
Self-Assessed Threshold Temperature for Cold among Poultry Industry Workers in Thailand

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Interview
2.3. Measurements
2.4. Data Analysis
3. Results
3.1. Characteristics of the Subjects and Variations between Subgroups
3.1.1. Personal Characteristics
3.1.2. Work-Related Factors
3.1.3. Workplace Physical Conditions
3.2. Self-Assessed Cold Threshold
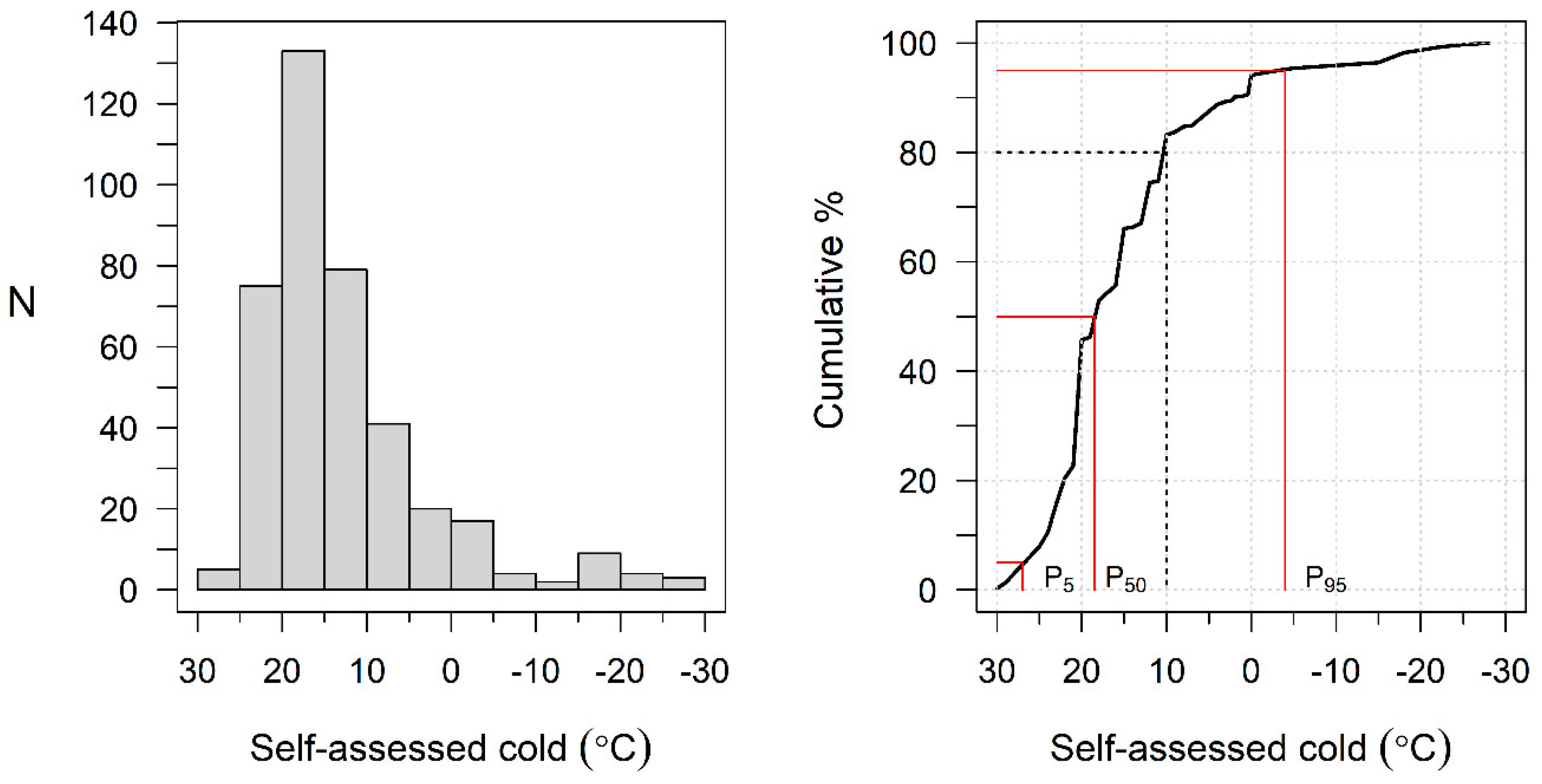
3.2.1. Distribution of CT
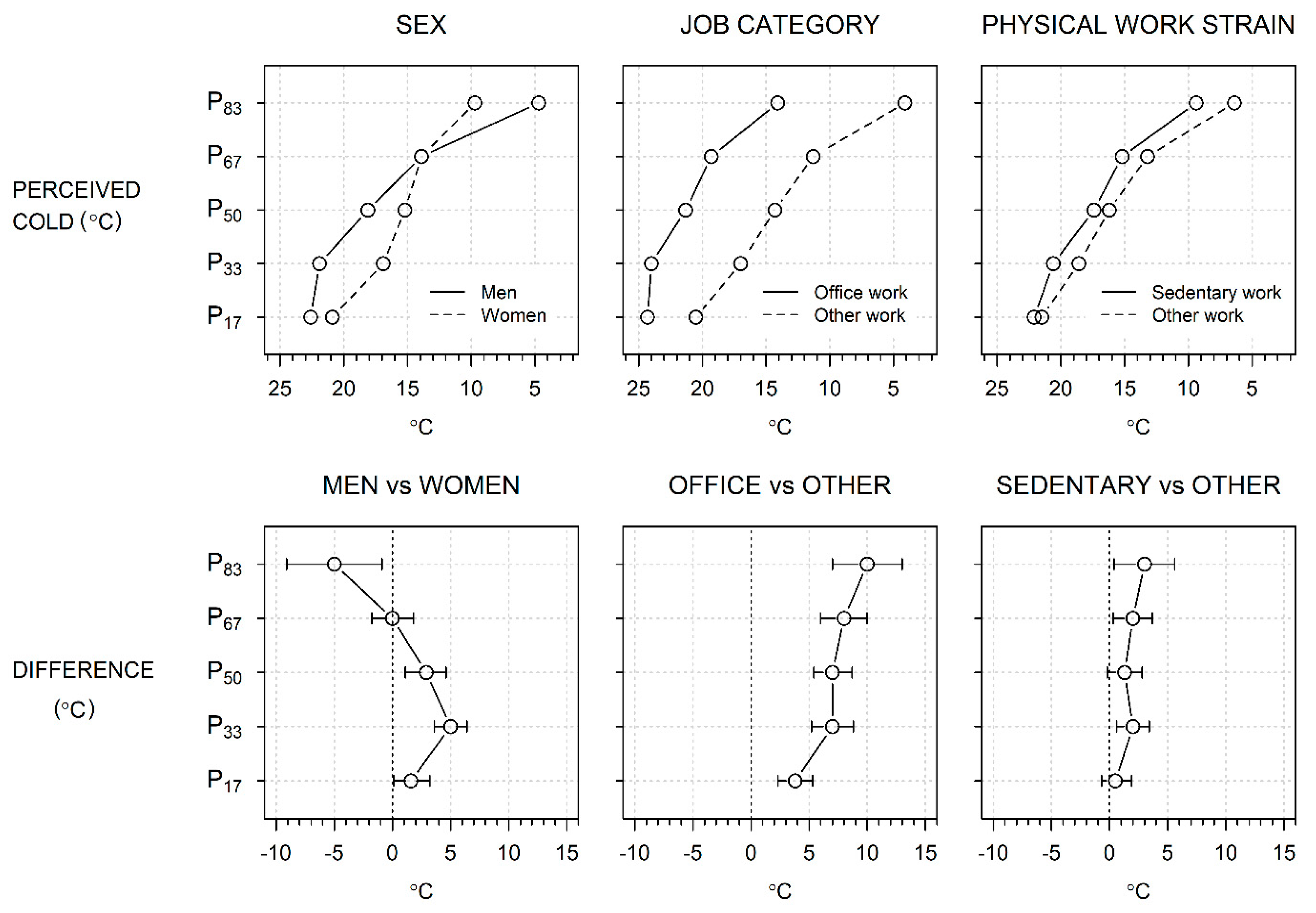
3.2.2. Subgroup Differences of the Mean CT
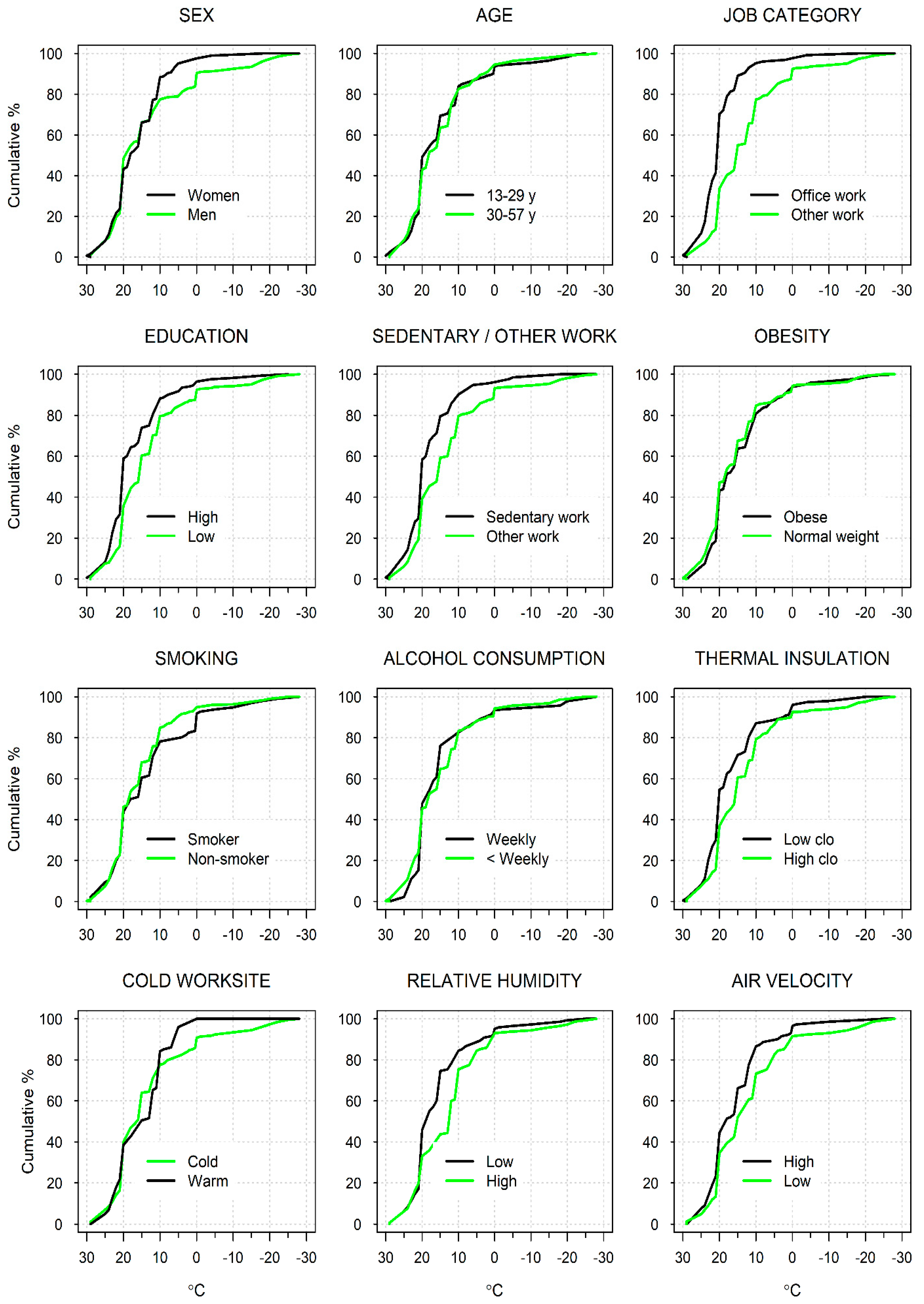
3.2.3. Cumulative Distributions of CI by Subgroups
3.3. Regression of Self-Assessed Threshold for Cold
3.4. Self-Assessed Cold Threshold in Relation to Worksite Physical Conditions
4. Discussion
4.1. Summary of Findings
4.2. Self-Assessed Threshold for Cold Temperature
4.3. Vulnerable Groups
4.4. Other Factors Affecting CT
4.5. Strengths and Limitations
4.6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Thermo-hygrometer (air temperature and relative humidity) | 303 C thermo-hygrometer (Shenzhen Graigar Technology, China) | Thermometer measure range: indoor −50 °C to +70 °C and outdoor −50 °C to +70 °C Resolution: 0.1 °C Accuracy: ±1.0 °C Temperature measuring period: 10 s Humidity range: 10%RH~99%RH Resolution: 1% Accuracy: ±3% RH (50%RH~80%RH): ±5% RH (10%RH~50%RH, 80%RH~99%RH): Humidity measuring period: 10 s |
| Air Velocity meter | VelociCalc® 9545-A (TSI Incorporated, MN, USA) | Accurate air velocity measurement 0 to 6000 ft/min (0 to 30 m/s) range Range: 0 to 6000 ft/min (0 to 30 m/s) Accuracy 1 & 2: ±3% of reading or ±3 ft/min (±0.015 m/s), whichever is greater Resolution: 1 ft/min (0.01 m/s) Temperature from Velocity Probe: Range: 14 to 140 °F (−10 to 60 °C) Accuracy 3: ±0.5 °F (±0.3 °C) Resolution: 0.1 °F (0.1 °C) Response Time: Velocity: 200 msec-Temperature: 2 min (to 66% of final value) |
| Mean (SD) (°C) | Difference (°C) | Median (°C) | Range (°C) | N (%) | |
|---|---|---|---|---|---|
| Sex | |||||
| Women | 14.1 (6.9) | 1.1 (−0.9, 3.1) | 15.0 | −18, 25 | 120 (42) |
| Men | 13.1 (12.1) | Ref. | 18.0 | −28, 29 | 164 (58) |
| Age | |||||
| 30–57 yr | 14.7 (9.8) | 0.7 (-1.3, 2.7) | 18.0 | −25, 30 | 131 (46) |
| 18–29 yr | 14.6 (10.4) | Ref. | 18.0 | −28, 29 | 153 (54) |
| Job category | |||||
