

Challenges in Accessing and Delivering Maternal and Child Health Services during the COVID-19 Pandemic: A Cross-Sectional Rapid Survey from Six States of India
 , , , , , , , , , , ,
, , , , , , , , , , ,  , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Study Design and Setting
2.2. Sample Size for Patients
2.3. Sample Size for Health Care Workers
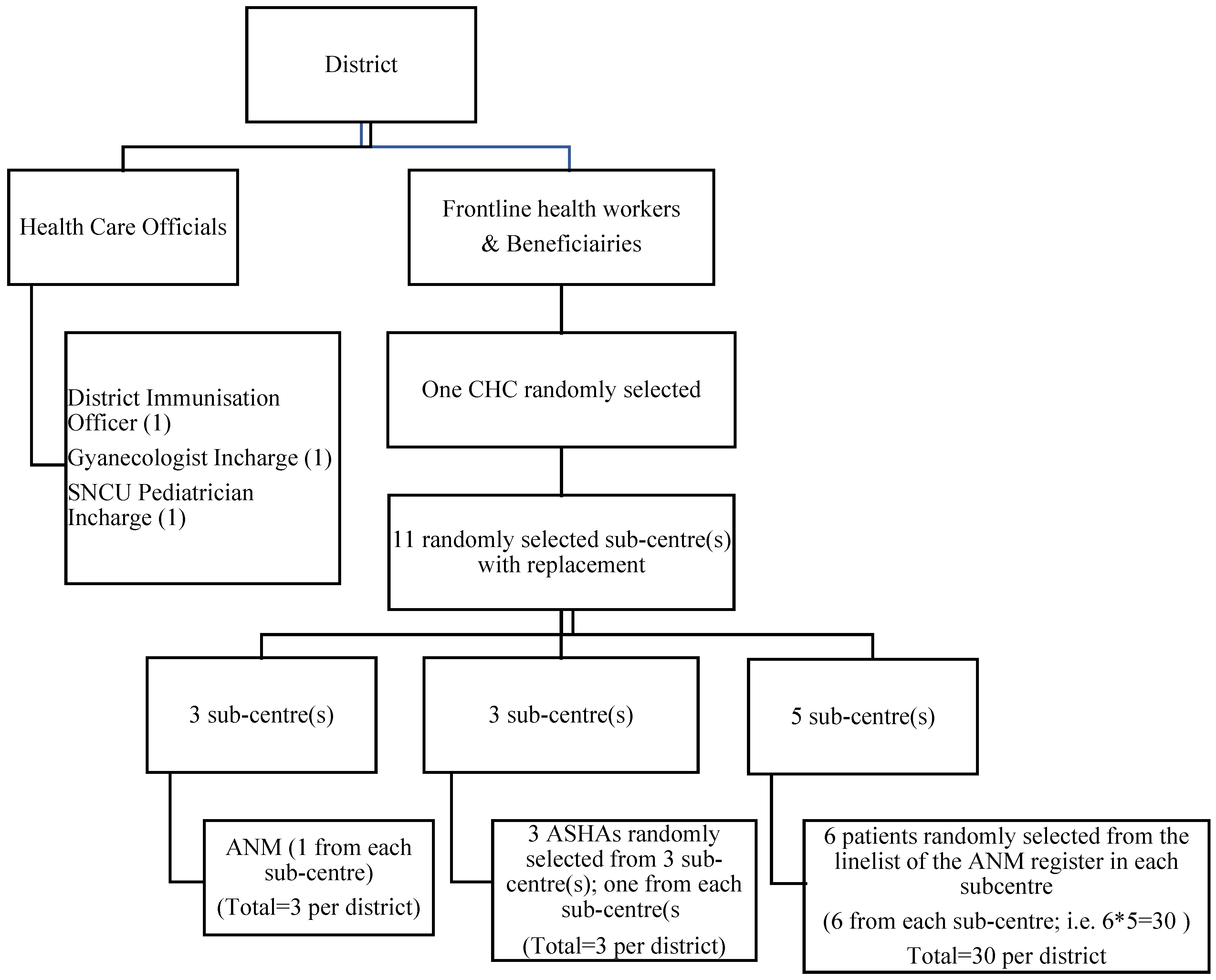
2.4. Sampling Strategy
2.4.1. Selection of MCH Patients
2.4.2. Selection of Health Care Workers
2.5. Data Collection
2.6. Data Processing and Analysis
2.7. Ethical Considerations
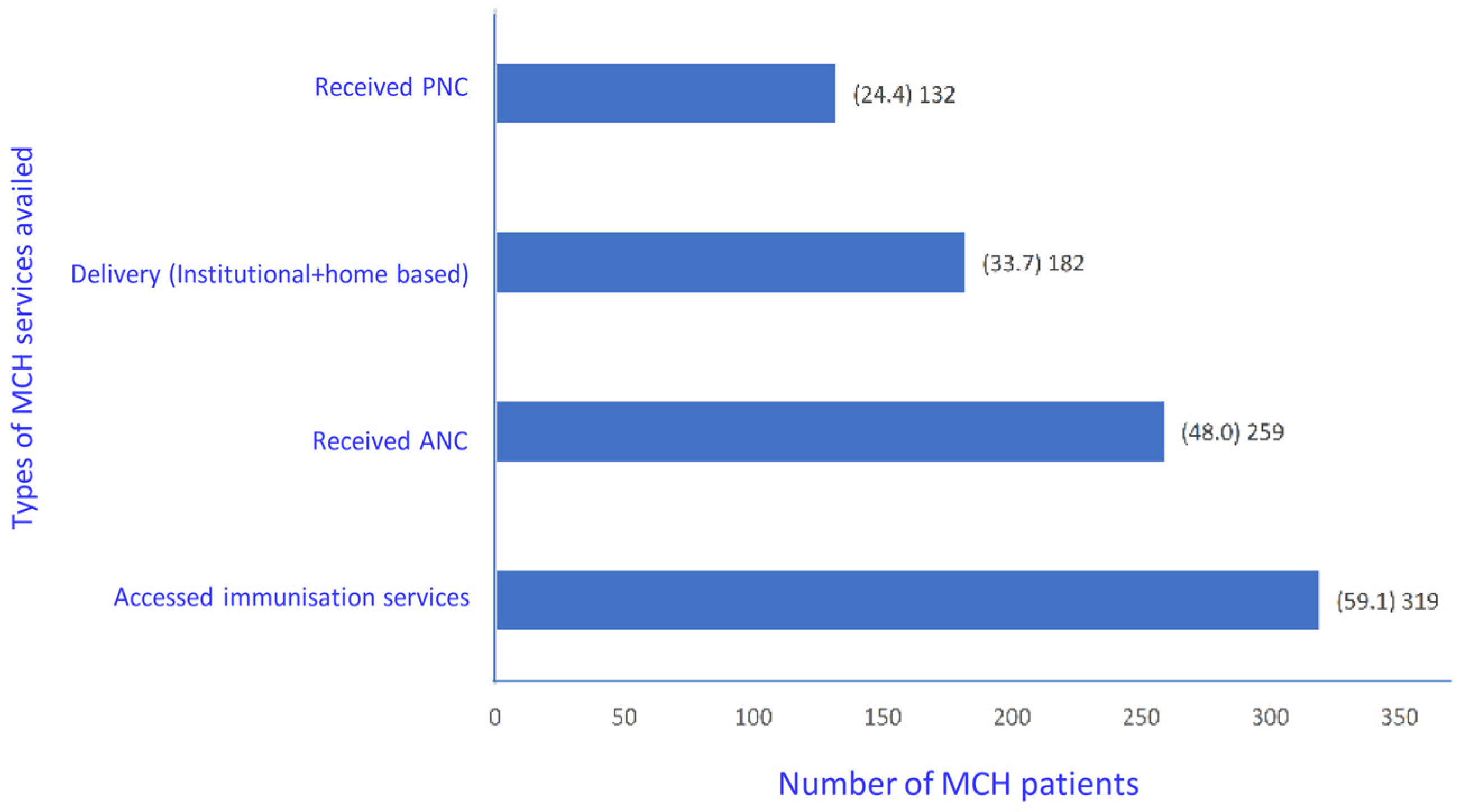
3. Results
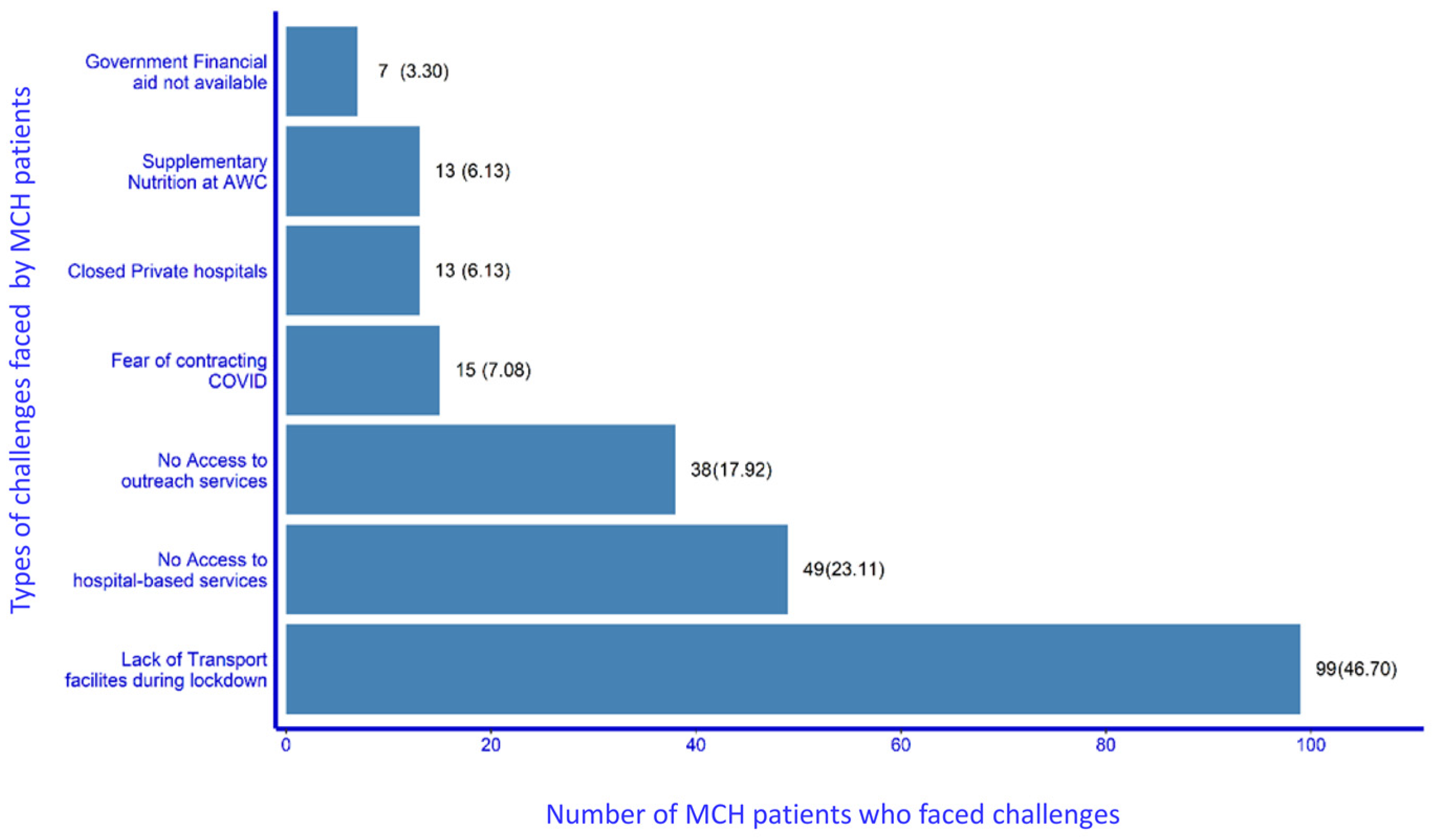
