
Lessons Learned during a Rapidly Evolving COVID-19 Pandemic: Aboriginal and Torres Strait Islander-Led Mental Health and Wellbeing Responses Are Key

Abstract
:1. Introduction
1.1. The COVID-19 Pandemic and Early Public Health Responses in Australia
1.2. The Mental Health Response—The First Roundtable
1.3. Second Roundtable Context
2. Methods
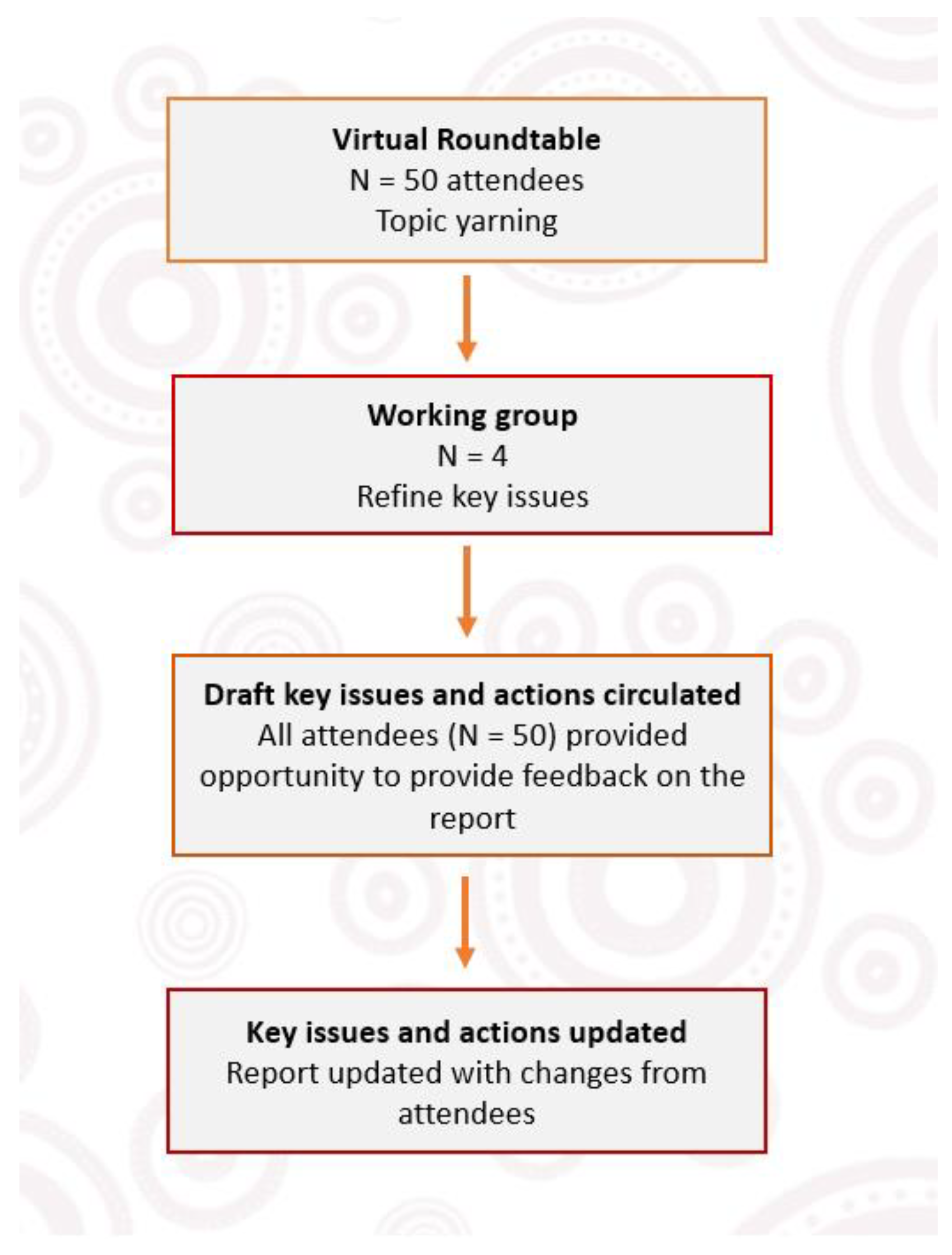
Collaboration Process
3. Results: Key Findings from the Roundtable
3.1. A Lack of Cultural Safety in Mainstream Services and Public Health Responses to COVID-19 Has Added to the Cumulative Trauma Experienced by Some Aboriginal and Torres Strait Islander Peoples—Governments Must Uphold Their Commitments to Formal Partnerships and Shared Decision Making to Ensure Cultural Safety
3.2. Aboriginal and Torres Strait Islander Mental Health and SEWB Challenges Were Amplified during COVID-19 due to a Lack of Appropriate Consultation with and Resourcing to ACCHOs—ACCHOs Must Be Empowered through Consultation and Needs-Based Funding
3.3. COVID-19 Has Exacerbated the Social Determinants of Health and Contributed to Health Inequity—Mental Health Challenges Must Be Addressed through Renewed Policy Focus and Government Funding to Target the Social and Cultural Determinants of Health
3.4. There Are Limited Data Relating to the Impacts of COVID-19 on Aboriginal and Torres Strait Islander Mental Health, and Effective Mental Health Responses—Data Sovereignty and Aboriginal and Torres Strait Islander Governance Are Essential to Building the Evidence Base of What Works for Aboriginal and Torres Strait Islander Peoples
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sachs, J.D.; Karim, S.S.A.; Aknin, L.; Allen, J.; Brosbøl, K.; Colombo, F.; Barron, G.C.; Espinosa, M.F.; Gaspar, V.; Gaviria, A.; et al. The Lancet Commission on lessons for the future from the COVID-19 pandemic. Lancet 2022, 400, 1224–1280. [Google Scholar] [CrossRef] [PubMed]
