
Utilization of Proximate Healthcare Facilities and Children’s Wait Times in Senegal: An IV-Tobit Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Participation Consent and Ethical Compliance
2.3. Limitation of the Study
2.4. Analytical Model3
3. Results
3.1. Facilities Attended by Sick Children and Waiting Time
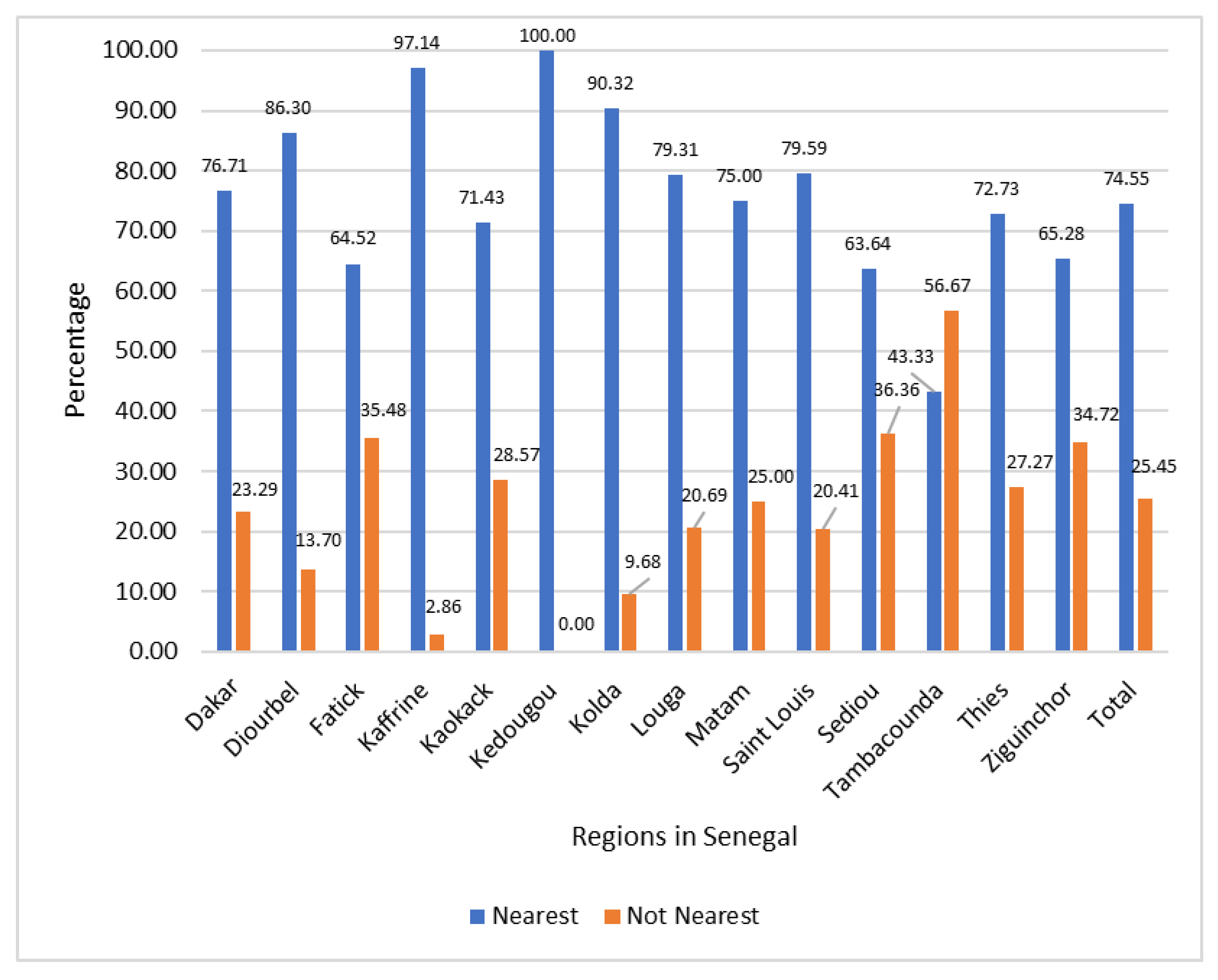
3.2. Children’s Utilization of the Nearest Healthcare Facilities
3.3. Determinants of Sick Children’s Utilization of the Nearest Healthcare Facilities
3.4. Determinants of Child’s Healthcare Utilization Waiting Time
4. Discussion
4.1. Healthcare Proximity and Types
4.2. Caregivers’ Characteristics and Perception of Sickness’ Seriousness
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sdgs.un.org/2030agenda (accessed on 13 May 2023).
- United Nations Development Programme (UNDP). Goal 3 Good Health and Well-,2Being. Available online: https://www.undp.org/sustainable-development-goals/good-health (accessed on 13 May 2023).