3.1. Challenges Faced by the Patients in Accessing MCH Services during the Lockdown Period
3.1.1. Institutional Services
“We faced lots of problem during going to hospital and home as we could not find any vehicle for that. whatever we found they demanded more money from us.”(MCH Beneficiary No 59)
“During Covid 19, there was no transport so my husband had to rent a private vehicle for my check-up.”(MCH Beneficiary No 75)
“During the last moment of delivery, we didn’t get any ambulance services, we went to hospital by auto.”(MCH Beneficiary No 77)
3.1.2. Outreach Services
3.2. Health Care Workers’ Experiences during the Lockdown Period of the COVID-19 Pandemic in India
3.2.1. Institutional Services
3.2.2. Outreach Services including Childhood Immunisation
4. Discussion
4.1. Implications to Policy and Practices
4.1.1. Outreach Services
4.1.2. Institutional Services
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MCH | Maternal and Child Health |
| DIO | District Immunisation Officer |
| ASHA | Accredited Social Health Activist |
| ANM | Auxiliary Nurse Midwife |
| KCR | K Chandrashekar Rao kit |
| SNCU | Special Newborn Care Unit |
References
- World Health Organization. Maintaining Essential Health Services: Operational Guidance for the COVID-19 Context: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/332240 (accessed on 1 June 2020).