- Eades, S.; Eades, F.; McCaullay, D.; Nelson, L.; Phelan, P.; Stanley, F. Australia’s First Nations’ response to the COVID-19 pandemic. Lancet 2020, 396, 237–238. [Google Scholar] [CrossRef]
- Stanley, F.; Langton, M.; Ward, J.; McAullay, D.; Eades, S. Australian First Nations response to the pandemic: A dramatic reversal of the ‘gap’. J. Paediatr. Child Health 2021, 57, 1853–1856. [Google Scholar] [CrossRef]
- Crooks, K.; Casey, D.; Ward, J.S. First Nations people leading the way in COVID-19 pandemic planning, response and management. Med. J. Aust. 2020, 213, 151–152. [Google Scholar] [CrossRef]
- Dudgeon, P.; Alexi, J.; Derry, K.; Brideson, T.; Calma, T.; Darwin, L.; Gray, P.; Hirvonen, T.; McPhee, R.; Milroy, H. Mental health and well-being of Aboriginal and Torres Strait Islander peoples in Australia during COVID-19. Aust. J. Soc. Issues 2021, 56, 485–502. [Google Scholar] [CrossRef] [PubMed]
- Milroy, H.; COVID-19: Equity and Ethics in a Pandemic: Indigenous Perspectives. University of Western Australia. 2020. Available online: https://www.news.uwa.edu.au/archive/2020061712163/indigenous/covid-19-equity-and-ethics-pandemic-indigenous-perspectives/ (accessed on 3 March 2022).
- Bower, M.; Smout, S.; Ellsmore, S.; Donohoe-Bales, A.; Sivaprakash, P.P.; Lim, C.; Gray, M.; Francis, A.; Grager, A.; Riches, J. COVID-19 and Australia’s Mental Health: An Overview of Academic Literature, Policy Documents, Lived Experience Accounts, Media and Community Reports; Australia’s Mental Health Think Tank: Sydney, Australia, 2021. [Google Scholar]
- Faulkner, N.; Borg, K.; Zhao, K.; Smith, L. The Inclusive Australia Social Inclusion Index: 2021 Report. I. Australia. 2021. Available online: https://inclusive-australia.s3.amazonaws.com/files/Inclusive-Australia-2020-21-Social-Inclusion-Index-min.pdf (accessed on 22 March 2022).
