



Biomechanical Consequences of Using Passive and Active Back-Support Exoskeletons during Different Manual Handling Tasks


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.2.1. Simulated Work Tasks
- The static task (Static_task) consisted of holding, for a duration of 10 s, a 15 kg load at knee height (Figure 1A). The participants maintained the load with the trunk flexed, the arms extended, and without locking the knee joint in full extension. The position was visually checked by the experimenters and adjusted if necessary. This task was repeated twice with a recovery period of at least 30 s.
- The symmetric lifting task (Sym_task) consisted of lifting a 15 kg load from a platform positioned at ankle level to a platform located at elbow level, and vice versa, at an imposed rate of 15 cycles/min while using a rhythmic beep (Figure 1B). Both platforms were located in front of the participants to impose a trunk flexion and extension in the sagittal plane. The higher platform was set back from the lower platform to require a slight elbow extension in the sagittal plane after the trunk extension. The height of the two platforms was adjusted to the anthropometric characteristics of the participants. Participants performed the task with a stoop technique. The working posture was visually checked by the experimenters and adjusted if necessary. During the task, the subjects did not deposit the load on the platforms but simply had to touch it. The participants completed two trials of five successive cycles (a cycle corresponds to the lifting and lowering of the load). A minimum 1-min rest period was observed between each trial.
- The asymmetric lifting task (Asym_task) was similar to the previous one, but with a high platform placed on the right-hand side of the participant (Figure 1C). Therefore, a 90° trunk rotation around the longitudinal axis to the right was imposed during lifting and lowering movements.
2.2.2. Exoskeletons
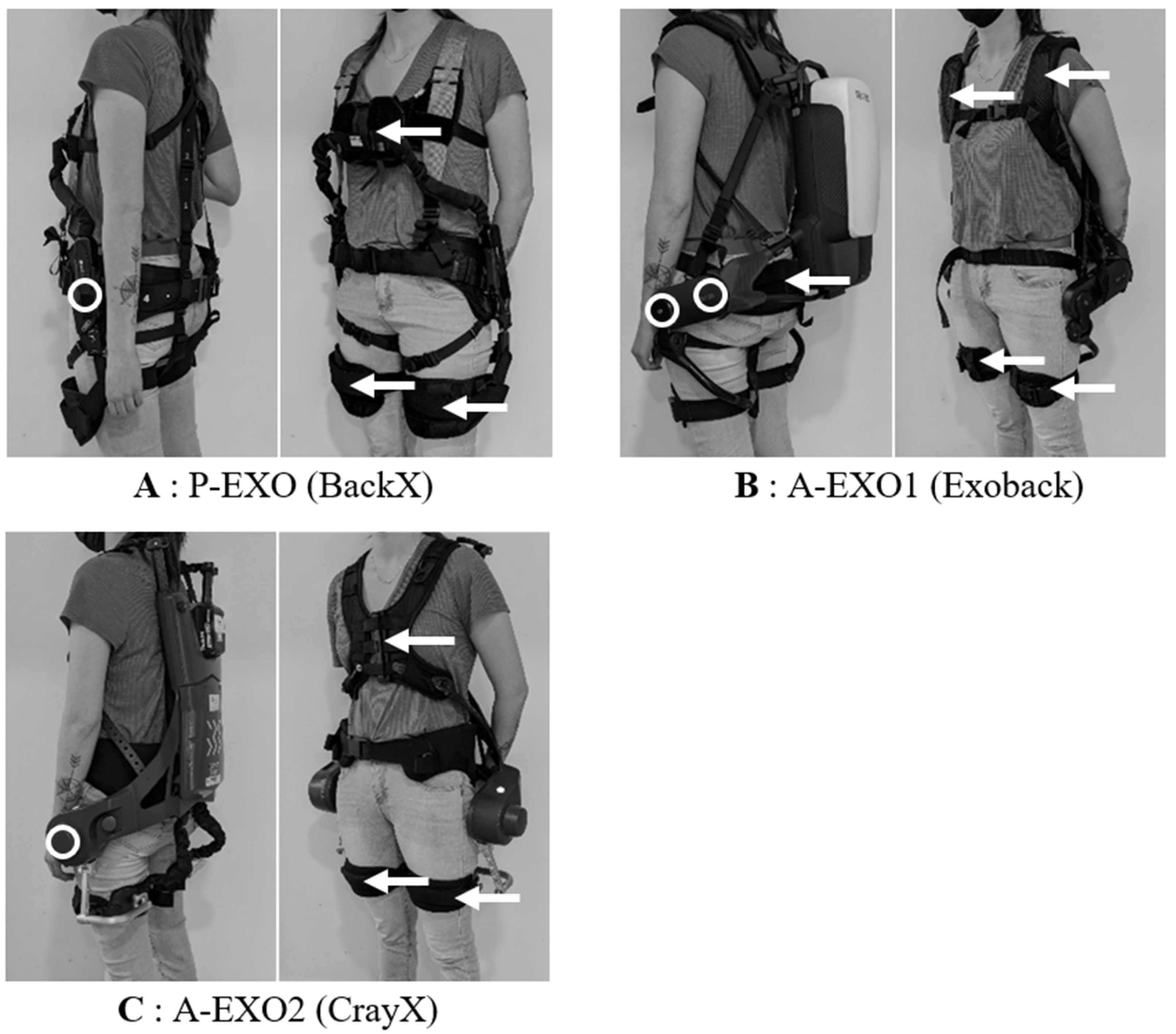
- P-EXO: the BackX model (S model, 2019) was a passive exoskeleton from SuitX (Emeryville, CA, USA) (Figure 2A). The exoskeleton was adjusted to each participant’s morphology and was set to the “instant” mode with the “high” assistance level, corresponding approximately to a maximum torque of 41 Nm at a 90° trunk flexion. This assistance level was chosen according to the weight to be handled (15 kg).