| Office worker | 21.3 (2.4) | 8.7 (5.6, 11.9) | 21.0 | 12, 25 | 29 (10) |
| Other | 12.6 (10.3) | Ref. | 15.0 | −28, 29 | 255 (90) |
| Educ | |||||
| High | 14.9 (9.7) | 1.9 (−0.3, 4.2) | 20.0 | −28, 29 | 76 (27) |
| Low | 13.0 (10.3) | Ref. | 15.0 | −25, 25 | 208 (73) |
| Sedentary work | |||||
| Sedentary | 16.5 (7.2) | 4.0 (1.2, 6.7) | 20.0 | −18, 25 | 67 (23.6) |
| Other | 12.5 (10.8) | 15.0 | −28, 29 | 217 (76.4) | |
| Thermal insulation of clothing | |||||
| Low (clo below median, 1.26) | 12.7 (10.8) | −1.6 (−3.5, 0.4) | 15.0 | −28, 25 | 143 (50) |
| High (clo at least median, 1.26) | 14.3 (9.4) | Ref. | 16.0 | −25, 29 | 141 (50) |
| Obesity | |||||
| Obese (BMI ≥ 25.0 kg/m2) | 13.2 (9.7) | −0.5 (−2.6, 1.6) | 15.0 | −25, 29 | 104 (37) |
| Normal (BMI < 25.0 kg/m2) | 13.7 (10.5) | Ref. | 15.0 | −28, 25 | 180 (63) |
| Leisure-time physical exercise | |||||
| At least 1×/week | 12.1 (11.9) | −2.5 (−4.9, −0.1) | 15.0 | −28, 29 | 121 (43) |
| Never | 14.5 (8.5) | Ref. | 16.0 | −18, 29 | 163 (57) |
| Smoking | |||||
| Smoker | 13.1 (11.5) | −0.6 (−3.1, 1.9) | 16.0 | −28, 29 | 93 (32.7) |
| Non-smoker | 13.7 (9.5) | Ref. | 15.0 | −25, 25 | 191 (67) |
| Alcohol consumotion | |||||
| Weekly | 13.8 (11.6) | 0.3 (−3.0, 3.6) | 18.0 | −28, 25 | 44 (16) |
| Less often | 13.4 (9.9) | Ref. | 15.0 | −25, 29 | 240 (84) |
| Air temperature at workplace | |||||
| Warm (Ta ≥ 10 °C) | 14.7 (6.6) | 1.8 (−0.2, 3.9) | 15.0 | 0, 25 | 101 (36) |
| Cold (Ta < 10 °C) | 12.8 (11.6) | Ref. | 16.0 | −28, 29 | 183 (64) |
| Relative humidity at workplace | |||||
| Dry (RH below median, <41%) | 15.2 (9.1) | 3.4 (1.4, 5.3) | 18.0 | −25, 29 | 142 (50) |
| Wet (RH median or higher, ≥41%) | 11.8 (10.9) | Ref. | 12.0 | −28, 29 | 142 (50) |
| Air velocity at workplace | |||||
| High (AV above median, >0.38 m/s) | 15.3 (8.3) | 3.6 (1.6, 5.5) | 18.0 | −25, 25 | 142 (50) |
| Low (AV median or lower, ≤0.38 m/s) | 11.9 (11.5) | Ref. | 15.0 | −28, 29 | 142 (50) |
| All | 13.5 (10.2) | 15.0 | −28, 29 | 284 |
| Percentile | b (95% CI) (°C) | |
|---|---|---|
| Temperature (warm ([Ta ≥ 10 °C] vs. cold [Ta < 10 °C]) | ||
| Ordinary linear regression | 1.8 (−0.2, 3.9) | |
| Quantile regression | P83 | 7.0 (2.0, 12.0) |
| P67 | −2.0 (−4.9, 0.9) | |
| P50 | −1.0 (−4.6, 2.6) | |
| P33 | 0.0 (−1.8, 1.8) | |
| P17 | 2.0 (0.2, 3.8) | |