- The Australian Government Department of Health. Australian Suicide Rates Down during COVID-19. 2021. Available online: https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/australian-suicide-rates-down-during-covid-19 (accessed on 1 October 2022).
- Coroners Court of Victoria. Suicides of Aboriginal and Torres Strait Islander People. Victoria 2018–2021. 2022. Available online: https://www.coronerscourt.vic.gov.au/sites/default/files/2022-01/Victorian%20suicides%20of%20Aboriginal%20and%20Torres%20Strait%20Islander%20people%20-%20Victoria%20-%202018-2021%20-%2020Jan2022.pdf (accessed on 1 October 2022).
- Dudgeon, P.; Collova, J.R.; Sutherland, S.; Derry, K.; Milroy, H.; Al Yaman, F.; Alexi, J.; Ansloos, J.; Banjavcic-Booker, S.; Bower, M.; et al. Aboriginal and Torres Strait Islander Mental Health and Wellbeing during the Evolving COVID-19 Pandemic: An Issues Paper. Transforming Indigenous Mental Health and Wellbeing Grant, The University of Western Australia, Poche Centre for Indigenous Health. 2022. Available online: https://api.research-repository.uwa.edu.au/ws/portalfiles/portal/200974240/Dudgeon_Collova_et_al_2022_COVID_Issues_Paper_2.pdf (accessed on 1 July 2022).
- Dudgeon, P.; Derry, K.; Arabena, K.; Brideson, T.; Cairney, S.; Calma, T.; Dalton, T.; Darwin, L.; Duarte, B.; Dyall, D. National COVID-19 Pandemic Issues Paper on Mental Health and Wellbeing for Aboriginal and Torres Strait Islander Peoples (Rosenburg, S.) 2020 The impact of COVID-19 on mental health–implications for policy and practice in Australia. The University of Western Australia, Poche Centre for Indigenous Health. 2020. Available online: https://apo.org.au/node/306661 (accessed on 1 December 2021).
- Moodie, N.; Ward, J.; Dudgeon, P.; Adams, K.; Altman, J.; Casey, D.; Cripps, K.; Davis, M.; Derry, K.; Eades, S. Roadmap to recovery: Reporting on a research taskforce supporting Indigenous responses to COVID-19 in Australia. Aust. J. Soc. Issues 2021, 56, 4–16. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Archived: WHO Timeline—COVID-19. 2020. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 13 September 2022).
- Finlay, S.; Wenitong, M. Aboriginal Community Controlled Health Organisations are taking a leading role in COVID-19 health communication. Aust. N. Z. J. Public Health 2020, 44, 251–252. [Google Scholar] [CrossRef]
- Wilson-Matenga, G.; Campbell, M.; Katterl, R.; Ellis, E.; Skeen, R. Partnership, trust and respect: NSW’s response to COVID-19 among Aboriginal people. Aust. N. Z. J. Public Health 2021, 45, 315. [Google Scholar] [CrossRef]
- Thornburn, K.; Golson, K.; Ridley, C.; Angus, R.; Marshall, M. Really Proper Dangerous One: Aboriginal Responses to the First Wave of COVID-19 in the Kimberley. N. R. Institute. 2022. Available online: https://apo.org.au/node/316406 (accessed on 1 December 2022).
- Kerrigan, V.; Lee, A.M.; Ralph, A.P.; Lawton, P.D. Stay strong: Aboriginal leaders deliver COVID-19 health messages. Health Promot. J. Aust. 2020, 32, 203. [Google Scholar] [CrossRef]
- The Australian Government Department of Health. Australian Health Sector Response Plan for Novel Coronavirus (COVID-19). 2020. Available online: https://www.health.gov.au/resources/publications/management-plan-for-aboriginal-and-torres-strait-islander-populations (accessed on 26 April 2022).
- Group of Eight Australia. COVID-19 Roadmap to Recovery: A Report for the Nation. Group of Eight. 2020. Available online: https://go8.edu.au/wp-content/uploads/2020/05/Go8-Road-to-Recovery.pdf (accessed on 1 December 2021).
