
Personal Growth and Life Satisfaction during Fertility Treatment—A Comparison between Arab and Jewish Women



Abstract
1. Introduction
1.1. Infertility and Stress
1.2. Personal Growth and Life Satisfaction
1.3. Coping Flexibility
1.4. Infertility and Cultural Orientation: Individualism vs. Collectivism
1.5. Stigma
1.6. The Current Study
- (1)
- A negative linear relationship would be found between level of stress and life satisfaction, so that the higher the level of stress, the lower the satisfaction with life.
- (2)
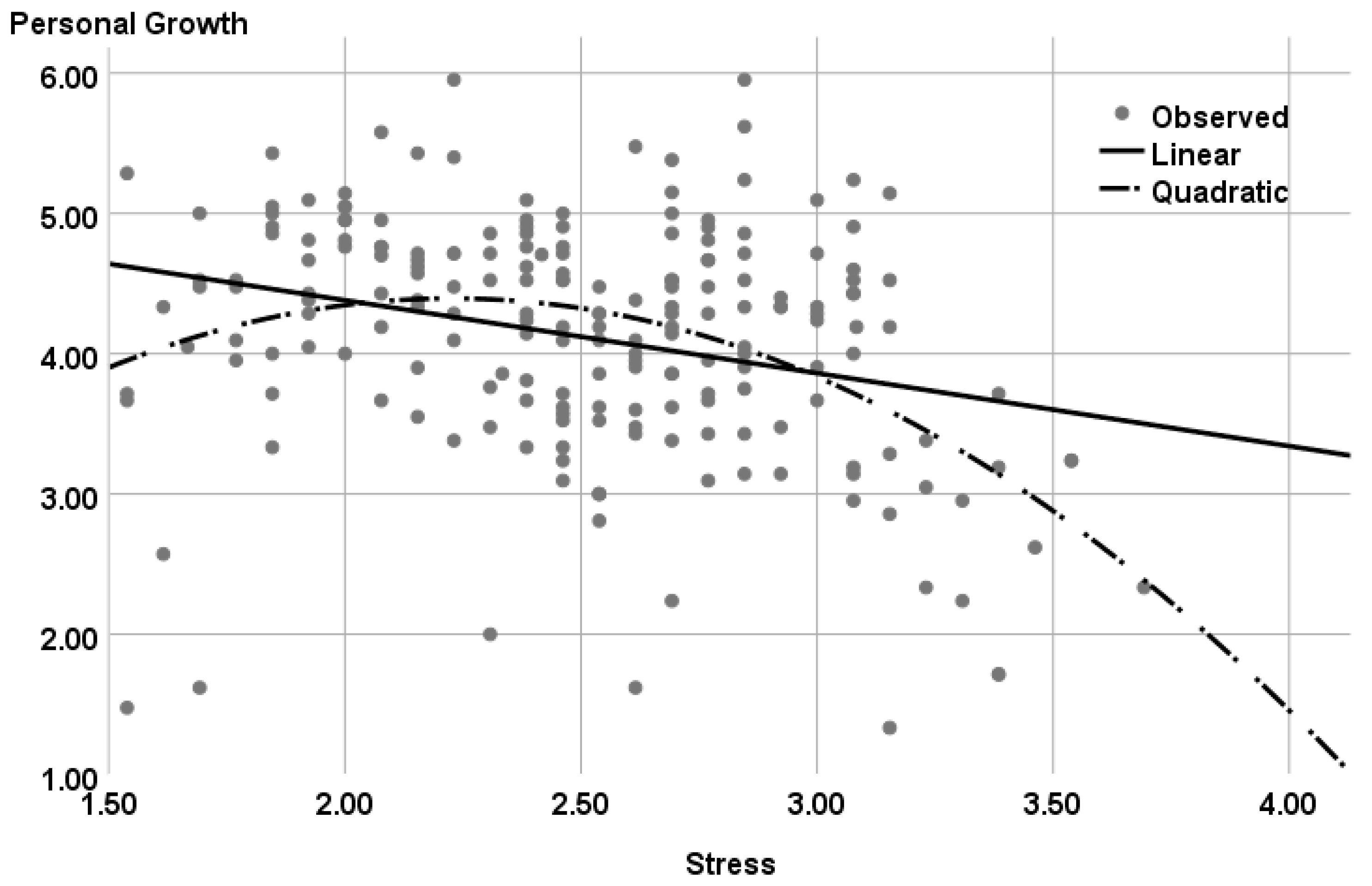
- A curvilinear relationship would be found between level of stress and personal growth, so that moderate levels of stress would be associated with higher levels of growth and high or low levels of stress would be associated with lower levels of growth.
- (3)
- Coping flexibility would be positively associated with both life satisfaction and personal growth, so that the higher the level of coping flexibility, the higher the satisfaction with life and growth.
- (1)
- Is there a difference in the levels of stress, personal growth, and life satisfaction between Arab and Jewish women?
- (2)
- Is the cultural orientation associated with personal growth and life satisfaction?
- (3)
- Is the perceived stigma attached to fertility treatment associated with personal growth and life satisfaction?
- (4)
- What is the unique and combined contribution of the study variables to personal growth and life satisfaction?
- (5)
- Do coping flexibility, cultural orientation (collectivism/individualism), perceived stigma, and ethnicity (Arab, Jewish) moderate the association between stress on the one hand and personal growth and life satisfaction on the other?
