

The Journey to Early Identification and Intervention for Children with Disabilities in Fiji

Abstract
:1. Introduction
Fijian Context
2. Materials and Methods
2.1. Participants
2.2. Data Analysis
3. Results
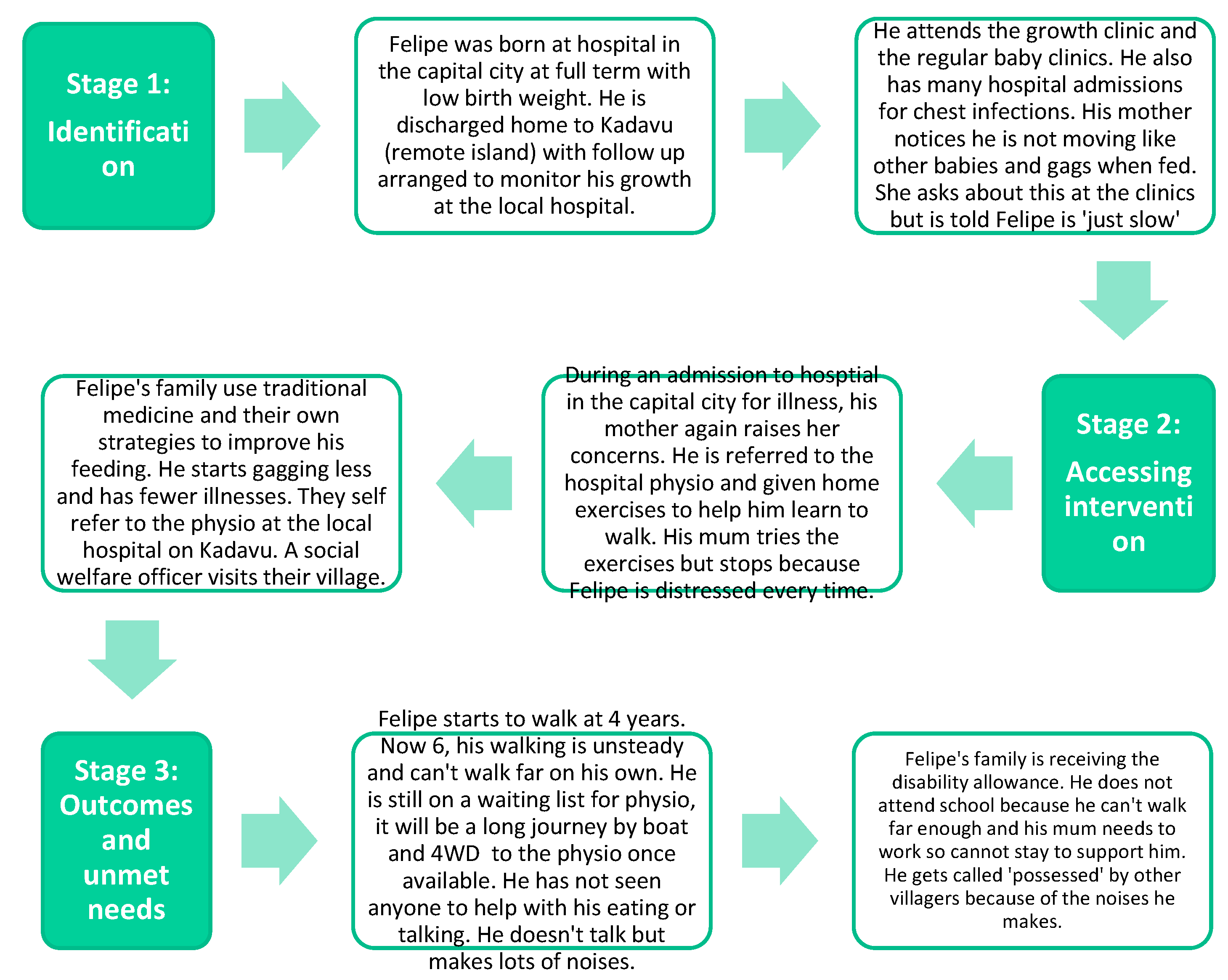
3.1. Journey Mapping
3.2. Thematic Analysis
3.2.1. Stage 1: Identification of Needs
Missed Opportunities for Identification
Sometimes even cases who are booked don’t come…we always call our patients a day prior to the clinic. And they say that they’re coming, but because of some bad weather conditions or transportation problems, financial issues, they don’t turn up.(Stakeholder, Health)
Lack of Information for Caregivers
Parent: They just told me Down Syndrome without even discussing the meaning of this word.
Interviewer: were you given any advice about how to care for your child?