- World Health Organization (WHO). Close to One Billion People Globally Are Served by Health-Care Facilities with No Electricity Access or with Unreliable Electricity. 2023. Available online: https://www.who.int/news/item/14-01-2023-close-to-one-billion-people-globally-are-served-by-health-care-facilities-with-no-electricity-access-or-with-unreliable-electricity (accessed on 14 May 2023).
- Howden-Chapman, P.; Siri, J.; Chisholm, E.; Chapman, R.; Doll, C.N.; Capon, A. SDG 3: Ensure Healthy Lives and Promote Wellbeing for All at All Ages. A Guide to SDG Interactions: From Science to Implementation; International Council for Science: Paris, France, 2017; pp. 81–126. Available online: https://council.science/wp-content/uploads/2017/03/SDGs-interactions-3-healthy-lives.pdf (accessed on 5 October 2023).
- World Bank and World Health Organization (WHO). World Bank and WHO: Half the World Lacks Access to Essential Health Services, 100 Million still Pushed into Extreme Poverty Because of Health Expenses. 2017. Available online: https://www.who.int/news/item/13-12-2017-world-bank-and-who-half-the-world-lacks-access-to-essential-health-services-100-million-still-pushed-into-extreme-poverty-because-of-health-expenses#:~:text=of%20health%20expenses-,World%20Bank%20and%20WHO%3A%20Half%20the%20world%20lacks%20access%20to,poverty%20because%20of%20health%20expenses&text=At%20least%20half%20of%20the,the%20World%20Bank%20and%20WHO (accessed on 14 May 2023).
- Sanogo, N.D.; Fantaye, A.W.; Yaya, S. Universal health coverage and facilitation of equitable access to care in Africa. Front. Public Health 2019, 26, 102. [Google Scholar] [CrossRef] [PubMed]
- Derkyi-Kwarteng, A.N.; Agyepong, I.A.; Enyimayew, N.; Gilson, L. A narrative synthesis review of out-of-pocket payments for health services under insurance regimes: A policy implementation gap hindering universal health coverage in sub-Saharan Africa. Int. J. Health Policy Manag. 2021, 10, 443. [Google Scholar] [CrossRef] [PubMed]
- République du Sénégal, Ministère de la Santé et de l’Action Sociale (MSAS). Stratégie Nationale de Financement de la Santé (SNFS) Pour Tendre vers la Couverture Sanitaire Universelle; MSAS: Dakar, Senegal, 2017. [Google Scholar]
- World Health Organization. Primary Health Care on the Road to Universal Health Coverage-2019 Monitoring Report; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Performances Majeures de la CMU [Internet] Agence de la Couverture Maladie Universelle. 2019. Available online: http://www.agencecmu.sn/performances-majeurs-de-la-cmu (accessed on 22 May 2020).
- UNICEF. Child Malnutrition. 2023. Available online: https://data.unicef.org/topic/nutrition/malnutrition/ (accessed on 17 May 2023).
- Ridde, V.; Kane, B.; Mbow, N.B.; Senghor, I.; Faye, A. The resilience of two departmental health insurance units during the COVID-19 pandemic in Senegal. BMJ Glob. Health 2022, 7 (Suppl. S9), e010062. [Google Scholar] [CrossRef]
- Waelkens, M.-P.; Werner, S.; Bart, C. Community Health Insurance in Low- and Middle-Income Countries. In International Encyclopedia of Public Health; Elsevier: Amsterdam, The Netherlands, 2017; pp. 82–92. [Google Scholar]
- Daff, B.M.; Diouf, S.; Diop, E.S.M.; Mano, Y.; Nakamura, R.; Sy, M.M.; Tobe, M.; Togawa, S.; Ngom, M. Reforms for financial protection schemes towards universal health coverage, Senegal. Bull. World Health Organ. 2020, 98, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Ly, M.S.; Faye, A.; Ba, M.F. Impact of community-based health insurance on healthcare utilisation and outof-pocket expenditures for the poor in Senegal. BMJ Open 2022, 12, e063035. [Google Scholar] [CrossRef]
- Agence Nationale de la Statistique et de la Démographie, ICF. Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue 2019)—Tableaux; ANSD et ICF: Rockville, MD, USA, 2020; Available online: https://www.dhsprogram.com/pubs/pdf/FR368/FR368.T.pdf (accessed on 5 October 2023).
