
New Conservative Approach for the Management of Recurrent Sublingual Ranula—A Case Report

 ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
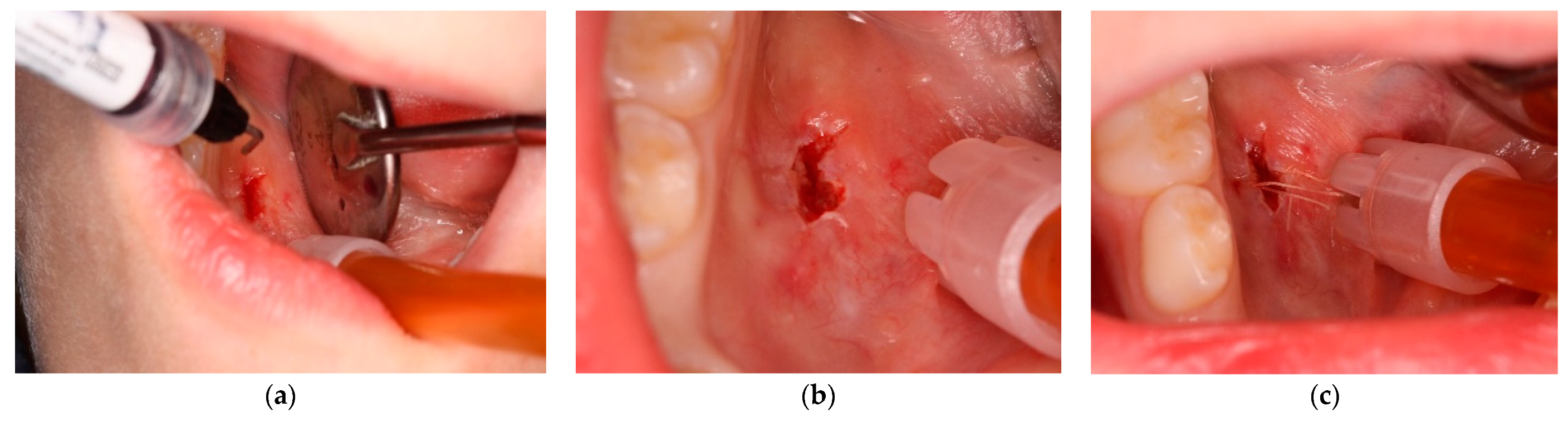
- Anesthesia. Premedication with topical anesthesia (Xylonor Spray—10% lidocaine analgesic solution; Septodont) was followed by infiltration with mepivacaine (Pierrel S.p.A. mepivacaine 20 mg/mL and adrenaline 1:100,000) around the margins of the lesion.
- Incision. Soft tissue incisions with microsurgical scissors to remove the pseudocystic dome and provide adequate access to the area of interest.
- Probing and irrigation. The lumen of the lesion was probed, irrigated with sterile saline solution, and dried with cotton gauze.
- Application of Hybenx®. Hybenx® gel was injected into the lumen of the lesion. The choice of gel was based on its consistency to avoid dispersion of the product into the surrounding tissues. The gel (0.5 mL) was allowed to act for approximately 20 s and then aspirated, and the area was rinsed with copious amounts of saline solution. After complete and careful gel removal, the lesion margins appeared opaque white, with no signs of bleeding.
