

“We Just Don’t Know Where They Are”: The Geographical Distribution of Exercise Classes for Older People, Including Those Living with Dementia in the East Midlands


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Study Data
- Demographic data: Percentages of population over 65 years were gathered from the 2011 census data, which was available through the ArcGIS software [29].
- Socio-economic data: UK Index of Multiple Deprivation 2015 was gathered from data available through the ArcGIS software [30].
- Population density data: World Population Density Estimate 2016 was gathered from data available through the ArcGIS software [31].
- Location data: Postcode data for exercise classes were gathered through an internet search using Google.
2.3. Data Collection
2.4. Geocoding and Mapping
2.5. Spatial Analysis
3. Results
3.1. Location
3.2. Classes Compared to Population over 65 Years
3.3. Classes Compared to Levels of Deprivation
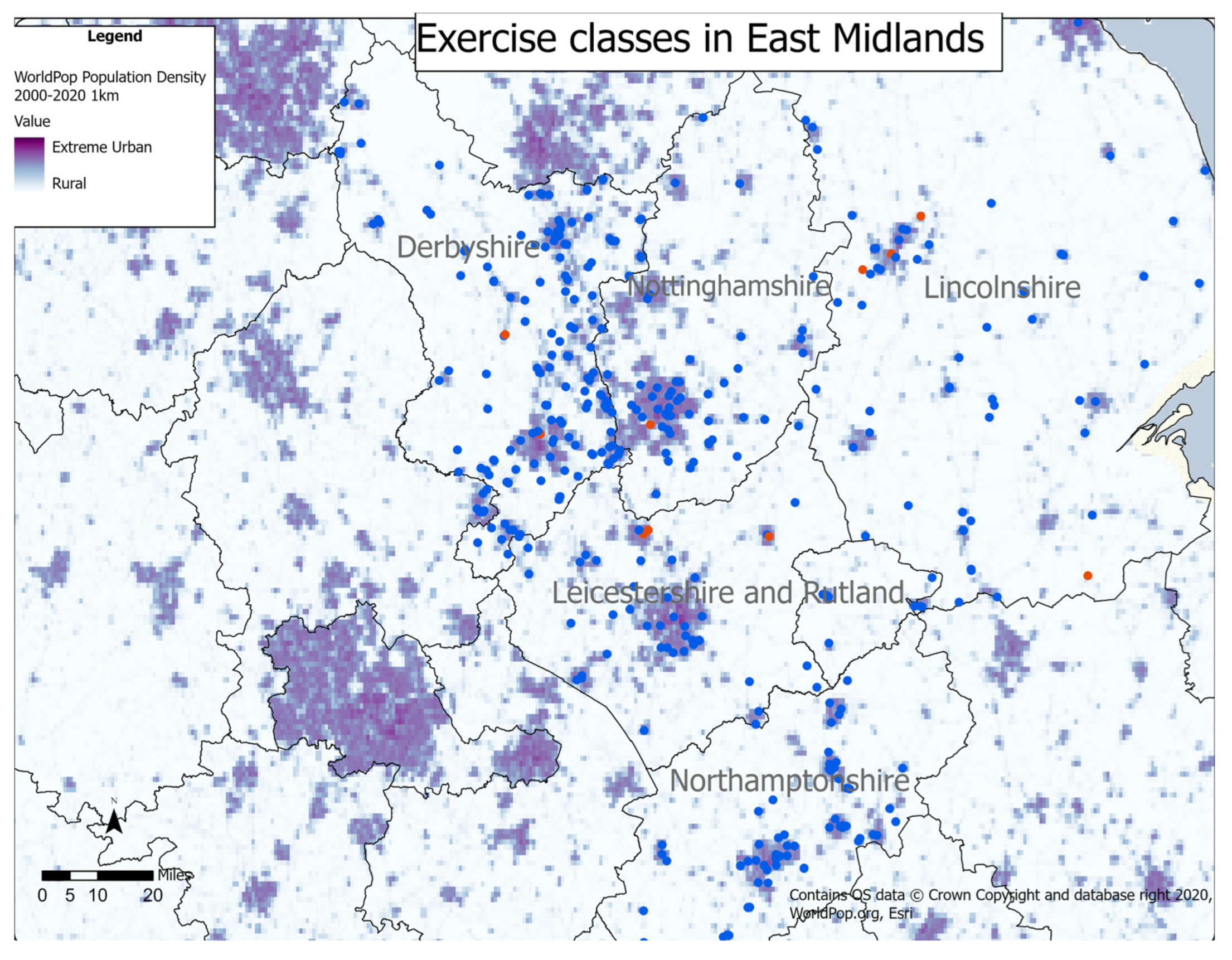
3.4. Classes Compared to Population Density
4. Discussion
4.1. Summary of Findings
4.2. Comparison with Other Studies
4.3. Strengths and Limitations
4.4. Further Research and Recommendations
4.4.1. Practice Recommendations
4.4.2. Research Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percentage Population 65+ | <15 | 15.1—17 | 17.1—20 | >20 | ||||
|---|---|---|---|---|---|---|---|---|
| County | Number | % | Number | % | Number | % | Number | % |
| Derbyshire | 0 | 0 | 47 | 24 | 109 | 54 | 45 | 22 |
| Leicestershire | 19 | 23 | 12 | 15 | 46 | 56 | 5 | 6 |
| Lincolnshire | 21 | 23 | 0 | 0 | 17 | 19 | 53 | 58 |
| Northamptonshire | 35 | 44 | 20 | 25 | 24 | 31 | 0 | 0 |
| Nottinghamshire | 12 | 18 | 0 | 0 | 55 | 82 | 0 | 0 |
| Socio-Economic Status | Low (0–1) | High (6—10) | ||
|---|---|---|---|---|
| County | Number | % | Number | % |
| Derbyshire | 91 | 45 | 107 | 55 |
| Leicestershire | 50 | 63 | 30 | 33 |
| Lincolnshire | 49 | 54 | 42 | 46 |
| Northamptonshire | 36 | 46 | 43 | 54 |
| Nottinghamshire | 26 | 39 | 41 | 61 |
| Level of Urbanisation | Settled | Light Urban | Urban | |||
|---|---|---|---|---|---|---|
| County | Number | % | Number | % | Number | % |
| Derbyshire | 11 | 6 | 59 | 32 | 115 | 62 |
| Leicestershire | 0 | 0 | 12 | 15 | 66 | 85 |
| Lincolnshire | 3 | 4 | 20 | 31 | 54 | 65 |
| Northamptonshire | 1 | 1 | 23 | 27 | 60 | 72 |
| Nottinghamshire | 7 | 10 | 27 | 39 | 35 | 51 |
References
- W.H.O. Global Action Plan on the Public Health Response to Dementia 2017–2025. World Health Organisation 2017. Available online: https://www.https://www.who.int/publications/i/item/global-action-plan-on-the-public-health-response-to-dementia-2017---2025 (accessed on 21 June 2022).
- N.I.C.E. Dementia: Assessment, Management and Support for People Living with Dementia and Their Carers; N.I.C.E.: London, UK, 2018. [Google Scholar]
