
Long-Term Lifestyle Habits and Quality of Life after Roux-in-Y Gastric Bypass in Brazilian Public versus Private Healthcare Systems: Beyond Weight Loss
 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Demographics, Socioeconomic, Clinical, and Surgical Data
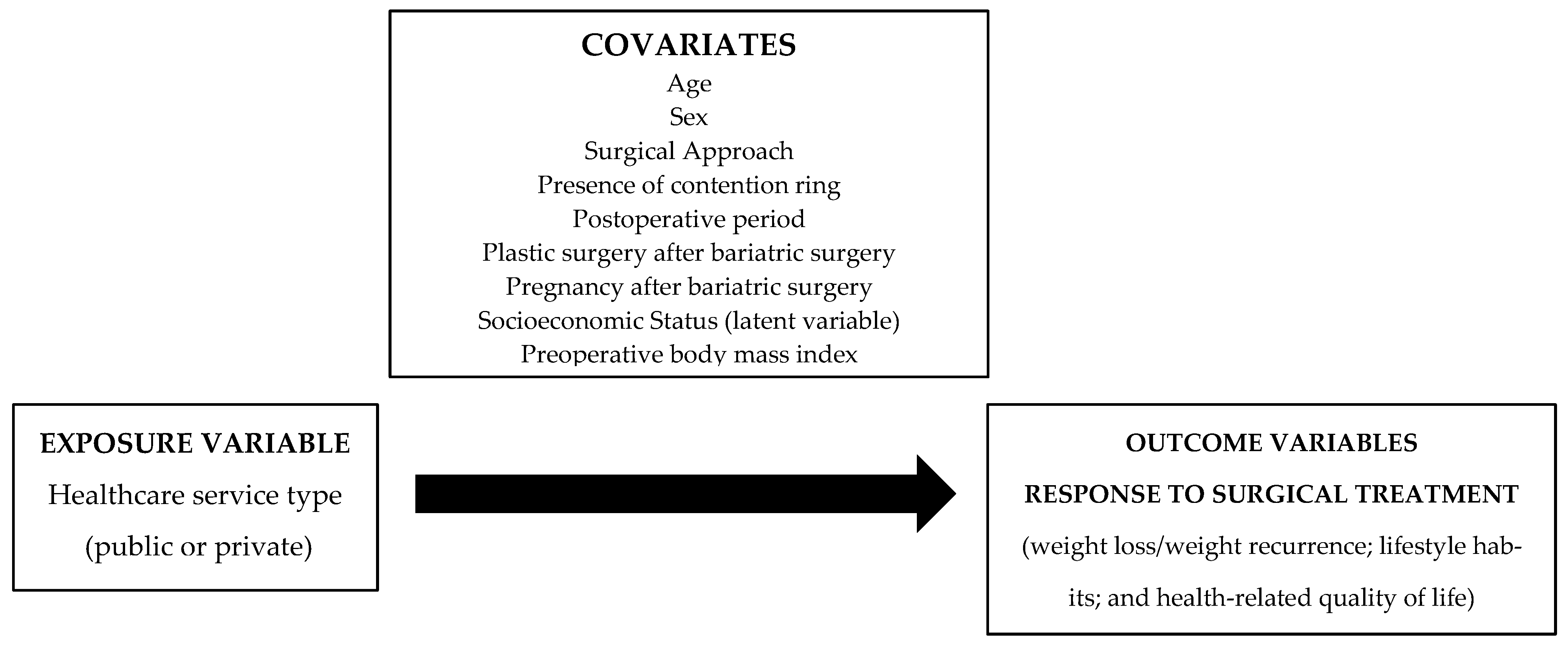
2.2. Study Variables and the Theoretical Model
2.2.1. Weight Loss and Weight Recurrence
2.2.2. Lifestyle Habits
2.2.3. Health-Related Quality of Life
2.3. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| TOTAL n = 123 | SUS n = 79 | PVT n = 44 | p-Value | |
|---|---|---|---|---|
| Age (years) (Mean ± SD) | 48.3 ± 9.2 | 49.9 ± 9.0 | 45.6 ± 9.2 | 0.013 a |
| Sex Female (n; %) | 112 (91.1) | 73 (92.4) | 39 (88.6) | 0.520 b |
| Preoperative BMI (kg/m2) (Mean ± SD) | 44.0 ± 8.2 | 46.0 ± 8.7 | 40.4 ± 5.8 | <0.001 a |
| Educational Level Years of study (Mean ± SD, min; max) | 13.29 ± 4.0 | 12.00 ± 3.9 | 15.61 ± 2.9 | <0.001 a |
| Monthly per capita income (U.S. dollars—Mean ± SD) | 480.1 ± 409.1 | 334.9 ± 296.9 | 740.8 ± 454.5 | 0.002 a |
| Employed (n; %) | 84 (68.2) | 49 (62.0) | 35 (79.5) | 0.045 c |
| SES (latent variable) | ||||
| Tertile 1 Tertile 2 Tertile 3 | 41(33.3) 41(33.3) 41(33.3) | 36 (45.5) 30 (38.0) 13 (16.5) | 5 (11.4) 11 (25.0) 28 (63.6) | <0.001 c |
| Postoperative time (years) (Mean ± SD) | 9.3 ± 2.6 | 9.8 ± 2.6 | 8.50 ± 2.2 | 0.005 a |
| Surgical Approach (n = 122) | ||||
| Open Laparoscopic | 83 (67.5) 39 (31.7) | 57 (73.1) 21 (26.9) | 26 (59.1) 18 (40.9) | 0.112 c |