| Relative humidity (dry [RH < 41%] vs. wet [RH ≥ 41%]) | ||
| Ordinary linear regression | 3.4 (1.4, 5.3) | |
| Quantile regression | P83 | 5.0 (−2.0, 10.0) |
| P67 | 5.0 (0.0, 10.0) | |
| P50 | 6.0 (4.0, 8.0) | |
| P33 | 2.0 (0.0, 5.0) | |
| P17 | 0.0 (−2.0, 2.0) | |
| Air velocity (high [AV > 0.38 m/s] vs. low [AV ≤ 0.38 m/s]) | ||
| Ordinary linear regression | 3.6 (1.6, 5.5) | |
| Quantile regression | P83 | 6.0 (0.0, 10.0) |
| P67 | 3.0 (−3.0, 5.0) | |
| P50 | 3.0 (−0.4, 6.4) | |
| P33 | 0.0 (−2.0, 2.0) | |
| P17 | 2.0 (0.0, 3.0) | |
References
- Auttanate, N.; Chotiphan, C.; Maruo, S.J.; Näyhä, S.; Jussila, K.; Rissanen, S.; Sripaiboonkij, P.; Ikäheimo, T.M.; Jaakkola, J.J.K.; Phanprasit, W. Cold-related symptoms and performance degradation among Thai poultry industry workers, with reference to vulnerable groups; a cross-sectional study. BMC Public Health 2020, 20, 1357. [Google Scholar] [CrossRef]
- Phanprasit, W.; Chotiphan, C.; Auttanate, N.; Maruo, S.J.; Jussila, K.; Rissanen, S.; Sripaiboonkij, P.; Ikäheimo, T.M.; Jaakkola, J.J.K.; Näyhä, S. Cold-related pain in the face, upper limbs, and lower body among Thai chicken industry workers: A cross-sectional study. Int. Arch. Occup. Environ. Health 2021, 94, 799–812. [Google Scholar] [CrossRef]
- Phanprasit, W.; Konthonbut, P.; Laohaudomchok, W.; Tangtong, C.; Ikäheimo, T.M.; Jaakkola, J.J.; Näyhä, S. Workplace cold and perceived work ability: Paradoxically greater disadvantage for more versus less educated poultry industry in Thailand. Front. Public Health 2021, 9, 762533. [Google Scholar] [CrossRef] [PubMed]
- Thetkathuek, A.; Meepradit, P.; Jaidee, W. Factors affecting the musculoskeletal disorders of workers in the frozen food manufacturing factories in Thailand. Int. J. Occup. Saf. Ergon. 2016, 22, 49–56. [Google Scholar] [CrossRef]
- Thetkathuek, A.; Yingratanasuk, T.; Jaidee, W.; Ekburanawat, W. Cold exposure and health effects among frozen food processing workers in eastern Thailand. Saf. Health Work 2015, 6, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, B.E.; Aasmoe, L.; Aardal, L.; Andorsen, G.S.; Bjørnbakk, A.K.; Egeness, C.; Espejord, I.; Kramvik, E. Feeling cold at work increases the risk of symptoms from muscles, skin, and airways in seafood industry workers. Am. J. Ind. Med. 2005, 47, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Ghani, N.; Tariq, F.; Javed, H.; Nisar, N.; Tahir, A. Low-temperature health hazards among workers of cold storage facilities in Lahore, Pakistan. Medyna Pr. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Inaba, R.; Okumura, M.; Mirbod, S.M. Subjective symptoms of female workers sorting goods in summer. Ind. Health 2011, 49, 464–474. [Google Scholar] [CrossRef] [Green Version]
- Jevons, R.; Carmichael, C.; Crossley, A.; Bone, A. Minimum indoor temperature threshold recommendations for English homes in winter—A systematic review. Public Health 2016, 136, 4–12. [Google Scholar] [CrossRef]
- Shiue, I.; Shiue, M. Indoor temperature below 18 °C accounts for 9% population attributable risk for high blood pressure in Scotland. Int. J. Cardiol. 2014, 171, e1–e2. [Google Scholar] [CrossRef]
- Sormunen, E.; Remes, J.; Hassi, J.; Pienimäki, T.; Rintamäki, H. Factors associated with self-estimated work ability and musculoskeletal symptoms among male and female workers in cooled food-processing facilities. Ind. Health 2009, 47, 271–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikäheimo, T.M.; Jokelainen, J.; Näyhä, S.; Laatikainen, T.; Jousilahti, P.; Laukkanen, J.; Jaakkola, J.J.K. Cold weather-related cardiorespiratory symptoms predict higher morbidity and mortality. Environ. Res. 2020, 191, 110108. [Google Scholar] [CrossRef] [PubMed]
- McMichael, A.J.; Wilkinson, P.; Kovats, R.S.; Pattenden, S.; Hajat, S.; Armstrong, B.; Vajanapoom, N.; Niciu, E.M.; Mahomed, H.; Gingkoes, C.; et al. International study of temperature, heat and urban mortality: The ’ISOTHURM’ project. Int. J. Epidemiol. 2008, 37, 1121–1131. [Google Scholar] [CrossRef] [Green Version]
- Chotiphan, C.; Auttanate, N.; Maruo, S.J.; Näyhä, S.; Jussila, K.; Rissanen, S.; Sripaiboonkij, P.; Ikäheimo, T.M.; Jaakkola, J.J.K.; Phanprasit, W. Prevalence of cold-related symptoms among Thai chicken industry workers: Association with workplace temperature and thermal insulation of clothing. Ind. Health 2020, 585, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Department of Trade Negotiations. Summary Report on the Production and Export of Chicken Meat and Products 2020. Ministry of Commerce: Thailand, 2021, [In Thai]. Available online: https://api.dtn.go.th/files/v3/60f91710ef4140b37906fdfc/download (accessed on 15 December 2022).