- Flint, S.M.; Davis, J.S.; Su, J.Y.; Oliver-Landry, E.P.; Rogers, B.A.; Goldstein, A.; Thomas, J.H.; Parameswaran, U.; Bigham, C.; Freeman, K. Disproportionate impact of pandemic (H1N1) 2009 influenza on Indigenous people in the Top End of Australia’s Northern Territory. Med. J. Aust. 2010, 192, 617–622. [Google Scholar] [CrossRef] [Green Version]
- Solomon, T.G.A.; Starks, R.R.B.; Attakai, A.; Molina, F.; Cordova-Marks, F.; Kahn-John, M.; Antone, C.L.; Flores, M., Jr.; Garcia, F. The Generational Impact of Racism On Health: Voices from American Indian Communities: Study examines the generational impact of racism on the health of American Indian communities and people. Health Aff. 2022, 41, 281–288. [Google Scholar] [CrossRef]
- Steyn, N.; Binny, R.N.; Hannah, K.; Hendy, S.C.; James, A.; Kukutai, T.; Lustig, A.; McLeod, M.; Plank, M.J.; Ridings, K. Estimated inequities in COVID-19 infection fatality rates by ethnicity for Aotearoa New Zealand. medRxiv 2020. [Google Scholar] [CrossRef]
- Donaldson, A. How The Navajo Nation Beat Back COVID-19. 2021. Available online: https://www.deseret.com/utah/2021/11/14/22775922/how-the-navajo-nation-beat-back-covid-pandemic-precautions-care-for-tribal-elders (accessed on 9 March 2022).
- Navajo Nation Department of Health. Navajo Nation COVID-19 Dashboard. 2022. Available online: https://www.ndoh.navajo-nsn.gov/COVID-19/Data (accessed on 7 November 2022).
- Bessarab, D.; Ng’Andu, B. Yarning about yarning as a legitimate method in Indigenous research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef] [Green Version]
- The Government of Western Australia. WA’s Border Opening from Thursday 3 March 2022. Available online: https://www.wa.gov.au/government/announcements/was-border-opening-thursday-3-march-2022 (accessed on 22 April 2022).
- Van Beek, M.; Patulny, R. ‘The threat is in all of us’: Perceptions of loneliness and divided communities in urban and rural areas during COVID-19. J. Community Psychol. 2022, 50, 1531–1548. [Google Scholar] [CrossRef]
- Patulny, R.; Bower, M. Beware the “loneliness gap”? Examining emerging inequalities and long-term risks of loneliness and isolation emerging from COVID-19. Aust. J. Soc. Issues 2022, 57, 562–583. [Google Scholar] [CrossRef]
- Power, T.; Wilson, D.; Best, O.; Brockie, T.; Bearskin, L.B.; Millender, E.; Lowe, J. COVID-19 and Indigenous Peoples: An imperative for action. J. Clin. Nurs. 2020, 29, 2737–2741. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.; Uink, B.; Cross, S. Beyond the social: Cumulative implications of COVID-19 for first nations university students in Australia. Soc. Sci. Humanit. Open 2020, 2, 100083. [Google Scholar] [CrossRef]
- Altman, J. The Deadly Virus Delivers Accidental Benefit to Remote Indigenous Australia. Arena. 2020. Available online: https://arena.org.au/the-deadly-virus-delivers-accidental-benefit-to-remote-indigenous-australia/ (accessed on 1 February 2022).
- Smith, C.; Kearney, A.; Kotarba-Morley, A.; Wilson, C.; Grant, J.; Pollard, K.; Saikia, U. Friday essay: Voices from the Bush—How Lockdown Affects Remote Indigenous Communities Differently. The Conversation. 2020. Available online: https://theconversation.com/friday-essay-voices-from-the-bush-how-lockdown-affects-remote-indigenous-communities-differently-136953 (accessed on 18 March 2022).
- 13-YARN. About 13 YARN. 2022. Available online: https://www.13yarn.org.au/about-us (accessed on 1 February 2022).
- Lifeline. Australians Reaching Out for Help in Record Numbers. 20 August 2021. Available online: https://www.lifeline.org.au/media/0olpjjfq/20210820-australians-reaching-out-for-help-in-record-numbers.pdf (accessed on 1 September 2021).