2. Method
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Differences between Study Groups
3.2. Associations between Study Variables
3.3. Contribution of the Study Variables to Personal Growth and Life Satisfaction
3.4. A Curvilinear Association between Stress and Personal Growth
4. Discussion
4.1. Comparison between Arab and Jewish Women
4.2. The Role of Stress in Life Satisfaction and Personal Growth
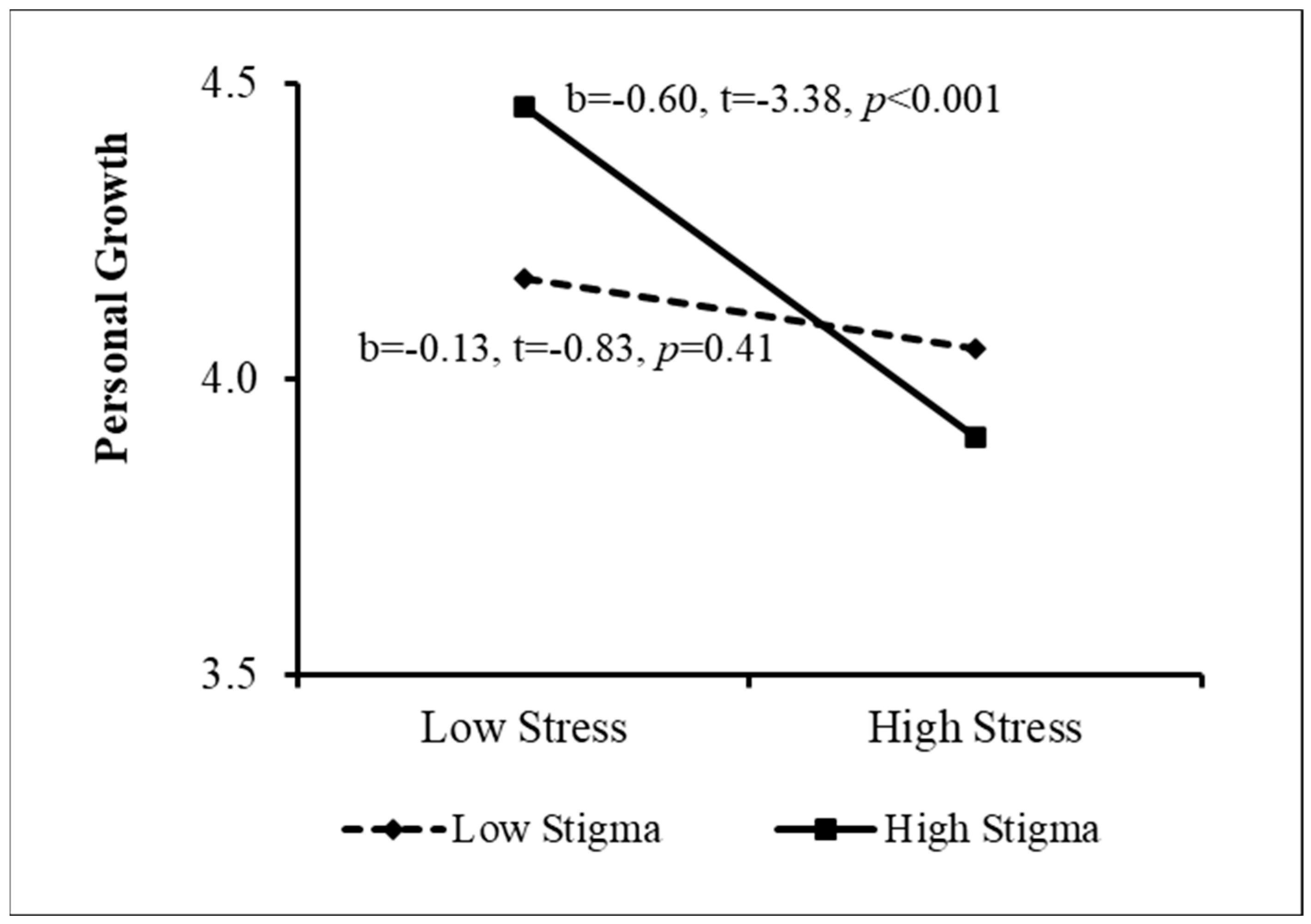
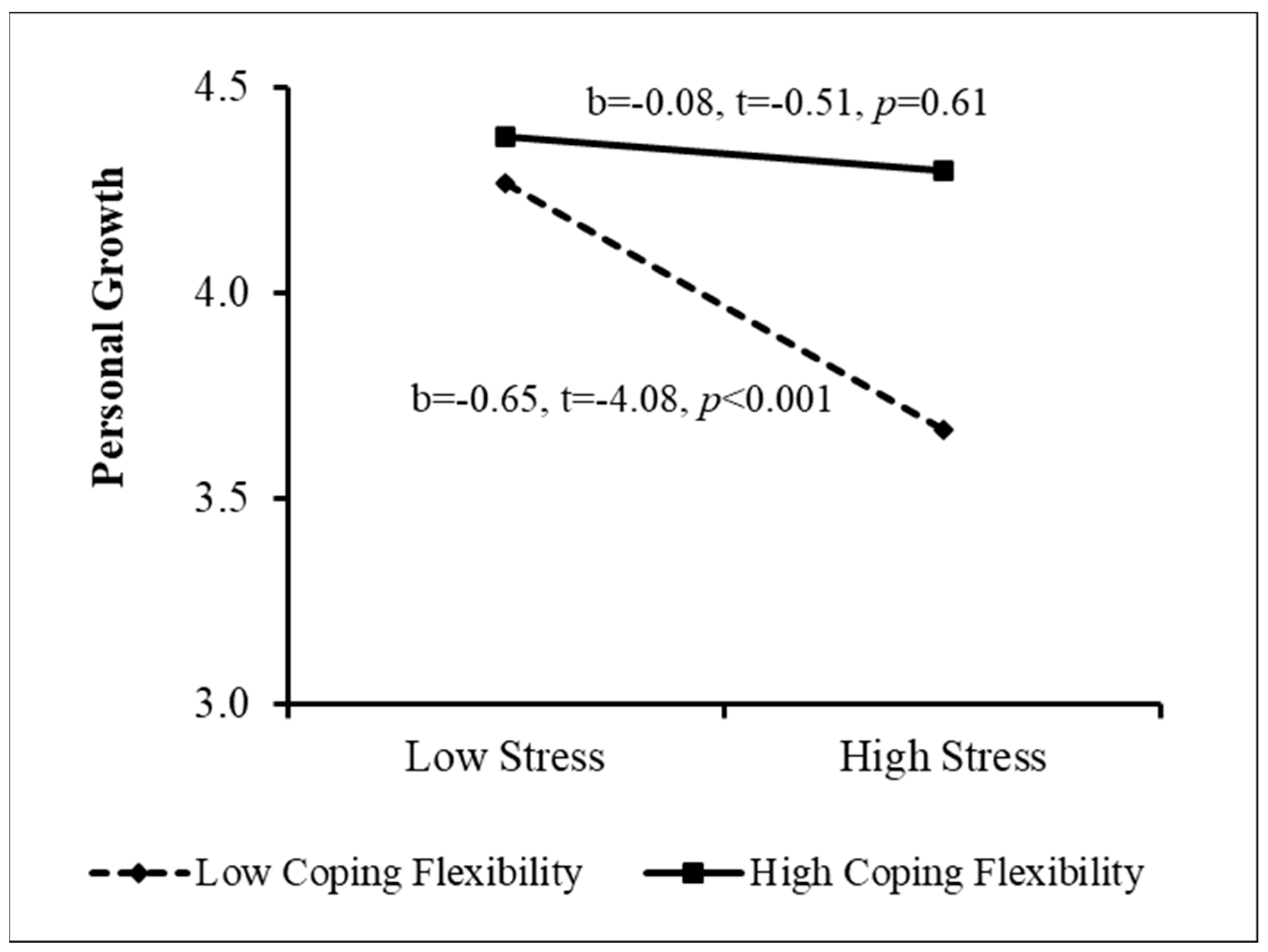
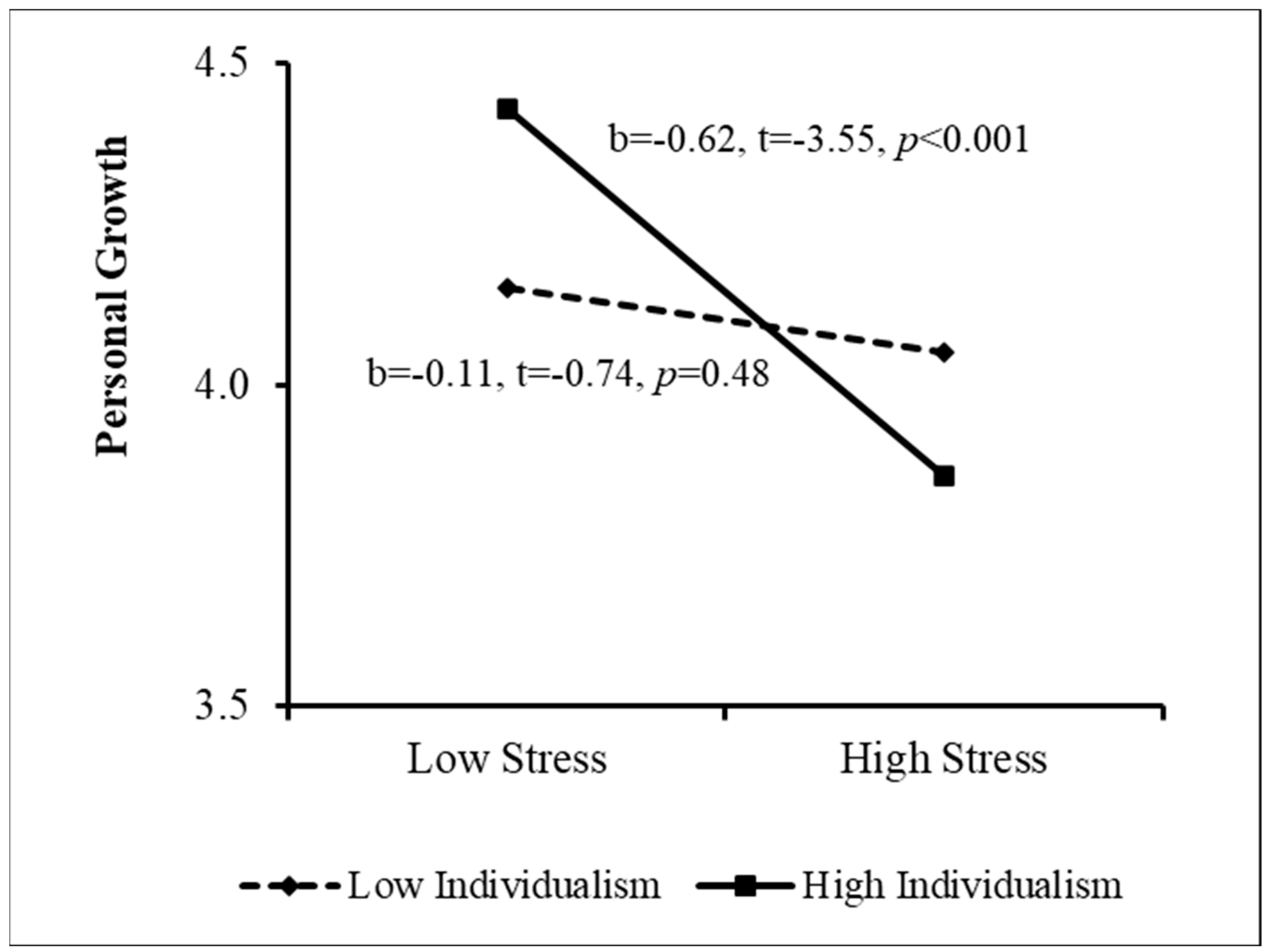
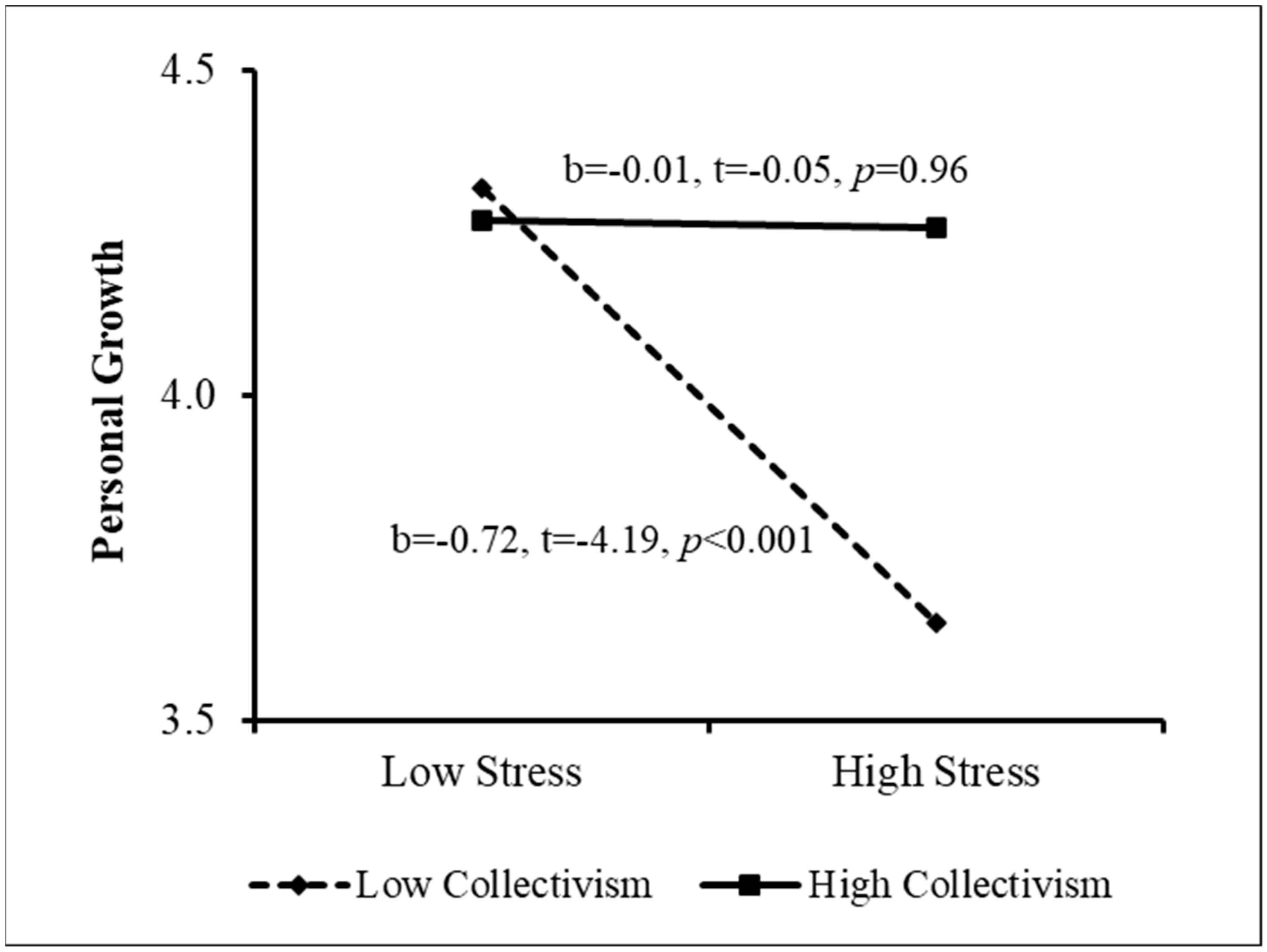
4.3. The Contribution of Coping Flexibility, Perceived Stigma, and Cultural Orientation to the Relationship between Stress and Growth
4.4. The Role of Coping Flexibility, Perceived Stigma, and Cultural Orientation in the Relationship between Stress and Life Satisfaction
4.5. Contribution of Sociodemographic Variables to Growth and Life Satisfaction