- Palm, R.; Jünger, S.; Reuther, S.; Schwab, C.G.G.; Dichter, M.N.; Holle, B.; Halek, M. People with Dementia in Nursing Home Research: A Methodological Review of the Definition and Identification of the Study Population. BMC Geriatr. 2016, 16, 78. [Google Scholar] [CrossRef]
- Wittenberg, R.; Hu, B.; Barraza-Araiza, L.; Funder, A.R. CPEC Working Paper 5: Modelling Outcome and Cost Impacts of Interventions for Dementia (MODEM) Study; CPEC: London, UK, 2019. [Google Scholar]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise Programs for People with Dementia. Cochrane Database Syst. Rev. 2015, 2015, Cd006489. [Google Scholar] [CrossRef] [PubMed]
- Fox, B.; Hodgkinson, B.; Parker, D. The Effects of Physical Exercise on Functional Performance, Quality of Life, Cognitive Impairment and Physical Activity Levels for Older Adults Aged 65 Years and Older with a Diagnosis of Dementia: A Systematic Review. JBI Database System Rev. Implement. Rep. 2014, 12, 158–276. [Google Scholar] [CrossRef]
- Pitkälä, K.; Savikko, N.; Poysti, M.; Strandberg, T.; Laakkonen, M.L. Efficacy of Physical Exercise Intervention on Mobility and Physical Functioning in Older People with Dementia: A Systematic Review. Exp. Gerontol. 2013, 48, 85–93. [Google Scholar] [CrossRef]
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.F.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise Interventions for Older Adults: A Systematic Review of Meta-Analyses. J Sport Health Sci 2020, 10, 29–47. [Google Scholar] [CrossRef]
- Long, A.L.; di Lorito, C.; Logan, P.; Booth, V.; Howe, L.; Hood-Moore, V.; van der Wardt, V. The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 4562. [Google Scholar] [CrossRef]
- Gallant, M.; Winjum, K. Step Up to Stop Falls; SUNY: Albany, NY, USA, 2014. [Google Scholar]
- Kraak, M.J. Visualising Spatial Distributions. In Geographical Information Systems: Principles, Techniques, Management and Applications: Abridged; Wiley & Sons: Hoboken, NJ, USA, 2005; pp. 157–173. [Google Scholar]
- Gatrell, A.; Senior, M. Health and Health Care Applications. Geogr. Inf. Syst. 1999, 2, 925–938. [Google Scholar]
- Tsegaw, T.; Gadisa, E.; Seid, A.; Abera, A.; Teshome, A.; Mulugeta, A.; Herrero, M.; Argaw, D.; Jorge, A.; Aseffa, A. Identification of Environmental Parameters and Risk Mapping of Visceral Leishmaniasis in Ethiopia by Using Geographical Information Systems and a Statistical Approach. Geospat. Health 2013, 7, 299–308. [Google Scholar] [CrossRef]
- Xi, Y.L.; Ren, F.; Liang, S.; Zhang, J.; Lin, D.N. Spatial Analysis of the Distribution, Risk Factors and Access to Medical Resources of Patients with Hepatitis B in Shenzhen, China. Int. J. Environ. Res. Public Health 2014, 11, 11505–11527. [Google Scholar] [CrossRef]
- Pedersen, M.; Overgaard, D.; Andersen, I.; Baastrup, M.; Egerod, I. Mechanisms and Drivers of Social Inequality in Phase II Cardiac Rehabilitation Attendance: A Convergent Mixed Methods Study. J. Adv. Nurs. 2018, 74, 2181–2195. [Google Scholar] [CrossRef]