- Mental Health Commission of NSW. The Ongoing Impact of the Pandemic. Insights from 2021 Survey Results. 2022. Available online: https://www.nswmentalhealthcommission.com.au/sites/default/files/2022-05/Community%20Wellbeing%20during%20COVID-19%202021%20Survey%20%20Insights%20Report.pdf (accessed on 7 November 2022).
- Marmot, M. Social determinants and the health of Indigenous Australians. Med. J. Aust. 2011, 194, 512–513. [Google Scholar] [CrossRef] [PubMed]
- Calma, T. Social determinants and the health of Indigenous peoples in Australia—A human rights based approach. In Proceedings of the International Symposium on the Social Determinants of Indigenous Health, Adelaide, Australia, 29–30 April 2007. [Google Scholar]
- Zubrick, S.R.; Shepherd, C.C.J.; Dudgeon, P.; Gee, G.; Paradies, Y.; Scrine, C.; Walker, R. Social determinants of social and emotional wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; De-partment of the Prime Minister and Cabinet: Perth, Australia, 2014; Volume 2, pp. 93–112. [Google Scholar]
- Gall, A.; Diaz, A.; Garvey, G.; Anderson, K.; Lindsay, D.; Howard, K. Self-reported wellbeing and health-related quality of life of Aboriginal and Torres Strait Islander people pre and post the first wave of the COVID-19 2020 pandemic. Aust. N. Z. J. Public Health 2022, 46, 170–176. [Google Scholar] [CrossRef]
- ALGA. Closing the Gap Implementation Plan. 2021. Available online: https://alga.com.au/app/uploads/ALGA-Closing-the-Gap-Implementation-Plan-4.pdf (accessed on 1 September 2022).
- Commonwealth of Australia. National Agreement on Closing the Gap. 2020. Available online: https://www.closingthegap.gov.au/national-agreement/national-agreement-closing-the-gap (accessed on 2 February 2022).
- Commonwealth of Australia. National Aboriginal and Torres Strait Islander Health Plan 2021–2031. 2021. Available online: https://www.health.gov.au/sites/default/files/documents/2021/12/national-aboriginal-and-torres-strait-islander-health-plan-2021-2031_2.pdf (accessed on 1 December 2022).
- Martin, K.; Mirraboopa, B. Ways of knowing, being and doing: A theoretical framework and methods for indigenous and indigenist research. J. Aust. Stud. 2003, 27, 203–214. [Google Scholar] [CrossRef] [Green Version]
- Geia, L.K.; Hayes, B.; Usher, K. Yarning/Aboriginal storytelling: Towards an understanding of an Indigenous perspective and its implications for research practice. Contemp. Nurse 2013, 46, 13–17. [Google Scholar] [CrossRef]
- Fogarty, W.; Lovell, M.; Langenberg, J.; Heron, M.-J. Deficit discourse and strengths-based approaches. In Changing the Narrative of Aboriginal and Torres Strait Islander Health and Wellbeing; The Lowitja Institute: Melbourne, Australia, 2018. [Google Scholar]
- Dudgeon, P.; Bray, A.; Walker, R. Self-determination and strengths-based Aboriginal and Torres Strait Islander suicide prevention: An emerging evidence-based approach. In Alternatives to Suicide; Elsevier: Amsterdam, The Netherlands, 2020; pp. 237–256. [Google Scholar]
- Commonwealth of Australia. National Strategic Framework for Aboriginal and Torres Strait Islander Peoples’ Mental Health and Social and Emotional Wellbeing (2017–2023); Commonwealth of Australia: Canberra, Australia, 2017. [Google Scholar]
- Milroy, H.; Dudgeon, P.; Walker, R. Community life and development programs–Pathways to healing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Telethon Kids Institute, Kulunga Aboriginal Research Development Unit, Department of the Prime Minister and Cabinet: Perth, Australia, 2014; Volume 2, pp. 419–436. [Google Scholar]
- Atkinson, J.; Nelson, J.; Atkinson, C. Trauma, transgenerational Transfer and Effects on Community Wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Telethon Kids Institute, Kulunga Aboriginal Research Development Unit, Department of the Prime Minister and Cabinet: Perth, Australia, 2010; pp. 135–144. [Google Scholar]
