18) | ||||
| BDI | Minimal (0–13) | 71% (186) | 0% (0) | 0% (0) | ||||||||||
| Low (14–19) | 0% (0) | 0% (0) | 0% (0) | |||||||||||
| Moderate (20–28) | 0% (1) | 2% (4) | 7% (15) | |||||||||||
| High (29–63) | 28% (74) | 98% (221) | 93% (187) | |||||||||||
| IES | Subclinical (0–8) | 66% (281) | 39% (22) | 32% (8) | 100% (186) | 50% (10) | 61% (295) | 95% (248) | 68% (154) | 44% (89) | ||||
| Mild (9–25) | 31% (131) | 39% (22) | 48% (12) | 0% (0) | 30% (6) | 33% (159) | 5% (13) | 28% (64) | 44% (88) | |||||
| Moderate (26–43) | 3% (12) | 18% (10) | 16% (4) | 0% (0) | 15% (3) | 5% (23) | 0% (0) | 2% (5) | 10% (21) | |||||
| Severe (>44) | 0% (2) | 5% (3) | 4% (1) | 0% (0) | 5% (1) | 1% (5) | 0% (0) | 1% (2) | 2% (4) | |||||
| GHQ | No problem (0–14) | 17% (72) | 12% (7) | 8% (2) | 100% (186) | 5% (1) | 15% (74) | 51% (248) | 8% (13) | 0% (0) | 0% (0) | |||
| Some problems (15–19) | 49% (210) | 18% (10) | 20% (5) | 0% (0) | 20% (4) | 46% (221) | 31% (154) | 39% (64) | 19% (5) | 33% (2) | ||||
| Several problems (20–36) | 34% (144) | 70% (40) | 72% (18) | 0% (0) | 75% (15) | 39% (187) | 18% (89) | 53% (88) | 81% (21) | 67% (4) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambaro, E.; Gramaglia, C.; Marangon, D.; Probo, M.; Rudoni, M.; Zeppegno, P. Health Workers’ Burnout and COVID-19 Pandemic: 1-Year after—Results from a Repeated Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2023, 20, 6087. https://doi.org/10.3390/ijerph20126087
Gambaro E, Gramaglia C, Marangon D, Probo M, Rudoni M, Zeppegno P. Health Workers’ Burnout and COVID-19 Pandemic: 1-Year after—Results from a Repeated Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2023; 20(12):6087. https://doi.org/10.3390/ijerph20126087
Chicago/Turabian StyleGambaro, Eleonora, Carla Gramaglia, Debora Marangon, Manuela Probo, Marco Rudoni, and Patrizia Zeppegno. 2023. "Health Workers’ Burnout and COVID-19 Pandemic: 1-Year after—Results from a Repeated Cross-Sectional Survey" International Journal of Environmental Research and Public Health 20, no. 12: 6087. https://doi.org/10.3390/ijerph20126087
APA StyleGambaro, E., Gramaglia, C., Marangon, D., Probo, M., Rudoni, M., & Zeppegno, P. (2023). Health Workers’ Burnout and COVID-19 Pandemic: 1-Year after—Results from a Repeated Cross-Sectional Survey. International Journal of Environmental Research and Public Health, 20(12), 6087. https://doi.org/10.3390/ijerph20126087