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 3 June 2021).
- Shapira, G.; Ahmed, T.; Drouard, S.H.P.; Amor Fernandez, P.; Kandpal, E.; Nzelu, C.; Wesseh, C.S.; Mohamud, N.A.; Smart, F.; Mwansambo, C.; et al. Disruptions in Maternal and Child Health Service Utilization during COVID-19: Analysis from Eight Sub-Saharan African Countries. Health Policy Plan. 2021, 36, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Rahman, A.E.; Amole, T.G.; Galadanci, H.; Matjila, M.; Soma-Pillay, P.; Gillespie, B.M.; El Arifeen, S.; Anumba, D.O. The Effect of COVID-19 on Maternal Newborn and Child Health (MNCH) Services in Bangladesh, Nigeria and South Africa: Call for a Contextualised Pandemic Response in LMICs. Int. J. Equity Health 2021, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ashish, K.C.; Gurung, R.; Kinney, M.V.; Sunny, A.K.; Moinuddin, M.; Basnet, O.; Paudel, P.; Bhattarai, P.; Subedi, K.; Shrestha, M.P.; et al. Effect of the COVID-19 Pandemic Response on Intrapartum Care, Stillbirth, and Neonatal Mortality Outcomes in Nepal: A Prospective Observational Study. Lancet Glob. Health 2020, 8, e1273–e1281. [Google Scholar]
- Khalil, A.; Von Dadelszen, P.; Draycott, T.; Ugwumadu, A.; O’Brien, P.; Magee, L. Change in the Incidence of Stillbirth and Preterm Delivery during the COVID-19 Pandemic. JAMA 2020, 324, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; von Dadelszen, P.; Kalafat, E.; Sebghati, M.; Ladhani, S.; Ugwumadu, A.; Draycott, T.; O’Brien, P.; Magee, L. Change in Obstetric Attendance and Activities during the COVID-19 Pandemic. Lancet Infect. Dis. 2020, 21, e115. [Google Scholar] [CrossRef]
- Calvert, C.; John, J.; Nzvere, F.P.; Cresswell, J.A.; Fawcus, S.; Fottrell, E.; Say, L.; Graham, W.J. Maternal Mortality in the Covid-19 Pandemic: Findings from a Rapid Systematic Review. Glob. Health Action 2021, 14, 1974677. [Google Scholar] [CrossRef]
- Bauni, E.; Ndila, C.; Mochamah, G.; Nyutu, G.; Matata, L.; Ondieki, C.; Mambo, B.; Mutinda, M.; Tsofa, B.; Maitha, E.; et al. Validating Physician-Certified Verbal Autopsy and Probabilistic Modeling (InterVA) Approaches to Verbal Autopsy Interpretation Using Hospital Causes of Adult Deaths. Popul. Health Metr. 2011, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bell, D.; Hansen, K.S.; Kiragga, A.N.; Kambugu, A.; Kissa, J.; Mbonye, A.K. Predicting the Impact of COVID-19 and the Potential Impact of the Public Health Response on Disease Burden in Uganda. Am. J. Trop. Med. Hyg. 2020, 103, 1191–1197. [Google Scholar] [CrossRef]
- Riley, T.; Sully, E.; Ahmed, Z.; Biddlecom, A. Estimates of the Potential Impact of the Covid-19 Pandemic on Sexual and Reproductive Health in Low-and Middle-Income Countries. Int. Perspect. Sex. Reprod. Health 2020, 46, 73–76. [Google Scholar] [CrossRef]
- Wanyana, D.; Wong, R.; Hakizimana, D. Rapid Assessment on the Utilization of Maternal and Child Health Services during COVID-19 in Rwanda. Public Health Action 2021, 11, 12–21. [Google Scholar] [CrossRef]