- Blanchet, K.; Gordon, I.; Gilbert, C.E.; Wormald, R.; Awan, H. How to achieve universal coverage of cataract surgical services in developing countries: Lessons from systematic reviews of other services. Ophthalmic Epidemiol. 2012, 19, 329–339. [Google Scholar] [CrossRef]
- Morgan, R.; Ensor, T.; Waters, H. Performance of private sector health care: Implications for universal health coverage. Lancet 2016, 388, 606–612. [Google Scholar] [CrossRef]
- Sun, J.; Lin, Q.; Zhao, P.; Zhang, Q.; Xu, K.; Chen, H.; Hu, C.J.; Stuntz, M.; Li, H.; Liu, Y. Reducing wait times and raising outpatient satisfaction in a Chinese public tertiary general hospital-an interrupted time series study. BMC Public Health 2017, 17, 668. [Google Scholar] [CrossRef]
- Wouters, A. Essential national health research in developing countries: Health care financing and the quality of care. Int. J. Health Plan. Manag. 1991, 6, 253–271. [Google Scholar] [CrossRef]
- McPake, B. User charges for health services in developing countries: A review of the economic literature. Soc. Sci. Med. 1993, 36, 1397–1405. [Google Scholar] [CrossRef]
- Gilson, L.; Alilio, M.; Heggenhougen, K. Community satisfaction with primary health care services: An evaluation undertaken in the Morogoro region of Tanzania. Soc. Sci. Med. 1994, 39, 767–780. [Google Scholar] [CrossRef]
- Aharony, L.; Strasser, S. Patient satisfaction: What we know about and we still need to explore. Med. Care Rev. 1993, 50, 49–79. [Google Scholar] [CrossRef]
- Ware, J.; Snyder, M.; Wright, W.; Davies, A. Defining and measuring patient satisfaction with medical care. Eval. Program Plan. 1983, 6, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Landi, S.; Ivaldi, E.; Testi, A. Socioeconomic Status and Waiting Times for Health Services: Current Evidences and Next Area of Research. Health Serv. Insights 2019, 12, 1178632919871295. [Google Scholar] [CrossRef] [PubMed]
- Monstad, K.; Engesæter, L.B.; Espehaug, B. Waiting time and socioeconomic status—An individual-level analysis. Health Econ. 2014, 23, 446–461. [Google Scholar] [CrossRef] [PubMed]
- Laudicella, M.; Siciliani, L.; Cookson, R. Waiting times and socioeconomic status: Evidence from England. Soc. Sci. Med. 2012, 74, 1331–1341. [Google Scholar] [CrossRef]
- García-Corchero, J.D.; Jiménez-Rubio, D. Waiting times in healthcare: Equal treatment for equal need? Int. J. Equity Health 2022, 21, 184. [Google Scholar] [CrossRef]
- McIntyre, D.; Marschner, S.; Thiagalingam, A.; Pryce, D.; Chow, C.K. Impact of Socio-demographic Characteristics on Time in Outpatient Cardiology Clinics: A Retrospective Analysis. Inquiry 2023, 60, 469580231159491. [Google Scholar] [CrossRef]
- Gallego, G.; Dew, A.; Lincoln, M.; Bundy, A.; Chedid, R.J.; Bulkeley, K.; Brentnall, J.; Veitch, C. Access to therapy services for people with disability in rural Australia: A carers’ perspective. Health Soc. Care Community 2017, 25, 1000–1010. [Google Scholar] [CrossRef]
- Ndu, I.K.; Osuorah, C.D.I.; Amadi, O.F.; Ekwochi, U.; Ekeh, B.C.; Nduagubam, O.C.; Okeke, I.B. Evaluation of Wait Time in the Children’s Emergency and Outpatient Units of a Tertiary Hospital in Southeast Nigeria. J. Emerg. Trauma Shock 2020, 13, 78–83. [Google Scholar] [CrossRef]
- James, C.A.; Bourgeois, F.T.; Shannon, M.W. Association of race/ethnicity with emergency department wait times. Pediatrics 2005, 115, e310–e315. [Google Scholar] [CrossRef] [PubMed]
- Park, C.Y.; Lee, M.A.; Epstein, A.J. Variation in emergency department wait times for children by race/ethnicity and payment source. Health Serv. Res. 2009, 44, 2022–2039. [Google Scholar] [CrossRef]
- Wagenaar, B.H.; Gimbel, S.; Hoek, R.; Pfeiffer, J.; Michel, C.; Cuembelo, F.; Quembo, T.; Afonso, P.; Gloyd, S.; Lambdin, B.H.; et al. Wait and consult times for primary healthcare services in central Mozambique: A time-motion study. Glob. Health Action 2016, 9, 31980. [Google Scholar] [CrossRef] [PubMed]
- Newman, R.; Gloyd, S.; Nyangezi, J.; Machobo, F.; Muiser, J. Satisfaction with outpatient health care services in Manica Province, Mozambiaue. Health Policy Plan. 1998, 13, 174–180. [Google Scholar] [CrossRef]
- Harper, P.R.; Gamlin, H.M. Reduced outpatient wait times with improved appointment scheduling: A simulation modeling approach. OR Spectr. 2003, 25, 207–222. [Google Scholar] [CrossRef]
- Demographic and Health Survey (DHS). Definition of Urban and Rural Areas. Available online: https://dhsprogram.com/pubs/pdf/FR01/11AppendixA.pdf (accessed on 5 October 2023).