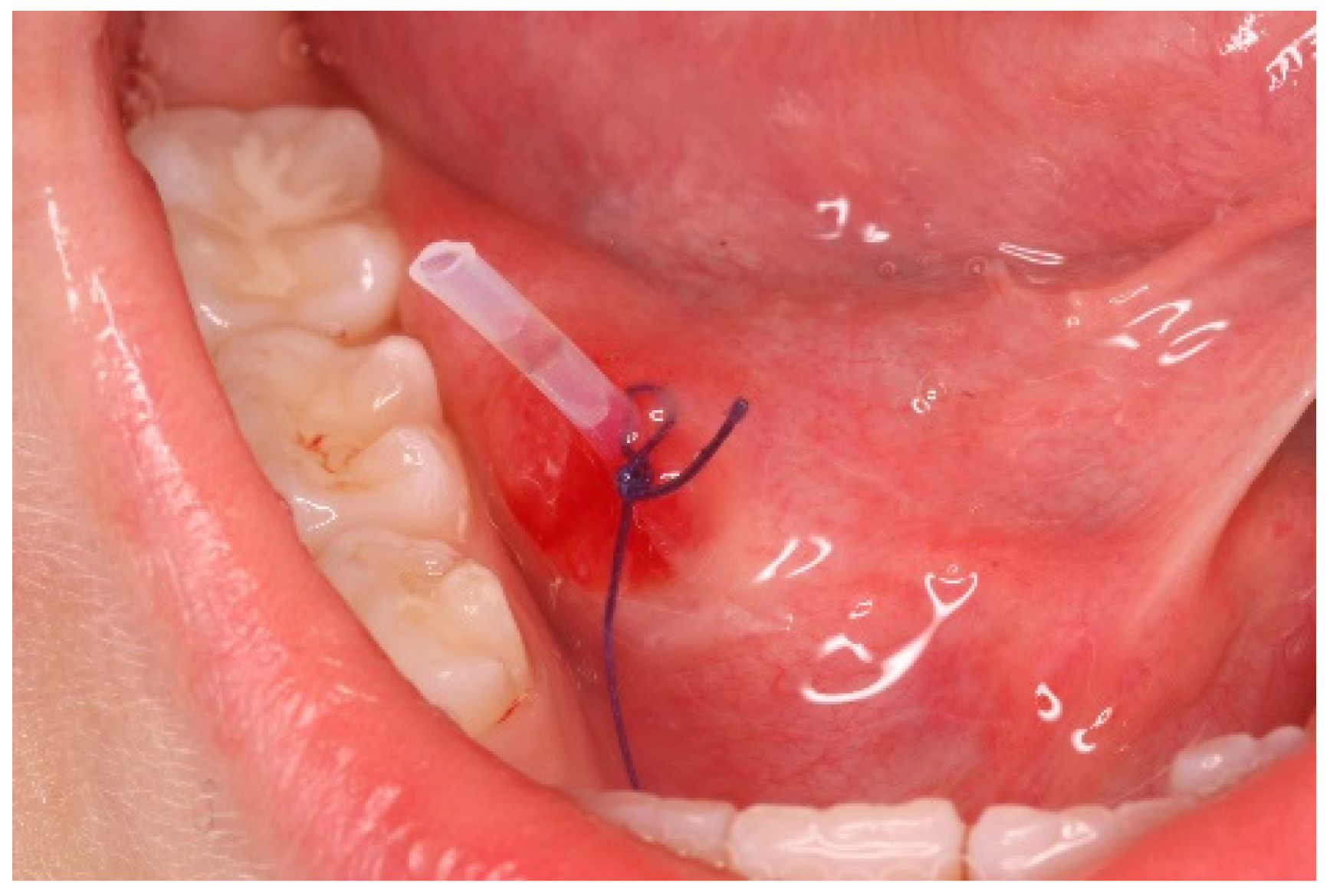
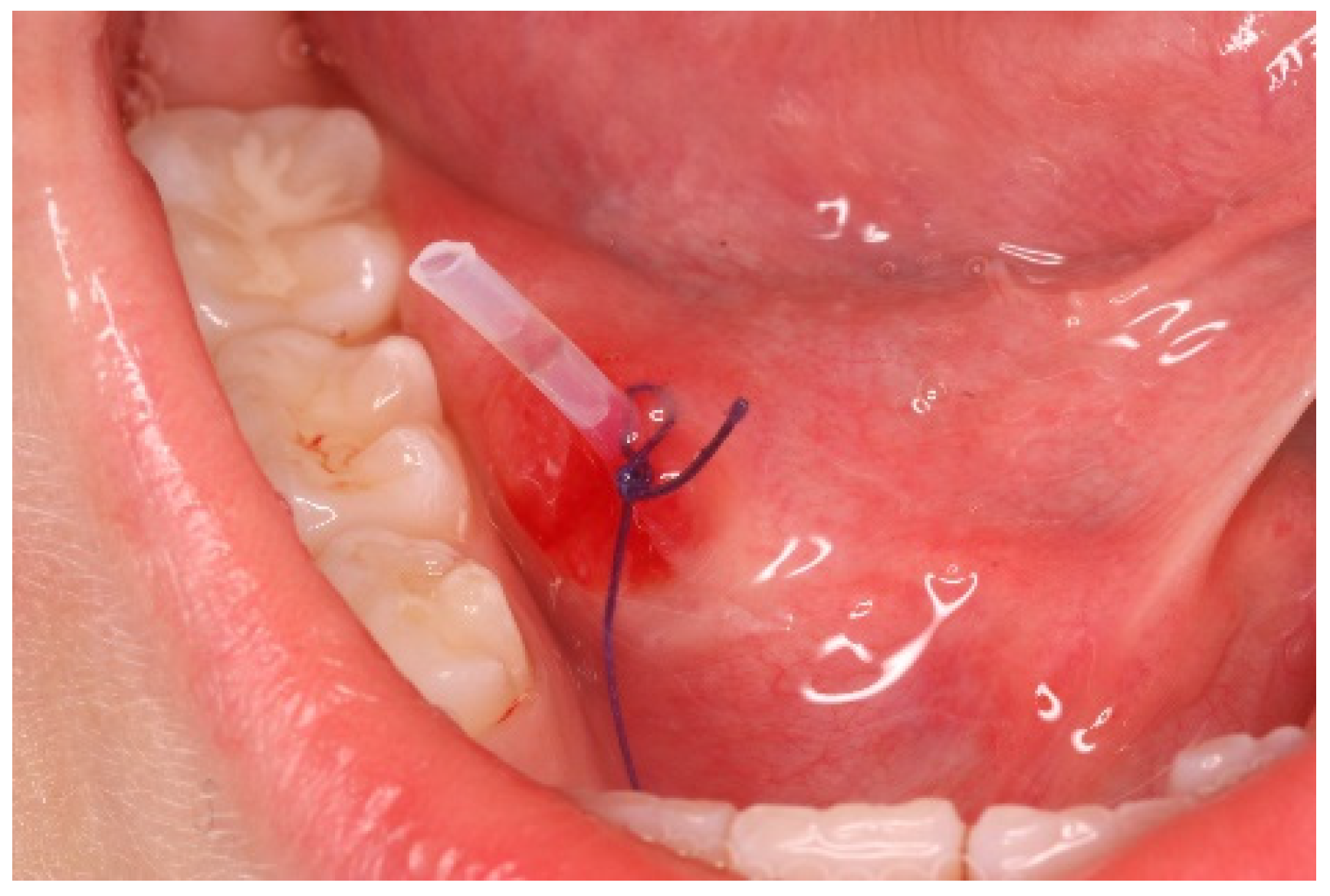
- Suturing. To delay closure of the ostium and inversion of the margins of the lesion, horizontal mattress sutures (6-0 coated Vicryl® undyed 1 × 18″ s-14 double armed—Ethicon®) were performed to evert the wound edges and keep the ostium open (Figure 5).
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhao, Y.F.; Jia, Y.; Chen, X.M.; Zhang, W.F. Clinical review of 580 ranulas. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Zhi, K.; Gao, L.; Ren, W. What is new in management of pediatric ranula? Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Chin, S.J.; Zeng, I.S.; Morton, R.P. The epidemiology of plunging ranula in South Auckland. Laryngoscope 2016, 126, 2739–2743. [Google Scholar] [CrossRef]
- Vallogini, G.; Nobili, V.; Rongo, R.; De Rosa, S.; Magliarditi, F.; D’Anto, V.; Galeotti, A. Evaluation of the relationship between obesity, dental caries and periodontal disease in adolescents. Eur. J. Paediatr. Dent. 2017, 18, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Bowers, E.M.R.; Schaitkin, B. Management of Mucoceles, Sialoceles, and Ranulas. Otolaryngol. Clin. North Am. 2021, 54, 543–551. [Google Scholar] [CrossRef]
- Bucci, R.; Montanaro, D.; Rongo, R.; Valletta, R.; Michelotti, A.; D’Anto, V. Effects of maxillary expansion on the upper airways: Evidence from systematic reviews and meta-analyses. J. Oral Rehabil. 2019, 46, 377–387. [Google Scholar] [CrossRef]
- Parekh, D.; Stewart, M.; Joseph, C.; Lawson, H.H. Plunging ranula: A report of three cases and review of the literature. Br. J. Surg. 1987, 74, 307–309. [Google Scholar] [CrossRef]
- Sigismund, P.E.; Bozzato, A.; Schumann, M.; Koch, M.; Iro, H.; Zenk, J. Management of ranula: 9 years’ clinical experience in pediatric and adult patients. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2013, 71, 538–544. [Google Scholar] [CrossRef]
- Bhaskar, S.N.; Bolden, T.E.; Weinmann, J.P. Pathogenesis of mucoceles. J. Dent. Res. 1956, 35, 863–874. [Google Scholar] [CrossRef]
- Harrison, J.D. Modern management and pathophysiology of ranula: Literature review. Head Neck 2010, 32, 1310–1320. [Google Scholar] [CrossRef]