- Mukunya, D.; Tumwine, J.K. Challenges of Tackling Non Covid-19 Emergencies during the Unprecedent Pandemic. Afr. Health Sci. 2020, 20, V–VI. [Google Scholar] [CrossRef] [PubMed]
- Aranda, Z.; Binde, T.; Tashman, K.; Tadikonda, A.; Mawindo, B.; Maweu, D.; Boley, E.J.; Mphande, I.; Dumbuya, I.; Montaño, M.; et al. Disruptions in Maternal Health Service Use during the COVID-19 Pandemic in 2020: Experiences from 37 Health Facilities in Low-Income and Middle-Income Countries. BMJ Glob. Health 2022, 7, e007247. [Google Scholar] [CrossRef] [PubMed]
- Semaan, A.; Audet, C.; Huysmans, E.; Afolabi, B.; Assarag, B.; Banke-Thomas, A.; Blencowe, H.; Caluwaerts, S.; Campbell, O.M.R.; Cavallaro, F.L.; et al. Voices from the Frontline: Findings from a Thematic Analysis of a Rapid Online Global Survey of Maternal and Newborn Health Professionals Facing the COVID-19 Pandemic. BMJ Glob. Health 2020, 5, e002967. [Google Scholar] [CrossRef] [PubMed]
- Balogun, M.; Banke-Thomas, A.; Sekoni, A.; Boateng, G.O.; Yesufu, V.; Wright, O.; Ubani, O.; Abayomi, A.; Afolabi, B.B.; Ogunsola, F. Challenges in Access and Satisfaction with Reproductive, Maternal, Newborn and Child Health Services in Nigeria during the COVID-19 Pandemic: A Cross-Sectional Survey. PLoS ONE 2021, 16, e0251382. [Google Scholar] [CrossRef] [PubMed]
- Graham, W.J.; Afolabi, B.; Benova, L.; Campbell, O.M.R.; Filippi, V.; Nakimuli, A.; Penn-Kekana, L.; Sharma, G.; Okomo, U.; Valongueiro, S.; et al. Protecting Hard-Won Gains for Mothers and Newborns in Low-Income and Middle-Income Countries in the Face of COVID-19: Call for a Service Safety Net. BMJ Glob. Health 2020, 5, e002754. [Google Scholar] [CrossRef]
- Cardoso, P.C.; Sousa, T.M.D.; Rocha, D.D.S.; Menezes, L.R.D.D.; Santos, L.C.D. Maternal and Child Health in the Context of COVID-19 Pandemic: Evidence, Recommendations and Challenges. Rev. Bras. De Saude Matern. Infant. 2021, 21, 213–220. [Google Scholar] [CrossRef]
- Mukherjee, A.; Bandopadhyay, G.; Chatterjee, S.S. COVID-19 Pandemic: Mental Health and beyond-The Indian Perspective. Ir. J. Psychol. Med. 2020, 38, 140–144. [Google Scholar] [CrossRef]
- Pant, S.; Koirala, S.; Subedi, M. Access to Maternal Health Services during COVID-19. Eur. J. Med. Sci. 2020, 2, 46–50. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, P.; Singh, K.; Shekhar, S.; Agrawal, N.; Misra, S. The Effect of the COVID-19 Pandemic on Maternal Health Due to Delay in Seeking Health Care: Experience from a Tertiary Center. Int. J. Gynecol. Obstet. 2021, 152, 231–235. [Google Scholar] [CrossRef]
- Singh, A.K.; Jain, P.K.; Singh, N.P.; Kumar, S.; Bajpai, P.K.; Singh, S.; Jha, M. Impact of COVID-19 Pandemic on Maternal and Child Health Services in Uttar Pradesh, India. J. Fam. Med. Prim. Care 2021, 10, 509. [Google Scholar]
- Guidance Note on Provision of Reproductive, Maternal, Newborn, Child, Adolescent Health Plus Nutrition (RMNCAH+N) Services during & Post COVID-19 Pandemic. 2020. Available online: https://www.mohfw.gov.in/pdf/UpdatedAdditionalguidelinesonrationaluseofPersonalProtectiveEquipmentsettingapproachforHealthf (accessed on 5 April 2021).
