
Associations of Preterm Birth with Dental and Gastrointestinal Diseases: Machine Learning Analysis Using National Health Insurance Data

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Variables
2.2. Analysis
3. Results
4. Discussion
4.1. Summary
4.2. Contributions
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; Van Look, P.F. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Mangham, L.J.; Petrou, S.; Doyle, L.W.; Draper, E.S.; Marlow, N. The cost of preterm birth throughout childhood in England and Wales. Pediatrics 2009, 123, e312–e327. [Google Scholar] [CrossRef] [PubMed]
- Waitzman, N.J.; Jalali, A.; Grosse, S.D. Preterm birth lifetime costs in the united states in 2016: An update. Semin. Perinatol. 2021, 45, 151390. [Google Scholar] [CrossRef] [PubMed]
- Markopoulou, P.; Papanikolaou, E.; Analytis, A.; Zoumakis, E.; Siahanidou, T. Preterm birth as a risk factor for metabolic syndrome and cardiovascular disease in adult life: A systematic review and meta-analysis. J. Pediatr. 2019, 210, 69–80.e5. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.H.; Lee, S.A.; Yoon, S.W. Medical utilization and costs in preterm infants in the first 6 years of life after discharge from neonatal intensive care unit: A nationwide population-based study in korea. J. Korean Med. Sci. 2022, 37, e93. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [Green Version]
- Vergnes, J.N.; Sixou, M. Preterm low birth weight and maternal periodontal status: A meta-analysis. Am. J. Obstet. Gynecol. 2007, 196, 135.e1–135.e7. [Google Scholar] [CrossRef]
- Puertas, A.; Magan-Fernandez, A.; Blanc, V.; Revelles, L.; O’Valle, F.; Pozo, E.; León, R.; Mesa, F. Association of periodontitis with preterm birth and low birth weight: A comprehensive review. J. Matern. Fetal Neonatal Med. 2018, 31, 597–602. [Google Scholar] [CrossRef]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on prevalence of periodontitis in adults in the united states: Nhanes 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontology 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Takeshita, T.; Matsuo, K.; Furuta, M.; Shibata, Y.; Fukami, K.; Shimazaki, Y.; Akifusa, S.; Han, D.H.; Kim, H.D.; Yokoyama, T.; et al. Distinct composition of the oral indigenous microbiota in south Korean and Japanese adults. Sci. Rep. 2014, 4, 6990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinesh, E.; Masthan, K.; Kumar, M.S.; Jeyapriya, S.M.; Babu, A.; Thinakaran, M. A clinicopathologic study of oral changes in gastroesophageal reflux disease, gastritis, and ulcerative colitis. J. Contemp. Dent. Pract. 2016, 17, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Fill Malfertheiner, S.; Malfertheiner, M.V.; Mönkemüller, K.; Röhl, F.W.; Malfertheiner, P.; Costa, S.D. Gastroesophageal reflux disease and management in advanced pregnancy: A prospective survey. Digestion 2009, 79, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.E.; Rubenstein, J.H. Presentation and epidemiology of gastroesophageal reflux disease. Gastroenterology 2018, 154, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.K.; Tae, C.H.; Song, K.H.; Kang, S.J.; Park, J.K.; Gong, E.J.; Shin, J.E.; Lim, H.C.; Lee, S.K.; Jung, D.H.; et al. 2020 Seoul consensus on the diagnosis and management of gastroesophageal reflux disease. J. Neurogastroenterol. Motil. 2021, 27, 453–481. [Google Scholar] [CrossRef]