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cousineau, T.M.; Domar, A.D. Psychological impact of infertility. Best Pract. Res. Clin. Obstet. Gynecol. 2007, 21, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Daibes, M.A.; Safadi, R.R.; Athamneh, T.; Anees, I.F.; Constantino, R.E. ‘Half a woman, half a man; that is how they make me feel’: A qualitative study of rural Jordanian women’s experience of infertility. Cult. Health Sex. 2018, 20, 516–530. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA.
- Schaefer, J.A.; Moos, R.H. The context for posttraumatic growth: Life crises, individual and social resources, and coping. In Posttraumatic Growth: Positive Changes in the Aftermath of Crisis; Tedeschi, R.G., Park, C., Calhoun, L.G., Eds.; Lawrence Erlbaum: Mahwah, NJ, USA, 1998; pp. 99–126. [Google Scholar]
- Tedeschi, R.G.; Shakespeare-Finch, J.; Taku, K.; Calhoun, L.G. Posttraumatic Growth. Theory, Research, and Applications; Routledge: London, UK, 2018. [Google Scholar]
- Kong, L.; Fang, M.; Ma, T.; Li, G.; Yang, F.; Meng, Q.; Li, Y.; Li, P. Positive affect mediates the relationships between resilience, social support and posttraumatic growth of women with infertility. Psychol. Health Med. 2018, 23, 707–716. [Google Scholar] [CrossRef]
- Yu, Y.; Peng, L.; Chen, L.; Long, L.; He, W.; Li, M.; Wang, T. Resilience and social support promote posttraumatic growth of women with infertility: The mediating role of positive coping. Psychiatry Res. 2014, 215, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Zegers-Hochschild, F.; Adamson, G.D.; de Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; van der Poel, S. The International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary on ART terminology, 2009. Hum. Reprod. 2009, 24, 2683–2687. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. 2015. Available online: http://www.health.gov.il/PublicationsFiles/IVF1986_2012.pdf (accessed on 20 June 2021).