- USDA. Poultry Expected to Continue Leading Global Meat Imports as Demand Rises. Available online: https://www.ers.usda.gov/amber-waves/2022/august/poultry-expected-to-continue-leading-global-meat-imports-as-demand-rises/ (accessed on 14 December 2022).
- Department of Foreign Trade. Foreign Trade Statistics and Information—Chicken Meat and Products. Ministry of Commerce, Thailand, 2022, [In Thai]. Available online: https://www.dft.go.th/th-th/dft-service-data-statistic (accessed on 15 December 2022).
- Centre for Agricultural Information Office of Agricultural Economics. Thailand Foreign Agricultural Trade Statistics 2021; Ministry of Agriculture and Co-operatives: Bangkok, Thailand, 2022.
- Ministry of Labour. Labour Statistics Yearbook 2021; Ministry of Labour: Bangkok, Thailand, 2022; ISBN 978-616-555-221-9.
- Pienimäki, T.; Karppinen, J.; Rintamäki, H.; Borodulin, K.; Laatikainen, T.; Jousilahti, P.; Hassi, J.; Näyhä, S. Prevalence of cold-related musculoskeletal pain according to self-reported threshold temperature among the Finnish adult population. Eur. J. Pain 2014, 18, 288–298. [Google Scholar] [CrossRef]
- ISO 9920; Ergonomics of the Thermal Environment. Estimation of Thermal Insulation and Water Vapour Resistance of a Clothing enSemble. International Organization for Standardization: Geneva, Switzerland, 2007.
- Koenker, R.; Hallock, K.F. Quantile regression. J. Econ. Perspect. 2001, 15, 143–156. [Google Scholar] [CrossRef]
- Koenker, R.; D’Orey, V. Computing regression quantiles. J. Royal Stat. Soc. 1987, 36, 383–393. [Google Scholar]
- Bieler, G.S.; Brown, G.G.; Williams, R.L.; Brogan, D.J. Estimating model-adjusted risks, risk differences, and risk ratios from complex survey data. Am. J. Epidemiol. 2010, 171, 618–623. [Google Scholar] [CrossRef]
- Graubard, B.I.; Korn, E.L. Predictive margins with survey data. Biometrics 1999, 55, 652–656. [Google Scholar] [CrossRef]
- ISO 15743; Ergonomics of the Thermal Environment. Cold Workplaces. Risk Assessments and Management. Finnish Standards Association: Geneva, Switzerland, 2008.