Parent: I wouldn’t say they gave me advice, the doctor only said they need to take the blood. I asked what are the bloods for and she said that’s because she [baby] has Down Syndrome. That’s it. Just that.(Caregiver, Serua)
We normally address care on a child as general, as a child health without the focus on whether they have disability or not. They get sick, they come and see us, and it’s just when they’re sick then we intervene. But there are other special areas of their needs that are being ignored at the moment which we think we need to improve on.(Stakeholder, Health)
Maybe if we were familiar with the symptoms at the very earlier age maybe we could have gone [to intervention] early. From hospital, we could have prepared to come early [to early intervention service], then maybe we could have, you know tackle her situation a bit more, because I kept thinking she’s going to grow out of it you know. But at that time we just left it and we didn’t ask for help’.(Caregiver, Suva)
Emerging Caregiver Concerns and Help-Seeking
They just told me that it will take him a long time to do something. When I came [to the clinic], at 1 year he was still only rolling around. Then they told me, it’s normal, Down Syndrome, they are weak. After that I didn’t take him anywhere, we just stayed together, and I’ve been taking care of him.(Caregiver, Serua)
One of the main cause [of parents not seeking help] is stigma. And the fear of knowing, you know, stigma in the sense. If they feel that their child is developmentally slow, they will usually keep that child at home, and not seek attention, because that would bring out the fault within the kid and in the family. And fear of knowing, because if they do accept that something is wrong, then there is something is wrong.(Stakeholder, Health)
Recommended Actions Targeting Stage 1—Identification of Needs
- Training on early identification of disabilities and referral for those who are the first point of contact for families. This may include health workers at the primary care level (e.g., village nurses/community health workers), teachers and early childhood educators, and welfare officers.
- Strengthen processes for developmental monitoring at routine baby clinics.
- Improve information given by health workers to new parents about their child’s condition, potential developmental implications, and sources of support available.
- Consider mechanisms for financial support for families of children born with complications to attend follow-up health and medical appointments to enable continuity of care and not being ‘lost’ to follow-up.
- Raise community awareness of developmental disabilities, the benefits of timely early intervention, and the services available.
3.2.2. Stage 2: Accessing Intervention and Supports
Barriers to Accessing Services
If children are identified in Lautoka they have to come all the way to Suva. If our children in the islands need services, they have to wait till someone can pay for them coming…this is one of the areas that we’re struggling with.(Stakeholder, Social Welfare)
So, fare is the main problem and secondly he is in diaper, I have to buy his diaper and other expenses to travel to town, and we have to buy something to eat.(Caregiver, Serua)
Facilitators of Access to Services
The awareness is there now, people now are coming out, like the parents they used to hesitate to come to us and say, ‘My child is blind’. But with lots of awareness and counselling, they have now come to us for support.(Stakeholder, Disability)
Recommended Actions Targeting Stage 2—Accessing Intervention and Supports
- Financial support mechanisms for caregivers to take time off work to attend appointments for intervention.
- Transport allowances or subsidies for travel to and from services for families of children with disabilities.
- Onward referral to local services where available for follow-up of rural and remote children (e.g., hospital-based physiotherapy services).
- Funding for new and existing services to improve capacity and coverage outside the main urban areas.
- Extend the use of outreach and remote/telehealth models of service delivery drawing on learnings from existing community-based programs.
- Strengthen existing national policies and action plans on ECD and disabilities to explicitly include children with disabilities, backed with appropriate resourcing.
- Develop locally contextualized, sustainable mechanisms to build the capacity of the early intervention/disability support workforce that include training, mentoring, and opportunities for career progression.
3.2.3. Stage 3: Outcomes—Impact of Intervention and Unmet Needs
Benefits of Access to Intervention and Supports
They [early intervention service] are able to tell us some of the techniques to do at home to help [my child]. Now he can sit on a chair together with the [other] students, and one of his biggest achievements now is that he is able to get down from the bed and go up again and get down by himself.(Caregiver, Suva)
Unmet Needs and Impact of Lack of Access to Intervention and Supports
Sometimes she wants something and I don’t really know what is it. She’ll be pointing and doing all this and indicating this and I’ll just say, “what is it you want? You tell Mama. Tell Mama, come on, you can do it.” And she’ll just start pointing. That’s the biggest challenge, the communication.(Caregiver, Suva)
I need one wheelchair…I just want him to get something to make him go here and there. Like even when he wants to go to town or something like that. I have to carry him and because I have 3 children, so I have to look after [all of] them.(Caregiver, Suva)
Recommended Actions Targeting Stage 3—Outcomes—Impact of Intervention and Unmet Needs
- Develop and resource models of care to provide interim advice and support for families on service waiting lists.
- Establish an OPD or advocacy group specifically for children with disabilities and their families, providing representation and voice to the lived experience of families of children with disabilities.
- Establish parent self-help groups, with consideration of options to meet in person or virtually using phone or digital technology, if available, to overcome issues of distance.