- Birenbaum-Carmeli, D. Thirty-five years of assisted reproductive technologies in Israel. Reprod. Biomed. Soc. Online 2016, 2, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Copen, C.E.; Stephen, E.H. Infertility Service Use in the United States: Data from the National Survey of Family Growth, 1982–2010 (No. 1250); US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Washington, DC, USA, 2014. [Google Scholar]
- Grant, L.E.; Cochrane, S. Acupuncture for the mental and emotional health of women undergoing IVF treatment: A comprehensive review. Aust. J. Acupunct. Chin. Med. 2014, 9, 5. [Google Scholar]
- Benyamini, Y.; Gefen-Bardarian, Y.; Gozlan, M.; Tabiv, G.; Shiloh, S.; Kokia, E. Coping specificity: The case of women coping with infertility treatments. Psychol. Health 2008, 23, 221–241. [Google Scholar] [CrossRef]
- Madge, V. Infertility, women and assisted reproductive technologies: An exploratory study in Pune, India. Indian J. Gend. Stud. 2011, 18, 1–26. [Google Scholar] [CrossRef]
- Papadatou, D.; Papaligoura, Z.G.; Bellali, T. From infertility to successful third-party reproduction: The trajectory of Greek women. Qual. Health Res. 2016, 26, 399–410. [Google Scholar] [CrossRef]
- Culley, L.; Hudson, N.; Van Rooij, F. (Eds.) Marginalized Reproduction: Ethnicity, Infertility and Assisted Reproductive Technologies; Earthscan: London, UK, 2012. [Google Scholar]
- Patel, A.; Sharma, P.S.V.N.; Narayan, P.; Binu, V.S.; Dinesh, N.; Pai, P.J. Prevalence and predictors of infertility-specific stress in women diagnosed with primary infertility: A clinic-based study. J. Hum. Reprod. Sci. 2016, 9, 28. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.S.; Berger, R.; Berlow, N.; Rovner-Ferguson, H.; Figlerski, L.; Gardner, S.; Malave, A.F. Posttraumatic growth and social support in individuals with infertility. Hum. Reprod. 2010, 25, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Valsangkar, S.; Bodhare, T.; Bele, S.; Sai, S. An evaluation of the effect of infertility on marital, sexual satisfaction indices and health-related quality of life in women. J. Hum. Reprod. Sci. 2011, 4, 80. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. Posttraumatic growth: Conceptual foundation and empirical evidence. Psychol. Inq. 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Rozen, G.; Taubman-Ben-Ari, O.; Strauss, T.; Morag, I. Personal growth of mothers of preterms: Objective severity of the event, subjective stress, personal resources, and maternal emotional support. J. Happiness Stud. 2018, 19, 2167–2186. [Google Scholar] [CrossRef]
- Berger, R.; Paul, M.S.; Henshaw, L.A. Women’s experience of infertility: A multi-systemic perspective. J. Int. Women Stud. 2013, 14, 54–68. [Google Scholar]
- Diener, E. Subjective well-being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef]
- Huebner, E.S.; Gilman, R.; Laughlin, J.E. A multimethod investigation of the multidimensionality of children’s well-being reports: Discriminant validity of life satisfaction and self-esteem. Soc. Indic. Res. 1999, 46, 1–22. [Google Scholar] [CrossRef]
- Maroufizadeh, S.; Ghaheri, A.; Samani, R.O.; Ezabadi, Z. Psychometric properties of the Satisfaction with Life Scale (SWLS) in Iranian infertile women. Int. J. Reprod. Biomed. 2016, 14, 57. [Google Scholar] [CrossRef]
- Dembińska, A.A. Psychological determinants of life satisfaction in women undergoing infertility treatment. Health Psychol. Rep. 2016, 4, 146–158. [Google Scholar] [CrossRef]
- McCracken, L.M.; Morley, S. The psychological flexibility model: A basis for integration and progress in psychological approaches to chronic pain management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Katz, M. Grief and growth of bereaved siblings as related to attachment style and flexibility. Death Stud. 2015, 39, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Verhaak, C.M.; Smeenk, J.M.J.; Nahuis, M.J.; Kremer, J.A.M.; Braat, D.D.M. Long-term psychological adjustment to IVF/ICSI treatment in women. Hum. Reprod. 2007, 22, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Greil, A.L.; Slauson-Blevins, K.; McQuillan, J. The experience of infertility: A review of recent literature. Sociol. Health Illn. 2010, 32, 140–162. [Google Scholar] [CrossRef] [PubMed]
- Pines, A.M.; Zaidman, N. Gender, culture, and social support: A male–female, Israeli Jewish-Arab comparison. Sex Roles 2003, 49, 571–586. [Google Scholar] [CrossRef]
- Kasler, J.; Zysberg, L.; Gal, R. Culture, collectivism-individualism and college student plagiarism. Ethics Behav. 2021, 31, 488–497. [Google Scholar] [CrossRef]
- Triandis, H.C. Individualism and Collectivism; Westview: New York, NY, USA, 1995. [Google Scholar]
- Inhorn, M.C. Making Muslim babies: IVF and gamete donation in Sunni versus Shi’a Islam. Cult. Med. Psychiatry 2006, 30, 427–450. [Google Scholar] [CrossRef]
- Obeidat, H.M.; Hamlan, A.M.; Callister, L.C. Missing motherhood: Jordanian women’s experiences with infertility. Adv. Psychiatry 2014, 2014, 241075. [Google Scholar] [CrossRef]
- Brehm, S.S.; Kassin, S.M.; Fein, S. Social identity theory. In Social Psychology; Houghton Mifflin Company: Boston, MA, USA, 1999. [Google Scholar]
- Missmer, S.A.; Seifer, D.B.; Jain, T. Cultural factors contributing to health care disparities among patients with infertility in Midwestern United States. Fertil. Steril. 2011, 95, 1943–1949. [Google Scholar] [CrossRef]