- Shoemaker, J.A.; Refinetti, R. Day-night difference in the preferred ambient temperature of human subjects. Physiol. Behav. 1996, 59, 1001–1003. [Google Scholar] [CrossRef]
- Karyono, T.H. Report on thermal comfort and building energy studies in Jakarta—Indonesia. Build. Environ. 2000, 35, 77–90. [Google Scholar] [CrossRef]
- Mäkinen, T.M.; Hassi, J. Health problems in cold work. Ind. Health 2009, 47, 207–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, T.P.; Matzarakis, A. Tourism climate and thermal comfort in Sun Moon Lake, Taiwan. Int. J. Biometeorol. 2008, 52, 281–290. [Google Scholar] [CrossRef]
- Chen, X.; Gao, L.; Xue, P.; Du, J.; Liu, J. Investigation of outdoor thermal sensation and comfort evaluation methods in severe cold area. Sci. Tot. Environ. 2020, 749, 141520. [Google Scholar] [CrossRef] [PubMed]
- Sepehri, S.; Aliabadi, M.; Golmohammadi, R.; Babamiri, M. Human cognitive functions and psycho-physiological responses under low thermal conditions in a simulated office environment. Work 2021, 69, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Pochter, O.; Cohen, P.; Lin, T.P.; Matzarakis, A. Outdoor human thermal perception in various climates: A comprehensive review of approaches, methods and quantification. Sci. Tot. Environ. 2018, 631–632, 390–406. [Google Scholar]
- Sato, M.; Katsuura, T.; Yasukouchi, A. The lower and upper critical temperatures in male Japanese. J. Hum. Ergol. 1979, 8, 145–153. [Google Scholar]
- Sato, M.; Watanuki, S.; Iwanaga, K.; Shinozaki, F. The influence of clothing ensembles on the lower critical temperature. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Yamtraipat, N.; Khedari, J.; Hirunlabh, J. Thermal comfort standards for air conditioned buildings in hot and humid Thailand considering additional factors of acclimatization and education level. Sol. Energy 2005, 78, 504–517. [Google Scholar] [CrossRef]
- Neild, P.J.; Syndercombe-Court, D.; Keatinge, W.R.; Donaldson, G.C.; Mattock, M.; Caunce, M. Cold-induced increases in erythrocyte count, plasma cholesterol and plasma fibrinogen of elderly people without a comparable rise in protein C or factor X. Clin. Sci. 1994, 86, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Reste, J.; Zvagule, T.; Kurjane, N.; Martinsone, Z.; Martinsone, I.; Seile, A.; Vanadzins, I. Wrist hypothermia related to continuous work with a computer mouse: A digital infrared imaging pilot study. Int. J. Environ. Res. Public. Health 2015, 12, 9265–9281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekhar, S.C. Thermal comfort in air-conditioned buildings in hot and humid climates—Why we are not getting it right? Indoor Air 2016, 26, 138–152. [Google Scholar] [CrossRef] [PubMed]
- Wankhade, P. Different cultures of management and their relationships with organizational performance: Evidence from the UK ambulance service. Public Money Manag. 2012, 32, 381–388. [Google Scholar] [CrossRef]
- Becher, T.; Trowler, P.R. Academic Tribes and Territories. Intellectual Enquiry and the Cultures of Discipline; St. Edmundsbury Press: Bury St Edmunds, Suffolk, UK, 2001. [Google Scholar]
- Bell, C.R.; Watts, A.J. Thermal limits for industrial workers. Brit. J. Ind. Med. 1971, 28, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voelcker, T. Perception of cold hands: Comparison between women and men. Extrem. Physiol. Med. 2015, 4 (Suppl. S1), A80. [Google Scholar] [CrossRef] [Green Version]
- Karjalainen, S. Thermal comfort and gender: A literature review. Indoor Air 2012, 22, 96–109. [Google Scholar] [CrossRef]
- Lan, L.; Lian, Z.; Liu, W.; Liu, Y. Investigation of gender difference in thermal comfort for Chinese people. Eur. J. Appl. Physiol. 2008, 102, 471–480. [Google Scholar] [CrossRef]
- Hashiguchi, N.; Feng, Y.; Tochihara, Y. Gender differences in thermal comfort and mental performance at different vertical air temperatures. Eur. J. Appl. Physiol. 2010, 109, 41–48. [Google Scholar] [CrossRef]
- Barsky, A.J.; Peekna, H.M.; Borus, J.F. Somatic symptom reporting in women and men. J. Gen. Intern. Med. 2001, 16, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Bingefors, K.; Isacson, D. Epidemiology, co-morbidity, and impact on health-related quality of life of self-reported headache and musculoskeletal pain—A gender perspective. Eur. J. Pain 2004, 8, 435–450. [Google Scholar] [CrossRef]
- Blatteis, C.M. Age-dependent changes in temperature regulation—A mini review. Gerontology 2012, 58, 289–295. [Google Scholar] [CrossRef]
- Nahon, K.J.; Boon, M.R.; Doornink, F.; Jazet, I.M.; Rensen, P.C.N.; Abreu-Vieira, G. Lower critical temperature and cold-induced thermogenesis of lean and overweight humans are inversely related to body mass and basal metabolic rate. J. Therm. Biol. 2017, 69, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Crawshaw, L.I.; Saito, K.; Nakamura, M.; Nagashima, K.; Kanosue, K. Effects of alcohol on autonomic responses and thermal sensation during cold exposure in humans. Alcohol 2008, 42, 207–212. [Google Scholar] [CrossRef]
- Granberg, P.O. Alcohol and cold. Arct. Med. Res. 1991, 50 (Suppl. S6), 43–47. [Google Scholar]
- Penning, R.; McKinney, A.; Bus, L.D.; Olivier, B.; Slot, K.; Verster, J.C. Measurement of alcohol hangover severity: Development of the Alcohol Hangover Severity Scale (AHSS). Psychopharmacology 2013, 225, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Petschke, F.T.; Engelhardt, T.O.; Ulmer, H.; Piza-Katzer, H. Einfluss des Zigarettenrauchens auf die Hautdurchblutung der Hand. [Effect of cigarette smoking on skin perfusion of the hand, in German]. Chirurg 2006, 77, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Pistelli, F.; Pesce, M.; Aquilini, F.; Franzoni, F.; Santoro, G.; Carrozzi, L. Impact of long-term exposure to cigarette smoking on skin microvascular function. Microvasc. Res. 2014, 93, 46–51. [Google Scholar] [CrossRef]
- Castellani, J.W.; Young, A.J. Human physiological responses to cold exposure: Acute responses and acclimatization to prolonged exposure. Auton. Neurosci. 2016, 196, 63–74. [Google Scholar] [CrossRef] [Green Version]
- Cheung, S.S.; Lee, J.K.W.; Oksa, J. Thermal stress, human performance, and physical employment standards. Appl. Physiol. Nutr. Metab. 2016, 41, S148–S164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunwoo, Y.; Chou, C.; Takeshita, J.; Murakami, M.; Tochihara, Y. Physiological and subjective responses to low relative humidity. J. Physiol. Anthropol. 2006, 25, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Healthline. Why Do I Always Feel Cold, and Can I Treat It? Available online: https://web.archive.org/web/20201214065407/https://www.healthline.com/health/always-cold#causes (accessed on 15 January 2023).
