
Demand–Resource Profiles and Job Satisfaction in the Healthcare Sector: A Person-Centered Examination Using Bayesian Informative Hypothesis Testing
 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Background: The JD–R Model and Job Satisfaction
1.2. The Interplay among Different Levels of Job Demands and Resources
1.3. JD–R Profiles in the Healthcare Sector
1.4. Association between JD–R Profiles and Employee Well-Being
2. Materials and Methods
2.1. Procedure and Participants
2.2. Measures
2.2.1. Job Demands
Workload
Patient Demands
Emotional Dissonance
Physical Demands
2.2.2. Job Resources
Control
Management Support
Peers’ Support
2.2.3. Employee Well-Being
Job Satisfaction
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics Results
3.2. Psychometric Characteristics of the Tools
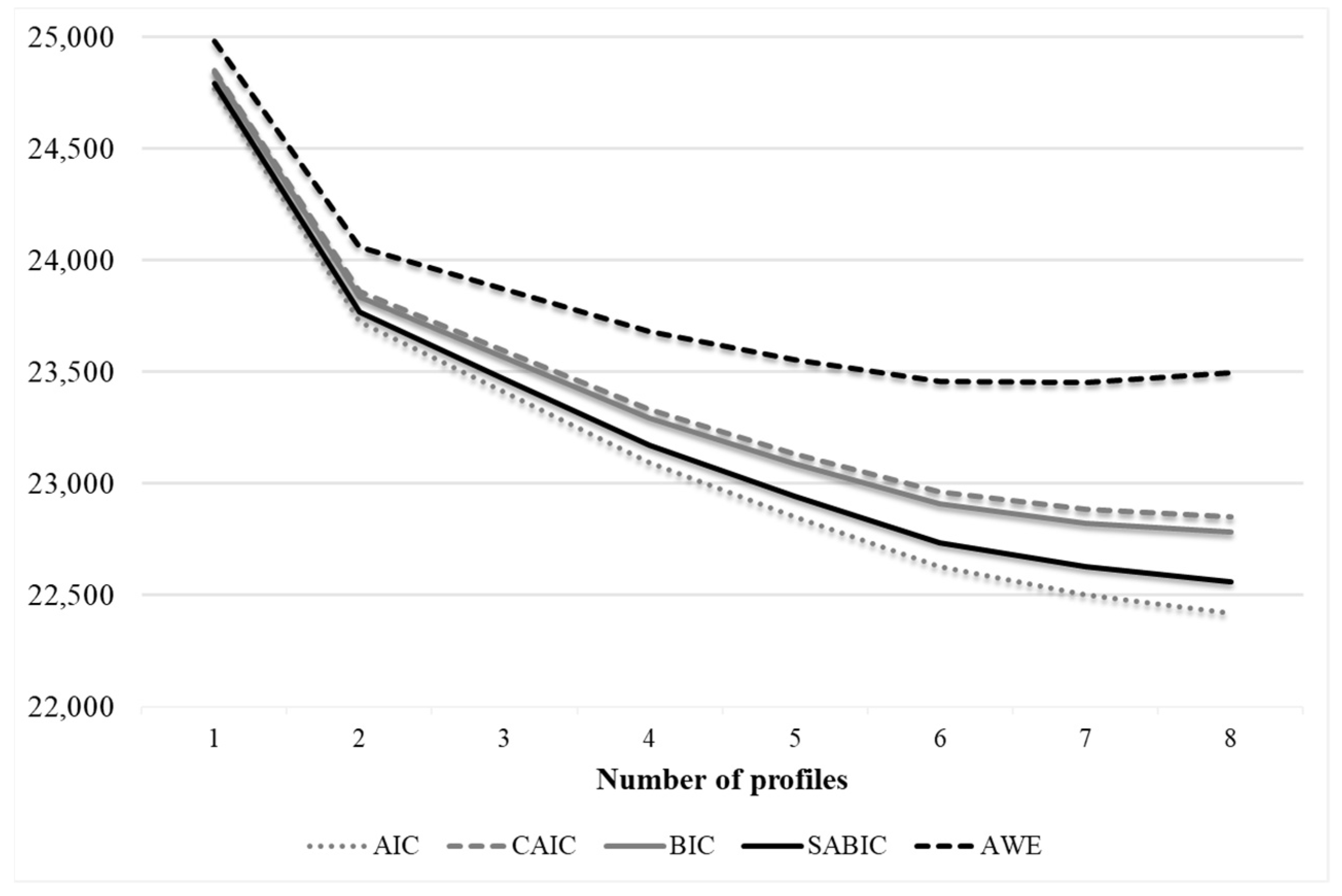
3.3. Latent Profile Analysis Results
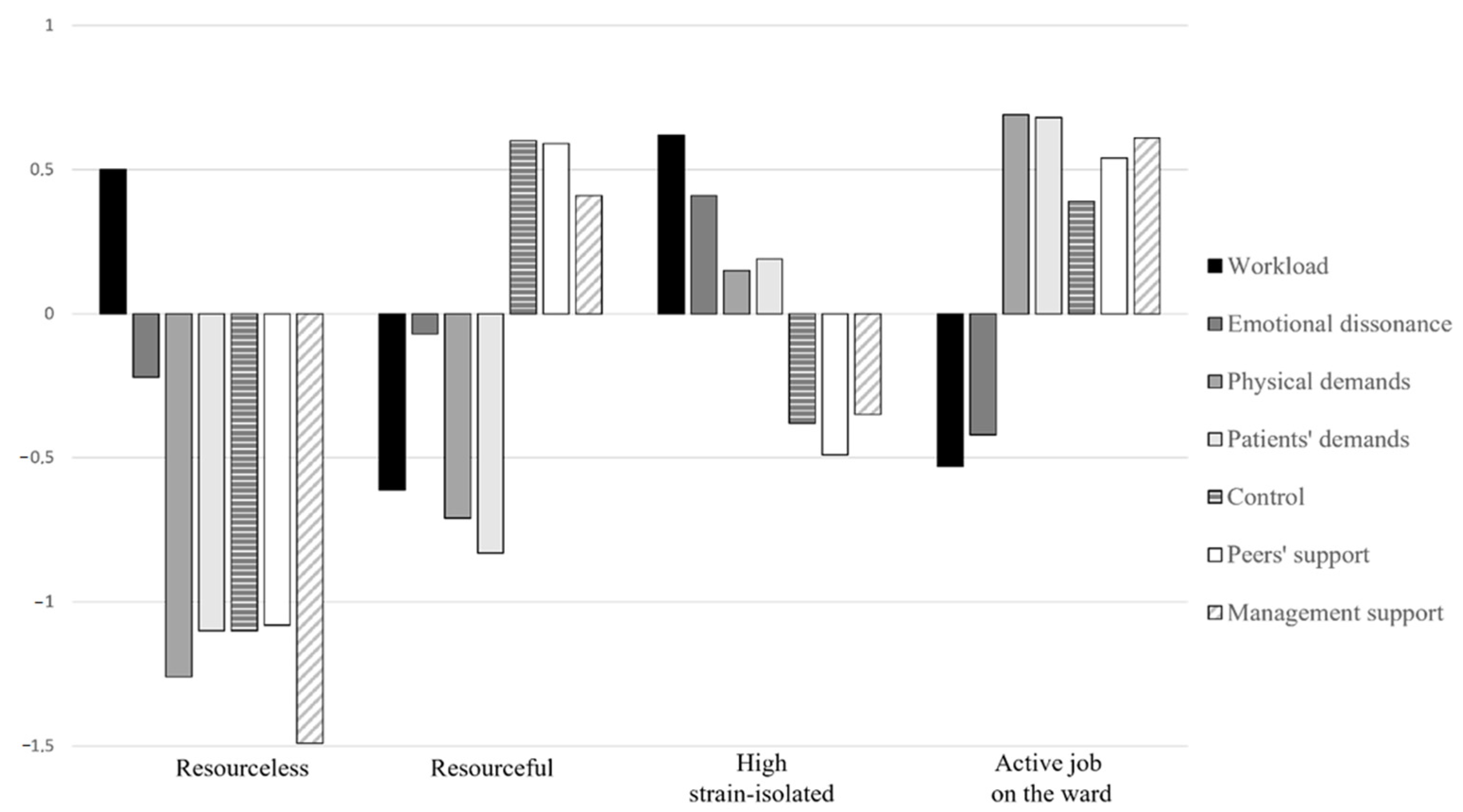
3.4. Characteristics of the JD–R Profiles
3.5. Association between JD–R Profiles and Job Satisfaction
4. Discussion
4.1. Implications for Practice in the COVID-19 Era
4.2. Study Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alarcon, G.M. A Meta-Analysis of Burnout with Job Demands, Resources, and Attitudes. J. Vocat. Behav. 2011, 79, 549–562. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Job Demands-Resources Theory: Taking Stock and Looking Forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef]
- Luchman, J.N.; González-Morales, M.G. Demands, Control, and Support: A Meta-Analytic Review of Work Characteristics Interrelationships. J. Occup. Health Psychol. 2013, 18, 37–52. [Google Scholar] [CrossRef]
- Van Der Doef, M.; Maes, S. The Job Demand-Control(-Support) Model and Psychological Well-Being: A Review of 20 Years of Empirical Research. Work Stress 1999, 13, 87–114. [Google Scholar] [CrossRef]
- Bergman, L.R.; Wångby, M. The Person-Oriented Approach: A Short Theoretical and Practical Guide. Eest. Haridusteaduste Ajak. Est. J. Educ. 2014, 2, 29–49. [Google Scholar] [CrossRef] [Green Version]
- Eurofound. Sixth European Working Conditions Survey—Overview Report; Publications Office of the European Union: Luxembourg, 2017; ISBN 9789289715966. [Google Scholar]
- Andela, M.; Truchot, D.; Van Der Doef, M. Job Stressors and Burnout in Hospitals: The Mediating Role of Emotional Dissonance. Artic. Int. J. Stress Manag. 2015, 23, 298–317. [Google Scholar] [CrossRef]
- Broetje, S.; Jenny, G.J.; Bauer, G.F. The Key Job Demands and Resources of Nursing Staff: An Integrative Review of Reviews. Front. Psychol. 2020, 11, 84. [Google Scholar] [CrossRef]
- Kluytmans, A.; van de Schoot, R.; Mulder, J.; Hoijtink, H. Illustrating Bayesian Evaluation of Informative Hypotheses for Regression Models. Front. Psychol. 2012, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E.; Nachreiner, F.; Bakker, A.B.; Schaufeli, W.B. The Job Demands-Resources Model of Burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Holman, D.; Martinez-Iñigo, D.; Totterdell, P. Emotional Labour and Employee Well-Being: An Integrative Review. Res. Companion Emot. Organ. 2008, 301–315. [Google Scholar] [CrossRef]