- Serour, G.I. Islamic perspectives in human reproduction. Reprod. Biomed. Online 2008, 17, 34–38. [Google Scholar] [CrossRef]
- Moura-Ramos, M.; Gameiro, S.; Canavarro, M.C.; Soares, I. Assessing infertility stress: Re-examining the factor structure of the Fertility Problem Inventory. Hum. Reprod. 2012, 27, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Taubman-Ben-Ari, O. Blossoming and growing in the transition to parenthood. In Pathways and Barriers to the Transition to Parenthood—Existential Concerns Regarding Fertility, Pregnancy, and Early Parenthood; Taubman-Ben-Ari, O., Ed.; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Kiesswetter, M.; Marsoner, H.; Luehwink, A.; Fistarol, M.; Mahlknecht, A.; Duschek, S. Impairments in life satisfaction in infertility: Associations with perceived stress, affectivity, partnership quality, social support and the desire to have a child. Behav. Med. 2020, 46, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 4, 385–396. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma. J. Trauma. Stress 1996, 9, 455–471. [Google Scholar] [PubMed]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Vriezekolk, J.E.; van Lankveld, W.G.; Eijsbouts, A.M.; van Helmond, T.; Geenen, R.; van den Ende, C.H. The Coping Flexibility Questionnaire: Development and initial validation in patients with chronic rheumatic diseases. Rheumatol. Int. 2012, 32, 2383–2391. [Google Scholar] [CrossRef]
- Singelis, T.M.; Triandis, H.C.; Bhawuk, D.P.; Gelfand, M.J. Horizontal and vertical dimensions of individualism and collectivism: A theoretical and measurement refinement. Cross Cult. Res. 1995, 29, 240–275. [Google Scholar] [CrossRef]
- Komiya, N.; Good, G.E.; Sherrod, N.B. Emotional openness as a predictor of college students’ attitudes toward seeking psychological help. J. Couns. Psychol. 2000, 47, 138. [Google Scholar] [CrossRef]
- Naab, F.; Brown, R.; Heidrich, S. Psychosocial health of infertile Ghanaian women and their infertility beliefs. J. Nurs. Scholarsh. 2013, 45, 132–140. [Google Scholar] [CrossRef]
- Hayes, A.F. Methodology in the Social Sciences. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Bar, H. Missing data—Mechanisms and possible solutions. Cult. Educ. 2017, 29, 492–525. [Google Scholar]
- Little, R.J. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Cohen, A. The relationship between multiple commitments and organizational citizenship behavior in Arab and Jewish culture. J. Vocat. Behav. 2006, 69, 105–118. [Google Scholar] [CrossRef]
- Dwairy, M.A. Counseling and Psychotherapy with Arabs and Muslims: A Culturally Sensitive Approach; Teachers College Press: New York, NY, USA, 2006. [Google Scholar]
- Joseph, S. (Ed.) Intimate Selving in Arab Families: Gender, Self, and Identity; Syracuse University Press: Syracuse, NY, USA, 1999. [Google Scholar]
- Rashad, H.; Osman, M.I.; Roudi-Fahimi, F. Marriage in the Arab World; Population Reference Bureau: Washington, DC, USA, 2005; pp. 1–8. [Google Scholar]
- Hammoudeh, D.; Hamayel, L.; Abu-Rmeileh, N.M.; Giacaman, R. Effect of infertility on women in the occupied Palestinian territory: A pilot qualitative study. Lancet 2013, 382, S15. [Google Scholar] [CrossRef]
- Dwairy, M. Culture-analysis and metaphor therapy with Arab-Muslim clients. J. Clin. Psychol. 2009, 65, 199–209. [Google Scholar] [PubMed]
- Fido, A.; Zahid, M.A. Coping with infertility among Kuwaiti women: Cultural perspectives. Int. J. Soc. Psychiatry 2004, 50, 294–300. [Google Scholar] [CrossRef]
- Ghafouri, S.F.; Ghanbari, S.; Fallahzadeh, H.; Shokri, O. The relation between marital adjustment and posttraumatic growth in infertile couples: The mediatory role of religious coping strategies. J. Reprod. Infertil. 2016, 17, 221–229. [Google Scholar]
- Ng, G.C.; Mohamed, S.; Sulaiman, A.H.; Zainal, N.Z. Anxiety and depression in cancer patients: The association with religiosity and religious coping. J. Relig. Health 2017, 56, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, L.G.; Cann, A.; Tedeschi, R.G. The posttraumatic growth model: Sociocultural considerations. In Posttraumatic Growth and Culturally Competent Practice: Lessons Learned from around the Globe; Weiss, T., Berger, R., Eds.; John Wiley and Sons Inc.: Hoboken, NJ, USA, 2010; pp. 1–14. [Google Scholar]
- Taubman-Ben-Ari, O. Becoming and developing: Personal growth in the wake of parenthood and grandparenthood. In Meaning, Mortality, and Choice—The Social Psychology of Existential Concerns; Shaver, P.R., Mikulincer, M., Eds.; APA: Washington, DC, USA, 2012; pp. 163–181. [Google Scholar]
- Park, C.L.; Fenster, J.R. Stress-related growth: Predictors of occurrence and correlates with psychological adjustment. J. Soc. Clin. Psychol. 2004, 23, 195–215. [Google Scholar] [CrossRef]
- Dekel, R.; Shaked, O.Z.; Ben-Porat, A.; Itzhaky, H. Posttraumatic stress disorder upon admission to shelters among female victims of domestic violence: An ecological model of trauma. Violence Vict. 2019, 34, 329–345. [Google Scholar] [CrossRef]
- Benyamini, Y.; Gozlan, M.; Weissman, A. Normalization as a strategy for maintaining quality of life while coping with infertility in a pronatalist culture. Int. J. Behav. Med. 2017, 24, 871–879. [Google Scholar] [CrossRef]