- Lee, K.S.; Song, I.S.; Kim, E.S.; Ahn, K.H. Determinants of spontaneous preterm labor and birth including gastroesophageal reflux disease and periodontitis. J. Korean Med. Sci. 2020, 35, e105. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.S.; Kim, E.S.; Kim, D.Y.; Song, I.S.; Ahn, K.H. Association of gastroesophageal reflux disease with preterm birth: Machine learning analysis. J. Korean Med. Sci. 2021, 36, e282. [Google Scholar] [CrossRef]
- Meis, P.J.; Michielutte, R.; Peters, T.J.; Wells, H.B.; Sands, R.E.; Coles, E.C.; Johns, K.A. Factors associated with preterm birth in cardiff, wales. Ii. Indicated and spontaneous preterm birth. Am. J. Obstet. Gynecol. 1995, 173, 597–602. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Fairley, L.; Leyland, A.H. Social class inequalities in perinatal outcomes: Scotland 1980–2000. J. Epidemiol. Community Health 2006, 60, 31–36. [Google Scholar] [CrossRef]
- Wang, Y.A.; Sullivan, E.A.; Black, D.; Dean, J.; Bryant, J.; Chapman, M. Preterm birth and low birth weight after assisted reproductive technology-related pregnancy in australia between 1996 and 2000. Fertil. Steril. 2005, 83, 1650–1658. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.X.; Norman, R.J.; Kristiansson, P. The effect of various infertility treatments on the risk of preterm birth. Hum. Reprod. 2002, 17, 945–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunkara, S.K.; Antonisamy, B.; Redla, A.C.; Kamath, M.S. Female causes of infertility are associated with higher risk of preterm birth and low birth weight: Analysis of 117 401 singleton live births following IVF. Hum. Reprod. 2021, 36, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Song, I.S.; Kim, E.S.; Kim, H.I.; Ahn, K.H. Association of preterm birth with medications: Machine learning analysis using national health insurance data. Arch. Gynecol. Obstet. 2022, 305, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Dole, N.; Savitz, D.A.; Hertz-Picciotto, I.; Siega-Riz, A.M.; McMahon, M.J.; Buekens, P. Maternal stress and preterm birth. Am. J. Epidemiol. 2003, 157, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Khanam, R.; Applegate, J.; Nisar, I.; Dutta, A.; Rahman, S.; Nizar, A.; Ali, S.M.; Chowdhury, N.H.; Begum, F.; Dhingra, U.; et al. Burden and risk factors for antenatal depression and its effect on preterm birth in south Asia: A population-based cohort study. PLoS ONE 2022, 17, e0263091. [Google Scholar] [CrossRef]