- Demographic and Health Survey (DHS). Protecting the Privacy of DHS Survey Respondents. Available online: https://dhsprogram.com/methodology/Protecting-the-Privacy-of-DHS-Survey-Respondents.cfm (accessed on 3 October 2023).
- Agence Nationale de la Statistique et de la Démographie (ANSD) et ICF. Sénégal: Enquête Continue sur la Prestation des Services de Soins de Santé (ECPSS) 2018; ANSD et ICF: Dakar, Sénégal; Rockville, MD, USA, 2020. [Google Scholar]
- Chesher, A.; Kim, D.; Rosen, A.M.; IV Methods for Tobit Models. The Institute for Fiscal Studies Department of Economics, UCL Cemmap Working Paper CWP16/22. 2023. Available online: https://ifs.org.uk/sites/default/files/2022-10/CWP1622-IV-Methods-for-Tobit-Models.pdf (accessed on 7 June 2023).
- Ridde, V.; Sombie, I. Street-level workers’ criteria for identifying indigents to be exempted from user fees in Burkina Faso. Trop. Med. Int. Health 2012, 17, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Ridde, V. “The problem of the worst-off is dealt with after all other issues”: The equity and health policy implementation gap in Burkina Faso. Soc. Sci. Med. 2008, 66, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghanim, S.A. Factors influencing the utilisation of public and private primary health care services in Riyadh City. JKAU Econ. Adm. 2004, 19, 3–27. [Google Scholar] [CrossRef]
- Awoyemi, T.T.; Obayelu, O.A.; Opaluwa, H.I. Effect of distance on utilization of health care services in rural Kogi State, Nigeria. J. Hum. Ecol. 2011, 35, 1–9. [Google Scholar] [CrossRef]
- Paul, P.; Chouhan, P. Socio-demographic factors influencing utilization of maternal health care services in India. Clin. Epidemiol. Glob. Health 2020, 8, 666–670. [Google Scholar] [CrossRef]
- Obiechina, G.O.; Ekenedo, G.O. Factors affecting utilization of university health services in a tertiary institution in South-West Nigeria. Niger. J. Clin. Pract. 2013, 16, 454–457. [Google Scholar] [CrossRef]
- Paul, E.; Ndiaye, Y.; Sall, F.L.; Fecher, F.; Porignon, D. An assessment of the core capacities of the Senegalese health system to deliver Universal Health Coverage. Health Policy Open 2020, 1, 100012. [Google Scholar] [CrossRef]
- République du Sénégal, Ministère de la Santé et de l’Action sociale Plan National de Développement Sanitaire et Social (PNDSS) 2019–2028. 2019. Available online: http://www.sante.gouv.sn/publications/plan-national-de-développement-sanitaire-et-social-2019-2028 (accessed on 18 May 2020).
- Masango-Makgobela, A.T.; Govender, I.; Ndimande, J.V.; Ndimande, J.V. Reasons patients leave their nearest healthcare service to attend Karen Park Clinic, Pretoria North. Afr. J. Prim. Health Care Fam. Med. 2013, 5, 1–5. [Google Scholar] [CrossRef]
- USAID. Senegal’s Community-Based Health System Model: Structure, Strategies, and Learning. 2019. Available online: https://www.advancingpartners.org/sites/default/files/technical-briefs/apc_senegal_brief_508.pdf (accessed on 7 August 2023).
- Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal], and ICF. Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue 2017); ANSD and ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Salif, N.; Ayad, M. Enquête Démographique et de Santé au Sénégal 2005; Centre de Recherche pour le Développement Humain [Sénégal] and ORC Macro: Calverton, MD, USA, 2006. [Google Scholar]
- Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal], et ICF. Sénégal: Enquête Démographique et de Santé Continue (EDS-Continue 2015); ANSD et ICF: Rockville, MD, USA, 2016. [Google Scholar]
- PHCPI. Senegal: Physical Infrastructure. Available online: https://www.improvingphc.org/senegal-physical-infrastructure (accessed on 6 August 2023).