- Rooney, K.L.; Domar, A.D. The impact of stress on fertility treatment. Curr. Opin. Obstet. Gynecol. 2016, 28, 198–201. [Google Scholar] [CrossRef] [PubMed]
- McQuillan, J.; Torres Stone, R.A.; Greil, A.L. Infertility and life satisfaction among women. J. Fam. Issues 2007, 28, 955–981. [Google Scholar] [CrossRef]
- Taku, K.; Cann, A.; Tedeschi, R.G.; Calhoun, L.G. Core beliefs shaken by an earthquake correlate with posttraumatic growth. Psychol. Trauma Theory Res. Pract. Policy 2015, 7, 563–569. [Google Scholar] [CrossRef]
- Triplett, K.N.; Tedeschi, R.G.; Cann, A.; Calhoun, L.G.; Reeve, C.L. Posttraumatic growth, meaning in life, and life satisfaction in response to trauma. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 400–410. [Google Scholar] [CrossRef]
- Buser, J.K.; Kearney, A. Stress, adaptive coping, and life satisfaction. J. Coll. Couns. 2017, 20, 224–236. [Google Scholar] [CrossRef]
- Cheng, C.; Lau, H.P.B.; Chan, M.P.S. Coping flexibility and psychological adjustment to stressful life changes: A meta-analytic review. Psychol. Bull. 2014, 140, 1582–1607. [Google Scholar] [CrossRef]
- Pinto-Gouveia, J.; Galhardo, A.; Cunha, M.; Matos, M. Protective emotional regulation processes towards adjustment in infertile patients. Hum. Fertil. 2012, 15, 27–34. [Google Scholar] [CrossRef]
- Williams, P.; Barclay, L.; Schmied, V. Defining social support in context: A necessary step in improving research, intervention, and practice. Qual. Health Res. 2004, 14, 942–960. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L. Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. J. Loss Trauma 2009, 14, 364–388. [Google Scholar] [CrossRef]
- Taku, K.; Tedeschi, R.G.; Shakespeare-Finch, J.; Krosch, D.; David, G.; Kehl, D.; Grunwald, S.; Romeo, A.; Di Tella, M.; Kamibeppu, K.; et al. Posttraumatic growth (PTG) and posttraumatic depreciation (PTD) across ten countries: Global validation of the PTG-PTD theoretical model. Personal. Individ. Differ. 2021, 169, 110222. [Google Scholar] [CrossRef]
- Steuber, K.R.; Solomon, D.H. Factors that predict married partners’ disclosures about infertility to social network members. J. Appl. Commun. Res. 2011, 39, 250–270. [Google Scholar] [CrossRef]
- Raque-Bogdan, T.L.; Hoffman, M.A. The relationship among infertility, self-compassion, and well-being for women with primary or secondary infertility. Psychol. Women Q. 2015, 39, 484–496. [Google Scholar] [CrossRef]
- Levi-Belz, Y. Stress-related growth among suicide survivors: The role of interpersonal and cognitive factors. Arch. Suicide Res. 2015, 19, 305–320. [Google Scholar] [CrossRef]
- Levi-Belz, Y. To share or not to share? The contribution of self-disclosure to stress-related growth among suicide survivors. Death Stud. 2016, 40, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Karlidere, T.; Bozkurt, A.; Ozmenler, K.N.; Ozsahin, A.; Kucuk, T.; Yetkin, S. The influence of emotional distress on the outcome of in-vitro fertilization (IVF) and/or intracytoplasmic sperm injection (ICSI) treatment among infertile Turkish women. Isr. J. Psychiatry Relat. Sci. 2008, 45, 55–65. [Google Scholar] [PubMed]
- Galhardo, A.; Cunha, M.; Pinto-Gouveia, J.; Matos, M. The mediator role of emotion regulation processes on infertility-related stress. J. Clin. Psychol. Med. Settings 2013, 20, 497–507. [Google Scholar] [CrossRef]
- Agostini, F.; Monti, F.; De Pascalis, L.; Paterlini, M.; La Sala, G.B.; Blickstein, I. Psychosocial support for infertile couples during assisted reproductive technology treatment. Fertil. Steril. 2011, 9, 707–710. [Google Scholar] [CrossRef]
- Rudnik, A.; Piotrowicz, G.; Basińska, M.A.; Rashedi, V. The importance of cognitive flexibility and flexibility in coping with stress for the quality of life in inflammatory bowel disease patients during biological therapy: A preliminary report. Przegląd Gastroenterol. 2019, 14, 121. [Google Scholar] [CrossRef]
- Shrestha, R.; Altice, F.L.; Copenhaver, M.M. HIV-related stigma, motivation to adhere to antiretroviral therapy, and medication adherence among HIV-positive methadone-maintained patients. J. Acquir. Immune Defic. Syndr. 2019, 80, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Felce, D.; Perry, J. Exploring current conceptions of quality of life. In Quality of Life in Health Promotion and Rehabilitation: Conceptual Approaches, Issues, and Application; Renwick, I., Brown, I., Nagler, M., Eds.; Sage: London, UK, 1996; pp. 51–62. [Google Scholar]
- Benyamini, Y.; Gozlan, M.; Kokia, E. Women’s and men’s perceptions of infertility and their associations with psychological adjustment: A dyadic approach. Br. J. Health Psychol. 2009, 14, 1–16. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Jewish (n = 100) | Arab (n = 105) | df | χ2 | ||||
|---|---|---|---|---|---|---|---|
| Variable | Category | Frequency | % | Frequency | % | ||
| Religiosity | Religious | 4 | 4.0 | 27 | 25.7 | 2 | 105.65 *** |
| Traditional | 23 | 23.0 | 74 | 70.5 | |||
| Secular | 73 | 73.0 | 4 | 3.8 | |||
| Place of birth | Abroad | 16 | 16.0 | 0 | 0.0 | 1 | 15.72 *** |
| Israel | 84 | 84.0 | 90 | 100.0 | |||
| Employed outside the home | No | 17 | 17.0 | 57 | 55.3 | 1 | 32.20 *** |
| Yes | 83 | 83.0 | 46 | 44.7 | |||
| Location of treatment | Private clinic | 47 | 48.0 | 47 | 46.1 | 1 | 0.07 |
| Public clinic | 51 | 52.0 | 55 | 53.9 | |||