- Madariaga, A.C.P.; Bucci, R.; Rongo, R.; Simeon, V.; D’Anto, V.; Valletta, R. Impact of Fixed Orthodontic Appliance and Clear Aligners on the Periodontal Health: A Prospective Clinical Study. Dent. J. 2020, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Mun, S.J.; Choi, H.G.; Kim, H.; Park, J.H.; Jung, Y.H.; Sung, M.W.; Kim, K.H. Ductal variation of the sublingual gland: A predisposing factor for ranula formation. Head Neck 2014, 36, 540–544. [Google Scholar] [CrossRef]
- Davison, M.J.; Morton, R.P.; McIvor, N.P. Plunging ranula: Clinical observations. Head Neck 1998, 20, 63–68. [Google Scholar] [CrossRef]
- Sergio Paduano, M.D.; Bucci, R.; Rongo, R.; Silva, R.; Michelotti, A. Prevalence of temporomandibular disorders and oral parafunctions in adolescents from public schools in Southern Italy. Cranio J. Craniomandib. Pract. 2020, 38, 370–375. [Google Scholar] [CrossRef]
- Morita, Y.; Sato, K.; Kawana, M.; Takahasi, S.; Ikarashi, F. Treatment of ranula--excision of the sublingual gland versus marsupialization. Auris Nasus Larynx 2003, 30, 311–314. [Google Scholar] [CrossRef]
- Chung, Y.S.; Cho, Y.; Kim, B.H. Comparison of outcomes of treatment for ranula: A proportion meta-analysis. Br. J. Oral Maxillofac. Surg. 2019, 57, 620–626. [Google Scholar] [CrossRef]
- Michelotti, A.; Rongo, R.; Valentino, R.; D’Anto, V.; Bucci, R.; Danzi, G.; Cioffi, I. Evaluation of masticatory muscle activity in patients with unilateral posterior crossbite before and after rapid maxillary expansion. Eur. J. Orthod. 2019, 41, 46–53. [Google Scholar] [CrossRef]
- Laranne, J.; Keski-Nisula, L.; Rautio, R.; Rautiainen, M.; Airaksinen, M. OK-432 (Picibanil) therapy for lymphangiomas in children. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. 2002, 259, 274–278. [Google Scholar] [CrossRef]
- Roh, J.L.; Kim, H.S. Primary treatment of pediatric plunging ranula with nonsurgical sclerotherapy using OK-432 (Picibanil). Int. J. Pediatric Otorhinolaryngol. 2008, 72, 1405–1410. [Google Scholar] [CrossRef]
- Patel, M.R.; Deal, A.M.; Shockley, W.W. Oral and plunging ranulas: What is the most effective treatment? Laryngoscope 2009, 119, 1501–1509. [Google Scholar] [CrossRef]