- Bettina, B.; Barnes, J.; Carmona, A.; Kpangon, A.; Riley, P.; Mohebbi, E.; Miles, L. Senegal Private Health Sector Assessment: Selected Health Products and Services. In Strengthening Health Outcomes through the Private Sector Project; Abt Associates: Bethesda, MD, USA, 2016. [Google Scholar]
- Hong, T.K.; Dibley, M.J.; Tuan, T. Factors affecting utilization of health care services by mothers of children ill with diarrhea in rural Vietnam. Southeast Asian J. Trop. Med. Public Health 2003, 34, 187–198. [Google Scholar] [PubMed]
- Feikin, D.R.; Nguyen, L.M.; Adazu, K.; Ombok, M.; Audi, A.; Slutsker, L.; Lindblade, K.A. The impact of distance of residence from a peripheral health facility on pediatric health utilisation in rural western Kenya. Trop. Med. Int. Health 2009, 14, 54–61. [Google Scholar] [CrossRef]
- Becker, S.; Peters, D.H.; Gray, R.H.; Gultiano, C.; Black, R.E. The determinants of use of maternal and child health services in Metro Cebu, the Philippines. Health Transit. Rev. 1993, 3, 77–89. [Google Scholar]
- Sreeramareddy, C.T.; Shankar, R.P.; Sreekumaran, B.V.; Subba, S.H.; Joshi, H.S.; Ramachandran, U. Care seeking behaviour for childhood illness-a questionnaire survey in western Nepal. BMC Int. Health Hum. Rights 2006, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Black, D.; Morris, J.N.; Smith, C.; Townsend, P.; Whitehead, M. Inequalities in Health: The Black Report. The Health Divide; Penguin: London, UK, 1988. [Google Scholar]
- Gage, T.B.; Fang, F.; O’Neill, E.; Dirienzo, G. Maternal education, birth weight, and infant mortality in the United States. Demography 2013, 50, 615–635. [Google Scholar] [CrossRef]
- Prickett, K.C.; Augustine, J.M. Maternal Education and Investments in Children’s Health. J. Marriage Fam. 2016, 78, 7–25. [Google Scholar] [CrossRef]
- Amwonya, D.; Kigosa, N.; Kizza, J. Female education and maternal health care utilization: Evidence from Uganda. Reprod. Health 2022, 19, 142. [Google Scholar] [CrossRef]
- Nagai, M.; Fujita, N.; Diouf, I.S.; Salla, M. Retention of qualified healthcare workers in rural Senegal: Lessons learned from a qualitative study. Rural Remote Health 2017, 17, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kahabuka, C.; Kvale, G.; Moland, K.M.; Hinderaker, S.G. Why caretakers bypass primary health care facilities for child care—A case from rural Tanzania. BMC Health Serv. Res. 2011, 11, 315. [Google Scholar] [CrossRef] [PubMed]
- Federal Ministry of Health. Guideline for Implementation of a Patient Referral System. Addis Ababa, Ethiopia 2010 [27/05/2021]. Available online: https://www.medbox.org/pdf/5e148832db60a2044c2d3f0e (accessed on 12 July 2023).
- Oyekale, A.S. Assessment of Malawian Mothers’ Malaria Knowledge, Healthcare Preferences and Timeliness of Seeking Fever Treatments for Children Under Five. Int. J. Environ. Res. Public Health 2015, 12, 521–540. [Google Scholar] [CrossRef]
- Bekele, M.; Urgessa, M.; Kumsa, K.; Sinba, E. Contributing factors of delay in seeking treatment for childhood diarrheal diseases in Berbere Woreda, Ethiopia: An unmatched case–control study. J. Health Popul. Nutr. 2023, 42, 65. [Google Scholar] [CrossRef]
- Lungu, E.A.; Biesma, R.; Chirwa, M.; Darker, C. Healthcare seeking practices and barriers to accessing under-five child health services in urban slums in Malawi: A qualitative study. BMC Health Serv. Res. 2016, 16, 410. [Google Scholar] [CrossRef] [PubMed]
- Kassile, T.; Lokina, R.; Mujinja, P.; Mmbando, B.P. Determinants of delay in care seeking among children under five with fever in Dodoma region, central Tanzania: A cross-sectional study. Malar. J. 2014, 13, 348. [Google Scholar] [CrossRef]
- Abdulraheem, I.S.; Parakoyi, D.B. Factors affecting mothers’ healthcare-seeking behaviour for childhood illnesses in a rural Nigerian setting. Early Child Dev. Care 2009, 179, 671–683. [Google Scholar] [CrossRef]