- Chambers, M.; Kantaris, X.; Guise, V.; Välimäki, M. Managing and Caring for Distressed and Disturbed Service Users: The Thoughts and Feelings Experienced by a Sample of English Mental Health Nurses. J. Psychiatr. Ment. Health Nurs. 2015, 22, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Heuven, E. Emotional Dissonance, Burnout, and in-Role Performance among Nurses and Police Officers. Int. J. Stress Manag. 2006, 13, 423–440. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Schaufeli, W.B.; Sixma, H.J.; Bosveld, W.; Dierendonck, D. Van Patient Demands, Lack of Reciprocity, and Burnout: A Five-Year Longitudinal Study among General Practitioners. J. Organ. Behav. 2000, 21, 425–441. [Google Scholar] [CrossRef]
- Cherniss, C. Beyond Burnout: Helping Teachers, Nurses, Therapists and Lawyers Recover From Stress and Disillusionment; Routledge: London, UK, 1995; ISBN 9781315021904. [Google Scholar]
- Rout, U.; Cooper, C.L.; Rout, J.K. Job Stress among British General Pratictioners: Predictors of Job Dissatisfaction and Mental Ill-Health. Stress Med. 1996, 12, 155–166. [Google Scholar] [CrossRef]
- Oyama, Y.; Fukahori, H. A Literature Review of Factors Related to Hospital Nurses’ Health-related Quality of Life. J. Nurs. Manag. 2015, 23, 661–673. [Google Scholar] [CrossRef]
- De Jonge, J.; Van Vegchel, N.; Shimazu, A.; Schaufeli, W.; Dormann, C. A Longitudinal Test of the Demand-Control Model Using Specific Job Demands and Specific Job Control. Int. J. Behav. Med. 2010, 17, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, T.; Serranheira, F.; Loureiro, H. Work Related Musculoskeletal Disorders in Primary Health Care Nurses. Appl. Nurs. Res. 2017, 33, 72–77. [Google Scholar] [CrossRef]
- Nedvědová, D.; Dušová, B.; Jarošová, D. Job Satisfaction of Midwives: A Literature Review. Cent. Eur. J. Nurs. Midwifery 2017, 8, 650–656. [Google Scholar] [CrossRef] [Green Version]
- Van Der Heijden, B.I.J.M.; Demerouti, E.; Bakker, A.B. Work-Home Interference among Nurses: Reciprocal Relationships with Job Demands and Health. J. Adv. Nurs. 2008, 62, 572–584. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B. Job Demands, Job Resources, and Their Relationship with Burnout and Engagement: A Multi-Sample Study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Stony Brook University: Stony Brook, NY, USA, 1990. [Google Scholar]
- Kaiser, S.; Patras, J.; Adolfsen, F.; Richardsen, A.M.; Martinussen, M. Using the Job Demands–Resources Model to Evaluate Work-Related Outcomes Among Norwegian Health Care Workers. SAGE Open 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Oshagbemi, T. Overall Job Satisfaction: How Good Are Single versus Multiple-Item Measures? J. Manag. Psychol. 1999, 14, 388–403. [Google Scholar] [CrossRef]
- Faragher, E.B.; Cass, M.; Cooper, C.L. The Relationship between Job Satisfaction and Health: A Meta-Analysis. Occup. Environ. Med. 2005, 62, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Ostroff, C. The Relationship Between Satisfaction, Attitudes, and Performance: An Organizational Level Analysis. J. Appl. Psychol. 1992, 77, 963–974. [Google Scholar] [CrossRef]
- Wright, T.A.; Cropanzano, R. Psychological Well-Being and Job Satisfaction as Predictors of Job Performance. J. Occup. Health Psychol. 2000, 5, 84–94. [Google Scholar] [CrossRef]
- Hacket, R.D. Work Attitudes and Employee Absenteeism: A Synthesis of the Literature. J. Occup. Psychol. 1989, 62, 235–248. [Google Scholar] [CrossRef]