- Liu, C.; Cnattingius, S.; Bergstrom, M.; Ostberg, V.; Hjern, A. Prenatal parental depression and preterm birth: A national cohort study. BJOG 2016, 123, 1973–1982. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Lee, B.E.; Park, H.S.; Kang, J.G.; Kim, J.O.; Ha, E.H. Risk factors for preterm birth in Korea: A multicenter prospective study. Gynecol. Obstet. Investig. 2005, 60, 206–212. [Google Scholar] [CrossRef]
- Varner, M.W.; Esplin, M.S. Current understanding of genetic factors in preterm birth. BJOG 2005, 112 (Suppl. S1), 28–31. [Google Scholar] [CrossRef]
- Couceiro, J.; Matos, I.; Mendes, J.J.; Baptista, P.V.; Fernandes, A.R.; Quintas, A. Inflammatory factors, genetic variants, and predisposition for preterm birth. Clin. Genet. 2021, 100, 357–367. [Google Scholar] [CrossRef]
- Bengtson, M.B.; Solberg, I.C.; Aamodt, G.; Jahnsen, J.; Moum, B.; Vatn, M.H. Relationships between inflammatory bowel disease and perinatal factors: Both maternal and paternal disease are related to preterm birth of offspring. Inflamm. Bowel Dis. 2010, 16, 847–855. [Google Scholar] [CrossRef]
- Bröms, G.; Granath, F.; Stephansson, O.; Kieler, H. Preterm birth in women with inflammatory bowel disease—The association with disease activity and drug treatment. Scand. J. Gastroenterol. 2016, 51, 1462–1469. [Google Scholar] [CrossRef]
- Cornish, J.; Tan, E.; Teare, J.; Teoh, T.G.; Rai, R.; Clark, S.K.; Tekkis, P.P. A meta-analysis on the influence of inflammatory bowel disease on pregnancy. Gut 2007, 56, 830–837. [Google Scholar] [CrossRef] [Green Version]
- Nasef, N.A.; Ferguson, L.R. Inflammatory bowel disease and pregnancy: Overlapping pathways. Transl. Res. 2012, 160, 65–83. [Google Scholar] [CrossRef]

{kind=link}
| Accuracy | PTB 1 | PTB 2 | PTB 3 | PTB 4 |
|---|---|---|---|---|
| No Sampling | ||||
| Logistic Regression | 0.9827 | 0.9932 | 0.9781 | 0.9772 |
| Random Forest | 0.9818 | 0.9927 | 0.9767 | 0.9758 |
| Oversampling | ||||
| Logistic Regression | 0.5445 | 0.6025 | 0.5551 | 0.5582 |
| Random Forest | 0.8599 | 0.8403 | 0.8403 | 0.8403 |
| AUC | PTB 1 | PTB 2 | PTB 3 | PTB 4 |
| No Sampling | ||||
| Logistic Regression | 0.5000 | 0.5000 | 0.5000 | 0.5000 |
| Random Forest | 0.5022 | 0.5027 | 0.5023 | 0.5023 |
| Oversampling | ||||
| Logistic Regression | 0.8403 | 0.6019 | 0.5539 | 0.5572 |
| Random Forest | 0.8404 | 0.8404 | 0.8404 | 0.8404 |
| PTB1 | PTB2 | PTB3 | PTB4 | |||||
|---|---|---|---|---|---|---|---|---|
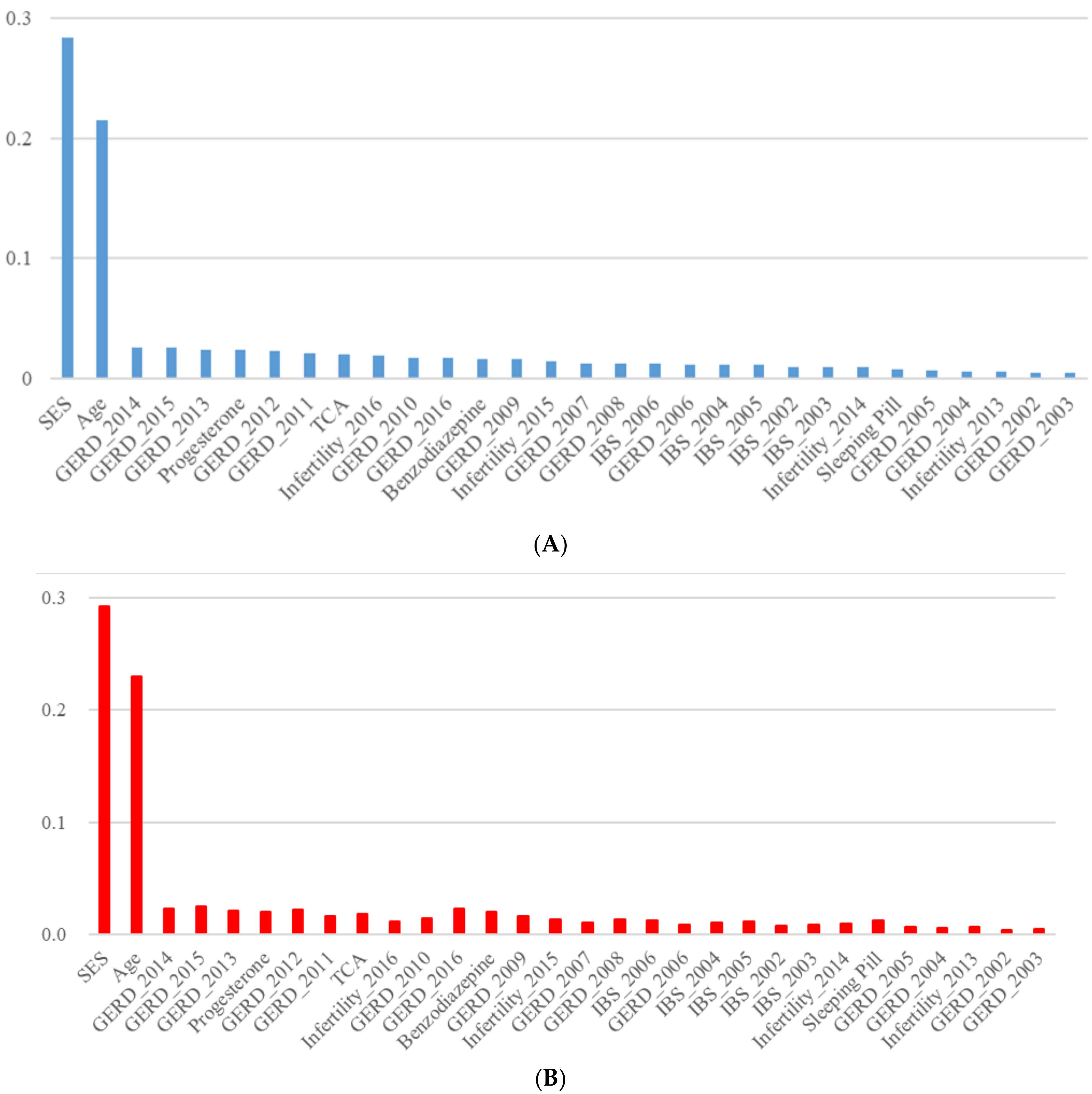
| 1 | SES | 0.284 | SES | 0.274 | SES | 0.281 | SES | 0.284 |
| 2 | Age | 0.227 | Age | 0.198 | Age | 0.218 | Age | 0.215 |
| 3 | GERD_2013 | 0.025 | Infertility_2016 | 0.038 | GERD_2014 | 0.025 | GERD_2014 | 0.026 |
| 4 | GERD_2015 | 0.025 | Benzodiazepine | 0.034 | GERD_2015 | 0.025 | GERD_2015 | 0.026 |
| 5 | GERD_2012 | 0.024 | GERD_2014 | 0.025 | Progesterone | 0.024 | GERD_2013 | 0.024 |
| 6 | Progesterone | 0.023 | GERD_2015 | 0.025 | GERD_2012 | 0.023 | Progesterone | 0.024 |
| 7 | TCA | 0.022 | GERD_2016 | 0.025 | GERD_2013 | 0.023 | GERD_2012 | 0.023 |
| 8 | GERD_2014 | 0.021 | GERD_2013 | 0.024 | GERD_2010 | 0.020 | GERD_2011 | 0.021 |