- Falade, C.O.; Ogundiran, M.O.; Bolaji, M.O.; Ajayi, I.O.; Akinboye, D.O.; Oladepo, O.; Adeniyi, J.D.; Oduola, A.M. The Influence of Cultural Perception of Causation, Complications, and Severity of Childhood Malaria on Determinants of Treatment and Preventive Pathways. Int. Q. Community Health Educ. 2005, 24, 347–363. [Google Scholar] [CrossRef]
- Williams, A.; O’Rourke, P.; Keogh, S. Making choices: Why parents present to the emergency department for non-urgent care. Arch. Dis. Child. 2009, 94, 817–820. [Google Scholar] [CrossRef]
- Mensah, B.N.; Agyemang, I.B.; Afriyie, D.K.; Amponsah, S.K. Self-medication practice in Akuse, a rural setting in Ghana. Niger. Postgrad. Med. J. 2019, 26, 189–194. [Google Scholar]
- Asenso-Okyere, W.K.; Dzator, J.A.; Osel-akoto, I. The behaviour towards malaria care—A multinomial logit approach. Soc. Indic. Res. 1996, 39, 167–186. [Google Scholar] [CrossRef]
- Tabuti, J.R.; Dhillion, S.S.; Lye, K.A. Traditional medicine in Bulamogi county, Uganda: Its practitioners, users and viability. J. Ethnopharmacol. 2003, 85, 119–129. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Nature of Variables | Coding Format | Nature of Variables | Coding Format |
|---|---|---|---|
| First visit | Yes = 1, 0 otherwise | Facility visitation pattern | |
| Type of facilities | Visited other units (same facility) | Reference variable | |
| Hospital | Reference variable | Visited other facilities | Yes = 1, 0 otherwise |
| Health center | Yes = 1, 0 otherwise | Visited traditional healers | Yes = 1, 0 otherwise |
| Health posts | Yes = 1, 0 otherwise | Visited no other facilities | Yes = 1, 0 otherwise |
| Education of caregivers | Administrator | ||
| No formal education | Reference variable | Government | Reference variable |
| Primary | Yes = 1, 0 otherwise | NGO/private not-for-profit | Yes = 1, 0 otherwise |
| Post-primary/vocational | Yes = 1, 0 otherwise | Private for-profit | Yes = 1, 0 otherwise |
| Secondary | Yes = 1, 0 otherwise | Sector of location | |
| Higher | Yes = 1, 0 otherwise | Rural | Reference variable |
| University | Yes = 1, 0 otherwise | Urban | Yes = 1, 0 otherwise |
| Regions | Dangerous symptoms | ||
| Dakar | Reference variable | Unable to drink/breastfeed | Reference variable |
| Diourbel | Yes = 1, 0 otherwise | Vomited everything | Yes = 1, 0 otherwise |
| Fatick | Yes = 1, 0 otherwise | Had convulsions | Yes = 1, 0 otherwise |
| Kaffrine | Yes = 1, 0 otherwise | Showed none of these | Yes = 1, 0 otherwise |
| Kaokack | Yes = 1, 0 otherwise | Treatment outcome | |
| Kedougou | Yes = 1, 0 otherwise | Sent home | Reference variable |
| Kolda | Yes = 1, 0 otherwise | Referred to other units | Yes = 1, 0 otherwise |
| Louga | Yes = 1, 0 otherwise | Admitted to same facility | Yes = 1, 0 otherwise |
| Matam | Yes = 1, 0 otherwise | Sent to laboratory | Yes = 1, 0 otherwise |
| Saint Louis | Yes = 1, 0 otherwise | Referred to other facility | Yes = 1, 0 otherwise |
| Sediou | Yes = 1, 0 otherwise | Instrumental variables | |
| Tambacounda | Yes = 1, 0 otherwise | Child dehydrated | Yes = 1, 0 otherwise |
| Thies | Yes = 1, 0 otherwise | Age of respondents | Years |
| Ziguinchor | Yes = 1, 0 otherwise |
| Healthcare Facilities’ Type | Management Structure | Location | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | Hospital | Health Center | Health Post | Government | Private/NGO | Private for-Profit | Urban | Rural | % of Total |
| Dakar | 26.71 | 32.88 | 40.41 | 88.36 | 7.53 | 4.11 | 100.00 | 0.00 | 40.35 |
| Diourbel | 6.85 | 13.70 | 79.45 | 87.67 | 10.96 | 1.37 | 100.00 | 0.00 | 6.91 |
| Fatick | 8.06 | 12.90 | 79.03 | 83.87 | 16.13 | 0.00 | 100.00 | 0.00 | 7.37 |
| Kaffrine | 14.29 | 14.29 | 71.43 | 80.00 | 20.00 | 0.00 | 100.00 | 0.00 | 3.14 |
| Kaokack | 0.00 | 17.14 | 82.86 | 85.71 | 14.29 | 0.00 | 100.00 | 0.00 | 6.44 |