- Carsten, J.M.; Spector, P.E. Unemployment, Job Satisfaction, and Employee Turnover: A Meta-Analytic Test of the Muchinsky Model. J. Appl. Psychol. 1987, 72, 374–381. [Google Scholar] [CrossRef]
- Chen, P.Y.; Spector, P.E. Relationships of Work Stressors with Aggression, Withdrawal, Theft and Substance Use: An Exploratory Study. J. Occup. Organ. Psychol. 1992, 65, 177–184. [Google Scholar] [CrossRef]
- Liu, Y.; Aungsuroch, Y.; Yunibhand, J. Job Satisfaction in Nursing: A Concept Analysis Study. Int. Nurs. Rev. 2016, 63, 84–91. [Google Scholar] [CrossRef]
- Bhatnagar, K.; Srivastava, K. Job Satisfaction in Health-Care Organizations. Ind. Psychiatry J. 2012, 21, 75. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources Model: State of the Art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E.; Bakker, A.B. The Job Demands-Resources Model: Challenges for Future Research. SA J. Ind. Psychol. 2011, 37, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Podsakoff, N.P.; Lepine, J.A.; Lepine, M.A. Differential Challenge Stressor-Hindrance Stressor Relationships with Job Attitudes, Turnover Intentions, Turnover, and Withdrawal Behavior: A Meta-Analysis. J. Appl. Psychol. 2007, 92, 438–454. [Google Scholar] [CrossRef] [PubMed]
- Hakanen, J.J.; Bakker, A.B.; Demerouti, E. How Dentists Cope with Their Job Demands and Stay Engaged: The Moderating Role of Job Resources. Eur. J. Oral Sci. 2005, 113, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Peters, V.; Houkes, I.; de Rijk, A.E.; Bohle, P.L.; Engels, J.A.; Nijhuis, F.J.N. Which Resources Moderate the Effects of Demanding Work Schedules on Nurses Working in Residential Elder Care? A Longitudinal Study. Int. J. Nurs. Stud. 2016, 58, 31–46. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E.; Taris, T.W.; Schaufeli, W.B.; Schreurs, P.J.G. A Multigroup Analysis of the Job Demands-Resources Model in Four Home Care Organizations. Int. J. Stress Manag. 2003, 10, 16–38. [Google Scholar] [CrossRef]
- Gonzalez-Mulé, E.; Kim, M.M.; Ryu, J.W. A Meta-Analytic Test of Multiplicative and Additive Models of Job Demands, Resources, and Stress. J. Appl. Psychol. 2021, 106, 1391–1411. [Google Scholar] [CrossRef]
- Taris, T.W. Bricks without Clay: On Urban Myths in Occupational Health Psychology. Work Stress 2006, 20, 99–104. [Google Scholar] [CrossRef]
- Fila, M.J. The Job Demands, Control, Support Model: Where Are We Now? TKM Int. J. Res. Manag. 2016, 1, 15–44. [Google Scholar]
- Terry, D.J.; Jimmieson, N.L. Work Control and Employee Well-Being: A Decade Review. In International Review of Industrial and Organizational Psychology; Wiley: Hoboken, NJ, USA, 1999; Volume 14. [Google Scholar]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An Instrument for Internationally Comparative Assessments of Psychosocial Job Characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory: A New Tool for the Assessment of Burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Brough, P.; Biggs, A. Job Demands x Job Control Interaction Effects: Do Occupation-Specific Job Demands Increase Their Occurrence? Stress Health 2015, 31, 138–149. [Google Scholar] [CrossRef]
- Sparks, K.; Cooper, C.L. Occupational Differences in the Work-Strain Relationship: Towards the Use of Situation-Specific Models. J. Occup. Organ. Psychol. 1999, 72, 219–229. [Google Scholar] [CrossRef]