- A-EXO1: the Exoback model (V1, 2020) is an active exoskeleton from RB3D (France) (Figure 2B). During the Static_task, the exoskeleton assistance of the trunk flexion (called “support level” in the settings) was individually adjusted so that the exoskeleton fully supported the weight of the trunk, and the load was handled in the desired static posture (this adjustment was made according to the participant’s feeling of being fully supported). Most of the participants could remain, without any effort, fully supported by the exoskeleton. For some participants (seven men and three women), the maximum assistance level (72 Nm) was not sufficient to feel fully supported. In this case, maximal assistance was selected in the settings. During dynamic tasks (Sym_task and Asym_task), the assistance level of the trunk extension was set to 100%, corresponding to 72 Nm. We chose this level according to the manufacturer’s recommendation with respect to the weight to be handled (15 kg). The reactivity as well as the softness parameters were set at 50% (default settings). The support level, level of assistance at the end of the movement, and hold threshold parameters were set to 20% (default settings). The exoskeleton was adjusted to each participant’s morphology.
- A-EXO2: the Cray X (2019) is an active exoskeleton from German Bionic (Augsburg, Germany). During the Static_task, the static mode was selected, and the assistance was individually set so that the weight of the participant’s trunk and the load handled were fully supported (based on the same criteria as above). For some participants (11 men and 4 women), the maximum level of assistance (120 Nm) was not sufficient to feel fully supported. In this case, maximal assistance was selected in the settings. During the dynamic tasks (Sym_task and Asym_task), the dynamic mode was selected with the assistance level set at 60%, corresponding to 72 Nm and comparable to A-EXO1. The sensitivity, reaction, and counter force parameters were set to 5 (default settings on a scale of 0–10). The exoskeleton was adjusted to each participant’s morphology.
2.3. Data Acquisition and Analyses
2.3.1. Electromyography
2.3.2. Kinematics
2.4. Statistical Analysis
3. Results
3.1. Electromyography
3.1.1. ES Muscles
Exoskeleton Effect
The Effect of Sex and Interaction
3.1.2. Other Muscles
Exoskeleton Effect
The Effect of Sex and Interaction
3.2. Kinematics
3.2.1. Exoskeleton Effect
3.2.2. Sex Effect and Interaction
4. Discussion
4.1. Consequences of Using a Passive Exoskeleton
4.2. Consequences of the Use of Active Exoskeletons
4.3. Influence of the User’s Sex
4.4. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Russo, F.; Papalia, G.F.; Vadala, G.; Fontana, L.; Iavicoli, S.; Papalia, R.; Denaro, V. The Effects of Workplace Interventions on Low Back Pain in Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12614. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Straube, S. Reporting on work-related low back pain: Data sources, discrepancies and the art of discovering truths. Pain Manag. 2016, 6, 553–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Looze, M.P.; Bosch, T.; Krause, F.; Stadler, K.S.; O’Sullivan, L.W. Exoskeletons for industrial application and their potential effects on physical work load. Ergonomics 2016, 59, 671–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kermavnar, T.; de Vries, A.W.; de Looze, M.P.; O’Sullivan, L.W. Effects of industrial back-support exoskeletons on body loading and user experience: An updated systematic review. Ergonomics 2021, 64, 685–711. [Google Scholar] [CrossRef]