- Wendt, M.; Papatziamos, G.; Munck-Wikland, E.; Marklund, L. Sclerotherapy of ranulas with OK-432—a prospective, randomized, double-blinded placebo-controlled study. Acta Oto-Laryngol. 2021, 141, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Hegde, S.; Bubna, K.; Rao, D. Management of Ranula in a Child by Modified Micro-Marsupialization Technique: A Case Report. J. Clin. Pediatric Dent. 2017, 41, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Verma, D.K.; Goyal, S.; Rai, M. Comparison of Micromarsupialization and Modified Micromarsupialization for the Management of Mucocoele of Lower Lip: A Prospective Randomized Clinical Trial. J. Maxillofac. Oral Surg. 2017, 16, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Sandrini, F.A.; Sant’ana-Filho, M.; Rados, P.V. Ranula management: Suggested modifications in the micro-marsupialization technique. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2007, 65, 1436–1438. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.R.; Al-Johani, K.; Fedele, S.; Moles, D.R. Randomised controlled trial of the efficacy of HybenX in the symptomatic treatment of recurrent aphthous stomatitis. Oral Dis. 2009, 15, 155–161. [Google Scholar] [CrossRef]
- Antonelli, A.; Giovannini, L.; Baccani, I.; Giuliani, V.; Pace, R.; Rossolini, G.M. In Vitro Antimicrobial Activity of the Decontaminant HybenX((R)) Compared to Chlorhexidine and Sodium Hypochlorite against Common Bacterial and Yeast Pathogens. Antibiotics 2019, 8, 188. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, M.D.; Prasad, H.S.; Savord, E.G. A histologic assessment of a HYBENX(R) oral tissue decontaminant in vital pulp therapy in dogs. J. Biol. Regul. Homeost. Agents 2016, 30, 189–197. [Google Scholar]
- Lee, H.M.; Lim, H.W.; Kang, H.J.; Chae, S.W.; Hwang, S.J.; Jung, K.Y.; Woo, J.S. Treatment of ranula in pediatric patients with intralesional injection of OK-432. Laryngoscope 2006, 116, 966–969. [Google Scholar] [CrossRef]
- Roh, J.L. Primary treatment of ranula with intracystic injection of OK-432. Laryngoscope 2006, 116, 169–172. [Google Scholar] [CrossRef]