- Review of the disability allowance to reduce financial pressure on families of children with disabilities.
- Promote community awareness of the right to education and early education for children with disabilities, alongside adequate resourcing for inclusion in mainstream education settings.
- Increase resourcing for disability-inclusive ECE/childcare to enable caregivers to work and opportunities for appropriate stimulation and early learning for young children with disabilities.
- Establish mechanisms for the funding, procurement, and supply of paediatric assistive technology including options for local fabrication and maintenance.
- Establish a pool for paediatric equipment that children have outgrown to be re-issued to other children.
3.2.4. Cross-Sector Collaboration
If it’s like funding for children, then Ministry of Education, go okay that’s our funding because it’s children. But they don’t talk to health to say, okay, you do the health aspect and we do the education aspects,….. so, if there is better coordination, then the resources can be better put to use.(Stakeholder, Disability)
Recommended Actions Targeting Cross-Sector Collaboration
- Key ministries to have a disability focal point who collaborate with each other to coordinate actions that support for children with disabilities.
- Establishment of formal agreements and guidelines between health, education, social welfare and disability sectors as to responsibilities with regard to children with disabilities.
- Establish effective referral mechanisms between service providers across sectors and appropriate sharing of information while ensuring privacy and confidentiality.
- Consider developing a common identification tool and referral form, using consistent language across sectors.
- Ensure introduction of any identification and referral mechanisms is supported by training for relevant workers in each of the sectors.
- Develop a directory of services available for children with disabilities that is available for all sectors and the community.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guralnick, M. Effectiveness of early intervention for vulnerable children: A developmental perspective. Am. J. Ment. Retard. 1998, 102, 319–345. [Google Scholar] [CrossRef]
- Scherzer, A.L.; Chhagan, M.; Kauchali, S.; Susser, E. Global perspective on early diagnosis and intervention for children with developmental delays and disabilities. Dev. Med. Child. Neurol. 2012, 54, 1079–1084. [Google Scholar] [CrossRef]
- Olusanya, B.O.; Gulati, S.; Newton, C.; Global Research on Developmental Disabilities Collaborators. The nurturing care framework and children with developmental disabilities in LMICs. Pediatrics 2023, 151, 1–4. [Google Scholar] [CrossRef]
- Vargas-Barón, E.; Small, J.; Wertlieb, D.; Hix-Small, H.; Gómez Botero, R.; Diehl, K.; Vegara, P.; Lynch, P. Global Survey of Inclusive Early Childhood Development and Early Childhood Intervention Programs; RISE Institute: Washington, DC, USA, 2019. [Google Scholar]
- Cieza, A.; Kamenov, K.; Sanchez, M.G.; Chatterji, S.; Balasegaram, M.; Lincetto, O.; Servili, C.; Bermejo, R.; Ross, D.A. Burden of disability in children and adolescents must be integrated into the global health agenda. BMJ 2021, 372, n9. [Google Scholar] [CrossRef] [PubMed]
- Yousafzai, A.K.; Lynch, P.; Gladstone, M. Moving beyond prevalence studies: Screening and interventions for children with disabilities in low-income and middle-income countries. Arch. Dis. Child. 2014, 99, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Milner, K.M.; Bernal Salazar, R.; Bhopal, S.; Brentani, A.; Britto, P.R.; Dua, T.; Gladstone, M.; Goh, E.; Hamadani, J.; Hughes, R.; et al. Contextual design choices and partnerships for scaling early child development programmes. Arch. Dis. Child. 2019, 104, S22–S33. [Google Scholar] [CrossRef] [PubMed]
- Almasri, N.; Smythe, T.; Hadders-Algra, M.; Olusanya, B.O. Prioritising rehabilitation in early childhood for inclusive education: A call to action. Disabil. Rehabil. 2022. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Sustainable Development Goals—Goal 4 Ensure Inclusive and Equitable Quality Education and Promote Lifelong Learning Opportunities for All. Available online: https://sdgs.un.org/goals/goal4 (accessed on 14 December 2022).
- World Health Organization; UNICEF. Early Childhood Development and Disability: A Discussion Paper; WHO: Geneva, Switzerland, 2012; p. 34. Available online: https://apps.who.int/iris/bitstream/handle/10665/75355/9789241504065_eng.pdf (accessed on 14 December 2022).
- World Health Organization; UNICEF; World Bank Group. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Smythe, T.; Zuurmond, M.; Tann, C.; Gladstone, M.; Kuper, H. Early intervention for children with developmental disabilities in low and middle-income countries—The case for action. Int. Health 2021, 13, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Pacific Regional Council for Early Childhood Development (PRC4ECD). Available online: https://pacific-child.org/pacific-council/ (accessed on 13 July 2023).