| Presence of contention ring (n; %) | 53 (43.1) | 37 (46.8) | 16 (36.4) | 0.261 c |
| Reported pregnancy(ies) after MBS (n = 112) (n; %) | 12 (9.8) | 5 (6.8) | 7 (18.4) | 0.102 b |
| Underwent plastic surgery after MBS (n;%) | 70 (56.9) | 46 (58.2) | 24 (54.5) | 0.693 c |
| TOTAL n = 123 | SUS n = 79 | PVT n = 44 | p-Value | ||
|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||
| Weight markers (Mean ± SD) | |||||
| % Total Weight Loss 1 | 24.64 ± 0.99 | 24.71 ± 1.32 | 24.5 ± 1.41 | 0.929 | 0.459 |
| % Excess Weight Loss 2 | 60.46 ± 2.41 | 56.88 ± 3.03 | 66.89 ± 3.83 | 0.046 | 0.219 |
| % Weight Recurrence 3 | 20.42 ± 1.46 | 20.89 ± 2.09 | 19.60 ± 1.64 | 0.675 | 0.384 |
| Diet quality 4 (Mean ± SD) | |||||
| Consumption (grams/1000 kcal) of: | |||||
| In natura/Unprocessed foods Processed foods Ultra-processed foods | 637.53 ± 181.37 113.68 ± 50.74 195.65 ± 110.00 | 660.1 ± 193.21 103.43 ± 41.72 186.94 ± 106.57 | 597.09 ± 151.70 132.10 ± 60.15 211.30 ± 115.49 | 0.065 0.002 0.241 | 0.395 0.093 0.645 |
| Health-related quality of life (n = 111) (Mean ± SD) | |||||
| Self-perception of current health (EQ-VAS) 5 EQ-5D-3L index 6 | 70.09 ± 21.54 0.70 ± 0.17 | 66.90 ± 23.37 0.67 ± 0.19 | 75.75 ± 16.66 0.76 ± 0.14 | 0.013 0.037 | 0.797 0.375 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional de Saúde 2019: Informações Sobre Domicílios, Acesso e Utilização Dos Serviços de Saúde: Brasil, Grandes Regiões e Unidades da Federação. 2020; ISBN 978-65-872-0118-4. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101748.pdf (accessed on 17 September 2022).