- Fukase, S.; Ohta, N.; Inamura, K.; Aoyagi, M. Treatment of ranula wth intracystic injection of the streptococcal preparation OK-432. Ann. Otol. Rhinol. Laryngol. 2003, 112, 214–220. [Google Scholar] [CrossRef]
- Kono, M.; Satomi, T.; Abukawa, H.; Hasegawa, O.; Watanabe, M.; Chikazu, D. Evaluation of OK-432 Injection Therapy as Possible Primary Treatment of Intraoral Ranula. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2017, 75, 336–342. [Google Scholar] [CrossRef]
- Rebuffini, E.; Zuccarino, L.; Grecchi, E.; Carinci, F.; Merulla, V.E. Picibanil (OK-432) in the treatment of head and neck lymphangiomas in children. Dent. Res. J. 2012, 9, S192–S196. [Google Scholar] [CrossRef]
- Kim, M.G.; Kim, S.G.; Lee, J.H.; Eun, Y.G.; Yeo, S.G. The therapeutic effect of OK-432 (picibanil) sclerotherapy for benign neck cysts. Laryngoscope 2008, 118, 2177–2181. [Google Scholar] [CrossRef]
- Choi, M.G. Case report of the management of the ranula. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 357–363. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorino, A.; Staderini, E.; Diana, R.; Rengo, C.; Gallenzi, P. New Conservative Approach for the Management of Recurrent Sublingual Ranula—A Case Report. Int. J. Environ. Res. Public Health 2023, 20, 2398. https://doi.org/10.3390/ijerph20032398
Fiorino A, Staderini E, Diana R, Rengo C, Gallenzi P. New Conservative Approach for the Management of Recurrent Sublingual Ranula—A Case Report. International Journal of Environmental Research and Public Health. 2023; 20(3):2398. https://doi.org/10.3390/ijerph20032398
Chicago/Turabian StyleFiorino, Antonino, Edoardo Staderini, Rosalba Diana, Carlo Rengo, and Patrizia Gallenzi. 2023. "New Conservative Approach for the Management of Recurrent Sublingual Ranula—A Case Report" International Journal of Environmental Research and Public Health 20, no. 3: 2398. https://doi.org/10.3390/ijerph20032398
APA StyleFiorino, A., Staderini, E., Diana, R., Rengo, C., & Gallenzi, P. (2023). New Conservative Approach for the Management of Recurrent Sublingual Ranula—A Case Report. International Journal of Environmental Research and Public Health, 20(3), 2398. https://doi.org/10.3390/ijerph20032398