- Gasparrini, A.; Guo, Y.; Sera, F.; Vicedo-Cabrera, A.M.; Huber, V.; Tong, S.; de Sousa Zanotti Stagliorio Coelho, M.; Nascimento Saldiva, P.H.; Lavigne, E.; Matus Correa, P.; et al. Projections of temperature-related excess mortality under climate change scenarios. Lancet Planet. Health 2017, 1, e360–e367. [Google Scholar] [CrossRef] [PubMed]
| Factor | Mean (SD) (°C) | Difference (°C) | Median (°C) | Range (°C) | N (%) |
|---|---|---|---|---|---|
| Sex | |||||
| Men | 13.2 (12.3) | −2.8 (−4.4, 1.1) | 18.0 | −18, 30 | 186 (47) |
| Women | 16.0 (7.3) | Ref. | 18.0 | −28, 29 | 206 (53) |
| Age | |||||
| 30–57 yr | 14.6 (9.8) | −0.1 (−1.8, 1.6) | 18.0 | −28, 29 | 219 (56) |
| 18–29 yr | 14.7 (10.4) | Ref. | 18.0 | −25, 30 | 173 (44) |
| Job category | |||||
| Office work | 19.3 (6.4) | 6.9 (5.2, 8.6) | 20.0 | −18, 30 | 128 (33) |
| Other work | 12.4 (10.7) | Ref. | 15.0 | −28, 29 | 264 (67) |
| Education | |||||
| High | 16.8 (8.5) | 3.8 (2.1, 5.4) | 20.0 | −25, 25 | 168 (43) |
| Low | 13.0 (10.8) | Ref. | 15.0 | −28, 29 | 224 (57) |
| Physical work strain | |||||
| Sedentary work | 17.5 (7.7) | 4.3 (2.3, 6.4) | 20.0 | −18, 30 | 132 (34) |
| Other work | 13.2 (10.8) | Ref. | 15.0 | −28, 29 | 260 (66) |
| Thermal insulation of clothing | |||||
| Low (clo below median, 1.15) | 16.2 (8.8) | 3.1 (1.2, 5.1) | 20.0 | −20, 30 | 194 (50) |
| High (clo at least median, 1.15) | 13.1 (10.9) | Ref. | 15.0 | −28, 29 | 198 (50) |
| Obesity | |||||
| Obese (BMI ≥ 25.0 kg/m2) | 14.1 (10.0) | −0.9 (−2.6, 0.9) | 18.0 | −28, 25 | 147 (38) |
| Normal (BMI < 25.0 kg/m2) | 15.0 (10.1) | Ref. | 18.0 | −25, 30 | 245 (62) |
| Leisure-time physical exercise | |||||
| At least 1×/week | 15.5 (8.5) | −1.8 (−3.8, 0.2) | 18.0 | −18, 30 | 182 (46) |
| Never | 13.7 (11.5) | Ref. | 18.0 | −28, 29 | 210 (54) |
| Smoking | |||||
| Smoker | 13.2 (11.4) | −1.8 (−3.8, 0.1) | 17.0 | −28, 29 | 96 (24) |
| Non-smoker | 15.1 (9.6) | Ref. | 18.0 | −25, 30 | 296 (76) |
| Alcohol consumption | |||||
| Weekly or more often | 14.1 (11.4) | −0.6 (−3.2, 2.0) | 18 | −28, 25 | 46 (12) |
| Less often | 14.7 (9.9) | Ref. | 18 | −25, 30 | 346 (88) |
| All | 14.6 (10.0) | 18.0 | −28, 30 | 392 |
| Characteristics | Percentile | Regression coefficient (95% CI) (°C) | ||
|---|---|---|---|---|
| All Participants (N = 392) | Subsample (N = 284) | |||
| Crude | Adjusted for Personal and Work-Related Factors 1 | Also Adjusted for Worksite Physical Conditions 2 | ||
| Sex (men vs. women) | ||||
| Ordinary linear regression | −2.8 (−4.4, −1.1) | −0.1 (−2.0, 1.8) | −0.4 (−2.9, 2.1) | |
| Quantile regression | P83 | −9.0 (−13.0, −5.0) | −5.0 (−9.1, −0.9) | −5.0 (−9.5, −0.5) |
| P67 | 0.0 (−1.8, 1.8) | 0.0 (−1.8, 1.8) | 0.0 (−2.2, 2.2) | |
| P50 | 0.0 (−2.7, 2.7) | 2.9 (1.1, 4.6) | 1.8 (−0.4, 4.1) | |
| P33 | 0.0 (−0.1, 0.1) | 5.0 (3.6, 6.4) | 1.5 (−0.7, 3.7) | |
| P17 | −1.0 (−2.5, 0.5) | 1.6 (0.1, 3.2) | 2.0 (−0.3, 4.3) | |
| Age (change/10 yrs) | ||||
| Ordinary linear regression | −0.1 (−1.8, 1.5) | −0.4 (−1.2, 0.5) | 0.5 (−0.4, 1.4) | |
| Quantile regression | P83 | −2.0 (−6.8, 2.8) | 0.0 (−1.3, 1.3) | 0.0 (−1.2, 1.2) |
| P67 | −3.0 (−5.6, −0.4) | 0.0 (−0.6, 0.6) | 0.0 (−0.8, 0.8) | |
| P50 | 0.0 (−2.7, 2.7) | −0.3 (−0.8, 0.2) | 0.3 (−0.3, 0.9) | |
| P33 | 0.0 (−0.1, 0.1) | 0.0 (−0.4, 0.4) | 0.0 (−0.5, 0.5) | |
| P17 | 1.0 (−0.5, 2.5) | 0.3 (−0.3, 0.9) | 0.5 (−0.5, 1.4) | |