- Graham, S.; Blaxland, M.; Bolt, R.; Beadman, M.; Gardner, K.; Martin, K.; Doyle, M.; Beetson, K.; Murphy, D.; Bell, S. Aboriginal peoples’ perspectives about COVID-19 vaccines and motivations to seek vaccination: A qualitative study. BMJ Glob. Health 2022, 7, e008815. [Google Scholar] [CrossRef]
- Sutherland, S. Reconciliation: The Effects of Reconciliation Initiatives (Apologies) on the Social and Emotional Wellbeing of People Affected by Past Forced Removal Policies—A Transnational Study (Australia, Canada and New Zealand); Australian National University: Canberra, Australia, 2016. [Google Scholar] [CrossRef]
- Menzies, K. Understanding the Australian Aboriginal experience of collective, historical and intergenerational trauma. Int. Soc. Work. 2019, 62, 1522–1534. [Google Scholar] [CrossRef]
- National Aboriginal Community Controlled Health Organisation. National Housing and Homelessness Agreement Review. Submission to the Australian Productivity Commission. 2022. Available online: https://www.naccho.org.au/app/uploads/2022/04/NACCHO-Submission-to-the-National-Housing-and-Homelessness-Agreement-Review.pdf (accessed on 1 December 2021).
- Chandler, A. Indigenous Australians Said Hit by Vaccine Misinformation. 2021. Available online: https://www.bloomberg.com/news/articles/2021-12-03/indigenous-australians-said-to-be-hit-by-vaccine-misinformation (accessed on 5 February 2022).
- Larsson, P.; The Inherent Racism of Anti-Vaxx Movements. The Conversation. 2021. Available online: https://theconversation.com/the-inherent-racism-of-anti-vaxx-movements-163456 (accessed on 5 December 2021).
- RACGP. RACGP: Aboriginal and Torres Strait Islander Vaccination Rates a Critical Risk as Holiday Season Approaches. 2021. Available online: https://www.racgp.org.au/gp-news/media-releases/2021-media-releases/november-2021/racgp-aboriginal-and-torres-strait-islander-vaccin (accessed on 7 February 2022).
- Panaretto, K.S.; Wenitong, M.; Button, S.; Ring, I.T. Aboriginal community controlled health services: Leading the way in primary care. Med. J. Aust. 2014, 200, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Pearson, O.; Schwartzkopff, K.; Dawson, A.; Hagger, C.; Karagi, A.; Davy, C.; Brown, A.; Braunack-Mayer, A. Aboriginal community controlled health organisations address health equity through action on the social determinants of health of Aboriginal and Torres Strait Islander peoples in Australia. BMC Public Health 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Naren T, Widdicombe D. Aboriginal communities need to be at the forefront of the COVID-19 vaccination campaign. Aust. J. Gen. Pract. 2022, 51 (Suppl. 2). [Google Scholar] [CrossRef]
- Naren, T.; Burzacott, J.; West, C.; Widdicombe, D. Role of Aboriginal Health Practitioners in administering and increasing COVID-19 vaccination rates in a Victorian Aboriginal Community Controlled Health Organisation. Rural Remote Health 2021, 21, 7043. [Google Scholar] [CrossRef]
- National Indigenous Times. Hitting 90 Percent Vaccination, Beagle Bay Re-Opens to Public. 2021. Available online: https://www.nit.com.au/hitting-90-per-cent-vaccination-beagle-bay-re-opens-to-public/ (accessed on 7 February 2022).
- Australian Health Ministers’ Advisory Council. Cultural respect Framework 2016–2026 for Aboriginal and Torres Strait Islander Health; Australian Health Ministers’ Advisory Council: Canberra, Australia, 2016. [Google Scholar]
- Aboriginal Health Council of Western Australia. Media Release: AHCWA Calls for More Partnership and Transparency on WA COVID-19 Response. n.d. Available online: https://www.ahcwa.org.au/2022/02/01/media-release-ahcwa-calls-for-more-partnership-and-transparency-on-wa-covid-19-response/ (accessed on 20 March 2022).