- Cazzo, E.; Ramos, A.C.; Chaim, E.A. Bariatric Surgery Offer in Brazil: A Macroeconomic Analysis of the Health System’s Inequalities. Obes. Surg. 2019, 29, 1874–1880. [Google Scholar] [CrossRef]
- Ramos, A.; Fasmbs, F.; Kow, L.; Brown, W.; Phd, M.; Fracs, F.; Welbourn, R.; Dixon, J.; Frcp, F.; Kinsman, E.R.; et al. The IFSO Global Registry 5th IFSO Global Registry Report; IFSO: Napoli, Italy, 2019; Available online: https://www.ifso.com/pdf/5th-ifso-global-registry-report-september-2019.pdf (accessed on 17 September 2022).
- Corcelles, R.; Boules, M.; Froylich, D.; Hag, A.; Daigle, C.R.; Aminian, A.; Brethauer, S.A.; Burguera, B.; Schauer, P.R. Total Weight Loss as the Outcome Measure of Choice After Roux-En-Y Gastric Bypass. Obes. Surg. 2016, 26, 1794–1798. [Google Scholar] [CrossRef] [PubMed]
- Alfadda, A.A.; Al-Naami, M.Y.; Masood, A.; Elawad, R.; Isnani, A.; Ahamed, S.S.; Alfadda, N.A. Long-Term Weight Outcomes after Bariatric Surgery: A Single Center Saudi Arabian Cohort Experience. J. Clin. Med. 2021, 10, 4922. [Google Scholar] [CrossRef]
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-Analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef]
- Junquera Bañares, S.; Ramírez Real, L.; Camuñas Segovia, J.; Martín García-Almenta, M.; Llanos Egüez, K.; Álvarez Hernández, J. Evaluation of Quality of Life, Weight Loss and Evolution of Comorbidities at 6 Years after Bariatric Surgery. Endocrinol. Diabetes Y Nutr. 2021, 68, 501–508. [Google Scholar] [CrossRef]
- Sierżantowicz, R.; Ładny, J.R.; Lewko, J. Quality of Life after Bariatric Surgery—A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 9078. [Google Scholar] [CrossRef]
- Nymo, S.; Lundanes, J.; Aukan, M.; Sandvik, J.; Johnsen, G.; Græslie, H.; Larsson, I.; Martins, C. Diet and Physical Activity Are Associated with Suboptimal Weight Loss and Weight Regain 10–15 Years after Roux-En-Y Gastric Bypass: A Cross-Sectional Study. Obes. Res. Clin. Pract. 2022, 16, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Martin-Fernandez, K.W.; Creel, D.B.; Schuh, L.M. Psychosocial and Behavioral Correlates of Weight Loss 12 to 15 Years after Bariatric Surgery. J. Behav. Med. 2022, 45, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Farias, G.; Silva, R.M.O.; da Silva, P.P.P.; Vilela, R.M.; Bettini, S.C.; Dâmaso, A.R.; Netto, B.D.M. Impact of Dietary Patterns According to NOVA Food Groups: 2 y after Roux-En-Y Gastric Bypass Surgery. Nutrition 2020, 74, 110746. [Google Scholar] [CrossRef]
- Sjöström, L. Review of the Key Results from the Swedish Obese Subjects (SOS) Trial-a Prospective Controlled Intervention Study of Bariatric Surgery. J. Intern. Med. 2013, 273, 219–234. [Google Scholar] [CrossRef]
- Ministério da Saúde Brasil. Diretrizes para o Cuidado das Pessoas com Doenças Crônicas nas Redes de Atenção à Saúde e nas Linhas de Cuidado Prioritárias. 2013; ISBN 978-85-334-2018-2. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes%20_cuidado_pessoas%20_doencas_cronicas.pdf (accessed on 17 September 2022).