| Kedougou | 0.00 | 14.29 | 85.71 | 85.71 | 14.29 | 0.00 | 100.00 | 0.00 | 0.23 |
| Kolda | 0.00 | 22.58 | 77.42 | 90.32 | 6.45 | 3.23 | 100.00 | 0.00 | 2.55 |
| Louga | 13.79 | 55.17 | 31.03 | 100.00 | 0.00 | 0.00 | 65.52 | 34.48 | 2.58 |
| Matam | 13.89 | 27.78 | 58.33 | 100.00 | 0.00 | 0.00 | 100.00 | 0.00 | 2.76 |
| Saint Louis | 8.16 | 20.41 | 71.43 | 91.84 | 8.16 | 0.00 | 100.00 | 0.00 | 6.26 |
| Sediou | 5.45 | 18.18 | 76.36 | 81.82 | 9.09 | 9.09 | 100.00 | 0.00 | 3.02 |
| Tambacounda | 16.67 | 30.00 | 53.33 | 73.33 | 26.67 | 0.00 | 100.00 | 0.00 | 6.60 |
| Thies | 0.00 | 45.45 | 54.55 | 85.45 | 12.73 | 1.82 | 98.18 | 1.82 | 5.37 |
| Ziguinchor | 6.94 | 22.22 | 70.83 | 75.00 | 16.67 | 8.33 | 100.00 | 0.00 | 6.42 |
| Total | 11.19 | 25.31 | 63.50 | 86.01 | 11.19 | 2.80 | 98.46 | 1.54 | 100.00 |
| Hospitals | Health Centers | Health Posts | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Waiting Time (minutes) | Freq | % | Freq | % | Freq | % | Freq. | % of Total | Average Time (minutes) |
| 0 < 30 | 24 | 6.23 | 102 | 26.49 | 259 | 67.27 | 385 | 53.85 | 14.77 |
| 30 < 60 | 17 | 9.77 | 41 | 23.56 | 116 | 66.67 | 174 | 24.34 | 37.43 |
| 60 < 90 | 12 | 17.91 | 17 | 25.37 | 38 | 56.72 | 67 | 9.37 | 61.45 |
| 90 < 120 | 4 | 20.00 | 4 | 20.00 | 12 | 60.00 | 20 | 2.80 | 96.25 |
| 120 < 150 | 11 | 28.95 | 9 | 23.68 | 18 | 47.37 | 38 | 5.31 | 121.89 |
| ≥150 | 12 | 38.71 | 8 | 25.81 | 11 | 35.48 | 31 | 4.34 | 219.06 |
| Total | 80 | 11.19 | 181 | 25.31 | 454 | 63.50 | 715 | 100.00 | 41.49 |
| Variables | Odds Ratio | Robust Std. Error | z Statistics |
|---|---|---|---|
| Demographic characteristics | |||
| Primary education | 0.422726 ** | 0.1482863 | −2.45 |
| Post-primary/vocational education | 0.5661392 | 0.2451324 | −1.31 |
| Secondary education | 2.021041 | 0.9347564 | 1.52 |
| Higher education | 0.2376322 ** | 0.1626052 | −2.10 |
| University education | 0.6057401 | 0.5977742 | −0.51 |
| Urban facility | 1.013217 | 1.24154 | 0.01 |
| Age of respondent | 0.9819595 * | 0.0103427 | −1.73 |
| Provider gender (male) | 1.452582 | 0.4270995 | 1.27 |
| Region of residence | |||
| Diourbel | 0.2700261 * | 0.1980297 | −1.79 |
| Fatick | 0.1681637 ** | 0.1188563 | −2.52 |
| Kaffrine | 13.41412 ** | 15.86089 | 2.20 |
| Kaokack | 0.0724768 *** | 0.0508559 | −3.74 |
| Kedougou | 1 | - | - |
| Kolda | 0.5396489 | 0.5425202 | −0.61 |
| Louga | 0.4616539 | 0.4290366 | −0.83 |
| Matam | 0.1449631 ** | 0.1139752 | −2.46 |
| Saint Louis | 0.323617 * | 0.2183897 | −1.67 |
| Sediou | 0.1737755 ** | 0.1375151 | −2.21 |
| Tambacounda | 0.1373578 *** | 0.0944989 | −2.89 |
| Thies | 0.4315295 | 0.2695468 | −1.35 |
| Ziguinchor | 0.3087374 | 0.2293771 | −1.58 |
| Visitation to other facilities | |||
| Visited other healthcare facilities | 0.6165949 | 0.6140672 | −0.49 |
| Visited traditional healers | 0.9438993 | 0.7194382 | −0.08 |
| Visited no other healthcare facilities | 2.622721 *** | 0.9559713 | 2.65 |
| First visit to the facilities | 1.611194 | 0.6841424 | 1.12 |
| Type of facilities | |||
| Health center | 3.134816 ** | 1.533333 | 2.34 |
| Health post | 17.68214 *** | 9.579755 | 5.30 |
| Hospital management types | |||
| Private/NGO not-for-profit | 0.2304086 *** | 0.0914951 | −3.70 |
| Private for-profit | 0.3044427 | 0.2222639 | −1.63 |
| Symptoms showed by child | |||
| Child vomits everything | 6.782206 *** | 4.906293 | 2.65 |
| Child had convulsion | 0.2633315 | 0.390746 | −0.90 |
| Child showed none of the symptoms | 4.373339 ** | 2.757639 | 2.34 |
| Treatment outcome | |||
| Child admitted to same facility | 5.033159 * | 4.313638 | 1.89 |
| Child sent to laboratory | 7.466214 | 10.55678 | 1.42 |
| Child referred to other external facilities | 3.242801 | 3.042426 | 1.25 |
| Child dehydrated | 2.054019 ** | 0.6736485 | 2.19 |
| Child referred to another facility | 0.3874237 * | 0.2116256 | −1.74 |
| Satisfied with the services | 1.808603 | 1.524662 | 0.70 |