- Leka, S.; Kortum, E. A European Framework to Address Psychosocial Hazards. J. Occup. Health 2008, 50, 294–296. [Google Scholar] [CrossRef] [Green Version]
- Hu, Q.; Schaufeli, W.B.; Taris, T.W. The Job Demands-Resources Model: An Analysis of Additive and Joint Effects of Demands and Resources. J. Vocat. Behav. 2011, 79, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Keller, A.C.; Igic, I.; Meier, L.L.; Semmer, N.K.; Schaubroeck, J.M.; Brunner, B.; Elfering, A. Testing Job Typologies and Identifying At-Risk Subpopulations Using Factor Mixture Models. J. Occup. Health Psychol. 2017, 22, 503–517. [Google Scholar] [CrossRef]
- Lee, Y.; Cho, D. The Effects of Job Demands, Job Resources, and Personal Resources on the Psychological Well-Being of Middle-Aged Workers in the United States: Assessing Latent Profile Differences. Int. J. Educ. Vocat. Guid. 2020, 20, 501–521. [Google Scholar] [CrossRef]
- van den Broeck, A.; de Cuyper, N.; Luyckx, K.; de Witte, H. Employees’ Job Demands-Resources Profiles, Burnout and Work Engagement: A Person-Centred Examination. Econ. Ind. Democr. 2012, 33, 691–706. [Google Scholar] [CrossRef] [Green Version]
- Spurk, D.; Hirschi, A.; Wang, M.; Valero, D.; Kauffeld, S. Latent Profile Analysis: A Review and “How to” Guide of Its Application within Vocational Behavior Research. J. Vocat. Behav. 2020, 120, 103445. [Google Scholar] [CrossRef]
- INAIL. Seconda Indagine Nazionale Sulla Salute e Sicurezza Nei Luoghi Di Lavoro (INSULA 2); Tipolitografia INAIL: Rome, Italy, 2021; ISBN 9788874846887. [Google Scholar]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and Prevalence of Burnout in Emergency Nurses: A Systematic Review of 25 Years of Research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef]
- Pisljar, T.; van der Lippe, T.; den Dulk, L. Health among Hospital Employees in Europe: A Cross-National Study of the Impact of Work Stress and Work Control. Soc. Sci. Med. 2011, 72, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Franklin, P.; Gkiouleka, A. A Scoping Review of Psychosocial Risks to Health Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2453. [Google Scholar] [CrossRef] [PubMed]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. A Model of Burnout and Life Satisfaction amongst Nurses. J. Adv. Nurs. 2000, 32, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Abraham, A.; Chaabna, K.; Doraiswamy, S.; Bhagat, S.; Sheikh, J.; Mamtani, R.; Cheema, S. Depression among Healthcare Workers in the Eastern Mediterranean Region: A Systematic Review and Meta-Analysis. Hum. Resour. Health 2021, 19, 81. [Google Scholar] [CrossRef]
- Glisson, C.; Durick, M. Predictors of Job Satisfaction and Organizational Commitment in Human Service Organizations. Adm. Sci. Q. 1988, 33, 61. [Google Scholar] [CrossRef]
- Portoghese, I.; Galletta, M.; Leiter, M.P.; Finco, G.; D’aloja, E.; Campagna, M. Job Demand–Control–Support Latent Profiles and Their Relationships with Interpersonal Stressors, Job Burnout, and Intrinsic Work Motivation. Int. J. Environ. Res. Public Health 2020, 17, 9430. [Google Scholar] [CrossRef]
- Jenull, B.B.; Wiedermann, W. The Different Facets of Work Stress: A Latent Profile Analysis of Nurses’ Work Demands. J. Appl. Gerontol. 2015, 34, 823–843. [Google Scholar] [CrossRef]