- MOHFW G of I. Categorization of Districts Based on COVID-19 Zones.MOHFW Order Dated 30/04/2020 Number 28015/19/2020-EMR [Internet]. India; 2020. Available online: https://www.mha.gov.in/sites/default/files/MHADOLrDt17052020_0.PDF. (accessed on 5 April 2021).
- Shrivastava, S.; Rai, S.; Sivakami, M. Challenges for Pregnant Women Seeking Institutional Care during the COVID-19 Lockdown in India: A Content Analysis of Online News Reports. Indian J. Med. Ethics 2021, 6, 1–24. [Google Scholar] [CrossRef] [PubMed]
- das Neves Martins Pires, P.H.; Macaringue, C.; Abdirazak, A.; Mucufo, J.R.; Mupueleque, M.A.; Zakus, D.; Siemens, R.; Belo, C.F. Covid-19 Pandemic Impact on Maternal and Child Health Services Access in Nampula, Mozambique: A Mixed Methods Research. BMC Health Serv. Res. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mishra, B.K.; Kanungo, S.; Patel, K.; Swain, S.; Dwivedy, S.; Panda, S.; Karna, S.; Bhuyan, D.; Som, M.; Merta, B.R.; et al. Resolution of Resilience: Empirical Findings on the Challenges Faced and the Mitigation Strategies Adopted by Community Health Workers (CHWs) to Provide Maternal and Child Health (MCH) Services during the COVID-19 Pandemic in the Context of Odisha, India. Healthcare 2022, 10, 88. [Google Scholar] [CrossRef] [PubMed]
- Kimani, R.W.; Maina, R.; Shumba, C.; Shaibu, S. Maternal and Newborn Care during the COVID-19 Pandemic in Kenya: Re-Contextualising the Community Midwifery Model. Hum. Resour. Health 2020, 18, 1–5. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics (n = 540) | No. of Women | Percent |
|---|---|---|
| Age in years | ||
| 15–19 | 35 | 6.5 |
| 20–24 | 256 | 47.4 |
| 25–29 | 179 | 33.1 |
| 30–34 | 54 | 10.0 |
| ≥35 | 16 | 3.0 |
| Education (years of schooling) | ||
| No schooling | 37 | 6.9 |
| Less than 5 years | 13 | 2.4 |
| 5–7 | 55 | 10.2 |
| 8–9 | 104 | 19.3 |
| 10–11 | 137 | 25.4 |
| 12 or more years | 194 | 35.9 |
| Religion | ||
| Hindu | 450 | 83.3 |
| Muslim | 72 | 13.3 |
| Others | 18 | 3.3 |
| Number of children | ||
| No child | 64 | 11.9 |
| 1 | 250 | 46.3 |
| 2 | 160 | 29.6 |
| More than 2 | 66 | 12.2 |
| Having ration card | ||
| Yes | 319 | 59.1 |
| No | 221 | 40.9 |
| Main Source of Income | ||
| Agriculture | 156 | 28.9 |
| Agricultural wages/Non-agricultural wages | 122 | 22.6 |
| Small Business | 103 | 19.1 |
| Salaried Employment/Professional | 130 | 24.1 |
| Pension/Rent/Dividend/Others | 29 | 5.4 |
| Main Source of Income During Lockdown | ||
| No Income | 307 | 56.9 |
| Government Schemes | 12 | 2.2 |
| Agriculture | 104 | 19.3 |
| Skilled/Unskilled labour | 31 | 5.7 |
| Small Business | 24 | 4.4 |
| Salaried Employment/Professional | 40 | 7.4 |
| Pension/Rent/Dividend/Others | 22 | 4.1 |
| COVID zone | ||
| Red | 361 | 66.9 |
| Green | 179 | 33.1 |
| Total | 540 | 100 |
| Socio-Demographic Characteristics | Unadjusted Odds Ratio (OR) | Adjusted Odds Ratio (OR) | ||||||
|---|---|---|---|---|---|---|---|---|
| Exp(B) | Sig. | 95% C.I. for Exp(B) | Exp(B) | Sig. | 95% C.I. for Exp(B) | |||