- United Nations General Assembly. Declaration on the Rights of Indigenous Peoples; United Nations General Assembly: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. Declaration of Alma-Ata. 1978. Available online: https://www.who.int/teams/social-determinants-of-health/declaration-of-alma-ata (accessed on 22 March 2021).
- TIMHWB. Transforming Indigenous Mental Health and Wellbeing Project. Social and Emotional Wellbeing Gathering 3 Report: 6th-8thSeptember 2022. 2022. Available online: https://timhwb.org.au/sewb-gatherings/ (accessed on 22 December 2022).
- Quinn, S.C.; Kumar, S. Health inequalities and infectious disease epidemics: A challenge for global health security. Biosecur. Bioterrorism Biodefense Strategy Pract. Sci. 2014, 12, 263–273. [Google Scholar] [CrossRef] [Green Version]
- Aboriginal Health Council of Western Australia. The “Unsung” Impact of COVID-19 on the Aboriginal Community Controlled Health Services in Western Australia. 2020. Available online: https://apo.org.au/sites/default/files/resource-files/2020-06/apo-nid306050.pdf (accessed on 1 February 2022).
- Walker, R.; Usher, K.; Jackson, D.; Reid, C.; Hopkins, K.; Shepherd, C.; Smallwood, R.; Marriott, R. Connection to... Addressing digital inequities in supporting the well-being of young Indigenous Australians in the wake of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2141. [Google Scholar] [CrossRef]
- Higgins, I.; This Family Tried to Self-Isolate with Four Generations under One Roof. It Led to ‘Boiling Point’. 2021. Available online: https://www.abc.net.au/news/2021-08-01/covid-restrictions-highlight-indigenous-community-housing-crisis/100317808 (accessed on 5 December 2021).
- Sutherland, S.; Wingett, A.; Payne, D.; Restrictions on Cultural Hunting Practices Are Limiting Indigenous People’s Access to Food during the Pandemic. The Conversation. 2021. Available online: https://theconversation.com/restrictions-on-cultural-hunting-practices-are-limiting-indigenous-peoples-access-to-food-during-the-pandemic-168267 (accessed on 1 December 2021).
- NPY Women’s Council. COVID Placing Women and Children at Greater Risk of Domestic Violence. 2022. Available online: https://www.npywc.org.au/news/covid-placing-women-and-children-at-greater-risk-of-domestic-violence/?mc_cid=deb41875f7&mc_eid=31bb07477c (accessed on 1 September 2022).
- O’Kane, G. COVID-19 puts the spotlight on food insecurity in rural and remote Australia. Aust. J. Rural Health 2020, 28, 319. [Google Scholar] [CrossRef]
- Gray, D.M.; Anyane-Yeboa, A.; Balzora, S.; Issaka, R.B.; May, F.P. COVID-19 and the other pandemic: Populations made vulnerable by systemic inequity. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 520–522. [Google Scholar] [CrossRef] [PubMed]
- National Indigenous Times. Derbarl Yerrigan Committed to Vaccine Rollout Despite Lack of Government Support. 2021. Available online: https://www.nit.com.au/derbarl-yerrigan-committed-to-vaccine-rollout-despite-lack-of-government-support/ (accessed on 7 September 2022).
- ABC News. Wilcannia Gets COVID Repreive as Motorhomes Arrive to Form Isolation Hub. 2021. Available online: https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846?utm_campaign=abc_news_web&utm_content=link&utm_medium=content_shared&utm_source=abc_news_web (accessed on 1 February 2022).