- Theurel, J.; Desbrosses, K. Occupational exoskeletons: Overview of their benefits and limitations in preventing work-related musculoskeletal disorders. IISE Trans. Occup. Erg. Hum. 2019, 7, 264–280. [Google Scholar] [CrossRef]
- Ziaei, M.; Choobineh, A.; Ghaem, H.; Abdoli-Eramaki, M. Evaluation of a passive low-back support exoskeleton (Ergo-Vest) for manual waste collection. Ergonomics 2021, 64, 1255–1270. [Google Scholar] [CrossRef]
- Poliero, T.; Fanti, V.; Sposito, M.; Caldwell, D.G.; Natali, C.D. Active and Passive Back-Support Exoskeletons: A Comparison in Static and Dynamic Tasks. IEEE Robot. Autom. Lett. 2022, 7, 8463–8470. [Google Scholar] [CrossRef]
- Schwartz, M.; Theurel, J.; Desbrosses, K. Effectiveness of soft versus rigid back-support exoskeletons during a lifting task. Int. J. Environ. Res. Public Health 2021, 18, 8062. [Google Scholar] [CrossRef]
- Alemi, M.M.; Madinei, S.; Kim, S.; Srinivasan, D.; Nussbaum, M.A. Effects of two passive back-support exoskeletons on muscle activity, energy expenditure, and subjective assessments during repetitive lifting. Hum. Factors 2020, 62, 458–474. [Google Scholar] [CrossRef]
- Luger, T.; Bar, M.; Seibt, R.; Rieger, M.A.; Steinhilber, B. Using a back exoskeleton during industrial and functional tasks-effects on muscle activity, posture, performance, usability, and wearer discomfort in a laboratory trial. Hum. Factors 2021, 65, 5–21. [Google Scholar] [CrossRef]
- Madinei, S.; Alemi, M.M.; Kim, S.; Srinivasan, D.; Nussbaum, M.A. Biomechanical assessment of two back-support exoskeletons in symmetric and asymmetric repetitive lifting with moderate postural demands. Appl. Ergon. 2020, 88, 103156. [Google Scholar] [CrossRef]
- So, B.C.L.; Cheung, H.H.; Liu, S.L.; Tang, C.I.; Tsoi, T.Y.; Wu, C.H. The effects of a passive exoskeleton on trunk muscle activity and perceived exertion for experienced auxiliary medical service providers in cardiopulmonary resuscitation chest compression. Int. J. Ind. Ergon. 2020, 76, 102906. [Google Scholar] [CrossRef]
- Huysamen, K.; de Looze, M.; Bosch, T.; Ortiz, J.; Toxiri, S.; O’Sullivan, L.W. Assessment of an active industrial exoskeleton to aid dynamic lifting and lowering manual handling tasks. Appl. Ergon. 2018, 68, 125–131. [Google Scholar] [CrossRef]
- Schwartz, M.; Desbrosses, K.; Theurel, J.; Mornieux, G. Using passive or active back-support exoskeletons during a repetitive lifting task: Influence on cardiorespiratory parameters. Eur. J. Appl. Physiol. 2022, 122, 2575–2583. [Google Scholar] [CrossRef]
- Abdoli, E.M.; Stevenson, J.M. The effect of on-body lift assistive device on the lumbar 3D dynamic moments and EMG during asymmetric freestyle lifting. Clin. Biomech. 2008, 23, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.A.; Alemi, M.M.; Asbeck, A.T. Kinematic effects of a passive lift assistive exoskeleton. J. Biomech. 2021, 120, 110317. [Google Scholar] [CrossRef]
- Bosch, T.; van Eck, J.; Knitel, K.; de Looze, M. The effects of a passive exoskeleton on muscle activity, discomfort and endurance time in forward bending work. Appl. Ergon. 2016, 54, 212–217. [Google Scholar] [CrossRef]
- Luger, T.; Bar, M.; Seibt, R.; Rimmele, P.; Rieger, M.A.; Steinhilber, B. A passive back exoskeleton supporting symmetric and asymmetric lifting in stoop and squat posture reduces trunk and hip extensor muscle activity and adjusts body posture—A laboratory study. Appl. Ergon. 2021, 97, 103530. [Google Scholar] [CrossRef]