| Respiratory infections | 0.8333609 | 0.2478156 | −0.61 |
| Digestive infections | 0.6781831 | 0.2327125 | −1.13 |
| Malaria infection | 0.263787 | 0.2552897 | −1.38 |
| Fever infection | 0.7097675 | 0.2687985 | −0.91 |
| Constant | 0.0276054 ** | 0.0449064 | −2.21 |
| Diagnostic indicators | |||
| Number of observations | 715 | ||
| Wald chi-square | 116.19 *** |
| Coefficients | Std. Error | z Statistics | |
|---|---|---|---|
| Nearest health facility | 114.9086 ** | 55.72138 | 2.06 |
| First visit (yes = 1, 0 otherwise) | −14.83495 | 11.94657 | −1.24 |
| Visited other facilities | |||
| Visited other healthcare facilities | 28.54269 | 18.58913 | 1.54 |
| Visited traditional healers | −14.21753 | 13.61236 | −1.04 |
| Visited no one | −21.45428 * | 11.34546 | −1.89 |
| Education | |||
| Primary education | 2.095776 | 7.841755 | 0.27 |
| Post-primary/vocational education | 4.079921 | 12.87535 | 0.32 |
| Secondary education | −26.44592 ** | 11.41158 | −2.32 |
| Higher education | 3.099546 | 22.00376 | 0.14 |
| University education | 9.464092 | 27.16536 | 0.35 |
| Regions | |||
| Diourbel region | 19.83818 ** | 9.377548 | 2.12 |
| Fatick region | 8.988693 | 12.03806 | 0.75 |
| Kaffrine region | −20.79079 * | 11.13523 | −1.87 |
| Kaokack region | 71.87024 *** | 20.70972 | 3.47 |
| Kedougou region | 2.68276 | 14.21874 | 0.19 |
| Kolda region | −1.052777 | 9.775943 | −0.11 |
| Louga region | −13.60771 | 16.77396 | −0.81 |
| Matam region | 43.92891 *** | 15.31938 | 2.87 |
| Saint Louis region | 55.67918 *** | 13.59337 | 4.10 |
| Sediou region | 8.225394 | 13.42222 | 0.61 |
| Tambacounda region | 53.54017 * | 28.66531 | 1.87 |
| Thies region | 11.40361 | 8.401836 | 1.36 |
| Ziguinchor region | −5.805092 | 10.75012 | −0.54 |
| Facility Type | |||
| Health center | −57.96009 *** | 15.14235 | −3.83 |
| Health post | −84.69879 *** | 24.64849 | −3.44 |
| Hospital Management Types | |||
| Private/NGO not-for-profit | 40.77879 *** | 14.1054 | 2.89 |
| Private for-profit | 32.15476 ** | 12.60406 | 2.55 |
| Facility Location | |||
| Urban facility | 90.7066 *** | 21.56068 | 4.21 |
| Symptoms Shown By Child | |||
| Child vomits everything | −80.53546 ** | 34.60835 | −2.33 |
| Child had convulsion | 3.862035 | 44.06009 | 0.09 |
| Child showed none of the symptoms | −71.12222 ** | 32.56936 | −2.18 |
| Treatment Outcome | |||
| Child referred to other units within same facility | −38.93408 * | 21.92744 | −1.78 |
| Child admitted to same facility | −14.01998 | 19.0114 | −0.74 |
| Child sent to laboratory | −30.06189 | 33.99239 | −0.88 |
| Child referred to other facility | −2.995982 | 15.52097 | −0.19 |
| Constant | 100.974 *** | 37.6959 | 2.68 |
| Corr (e.x206nearest,e.x201waitingtime) | −0.7535634 | 0.1425344 | |
| sd (e.x201waitingtime) | 52.67709 | 14.57313 | |
| sd (e.x206nearest) | 0.3151537 | 0.0298647 | |
| Number of observations | 715 | ||
| Uncensored | 688 | ||
| Left-censored | 27 | ||
| Wald chi2(35) | 133.72 *** | ||
| Log pseudolikelihood | −3657.4276 | ||
| Wald test of exogeneity (corr = 0): chi2(1) | 8.85 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oyekale, A.S. Utilization of Proximate Healthcare Facilities and Children’s Wait Times in Senegal: An IV-Tobit Analysis. Int. J. Environ. Res. Public Health 2023, 20, 7016. https://doi.org/10.3390/ijerph20217016
Oyekale AS. Utilization of Proximate Healthcare Facilities and Children’s Wait Times in Senegal: An IV-Tobit Analysis. International Journal of Environmental Research and Public Health. 2023; 20(21):7016. https://doi.org/10.3390/ijerph20217016
Chicago/Turabian StyleOyekale, Abayomi Samuel. 2023. "Utilization of Proximate Healthcare Facilities and Children’s Wait Times in Senegal: An IV-Tobit Analysis" International Journal of Environmental Research and Public Health 20, no. 21: 7016. https://doi.org/10.3390/ijerph20217016