- Pajecki, D.; Kawamoto, F.; Dantas, A.C.B.; Andrade, P.C.; Brasil, N.C.; Junqueira, S.M.; de Oliveira, F.M.P.; Ribeiro, R.A.; Santo, M.A. Real-World Evidence of Health Outcomes and Medication Use 24 Months after Bariatric Surgery in the Public Healthcare System in Brazil: A Retrospective, Single-Center Study. Clinics 2020, 75, e1588. [Google Scholar] [CrossRef] [PubMed]
- Rocha de Almeida, R.; Cândido de Souza, M.; Gama de Matos, D.; Monteiro Costa Pereira, L.; Batista Oliveira, V.; Menezes Oliveira, J.; Soares Barreto-Filho, J.; Almeida-Santos, M.; de Souza, R.; de Freitas Zanona, A.; et al. A Retrospective Study about the Differences in Cardiometabolic Risk Indicators and Level of Physical Activity in Bariatric Surgery Patients from Private vs. Public Units. Int. J. Environ. Res. Public Health 2019, 16, 4751. [Google Scholar] [CrossRef] [PubMed]
- Rasera, I.; Luque, A.; Junqueira, S.M.; Brasil, N.C.; Andrade, P.C. Effectiveness and Safety of Bariatric Surgery in the Public Healthcare System in Brazil: Real-World Evidence from a High-Volume Obesity Surgery Center. Obes. Surg. 2017, 27, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Almeida, R.R.; Aidar, F.J.; Souza, M.F.C.; Oliveira, V.B.; Oliveira, J.L.M.; Baumworcel, L.; Pereira, L.M.C.; de Oliveira, L.M.S.M.; Costa, J.O.; Rocha, R.M.S.; et al. Bariatric Surgery: Late Outcomes in Patients Who Reduced Comorbidities at Early Follow-Up. Medicina 2021, 57, 995. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Deitel, M.; Gawdat, K.; Melissas, J. Reporting Weight Loss 2007. Obes. Surg. 2007, 17, 565–568. [Google Scholar] [CrossRef]
- Magro, D.O.; Geloneze, B.; Delfini, R.; Pareja, B.C.; Callejas, F.; Pareja, J.C. Long-Term Weight Regain after Gastric Bypass: A 5-Year Prospective Study. Obes. Surg. 2008, 18, 648–651. [Google Scholar] [CrossRef]
- Da Silva, F.B.L.; Gomes, D.L.; de Carvalho, K.M.B. Poor Diet Quality and Postoperative Time Are Independent Risk Factors for Weight Regain after Roux-En-Y Gastric Bypass. Nutrition 2016, 32, 1250–1253. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method Reduces Bias in the Collection of Energy Intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Basset, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A. 2011 Compendium of Physical Activities. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Haskel, W.L.; Wood, P.D.; Fortmann, S.P.; Rogers, T.; Blair, S.N.; Paffenbarger, R.S. Physical activity assessment methodology in the five-city project1. Am. J. Epidemiol. 1985, 121, 91–106. [Google Scholar] [CrossRef] [PubMed]
- Saraiva Leão Borges, L.P.; Ries, D.C.; Sousa, A.G.; da Costa, T.H.M. Comparison and Calibration of 24-Hour Physical Activity Recall in Adult Population. Eur. J. Sport Sci. 2022, 22, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005; ISBN 978-0-309-08525-0. Available online: https://nap.nationalacademies.org/catalog/10490/dietary-reference-intakes-for-energy-carbohydrate-fiber-fat-fatty-acids-cholesterol-protein-and-amino-acids (accessed on 17 September 2022). [CrossRef]
- Lima, C.T.; Freire, A.C.C.; Silva, A.P.B.; Teixeira, R.M.; Farrel, M.; Prince, M. Concurrent and Construct Validity of the AUDIT in an Urban Brazilian Sample. Alcohol Alcohol. 2005, 40, 584–589. [Google Scholar] [CrossRef]
- Szend, A.; Janssen, B.; Cabasés, J. Self-Reported Population Health: An International Perspective Based on EQ-5D; Szende, A., Janssen, B., Cabases, J., Eds.; Springer Netherlands: Dordrecht, The Netherlands, 2014; ISBN 978-94-007-7595-4. [Google Scholar]