- Graham, R.B.; Sadler, E.M.; Stevenson, J.M. Does the personal lift-assist device affect the local dynamic stability of the spine during lifting? J. Biomech. 2011, 44, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Cote, J.N. A critical review on physical factors and functional characteristics that may explain a sex/gender difference in work-related neck/shoulder disorders. Ergonomics 2012, 55, 173–182. [Google Scholar] [CrossRef]
- Pan, F.; Firouzabadi, A.; Zander, T.; Schmidt, H. Sex-dependent differences in lumbo-pelvic coordination for different lifting tasks: A study on asymptomatic adults. J. Biomech. 2020, 102, 109505. [Google Scholar] [CrossRef]
- Plamondon, A.; Lariviere, C.; Denis, D.; Mecheri, H.; Nastasia, I.; IRSST MMH Research Group. Difference between male and female workers lifting the same relative load when palletizing boxes. Appl. Ergon. 2017, 60, 93–102. [Google Scholar] [CrossRef]
- Hermens, H.; Freriks, B. The State of the Art on Sensors and Sensor Placement Procedures for Surface Electromyography: A Proposal for Sensor Placement Procedures; Roessingh Research and Development: Enschede, The Netherlands, 1997. [Google Scholar]
- Drake, J.D.; Callaghan, J.P. Elimination of electrocardiogram contamination from electromyogram signals: An evaluation of currently used removal techniques. J. Electromyogr. Kinesiol. 2006, 16, 175–187. [Google Scholar] [CrossRef]
- Chen, H.; Schall, M.C., Jr.; Fethke, N. Accuracy of angular displacements and velocities from inertial-based inclinometers. Appl. Ergon. 2018, 67, 151–161. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Abdoli, E.M.; Agnew, M.J.; Stevenson, J.M. An on-body personal lift augmentation device (PLAD) reduces EMG amplitude of erector spinae during lifting tasks. Clin. Biomech. 2006, 21, 456–465. [Google Scholar] [CrossRef]
- Koopman, A.S.; Kingma, I.; Faber, G.S.; de Looze, M.P.; van Dieen, J.H. Effects of a passive exoskeleton on the mechanical loading of the low back in static holding tasks. J. Biomech. 2019, 83, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Peach, J.P.; Sutarno, C.G.; McGill, S.M. Three-dimensional kinematics and trunk muscle myoelectric activity in the young lumbar spine: A database. Arch. Phys. Med. Rehabil. 1998, 79, 663–669. [Google Scholar] [CrossRef]
- Kim, S.; Madinei, S.; Alemi, M.M.; Srinivasan, D.; Nussbaum, M.A. Assessing the potential for “undesired” effects of passive back-support exoskeleton use during a simulated manual assembly task: Muscle activity, posture, balance, discomfort, and usability. Appl. Ergon. 2020, 89, 103194. [Google Scholar] [CrossRef]
- Ko, H.K.; Lee, S.W.; Koo, D.H.; Lee, I.; Hyun, D.J. Waist-assistive exoskeleton powered by a singular actuation mechanism for prevention of back-injury. Robot. Auton. Syst. 2018, 107, 1–9. [Google Scholar] [CrossRef]
- Wei, W.; Zha, S.J.; Xia, Y.X.; Gu, J.H.; Lin, X.C. A hip active assisted exoskeleton that assists the semi-squat lifting. Appl. Sci. 2020, 10, 2424. [Google Scholar] [CrossRef] [Green Version]
- Yin, P.; Yang, L.; Du, S.F.; Qu, S.G.; Jia, B.C.; Zhao, N. The effect of mobile wearable waist assist robot on lower back pain during lifting and handling tasks. Mob. Netw. Appl. 2021, 26, 988–996. [Google Scholar] [CrossRef]
- Lariviere, C.; Gagnon, D.; Loisel, P. The comparison of trunk muscles EMG activation between subjects with and without chronic low back pain during flexion-extension and lateral bending tasks. J. Electromyogr. Kinesiol. 2000, 10, 79–91. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Static_task | |||||||