| Job category (office work vs. other work) | ||||
| Ordinary linear regression | 6.9 (5.2, 8.6) | 6.8 (4.5, 9.1) | 10.5 (6.7, 14.2) | |
| Quantile regression | P83 | 10.0 (6.7, 13.3) | 10.0 (7.0, 13.0) | 15.0 (9.5, 20.6) |
| P67 | 10.0 (8.1, 11.9) | 8.0 (6.0, 10.0) | 10.0 (6.7, 13.3) | |
| P50 | 5.0 (4.0, 6.0) | 7.0 (5.4, 8.7) | 10.3 (8.3, 12.3) | |
| P33 | 2.0 (−0.0, 4.0) | 7.0 (5.2, 8.8) | 9.5 (7.7, 11.2) | |
| P17 | 4.0 (2.9, 5.1) | 3.8 (2.3, 5.3) | 7.2 (4.2, 10.1) | |
| Physical work strain (sedentary work vs. other work) | ||||
| Ordinary linear regression | 4.3 (2.6, 6.1) | 2.0 (0.1, 3.8) | 1.5 (−0.8, 3.8) | |
| Quantile regression | P83 | 7.0 (2.7, 11.3) | 3.0 (0.4, 5.6) | 0.0 (−3.0, 3.0) |
| P67 | 6.0 (3.6, 8.4) | 2.0 (0.3, 3.7) | 0.0 (−1.9, 1.9) | |
| P50 | 5.0 (3.5, 6.5) | 1.3 (−0.2, 2.8) | 0.6 (−1.2, 2.3) | |
| P33 | 0.0 (−1.1, 1.1) | 2.0 (0.6, 3.4) | 1.5 (−0.1, 3.1) | |
| P17 | 2.0 (0.4, 3.6) | 0.5 (−0.7, 1.9) | 2.0 (0.1, 3.8) | |
| Thermal insulation of clothing (clo ≤ 1.15 vs. clo > 1.15) | ||||
| Orinary linear regression | 3.1 (2.1, 5.4) | −0.9 (−2.8, 1.0) | −1.6 (−3.6, 0.4) | |
| Quantile regression | P83 | 4.0 (0.4, 7.6) | 0.0 (−3.1, 3.1) | −4.0 (−8.2, 0.1) |
| P67 | 3.0 (0.3, 5.7) | 0.0 (−1.8, 1.8) | 0.0 (−2.5, 2.5) | |
| P50 | 5.0 (3.5, 6.5) | −0.8 (−2.8, 1.2) | −1.0 (−2.7, 0.8) | |
| P33 | 0.0 (−1.4, 1.4) | −2.0 (−3.6, −0.4) | −1.5 (−3.1, 0.1) | |
| P17 | 3.0 (1.5, 4.5) | −0.2 (−1.6, 1.1) | −1.2 (−3.2. 0.9) | |
| Alcohol consumption (weekly vs. less often) | ||||
| Ordinary linear regression | −0.6 (−3.2, 2.0) | 1.7 (−0.9, 4.4) | −0.8 (−3.6, 1.9) | |
| Quantile regression | P83 | −5.0 (−13.0, 3.0) | 4.0 (−2.8, 10.8) | 1.0 (−6.1, 8.1) |
| P67 | 3.0 (−0.5, 6.5) | 5.0 (1.5, 8.5) | 0.0 (−3.3, 3.3) | |
| P50 | 0.0 (−2.8, 2.8) | 1.8 (−1.0, 4.6) | −0.8 (−3.0, 1.4) | |
| P33 | 0.0 (−0.5, 0.5) | 0.0 (−1.3, 1.3) | −1.5 (−3.2, 0.0) | |
| P17 | −2.0 (−4.0, 0.0) | −0.6 (−2.7, 1.5) | −1.0 (−3.0, 0.9) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laohaudomchok, W.; Phanprasit, W.; Konthonbut, P.; Tangtong, C.; Sripaiboonkij, P.; Ikäheimo, T.M.; Jaakkola, J.J.K.; Näyhä, S. Self-Assessed Threshold Temperature for Cold among Poultry Industry Workers in Thailand. Int. J. Environ. Res. Public Health 2023, 20, 2067. https://doi.org/10.3390/ijerph20032067
Laohaudomchok W, Phanprasit W, Konthonbut P, Tangtong C, Sripaiboonkij P, Ikäheimo TM, Jaakkola JJK, Näyhä S. Self-Assessed Threshold Temperature for Cold among Poultry Industry Workers in Thailand. International Journal of Environmental Research and Public Health. 2023; 20(3):2067. https://doi.org/10.3390/ijerph20032067
Chicago/Turabian StyleLaohaudomchok, Wisanti, Wantanee Phanprasit, Pajaree Konthonbut, Chaiyanun Tangtong, Penpatra Sripaiboonkij, Tiina M. Ikäheimo, Jouni J. K. Jaakkola, and Simo Näyhä. 2023. "Self-Assessed Threshold Temperature for Cold among Poultry Industry Workers in Thailand" International Journal of Environmental Research and Public Health 20, no. 3: 2067. https://doi.org/10.3390/ijerph20032067
APA StyleLaohaudomchok, W., Phanprasit, W., Konthonbut, P., Tangtong, C., Sripaiboonkij, P., Ikäheimo, T. M., Jaakkola, J. J. K., & Näyhä, S. (2023). Self-Assessed Threshold Temperature for Cold among Poultry Industry Workers in Thailand. International Journal of Environmental Research and Public Health, 20(3), 2067. https://doi.org/10.3390/ijerph20032067