- Gee, G.; Dudgeon, P.; Schultz, C.; Hart, A.; Kelly, K. Aboriginal and Torres Strait Islander social and emotional wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Telethon Kids Institute, Kulunga Aboriginal Research Development Unit, Department of the Prime Minister and Cabinet: Perth, Australia, 2014; Volume 2, pp. 55–68. [Google Scholar]
- Finlay, S.M.; Canuto, K.; Canuto, K.; Neal, N.; Lovett, R.W. Aboriginal and Torres Strait Islander connection to culture: Building stronger individual and collective wellbeing. Med. J. Aust. 2021, 214, 12–16. [Google Scholar]
- Calma, T.; Dudgeon, P.; Bray, A. Aboriginal and Torres Strait Islander social and emotional wellbeing and mental health. Aust. Psychol. 2017, 52, 255–260. [Google Scholar] [CrossRef] [Green Version]
- Milroy, H. The Dance of Life. 2006. Available online: https://www.ranzcp.org/practice-education/aboriginal-torres-strait-islander-mental-health/the-dance-of-life (accessed on 5 March 2022).
- Dudgeon, P.; Milroy, J.; Calma, T.; Luxford, Y.; Ring, I.; Walker, R.; Cox, A.; Georgatos, G.; Holland, C. Solutions That Work: What the Evidence and Our People Tell Us; University of Western Australia: Perth, Australia, 2016. [Google Scholar]
- Kukutai, T.; Taylor, J. Indigenous Data Sovereignty: Toward an Agenda; ANU Press: Canberra, Australia, 2016. [Google Scholar]
- Carroll, S.R.; Garba, I.; Figueroa-Rodríguez, O.L.; Holbrook, J.; Lovett, R.; Materechera, S.; Parsons, M.; Raseroka, K.; Rodriguez-Lonebear, D.; Rowe, R.; et al. The CARE Principles for Indigenous Data Governance. Data Sci. J. 2020, 19, 43. [Google Scholar] [CrossRef]
- Productivity Commission. Indigenous Evaluation Strategy. 2020. Available online: https://www.pc.gov.au/inquiries/completed/indigenous-evaluation/strategy/indigenous-evaluation-strategy.pdf (accessed on 22 February 2022).


{kind=link}
| Key Issue Summary | Key Action Summary |
|---|---|
| A lack of cultural safety in mainstream services and public health responses to COVID-19 has added to the cumulative trauma experienced by some Aboriginal and Torres Strait Islander peoples. For example, a lack of cultural safety throughout the vaccine rollout contributed to vaccine hesitancy, with impacts to mental health. | Governments must uphold their commitments to formal partnerships and shared decision making to ensure cultural safety. All mainstream organisations whose work impacts Aboriginal and Torres Strait Islander people should implement the Cultural Respect Framework. |
| Aboriginal and Torres Strait Islander mental health and SEWB challenges were amplified during COVID-19 due to a lack of appropriate consultation with and resourcing to ACCHOs. | ACCHOs must be empowered through consultation and needs-based funding. |
| COVID-19 has exacerbated the social determinants of health and contributed to health inequity. | Mental health challenges must be addressed through renewed policy focus and government funding to target the social and cultural determinants of health. |
| There are limited data relating to the impacts of COVID-19 on Aboriginal and Torres Strait Islander mental health, and effective mental health responses. | Data sovereignty and Aboriginal and Torres Strait Islander governance are essential to building the evidence base of what works for Aboriginal and Torres Strait Islander peoples. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dudgeon, P.; Collova, J.R.; Derry, K.; Sutherland, S. Lessons Learned during a Rapidly Evolving COVID-19 Pandemic: Aboriginal and Torres Strait Islander-Led Mental Health and Wellbeing Responses Are Key. Int. J. Environ. Res. Public Health 2023, 20, 2173. https://doi.org/10.3390/ijerph20032173
Dudgeon P, Collova JR, Derry K, Sutherland S. Lessons Learned during a Rapidly Evolving COVID-19 Pandemic: Aboriginal and Torres Strait Islander-Led Mental Health and Wellbeing Responses Are Key. International Journal of Environmental Research and Public Health. 2023; 20(3):2173. https://doi.org/10.3390/ijerph20032173
Chicago/Turabian StyleDudgeon, Patricia, Jemma R. Collova, Kate Derry, and Stewart Sutherland. 2023. "Lessons Learned during a Rapidly Evolving COVID-19 Pandemic: Aboriginal and Torres Strait Islander-Led Mental Health and Wellbeing Responses Are Key" International Journal of Environmental Research and Public Health 20, no. 3: 2173. https://doi.org/10.3390/ijerph20032173