| CON | P-EXO | A-EXO1 | A-EXO2 | ||||
| TZ | 53.5 ± 39.9 | 49.0 ± 35.9 | 23.3 ± 30.4 | * # | 24.0 ± 22.0 | * # | |
| LD | 13.0 ± 8.7 | 9.4 ± 7.8 | * | 4.9 ± 4.3 | * # | 5.0 ± 4.2 | * # |
| GM | 14.7 ± 8.0 | 12.7 ± 7.5 | * | 8.2 ± 5.7 | * # | 8.9 ± 5.4 | * # |
| BF | 26.4 ± 15.2 | 22.7 ± 13.1 | * | 16.4 ± 10.5 | * # | 17.0 ± 10.8 | * # |
| Sym_task | |||||||
| CON | P-EXO | A-EXO1 | A-EXO2 | ||||
| TZ | 107.4 ± 70.5 | 114.5 ± 81.7 | 80.1 ± 57.9 | * # | 82.2 ± 58.5 | * # | |
| LD | 19.4 ± 12.4 | 15.4 ± 10.0 | * | 12.3 ± 8.6 | * # | 11.5 ± 7.8 | * # |
| GM | 31.2 ± 14.1 | 29.7 ± 13.4 | 22.0 ± 9.6 | * # | 24.2 ± 11.7 | * # | |
| BF | 37.7 ± 19.7 | 35.1 ± 18.9 | 30.0 ± 15.1 | * # | 30.3 ± 14.1 | * # | |
| Asym_task | |||||||
| CON | P-EXO | A-EXO1 | A-EXO2 | ||||
| Right TZ | 99.4 ± 37.1 | 99.9 ± 37.4 | 69.2 ± 29.4 | * # | 70.0 ± 25.4 | * # | |
| Right LD | 24.0 ± 15.0 | 21.5 ± 14.2 | 15.5 ± 9.2 | * # | 16.7 ± 12.0 | * # | |
| Right GM | 26.2 ± 15.2 | 24.7 ± 13.7 | 20.1 ± 12.4 | * # | 20.2 ± 11.0 | * # | |
| Right BF | 35.3 ± 20.2 | 32.0 ± 18.7 | 26.0 ± 14.0 | * # | 25.9 ± 12.7 | * # | |
| Left TZ | 97.4 ± 91.2 | 94.0 ± 87.7 | 68.6 ± 73.4 | * # | 70.4 ± 72.8 | * # | |
| Left LD | 17.9 ± 15.4 | 15.9 ± 14.0 | 12.7 ± 10.3 | * # | 12.5 ± 10.1 | * # | |
| Left GM | 36.2 ± 15.9 | 31.9 ± 15.4 | * | 23.9 ± 12.5 | * # | 27.8 ± 13.3 | * # $ |
| Left BF | 37.1 ± 18.8 | 36.1 ± 17.6 | 34.4 ± 16.8 | 37.2 ± 18.8 | |||
| Static_task | ||||||
| CON | P-EXO | A-EXO1 | A-EXO2 | |||
| Thoracic angle | 43 ± 13 | 44 ± 14 | 49 ± 13 | * # | 47 ± 14 | |
| Lumbar angle | 18 ± 18 | 19 ± 14 | 18 ± 15 | 14 ± 15 | * # | |
| Hip angle | 49 ± 21 | 53 ± 19 | 49 ± 19 | 58 ± 25 | * $ | |
| Sym_task | ||||||
| CON | P-EXO | A-EXO1 | A-EXO2 | |||
| Thoracic angle | 41 ± 19 | 35 ± 18 | 40 ± 18 | 41 ± 16 | ||
| Lumbar angle | −1 ± 22 | 1 ± 25 | −2 ± 21 | −9 ± 26 | * # $ | |
| Hip angle | 53 ± 20 | 57 ± 22 | 55 ± 21 | 64 ± 28 | * # $ | |
| Asym_task | ||||||
| CON | P-EXO | A-EXO1 | A-EXO2 | |||
| Thoracic angle | 37 ± 17 | 36 ± 15 | 37 ± 13 | 37 ± 14 | ||
| Lumbar angle | 1 ± 20 | 3 ± 22 | −2 ± 26 | # | −3 ± 25 | # |
| Hip angle | 54 ± 18 | 56 ± 18 | 57 ± 25 | 64 ± 26 | * # $ | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwartz, M.; Desbrosses, K.; Theurel, J.; Mornieux, G. Biomechanical Consequences of Using Passive and Active Back-Support Exoskeletons during Different Manual Handling Tasks. Int. J. Environ. Res. Public Health 2023, 20, 6468. https://doi.org/10.3390/ijerph20156468
Schwartz M, Desbrosses K, Theurel J, Mornieux G. Biomechanical Consequences of Using Passive and Active Back-Support Exoskeletons during Different Manual Handling Tasks. International Journal of Environmental Research and Public Health. 2023; 20(15):6468. https://doi.org/10.3390/ijerph20156468
Chicago/Turabian StyleSchwartz, Mathilde, Kévin Desbrosses, Jean Theurel, and Guillaume Mornieux. 2023. "Biomechanical Consequences of Using Passive and Active Back-Support Exoskeletons during Different Manual Handling Tasks" International Journal of Environmental Research and Public Health 20, no. 15: 6468. https://doi.org/10.3390/ijerph20156468
APA StyleSchwartz, M., Desbrosses, K., Theurel, J., & Mornieux, G. (2023). Biomechanical Consequences of Using Passive and Active Back-Support Exoskeletons during Different Manual Handling Tasks. International Journal of Environmental Research and Public Health, 20(15), 6468. https://doi.org/10.3390/ijerph20156468