- Bujacz, A.; Rudman, A.; Gustavsson, P.; Dahlgren, A.; Tucker, P. Psychosocial Working Conditions of Shiftworking Nurses: A Long-Term Latent Transition Analysis. J. Nurs. Manag. 2021, 29, 2603–2610. [Google Scholar] [CrossRef]
- Holman, D. Job Types and Job Quality in Europe. Hum. Relat. 2013, 66, 475–502. [Google Scholar] [CrossRef] [Green Version]
- Bujacz, A.; Bernhard-Oettel, C.; Rigotti, T.; Hanson, L.M.; Lindfors, P. Psychosocial Working Conditions among High-Skilled Workers: A Latent Transition Analysis. J. Occup. Health Psychol. 2018, 23, 223–236. [Google Scholar] [CrossRef]
- Taris, T.W.; Kompier, M.A.J.; De Lange, A.H.; Schaufeli, W.B.; Schreurs, P.J.G. Learning New Behaviour Patterns: A Longitudinal Test of Karasek’s Active Learning Hypothesis among Dutch Teachers. Work Stress 2003, 17, 1–20. [Google Scholar] [CrossRef]
- De Spiegelaere, S.; Ramioul, M.; Van Gyes, G. Good Employees through Good Jobs: A Latent Profile Analysis of Job Types and Employee Outcomes in the Belgian Electricity Sector. Empl. Relat. 2017, 39, 503–522. [Google Scholar] [CrossRef]
- Moeller, J.; Ivcevic, Z.; White, A.E.; Menges, J.I.; Brackett, M.A. Highly Engaged but Burned out: Intra-Individual Profiles in the US Workforce. Career Dev. Int. 2018, 23, 86–105. [Google Scholar] [CrossRef] [Green Version]
- Landsbergis, P.A.; Schnall, P.L.; Deitz, D.; Friedman, R.; Pickering, T. The Patterning of Psychological Attributes and Distress by “Job Strain” and Social Support in a Sample of Working Men. J. Behav. Med. 1992, 15, 379–405. [Google Scholar] [CrossRef]
- Hoijtink, H. Informative Hypotheses: Theory and Practice for Behavioral and Social Scientists; Chapman and Hall/CRC: Boca Raton, FL, USA, 2011; ISBN 9780429065453. [Google Scholar]
- INAIL. The Methodology for the Assessment and Management of Work-Related Stress Risk; Tipolitografia INAIL: Rome, Italy, 2018; ISBN 978-88-7484-119-6. [Google Scholar]
- INAIL. La Metodologia per La Valutazione e Gestione Del Rischio Stress Lavoro-Correlato. Modulo Contestualizzato Al Settore Sanitario; Tipolitografia INAIL: Rome, Italy, 2022; ISBN 978-88-7484-754-9. [Google Scholar]
- Rondinone, B.M.; Persechino, B.; Castaldi, T.; Valenti, A.; Ferrante, P.; Ronchetti, M.; Iavicoli, S. Work-Related Stress Risk Assessment in Italy: The Validation Study of Health Safety and Executive Indicator Tool. G. Ital. Med. Lav. Ergon. 2012, 34, 392–399. [Google Scholar]
- Dormann, C.; Zapf, D. Customer-Related Social Stressors and Burnout. J. Occup. Health Psychol. 2004, 9, 61–82. [Google Scholar] [CrossRef]
- Zapf, D.; Holz, M. On the Positive and Negative Effects of Emotion Work in Organizations. Eur. J. Work Organ. Psychol. 2006, 15, 1–28. [Google Scholar] [CrossRef]
- Consiglio, C. Interpersonal Strain at Work: A New Burnout Facet Relevant for the Health of Hospital Staff. Burn. Res. 2014, 1, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Morin, A.J.S.; Meyer, J.P.; Creusier, J.; Biétry, F. Multiple-Group Analysis of Similarity in Latent Profile Solutions. Organ. Res. Methods 2016, 19, 231–254. [Google Scholar] [CrossRef]
- Morin, A.J.S.; Marsh, H.W.; Nagengast, B. Exploratory Structural Equation Modeling. In Structural Equation Modeling: A Second Course; Hancock, G.R., Mueller, R.O., Eds.; IAP Information Age Publishing: Charlotte, NC, USA, 2013; pp. 395–436. [Google Scholar]