- Santos, M.; Cintra, M.A.C.T.; Monteiro, A.L.; Santos, B.; Gusmão-filho, F.; Andrade, M.V.; Noronha, K.; Cruz, L.N.; Camey, S.; Tura, B.; et al. Brazilian Valuation of EQ-5D-3L Health States. Med. Decis. Mak. 2016, 36, 253–263. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R.; Tatham, R. Análise Multivariada de Dados, 5th ed.; Bookman: Porto Alegre, Brazil, 2009; ISBN 9788577804023. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Melendez-Araújo, M.S.; Berber, L.C.L.; de Sousa, K.M.Q.; Figueiredo, A.C.M.G.; Lamarca, F.; Dutra, E.S.; de Carvalho, K.M.B. New Insights on the Association between Socioeconomic Status and Weight Loss After Bariatric Surgery: A Systematic Review and Meta-Analysis. Obes. Surg. 2022, 32, 3752–3770. [Google Scholar] [CrossRef]
- Cobo, B.; Cruz, C.; Dick, P.C. Desigualdades de Gênero e Raciais No Acesso e Uso Dos Serviços de Atenção Primária à Saúde No Brasil. Cien. Saude Colet. 2021, 26, 4021–4032. [Google Scholar] [CrossRef]
- Han, Y.; Jia, Y.; Wang, H.; Cao, L.; Zhao, Y. Comparative Analysis of Weight Loss and Resolution of Comorbidities between Laparoscopic Sleeve Gastrectomy and Roux-En-Y Gastric Bypass: A Systematic Review and Meta-Analysis Based on 18 Studies. Int. J. Surg. 2020, 76, 101–110. [Google Scholar] [CrossRef]
- Ferreira, J.S.; Diettrich, S.H.C.; Pedro, D.A. Influência Da Prática de Atividade Física Sobre a Qualidade de Vida de Usuários Do SUS. Saúde Em Debate 2015, 39, 792–801. [Google Scholar] [CrossRef][Green Version]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C. Evidence-Based Intervention in Physical Activity: Lessons from around the World. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef]
- Tennøy, A.; Knapskog, M.; Wolday, F. Walking Distances to Public Transport in Smaller and Larger Norwegian Cities. Transp. Res. D Transp. Environ. 2022, 103, 103169. [Google Scholar] [CrossRef]
- Freeland, A.L.; Banerjee, S.N.; Dannenberg, A.L.; Wendel, A.M. Walking Associated with Public Transit: Moving Toward Increased Physical Activity in the United States. Am. J. Public Health 2013, 103, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.F.; Tracy, A.L.; Schurdak, J.D.; Magrisso, I.J.; Grayson, B.E.; Seeley, R.J.; Benoit, S.C. Roux En Y Gastric Bypass Increases Ethanol Intake in the Rat. Obes. Surg. 2013, 23, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Hajnal, A.; Zharikov, A.; Polston, J.E.; Fields, M.R.; Tomasko, J.; Rogers, A.M.; Volkow, N.D.; Thanos, P.K. Alcohol Reward Is Increased after Roux-En-Y Gastric Bypass in Dietary Obese Rats with Differential Effects Following Ghrelin Antagonism. PLoS ONE 2012, 7, e49121. [Google Scholar] [CrossRef] [PubMed]
- Polston, J.E.; Pritchett, C.E.; Tomasko, J.M.; Rogers, A.M.; Leggio, L.; Thanos, P.K.; Volkow, N.D.; Hajnal, A. Roux-En-Y Gastric Bypass Increases Intravenous Ethanol Self-Administration in Dietary Obese Rats. PLoS ONE 2013, 8, e83741. [Google Scholar] [CrossRef] [PubMed]
- Sirohi, S.; Richardson, B.D.; Lugo, J.M.; Rossi, D.J.; Davis, J.F. Impact of Roux-En-Y Gastric Bypass Surgery on Appetite, Alcohol Intake Behaviors, and Midbrain Ghrelin Signaling in the Rat. Obesity 2017, 25, 1228–1236. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Basic Documents: Forty-Ninth Edition (Including Amendments up to 31 May 2019), 49th ed.; WHO: Geneva, Switzerland, 2020; ISBN 9789240000513. Available online: https://apps.who.int/gb/bd/pdf_files/BD_49th-en.pdf (accessed on 17 September 2022).