| Lower | Upper | Lower | Upper | |||||
| COVID zone | ||||||||
| Red | ||||||||
| Green | 0.89 | 0.54 | 0.62 | 1.29 | 0.88 | 0.518 | 0.59 | 1.31 |
| Age | ||||||||
| 15–24 | ||||||||
| 25 and above | 1.18 | 0.35 | 0.83 | 1.67 | 1.57 | 0.025 | 1.06 | 2.32 |
| Education | ||||||||
| No schooling and less than 5 years | ||||||||
| 5–7 | 1.53 | 0.30 | 0.69 | 3.40 | 1.42 | 0.402 | 0.62 | 3.24 |
| 8–9 | 1.12 | 0.75 | 0.55 | 2.31 | 0.99 | 0.969 | 0.46 | 2.09 |
| 10–11 | 1.76 | 0.11 | 0.89 | 3.48 | 1.87 | 0.092 | 0.9 | 3.88 |
| 12 or more years | 1.34 | 0.039 | 0.69 | 2.59 | 1.36 | 0.405 | 0.66 | 2.78 |
| Religion | ||||||||
| Hindu | ||||||||
| Muslim | 1.68 | 0.04 | 1.02 | 2.77 | 1.97 | 0.014 | 1.14 | 3.38 |
| Others | 1.34 | 0.54 | 0.052 | 3.47 | 1.3 | 0.597 | 0.49 | 3.45 |
| Number of children | ||||||||
| No child | ||||||||
| 1 | 0.83 | 0.51 | 0.48 | 1.45 | 0.81 | 0.474 | 0.45 | 1.45 |
| 2 | 0.76 | 0.37 | 0.42 | 1.37 | 0.68 | 0.232 | 0.36 | 1.28 |
| More than 2 | 0.49 | 0.05 | 0.24 | 1.01 | 0.36 | 0.014 | 0.16 | 0.81 |
| Having ration card | ||||||||
| No | ||||||||
| Yes | 0.99 | 0.97 | 0.70 | 1.41 | 1.02 | 0.935 | 0.7 | 1.47 |
| Main Source of Income | ||||||||
| Agriculture | ||||||||
| Agricultural wages/Non-agricultural wages | 1.27 | 0.33 | 0.79 | 2.06 | 1.5 | 0.151 | 0.86 | 2.62 |
| Salaried Employment/Professional | 0.88 | 0.59 | 0.54 | 1.42 | 0.91 | 0.747 | 0.52 | 1.61 |
| Small Business/Pension/ Rent/Dividend/Others | 1.04 | 0.87 | 0.65 | 1.67 | 0.96 | 0.882 | 0.56 | 1.66 |
| Main Source of Income During Lockdown | ||||||||
| No Income | ||||||||
| Agriculture | 1.11 | 0.64 | 0.71 | 1.75 | 1.28 | 0.362 | 0.75 | 2.19 |
| Other | 0.84 | 0.42 | 0.55 | 1.29 | 0.89 | 0.62 | 0.57 | 1.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, S.; Aggarwal, S.; Kulkarni, R.; Kumar, D.; Mishra, B.K.; Dwivedi, G.R.; Devi, K.R.; Mamidi, R.S.; Singh, K.J.; Singh, L.; et al. Challenges in Accessing and Delivering Maternal and Child Health Services during the COVID-19 Pandemic: A Cross-Sectional Rapid Survey from Six States of India. Int. J. Environ. Res. Public Health 2023, 20, 1538. https://doi.org/10.3390/ijerph20021538
Sharma S, Aggarwal S, Kulkarni R, Kumar D, Mishra BK, Dwivedi GR, Devi KR, Mamidi RS, Singh KJ, Singh L, et al. Challenges in Accessing and Delivering Maternal and Child Health Services during the COVID-19 Pandemic: A Cross-Sectional Rapid Survey from Six States of India. International Journal of Environmental Research and Public Health. 2023; 20(2):1538. https://doi.org/10.3390/ijerph20021538
Chicago/Turabian StyleSharma, Saurabh, Sumit Aggarwal, Ragini Kulkarni, Dinesh Kumar, Bijaya Kumar Mishra, Gaurav Raj Dwivedi, K. Rekha Devi, Raja Sriswan Mamidi, Khangembam Jitenkumar Singh, Lucky Singh, and et al. 2023. "Challenges in Accessing and Delivering Maternal and Child Health Services during the COVID-19 Pandemic: A Cross-Sectional Rapid Survey from Six States of India" International Journal of Environmental Research and Public Health 20, no. 2: 1538. https://doi.org/10.3390/ijerph20021538