- Browne, M.W. An Overview of Analytic Rotation in Exploratory Factor Analysis. Multivariate Behav. Res. 2001, 36, 111–150. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Skrondal, A.; Laake, P. Regression among Factor Scores. Psychometrika 2001, 66, 563–575. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus Statistical Analysis With Latent Variables: User’s Guide; Muthen & Muthen: Los Angeles, CA, USA, 2017; Volume 20. [Google Scholar]
- Clark, S.; Muthén, B.O. Relating Latent Class Analysis Results to Variables Not Included in the Analysis. 2009. Available online: https://www.statmodel.com/download/relatinglca.pdf (accessed on 2 January 2023).
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Marsh, H.W.; Muthén, B.; Asparouhov, T.; Lüdtke, O.; Robitzsch, A.; Morin, A.J.S.; Trautwein, U. Exploratory Structural Equation Modeling, Integrating CFA and EFA: Application to Students’ Evaluations of University Teaching. Struct. Equ. Model. 2009, 16, 439–476. [Google Scholar] [CrossRef]
- JASP Team. Version 0.15; JASP: Tokyo, Japan, 2019. [Google Scholar]
- Hoijtink, H.; Gu, X.; Mulder, J. Bayesian Evaluation of Informative Hypotheses for Multiple Populations. Br. J. Math. Stat. Psychol. 2019, 72, 219–243. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: Boston, MA, USA, 2012. [Google Scholar]
- Utriainen, K.; KyngÄs, H. Hospital Nurses’ Job Satisfaction: A Literature Review. J. Nurs. Manag. 2009, 17, 1002–1010. [Google Scholar] [CrossRef]
- Soosai-Nathan, L.; Negri, L.; Delle Fave, A. Beyond Pro-Social Behaviour: An Exploration of Altruism in Two Cultures. Psychol. Stud. Mysore 2013, 58, 103–114. [Google Scholar] [CrossRef]
- Vignoli, M.; Nielsen, K.; Guglielmi, D.; Tabanelli, M.C.; Violante, F.S. The Importance of Context in Screening in Occupational Health Interventions in Organizations: A Mixed Methods Study. Front. Psychol. 2017, 8, 1347. [Google Scholar] [CrossRef] [Green Version]
- Di Tecco, C.; Nielsen, K.; Ghelli, M.; Ronchetti, M.; Marzocchi, I.; Persechino, B.; Iavicoli, S. Improving Working Conditions and Job Satisfaction in Healthcare: A Study Concept Design on a Participatory Organizational Level Intervention in Psychosocial Risks Management. Int. J. Environ. Res. Public Health 2020, 17, 3677. [Google Scholar] [CrossRef]
- ILO. Managing Work-Related Psychosocial Risks During The COVID-19 Pandemic; ILO: Geneva, Switzerland, 2020. [Google Scholar]
- Jain, A.; Torres, L.D.; Teoh, K.; Leka, S. The Impact of National Legislation on Psychosocial Risks on Organisational Action Plans, Psychosocial Working Conditions, and Employee Work-Related Stress in Europe. Soc. Sci. Med. 2022, 302, 114987. [Google Scholar] [CrossRef]
- Leka, S.; Van Wassenhove, W.; Jain, A. Is Psychosocial Risk Prevention Possible? Deconstructing Common Presumptions. Saf. Sci. 2015, 71, 61–67. [Google Scholar] [CrossRef]
- Di Tecco, C.; Ronchetti, M.; Ghelli, M.; Russo, S.; Persechino, B.; Iavicoli, S. Do Italian Companies Manage Work-Related Stress Effectively? A Process Evaluation in Implementing the INAIL Methodology. Biomed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef]