- Burton, P.; Brown, W.; Chen, R.; Shaw, K.; Packiyanathan, A.; Bringmann, I.; Smith, A.; Nottle, P. Outcomes of High-Volume Bariatric Surgery in the Public System. ANZ J. Surg. 2016, 86, 572–577. [Google Scholar] [CrossRef]
- Turri, J.A.O.; Anokye, N.K.; dos Santos, L.L.; Júnior, J.M.S.; Baracat, E.C.; Santo, M.A.; Sarti, F.M. Impacts of Bariatric Surgery in Health Outcomes and Health Care Costs in Brazil: Interrupted Time Series Analysis of Multi-Panel Data. BMC Health Serv. Res. 2022, 22, 41. [Google Scholar] [CrossRef]
- Sun, S.; Stenberg, E.; Lindholm, L.; Salén, K.-G.; Franklin, K.A.; Luo, N.; Cao, Y. Prediction of Quality-Adjusted Life Years (QALYs) after Bariatric Surgery Using Regularized Linear Regression Models: Results from a Swedish Nationwide Quality Register. Obes. Surg. 2023, 33, 2452–2462. [Google Scholar] [CrossRef]
- Wang, L.; Martínez Steele, E.; Du, M.; Pomeranz, J.L.; O’Connor, L.E.; Herrick, K.A.; Luo, H.; Zhang, X.; Mozaffarian, D.; Zhang, F.F. Trends in Consumption of Ultraprocessed Foods Among US Youths Aged 2–19 Years, 1999–2018. JAMA 2021, 326, 519. [Google Scholar] [CrossRef]
- Rebelos, E.; Moriconi, D.; Scalese, M.; Denoth, F.; Molinaro, S.; Siciliano, V.; Anselmino, M.; Taddei, S.; Ferrannini, E.; Nannipieri, M. Impact of Postprandial Hypoglycemia on Weight Loss After Bariatric Surgery. Obes. Surg. 2020, 30, 2266–2273. [Google Scholar] [CrossRef]
- Dicken, S.J.; Batterham, R.L. The Role of Diet Quality in Mediating the Association between Ultra-Processed Food Intake, Obesity and Health-Related Outcomes: A Review of Prospective Cohort Studies. Nutrients 2021, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Lopes Pinto, S.; da Silva, D.C.G.; Bressan, J. Absolute and Relative Changes in Ultra-Processed Food Consumption and Dietary Antioxidants in Severely Obese Adults 3 Months After Roux-En-Y Gastric Bypass. Obes. Surg. 2019, 29, 1810–1815. [Google Scholar] [CrossRef] [PubMed]
- Reichmann, M.T.F.; Todeschini, S.; Setter, N.; Vilela, R.M.; Radominski, R.B. Comparison of the Dietary Intake amongst Women in the Late Postoperative Period after Roux-En-Y Gastric Bypass with the Bariatric Food Pyramidof Dietary Intake with Reference Values among Women in Late Postoperative of y-En-Roux Gastric Bypass. Nutr. Hosp. 2019, 36, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Molin Netto, B.D.; Earthman, C.P.; Farias, G.; Landi Masquio, D.C.; Grotti Clemente, A.P.; Peixoto, P.; Bettini, S.C.; von Der Heyde, M.E.; Dâmaso, A.R. Eating Patterns and Food Choice as Determinant of Weight Loss and Improvement of Metabolic Profile after RYGB. Nutrition 2017, 33, 125–131. [Google Scholar] [CrossRef] [PubMed]