- UNICEF. 2019 Pacific Early Childhood Development Forum: Implementing Pasifika Call to Action on ECD; UNICEF: Nadi, Fiji, 2020. [Google Scholar]
- World Health Organization. Global Report on Health Equity for Persons with Disabiltiies; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Fiji Bureau of Statistics. 2017 Population and Housing Census; Fiji Bureau of Statistics: Suva, Fiji, 2018. [Google Scholar]
- Fiji Bureau of Statistics. Fiji Multiple Indicator Cluster Survey 2021, Fact. Sheet; Fiji Bureau of Statistics: Suva, Fiji, 2021. [Google Scholar]
- Frank Hilton Organization. Frank Hilton Organization 2023. Available online: https://www.frankhilton.org.fj/ (accessed on 30 June 2023).
- United Nations. Convention on the Rights of Persons with Disabilities. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (accessed on 14 December 2022).
- United Nations. Convention on the Rights of the Child 1989. Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-rights-child (accessed on 14 December 2022).
- Underwood, K.; Smith, A.; Martin, J. Institutional mapping as a tool for resource consultation. J. Early Child. Res. 2019, 12, 129–139. [Google Scholar] [CrossRef]
- McCarthy, S.; O’Raghallaigh, P.; Woodworth, S.; Lim, Y.L.; Kenny, L.C.; Adam, F. An integrated patient journey mapping tool for embedding quality in healthcare service reform. J. Decis. Syst. 2016, 25, 354–368. [Google Scholar] [CrossRef]
- Ly, S.; Runacres, F.; Poon, P. Journey mapping as a novel approach to healthcare: A qualitative mixed methods study in palliative care. BMC Health Serv. Res. 2021, 21, 915. [Google Scholar] [CrossRef] [PubMed]
- Connell, E.; MartinRogers, N.; Petersen, A. Mapping the Journey of Families Who Have Children with Autism through Social and Human Services, Medical, and Education Systems; Wilder Research: Saint Paul, MN, USA, 2020. [Google Scholar]
- Nossal Institute for Global Health. Policy Brief: Early Identification and Intervention for Chidlren with Disability in Fiji: Current Practices and Opportunties. 2023. Available online: https://mspgh.unimelb.edu.au/research-groups/nossal-institute-for-global-health/completed-projects/Early-Childhood-Identification-and-Development-in-Fiji#details (accessed on 28 July 2023).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Caregiver Participant Details | ||
|---|---|---|
| Location | Suva | 4 |
| Serua | 4 | |
| Kadavu | 4 | |
| Interview participants | Female caregiver only | 9 |
| Both male and female caregivers | 3 | |
| Ethnicity | I-Taukei | 9 |
| Indo-Fijian | 3 |
| Age | Gender | Condition/s * |
|---|---|---|
| 2 | Female | Down Syndrome |
| 2 | Female | Cerebral Palsy |
| 2 | Male | Down Syndrome, Club Foot |
| 4 | Female | Autism spectrum disorder |
| 4 | Male | Cerebral Palsy |
| 4 | Male | Cerebral Palsy |
| 4 | Female | Speech delay, seizures |
| 5 | Male | Blind, cleft lip and palate |
| 5 | Male | Global developmental delay, seizures |
| 5 | Male | Global developmental delay |
| 6 | Male | Cerebral Palsy |
| 13 | Male | Cerebral Palsy |
| Stakeholder Location | Stakeholder Level | ||||
|---|---|---|---|---|---|
| Sector | Suva | Serua | Kadavu | Service Provider | Government |
| Health | 3 | 2 | 2 | 6 | 1 |
| Education | 3 | - | - | 2 | 1 |
| Disability | 3 | - | - | 2 | 1 |
| Social Support | 2 | 1 | 1 | 3 | 1 |
| Total | 11 | 3 | 3 | 13 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, F.; Perera, S.; Marella, M. The Journey to Early Identification and Intervention for Children with Disabilities in Fiji. Int. J. Environ. Res. Public Health 2023, 20, 6732. https://doi.org/10.3390/ijerph20186732
Smith F, Perera S, Marella M. The Journey to Early Identification and Intervention for Children with Disabilities in Fiji. International Journal of Environmental Research and Public Health. 2023; 20(18):6732. https://doi.org/10.3390/ijerph20186732
Chicago/Turabian StyleSmith, Fleur, Sureni Perera, and Manjula Marella. 2023. "The Journey to Early Identification and Intervention for Children with Disabilities in Fiji" International Journal of Environmental Research and Public Health 20, no. 18: 6732. https://doi.org/10.3390/ijerph20186732
APA StyleSmith, F., Perera, S., & Marella, M. (2023). The Journey to Early Identification and Intervention for Children with Disabilities in Fiji. International Journal of Environmental Research and Public Health, 20(18), 6732. https://doi.org/10.3390/ijerph20186732