- Holman, D.; Johnson, S.; O’connor, E. Stress Management Interventions: Improving Subjective Psychological Well-Being in the Workplace Stress Management Interventions: A Typology and Description. In Handbook of Well-Being; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Nielsen, K.; Miraglia, M. What Works for Whom in Which Circumstances? On the Need to Move beyond the ‘What Works?’ Question in Organizational Intervention Research. Hum. Relat. 2017, 70, 40–62. [Google Scholar] [CrossRef] [Green Version]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common Method Biases in Behavioral Research: A Critical Review of the Literature and Recommended Remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Mean (SD) | Skew | Kurt | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Workload | 2.4 (0.8) | 0.43 | −1.16 | (0.78) | |||||||
| 2. Emotional dissonance | 3.2 (0.8) | −0.25 | −0.23 | 0.45 *** | (0.68) | ||||||
| 3. Patient demands | 3.3 (0.8) | −0.33 | −0.11 | 0.06 * | −0.02 | (0.85) | |||||
| 4. Physical demands | 3.0 (1.0) | −0.10 | −0.80 | −0.07 ** | 0.11 *** | 0.57 *** | (0.70) | ||||
| 5. Control | 3.5 (0.9) | −0.50 | −0.02 | −0.42 *** | −0.10 *** | 0.14 *** | 0.04 | (0.82) | |||
| 6. Peers’ support | 3.7 (0.8) | −0.70 | 0.59 | −0.39 *** | −0.20 *** | 0.02 | 0.14 *** | 0.48 *** | (0.86) | ||
| 7. Management support | 3.5 (1.1) | −0.55 | −0.45 | −0.36 *** | −0.10 *** | 0.18 *** | 0.29 *** | 0.39 *** | 0.54 *** | (0.90) | |
| 8. Job satisfaction | 3.8 (1.0) | −0.73 | −0.01 | −0.25 *** | −0.40 *** | 0.07 * | 0.02 | 0.26 *** | 0.32 *** | 0.33 *** | - |
| Number of Profiles | AIC | CAIC | BIC | SABIC | AWE | LRT (p) | AdjLRT (p) | Entropy | Smallest Profile (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 24,766 | 24,853 | 24,839 | 24,794 | 24,982 | - | - | - | - |
| 2 | 23,724 | 23,860 | 23,838 | 23,768 | 24,062 | <0.001 | <0.001 | 0.722 | 35.3 |
| 3 | 23,409 | 23,594 | 23,564 | 23,469 | 23,870 | >0.05 | >0.05 | 0.703 | 14.4 |
| 4 | 23,095 | 23,330 | 23,292 | 23,171 | 23,679 | <0.05 | <0.05 | 0.729 | 8.9 |
| 5 | 22,849 | 23,134 | 23,088 | 22,942 | 23,556 | >0.05 | >0.05 | 0.774 | 7.1 |
| 6 | 22,627 | 22,961 | 22,907 | 22,736 | 23,458 | <0.001 | <0.001 | 0.774 | 5.6 |
| 7 | 22,502 | 22,886 | 22,824 | 22,627 | 23,455 | <0.01 | <0.01 | 0.768 | 5 |
| 8 | 22,420 | 22,853 | 22,783 | 22,560 | 23,496 | >0.05 | >0.05 | 0.762 | 4 |
| Variable | Resourceless M (SE) | Resourceful M (SE) | High Strain–Isolated M (SE) | Active Job on the Ward M (SE) | F Value | Partial η2 |
|---|---|---|---|---|---|---|
| Workload | 0.5 (0.1) a | −0.6 (0.04) b | 0.6 (0.03) a | −0.5 (0.03) b | 292.13 *** | 0.40 |
| Emotional dissonance | −0.2 (0.1) bc | −0.1 (0.1) b | 0.4 (0.03) a | −0.4 (0.04) c | 88.52 *** | 0.17 |
| Physical demands | −1.3 (0.1) d | −0.7 (0.04) c | 0.2 (0.03) b | 0.7 (0.03) a | 416.29 *** | 0.49 |
| Patient demands | −1.1 (0.1) d | −0.8 (0.04) c | 0.2 (0.03) b | 0.7 (0.04) a | 385.78 *** | 0.47 |
| Control | −1.1 (0.1) d | 0.6 (0.04) a | −0.4 (0.03) c | 0.4 (0.04) b | 230.41 *** | 0.34 |
| Peers’ support | −1.1 (0.1) c | 0.6 (0.04) a | −0.5 (0.03) b | 0.5 (0.04) a | 314.40 *** | 0.42 |
| Management support | −1.5 (0.1) d | 0.4 (0.04) b | −0.4 (0.03) c | 0.6 (0.04) a | 333.34 *** | 0.43 |
| Variable | Resourceless | Resourceful | High Strain–Isolated | Active Job on the Ward | Test Statistic | Effect Size |
|---|---|---|---|---|---|---|
| Gender (N, %) | χ2(3) = 8.63 * | 0.08 a | ||||
| Male | 40 (35.7) | 69 (24.1) | 131 (25.2) | 120 (30.5) | ||