| TOTAL n (%) | SUS n (%) | PVT n (%) | OR (95% CI) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | ||||
| Weight markers (n = 123) | |||||||
| Individuals with weight recurrence 1 | 92 (74.8) | 57 (72.2) | 35 (79.5) | 1.50 (0.62; 3.63) | 0.90 (0.30; 2.70) | 0.367 | 0.850 a |
| Individual responders to weight loss 2 | 81 (65.9) | 47 (59.5) | 34 (77.3) | 2.32 (1.00; 5.34) | 1.25 (0.47; 3.36) | 0.049 | 0.655 b |
| Lifestyle habits | |||||||
| Alcohol Consumption 3 (n = 106) | |||||||
| High risk of developing alcohol-related problems (AUDIT) | 34 (32.08) | 17 (24.6) | 17 (45.9) | 2.60 (1.11; 6.07) | 3.23 (1.03; 10.10) | 0.025 | 0.044 a |
| Physical Activity Level 4 (n = 122) | |||||||
| Sedentary/Insufficiently Active Very active | 41 (33.6) 81 (66.4) | 19 (24.4) 59 (75.6) | 22 (50.0) 22 (50.0) | 1 0.32 (0.15; 0.71) | 1 0.23 (0.87; 0.63) | 0.004 | 0.004 a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melendez-Araújo, M.S.; do Carmo, A.S.; Vieira, F.T.; Lamarca, F.; Nakano, E.Y.; Lima, R.M.; Dutra, E.S.; de Carvalho, K.M.B. Long-Term Lifestyle Habits and Quality of Life after Roux-in-Y Gastric Bypass in Brazilian Public versus Private Healthcare Systems: Beyond Weight Loss. Int. J. Environ. Res. Public Health 2023, 20, 6494. https://doi.org/10.3390/ijerph20156494
Melendez-Araújo MS, do Carmo AS, Vieira FT, Lamarca F, Nakano EY, Lima RM, Dutra ES, de Carvalho KMB. Long-Term Lifestyle Habits and Quality of Life after Roux-in-Y Gastric Bypass in Brazilian Public versus Private Healthcare Systems: Beyond Weight Loss. International Journal of Environmental Research and Public Health. 2023; 20(15):6494. https://doi.org/10.3390/ijerph20156494
Chicago/Turabian StyleMelendez-Araújo, Mariana S., Ariene Silva do Carmo, Flávio Teixeira Vieira, Fernando Lamarca, Eduardo Yoshio Nakano, Ricardo M. Lima, Eliane Said Dutra, and Kênia Mara Baiocchi de Carvalho. 2023. "Long-Term Lifestyle Habits and Quality of Life after Roux-in-Y Gastric Bypass in Brazilian Public versus Private Healthcare Systems: Beyond Weight Loss" International Journal of Environmental Research and Public Health 20, no. 15: 6494. https://doi.org/10.3390/ijerph20156494
APA StyleMelendez-Araújo, M. S., do Carmo, A. S., Vieira, F. T., Lamarca, F., Nakano, E. Y., Lima, R. M., Dutra, E. S., & de Carvalho, K. M. B. (2023). Long-Term Lifestyle Habits and Quality of Life after Roux-in-Y Gastric Bypass in Brazilian Public versus Private Healthcare Systems: Beyond Weight Loss. International Journal of Environmental Research and Public Health, 20(15), 6494. https://doi.org/10.3390/ijerph20156494