| 9 | Benzodiazepine | 0.020 | GERD_2012 | 0.022 | Benzodiazepine | 0.019 | TCA | 0.020 |
| 10 | GERD_2011 | 0.017 | GERD_2011 | 0.021 | GERD_2016 | 0.019 | Infertility_2016 | 0.019 |
| 11 | GERD_2016 | 0.016 | INFE_2015 | 0.021 | GERD_2011 | 0.018 | GERD_2010 | 0.017 |
| 12 | Infertility_2015 | 0.015 | GERD_2010 | 0.020 | Infertility_2016 | 0.018 | GERD_2016 | 0.017 |
| 13 | GERD_2008 | 0.014 | Progesterone | 0.019 | TCA | 0.018 | Benzodiazepine | 0.016 |
| 14 | GERD_2009 | 0.014 | TCA | 0.019 | GERD_2009 | 0.016 | GERD_2009 | 0.016 |
| 15 | GERD_2010 | 0.014 | GERD_2008 | 0.013 | Infertility_2015 | 0.013 | Infertility_2015 | 0.014 |
| 16 | IBS_2006 | 0.013 | GERD_2007 | 0.012 | GERD_2007 | 0.012 | GERD_2007 | 0.012 |
| 17 | GERD_2007 | 0.012 | GERD_2009 | 0.012 | IBS_2005 | 0.012 | GERD_2008 | 0.012 |
| 18 | IBS_2005 | 0.012 | IBS_2005 | 0.012 | GERD_2008 | 0.011 | IBS_2006 | 0.012 |
| 19 | Infertility_2016 | 0.012 | IBS_2006 | 0.012 | IBS_2002 | 0.010 | GERD_2006 | 0.011 |
| 20 | GERD_2006 | 0.010 | Sleeping Pill | 0.012 | IBS_2003 | 0.010 | IBS_2004 | 0.011 |
| 21 | IBS_2004 | 0.010 | IBS_2004 | 0.011 | IBS_2004 | 0.010 | IBS_2005 | 0.011 |
| 22 | Infertility_2014 | 0.010 | Infertility_2014 | 0.011 | IBS_2006 | 0.010 | IBS_2002 | 0.009 |
| 23 | Sleeping Pill | 0.010 | IBS_2002 | 0.009 | Infertility_2014 | 0.010 | IBS_2003 | 0.009 |
| 24 | IBS_2002 | 0.009 | IBS_2003 | 0.009 | Sleeping Pill | 0.010 | Infertility_2014 | 0.009 |
| 25 | IBS_2003 | 0.009 | Infertility_2013 | 0.008 | GERD_2006 | 0.009 | Sleeping Pill | 0.008 |
| 26 | GERD_2005 | 0.007 | GERD_2006 | 0.007 | GERD_2005 | 0.007 | GERD_2005 | 0.007 |
| 27 | GERD_2004 | 0.006 | GERD_2004 | 0.006 | GERD_2004 | 0.006 | GERD_2004 | 0.006 |
| 28 | Infertility_2013 | 0.006 | GERD_2005 | 0.006 | Infertility_2013 | 0.006 | Infertility_2013 | 0.006 |
| 29 | GERD_2002 | 0.005 | Infertility_2012 | 0.005 | GERD_2002 | 0.005 | GERD_2002 | 0.005 |
| 30 | GERD_2003 | 0.005 | GERD_2002 | 0.004 | GERD_2003 | 0.005 | GERD_2003 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, I.-S.; Choi, E.-S.; Kim, E.S.; Hwang, Y.; Lee, K.-S.; Ahn, K.H. Associations of Preterm Birth with Dental and Gastrointestinal Diseases: Machine Learning Analysis Using National Health Insurance Data. Int. J. Environ. Res. Public Health 2023, 20, 1732. https://doi.org/10.3390/ijerph20031732
Song I-S, Choi E-S, Kim ES, Hwang Y, Lee K-S, Ahn KH. Associations of Preterm Birth with Dental and Gastrointestinal Diseases: Machine Learning Analysis Using National Health Insurance Data. International Journal of Environmental Research and Public Health. 2023; 20(3):1732. https://doi.org/10.3390/ijerph20031732
Chicago/Turabian StyleSong, In-Seok, Eun-Saem Choi, Eun Sun Kim, Yujin Hwang, Kwang-Sig Lee, and Ki Hoon Ahn. 2023. "Associations of Preterm Birth with Dental and Gastrointestinal Diseases: Machine Learning Analysis Using National Health Insurance Data" International Journal of Environmental Research and Public Health 20, no. 3: 1732. https://doi.org/10.3390/ijerph20031732