| Female | 72 (64.3) | 217 (75.9) | 389 (74.8) | 273 (69.5) | ||
| Age (N, %) | χ2(6) = 27.17 *** | 0.10 b | ||||
| Up to 30 | 4 (3.6) | 13 (4.5) | 28 (5.4) | 34 (8.6) | ||
| 31 to 50 | 67 (60.4) | 126 (43.9) | 277 (53.4) | 226 (57.4) | ||
| More than 50 | 40 (36) | 148 (51.6) | 214 (41.2) | 134 (34) | ||
| Type of contract (N, %) | χ2(12) = 17.36 | 0.12 b | ||||
| Permanent | 106 (94.6) | 268 (93.4) | 490 (94.2) | 358 (90.9) | ||
| Fixed term | 4 (3.6) | 10 (3.5) | 24 (4.6) | 21 (5.3) | ||
| Collaboration | 0 (0) | 0 (0) | 1 (0.2) | 4 (1) | ||
| Temporary | 0 (0) | 6 (2.1) | 3 (0.6) | 8 (2) | ||
| Other | 2 (1.8) | 3 (1) | 2 (0.4) | 3 (0.8) | ||
| Shift work (N, %) | χ2(3) = 115.11 *** | 0.30 a | ||||
| Yes | 77 (68.1) | 100 (34.8) | 350 (67.2) | 285 (72.3) | ||
| No | 36 (31.9) | 187 (65.2) | 171 (32.8) | 109 (27.7) | ||
| Organizational tenure in years (M, SD) | 16 (9.7) | 18.9 (11.3) | 16.2 (11.2) | 14.8 (11.6) | F(3) = 7.51 *** | 0.02 c |
| Informative Hypotheses | (In)Equality Constraints | Bayes Factor (BF) | Posterior Model Probability (PMP) |
|---|---|---|---|
| H0 | µActive = µResful = µResless = µStrain | 0.00 | 0.00 |
| H1 | µActive > µResful > µResless > µStrain | 23.08 | 0.45 |
| H2 | µResful > µActive > µResless > µStrain | 0.00 | 0.00 |
| H3 | µActive > µResful > µStrain > µResless | 1.23 | 0.02 |
| H4 | µActive > µResful > µResless = µStrain | 27.43 | 0.53 |
| H5 | µActive = µResful > µStrain = µResless | 0.02 | 0.00 |
| H6 | µResful > µActive > µStrain > µResless | 0.00 | 0.00 |
| H7 | µActive = µResful > µResless > µStrain | 0.01 | 0.00 |
| H8 | µActive = µResful > µStrain > µResless | 0.00 | 0.00 |
| H9 | µResful > µActive > µResless = µStrain | 0.00 | 0.00 |
| BF4,1 | 1.19 | ||
| Comparisons | Mean Difference (SE) | Cohen’s d | |
|---|---|---|---|
| Resourceless | Resourceful | −0.33 (0.1) | −0.34 ** |
| High strain–isolated | 0.16 (0.1) | 0.17 | |
| Active job on the ward | −0.66 (0.1) | −0.68 *** | |
| Resourceful | High strain–isolated | 0.50 (0.1) | 0.51 *** |
| Active job on the ward | −0.33 (0.1) | −0.33 *** | |
| High strain–isolated | Active job on the ward | −0.82 (0.1) | −0.84 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marzocchi, I.; Ghezzi, V.; Di Tecco, C.; Ronchetti, M.; Ciampa, V.; Olivo, I.; Barbaranelli, C. Demand–Resource Profiles and Job Satisfaction in the Healthcare Sector: A Person-Centered Examination Using Bayesian Informative Hypothesis Testing. Int. J. Environ. Res. Public Health 2023, 20, 967. https://doi.org/10.3390/ijerph20020967
Marzocchi I, Ghezzi V, Di Tecco C, Ronchetti M, Ciampa V, Olivo I, Barbaranelli C. Demand–Resource Profiles and Job Satisfaction in the Healthcare Sector: A Person-Centered Examination Using Bayesian Informative Hypothesis Testing. International Journal of Environmental Research and Public Health. 2023; 20(2):967. https://doi.org/10.3390/ijerph20020967
Chicago/Turabian StyleMarzocchi, Ivan, Valerio Ghezzi, Cristina Di Tecco, Matteo Ronchetti, Valeria Ciampa, Ilaria Olivo, and Claudio Barbaranelli. 2023. "Demand–Resource Profiles and Job Satisfaction in the Healthcare Sector: A Person-Centered Examination Using Bayesian Informative Hypothesis Testing" International Journal of Environmental Research and Public Health 20, no. 2: 967. https://doi.org/10.3390/ijerph20020967