| Children | No | 71 | 71.0 | 87 | 83.7 | 1 | 4.67 * |
| Yes | 29 | 29.0 | 17 | 16.3 | |||
| Source of problem | Woman | 35 | 37.2 | 22 | 21.4 | 3 | 14.57 ** |
| Spouse | 12 | 12.8 | 32 | 31.1 | |||
| Both | 18 | 19.1 | 11 | 10.7 | |||
| Unknown | 29 | 30.9 | 38 | 36.9 | |||
| Background Variables | Jewish (n = 100) | Arab (n = 105) | df | t | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | N | M | SD | N | |||
| Age | 34.34 | 5.60 | 96 | 27.51 | 4.78 | 97 | 185.80 | 9.11 *** |
| Economic status | 2.62 | 0.82 | 99 | 2.57 | 0.83 | 105 | 202 | 0.79 |
| Education | 3.62 | 0.78 | 100 | 3.59 | 0.66 | 103 | 201 | 0.27 |
| Years of marriage | 4.90 | 3.56 | 84 | 5.13 | 3.96 | 105 | 187 | 0.41 |
| Age of spouse | 35.33 | 5.29 | 83 | 32.96 | 6.62 | 97 | 178 | 2.62 ** |
| Months of fertility treatments | 20.58 | 24.56 | 96 | 30.04 | 31.31 | 96 | 179.80 | 2.33 * |
| Number of treatment cycles | 4.63 | 3.81 | 91 | 4.93 | 4.47 | 87 | 169.94 | 0.49 |
| Jewish | Arab | F(1, 203) | ηp2 | |||
|---|---|---|---|---|---|---|
| M | S.D. | M | S.D. | |||
| Stress | 2.54 | 0.49 | 2.47 | 0.45 | 1.16 | 0.006 |
| Life satisfaction | 4.18 | 1.25 | 4.33 | 1.23 | 0.80 | 0.004 |
| Personal growth | 3.83 | 0.99 | 4.39 | 0.60 | 24.69 *** | 0.108 |
| Perceived stigma | 1.92 | 0.59 | 2.22 | 0.70 | 10.71 ** | 0.050 |
| Individualism | 3.48 | 0.37 | 3.62 | 0.39 | 6.20 * | 0.030 |
| Collectivism | 3.68 | 0.33 | 3.70 | 0.33 | 0.10 | 0.000 |
| Coping flexibility | 3.00 | 0.38 | 3.41 | 0.37 | 60.89 *** | 0.231 |
| Stress | Life Satisfaction | Personal Growth | Perceived Stigma | Individualism | Collectivism | Coping Flexibility | |
|---|---|---|---|---|---|---|---|
| Stress | - | −0.42 *** | −0.24 * | 0.40*** | 0.16 | −0.18 | −0.37 *** |
| Life satisfaction | −0.57 *** | - | 0.33 ** | −0.22* | 0.07 | 0.22 * | 0.23 * |
| Personal growth | −0.35 *** | 0.59 *** | - | −0.09 | 0.20 * | 0.36 *** | 0.43 *** |
| Perceived stigma | 0.17 | −0.19 | 0.03 | - | 0.21 * | 0.08 | −0.01 |
| Individualism | −0.02 | 0.19 | 0.09 | 0.05 | - | 0.20 * | 0.22 * |
| Collectivism | 0.07 | 0.25 * | 0.22 * | 0.04 | 0.31 ** | - | 0.25 * |
| Coping flexibility | −0.21* | 0.31 ** | 0.35 *** | −0.004 | 0.26 ** | 0.17 | - |
| Personal Growth | Life Satisfaction | |||||
|---|---|---|---|---|---|---|
| β | t | ∆R2 | β | t | ∆R2 | |
| Step 1 | 0.15 *** | 0.217 *** | ||||
| Ethnicity a | 0.32 | 3.93 *** | 0.06 | 0.81 | ||
| Age | −0.06 | −0.75 | −0.08 | −1.03 | ||
| Economic status | 0.14 | 2.18 * | 0.38 | 6.06 *** | ||
| Months of fertility treatments | −0.08 | −0.93 | 0.05 | 0.68 | ||
| Fertility treatment cycles | −0.07 | −0.86 | −0.24 | −3.13 ** | ||
| Children b | −0.004 | 0.05 | 0.15 | 2.23 | ||
| R2 | 0.15 *** | 0.22 *** | ||||
| F | 5.81 *** | 9.14 *** | ||||
| Step 2 | 0.054 *** | 0.188 *** | ||||
| Stress | −0.24 | −3.66 ** | −0.45 | −7.89 *** | ||
| R2 | 0.204 *** | 0.41 *** | ||||
| F | 7.20 *** | 19.14 *** | ||||
| Step 3 | 0.119 *** | 0.056 ** | ||||
| Coping flexibility | 0.31 | 4.06 *** | 0.14 | 2.06 * | ||
| Perceived stigma | 0.01 | 0.17 | −0.08 | −1.31 | ||
| Individualism | 0.01 | 0.21 | 0.07 | 1.26 | ||
| Collectivism | 0.17 | 2.68 ** | 0.14 | 2.46 * | ||
| R2 | 0.323 *** | 0.46 *** | ||||
| F | 8.37 *** | 14.99 *** | ||||
| Step 4 | 0.08 *** | 0.011 | ||||
| Stress X Stigma | −0.12 | −1.99 * | −0.10 | −1.82 | ||
| Stress X Coping flexibility | 0.18 | 2.83 ** | −0.04 | −0.67 | ||
| Stress X Individualism | −0.14 | −2.15 * | −0.04 | −0.65 | ||
| Stress X Collectivism | 0.19 | 3.13 ** | −0.02 | −0.36 | ||
| Stress X Ethnicity | −0.03 | −0.26 | −0.16 | −1.69 | ||
| R2 | 0.403 *** | 0.472 *** | ||||
| F | 8.45 *** | 11.26 *** | ||||
| R2 | 0.403 *** | 0.472 *** | ||||
| F | 6.69 | 8.70 *** | ||||
| β | t | ∆R2 | |
|---|---|---|---|
| Step 1 | 0.150 | ||
| Ethnicity a | 0.32 | 3.93 *** | |
| Age | −0.06 | −0.75 | |
| Economic status | 0.14 | 2.18 * | |
| Months of fertility treatments | −0.08 | −0.93 | |
| Fertility treatment cycles | −0.07 | −0.86 | |
| Children b | −0.004 | −0.05 | |
| Step 2 | 0.054 *** | ||
| Stress | −0.24 | −3.66 *** | |
| Step 3 | 0.073 ** | ||
| Stress2 | −0.27 | −4.40 *** | |
| R2 | 0.277 | ||
| F(8, 196) | 9.37 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Sharkia, S.; Taubman - Ben-Ari, O.; Mofareh, A. Personal Growth and Life Satisfaction during Fertility Treatment—A Comparison between Arab and Jewish Women. Int. J. Environ. Res. Public Health 2023, 20, 2187. https://doi.org/10.3390/ijerph20032187
Abu-Sharkia S, Taubman - Ben-Ari O, Mofareh A. Personal Growth and Life Satisfaction during Fertility Treatment—A Comparison between Arab and Jewish Women. International Journal of Environmental Research and Public Health. 2023; 20(3):2187. https://doi.org/10.3390/ijerph20032187
Chicago/Turabian StyleAbu-Sharkia, Salam, Orit Taubman - Ben-Ari, and Ali Mofareh. 2023. "Personal Growth and Life Satisfaction during Fertility Treatment—A Comparison between Arab and Jewish Women" International Journal of Environmental Research and Public Health 20, no. 3: 2187. https://doi.org/10.3390/ijerph20032187
APA StyleAbu-Sharkia, S., Taubman - Ben-Ari, O., & Mofareh, A. (2023). Personal Growth and Life Satisfaction during Fertility Treatment—A Comparison between Arab and Jewish Women. International Journal of Environmental Research and Public Health, 20(3), 2187. https://doi.org/10.3390/ijerph20032187