- Yiannakoulias, N.; Rowe, B.H.; Svenson, L.W.; Schopflocher, D.P.; Kelly, K.; Voaklander, D.C. Zones of Prevention: The Geography of Fall Injuries in the Elderly. Soc. Sci. Med. 2003, 57, 2065–2073. [Google Scholar] [CrossRef] [PubMed]
- Pascual, C.; Regidor, E.; Astasio, P.; Ortega, P.; Navarro, P.; Domínguez, V. The Association of Current and Sustained Area-Based Adverse Socioeconomic Environment with Physical Inactivity. Soc. Sci. Med. 2007, 65, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Donovan, R.J. Socioeconomic Status Differences in Recreational Physical Activity Levels and Real and Perceived Access to a Supportive Physical Environment. Prev. Med. 2002, 35, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Billaudeau, N.; Oppert, J.M.; Simon, C.; Charreire, H.; Casey, R.; Salze, P.; Badariotti, D.; Banos, A.; Weber, C.; Chaix, B. Investigating Disparities in Spatial Accessibility to and Characteristics of Sport Facilities: Direction, Strength, and Spatial Scale of Associations with Area Income. Health Place 2011, 17, 114–121. [Google Scholar] [CrossRef]
- Carlson, T.; York, S.; Primomo, J. The Utilization of Geographic Information Systems to Create a Site Selection Strategy to Disseminate an Older Adult Fall Prevention Program. Soc. Sci. J. 2011, 48, 159–174. [Google Scholar] [CrossRef]
- Kamel Boulos, M.N.; Roudsari, A.V.; Carson, E.R. Health Geomatics: An Enabling Suite of Technologies in Health and Healthcare. J. Biomed. Inform. 2001, 34, 195–219. [Google Scholar] [CrossRef]
- Witten, K.; Exeter, D.; Field, A. The Quality of Urban Environments: Mapping Variation in Access to Community Resources. Urban Stud. 2003, 40, 161–177. [Google Scholar] [CrossRef]
- Office for National Statistics. Mid-2018 Population Estimates for Census Output Area East Midlands. Census Output Area Population Estimates—East Midlands, England. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/censusoutputareaestimatesintheeastmidlandsregionofengland (accessed on 27 July 2021).
- Public Health England. Health Profile for England: 2017, Chapter 5: Inequality in health. Available online: https://www.gov.uk/government/publications/health-profile-for-england/chapter-5-inequality-in-health (accessed on 1 July 2022).
- One East Midlands. Rural Community Action Nottinghamshire Case Study; Nottingham. 2010. Available online: www.intelligenceeastmidlands.org.uk (accessed on 1 July 2022).
- Center for Ageing and Demography. Estimates of the Population for the UK, England and Wales, Scotland and Northern Ireland. Office of National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland (accessed on 21 June 2022).
- Alzheimers Research UK. Dementia Hotspot Maps. Dementia Statistics Hub. Available online: https://www.dementiastatistics.org/statistics/dementia-maps (accessed on 21 June 2022).
- House of Commons. Constituency Data: Health Conditions. Available online: https://commonslibrary.parliament.uk/constituency-data-how-healthy-is-your-area/#nationalregional (accessed on 14 July 2022).
- Office for National Statistics. Census 2011—% of 65 years and over in England and Wales. UK Census 2011. Available online: https://services.arcgis.com/XSeYKQzfXnEgju9o/arcgis/rest/services/Census2011_EnglandandWales_population/FeatureServer (accessed on 27 January 2021).
- Ordnance Survey. Index of Multiple Deprivation (no scale). Available online: https://services.arcgis.com/XSeYKQzfXnEgju9o/arcgis/rest/services/IMD2015_7Domains/FeatureServer (accessed on 27 January 2021).
- Esri. World Population Density Estimate (no scale). Available online: https://landscape7.arcgis.com/arcgis/rest/services/World_Population_Density_Estimate_2016/ImageServer (accessed on 27 January 2021).
- Ordnance Survey. OS Open Background Map (no scale). Available online: https://tiles.arcgis.com/tiles/qHLhLQrcvEnxjtPr/arcgis/rest/services/OS_Open_Background_2/MapServer (accessed on 27 January 2021).
- McLafferty, S.L. GIS and Health Care. Annu. Rev. Public Health 2003, 24, 25–42. [Google Scholar] [CrossRef]
- Samarasundera, E.; Walsh, T.; Cheng, T.; Koenig, A.; Jattansingh, K.; Dawe, A.; Soljak, M. Methods and Tools for Geographical Mapping and Analysis in Primary Health Care. Prim. Health Care Res. Dev. 2012, 13, 10–21. [Google Scholar] [CrossRef]
- Shergold, I.; Parkhurst, G.; Musselwhite, C. Rural Car Dependence: An Emerging Barrier to Community Activity for Older People. Transp. Plan. Technol. 2012, 35, 69–85. [Google Scholar] [CrossRef]
- Higgs, G.; Langford, M.; Norman, P. Accessibility to Sport Facilities in Wales: A GIS-Based Analysis of Socio-Economic Variations in Provision. Geoforum 2015, 62, 105–120. [Google Scholar] [CrossRef]
- Christie, S.; Morgan, G.; Heaven, M.; Sandifer, Q.; van Woerden, H. Analysis of Renal Service Provision in South and Mid Wales. Public Health 2005, 119, 738–742. [Google Scholar] [CrossRef] [PubMed]
- Yin, P. Urban–Rural Inequalities in Spatial Accessibility to Prenatal Care: A GIS Analysis of Georgia, USA, 2000–2010. GeoJournal 2019, 84, 671–683. [Google Scholar] [CrossRef]




| County | Number of Classes for Older People (People with Dementia) | Population Over 65 Years (Population Over 65 Years with Dementia) | Ratio of Over 65s/Class (People with Dementia/Class) |
|---|---|---|---|
| Derbyshire | 201 (4) | 174,956 (14,749) | 870 (3690) |
| Leicestershire | 82 (3) | 144,892 (13,723) | 1767 (4574) |
| Lincolnshire | 91 (5) | 179,805 (17,596) | 1976 (3519) |
| Northamptonshire | 79 (0) | 136,682 (8883) | 1730 (-) |
| Nottinghamshire | 67 (1) | 173,311 (13,245) | 2586 (13,245) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, A.; Timmons, S.; Di Lorito, C.; Booth, V.; Logan, P. “We Just Don’t Know Where They Are”: The Geographical Distribution of Exercise Classes for Older People, Including Those Living with Dementia in the East Midlands. Int. J. Environ. Res. Public Health 2023, 20, 2142. https://doi.org/10.3390/ijerph20032142
Long A, Timmons S, Di Lorito C, Booth V, Logan P. “We Just Don’t Know Where They Are”: The Geographical Distribution of Exercise Classes for Older People, Including Those Living with Dementia in the East Midlands. International Journal of Environmental Research and Public Health. 2023; 20(3):2142. https://doi.org/10.3390/ijerph20032142
Chicago/Turabian StyleLong, Annabelle, Stephen Timmons, Claudio Di Lorito, Vicky Booth, and Pip Logan. 2023. "“We Just Don’t Know Where They Are”: The Geographical Distribution of Exercise Classes for Older People, Including Those Living with Dementia in the East Midlands" International Journal of Environmental Research and Public Health 20, no. 3: 2142. https://doi.org/10.3390/ijerph20032142
APA StyleLong, A., Timmons, S., Di Lorito, C., Booth, V., & Logan, P. (2023). “We Just Don’t Know Where They Are”: The Geographical Distribution of Exercise Classes for Older People, Including Those Living with Dementia in the East Midlands. International Journal of Environmental Research and Public Health, 20(3), 2142. https://doi.org/10.3390/ijerph20032142